Degree of Left Renal Vein Compression Predicts Nutcracker Syndrome

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
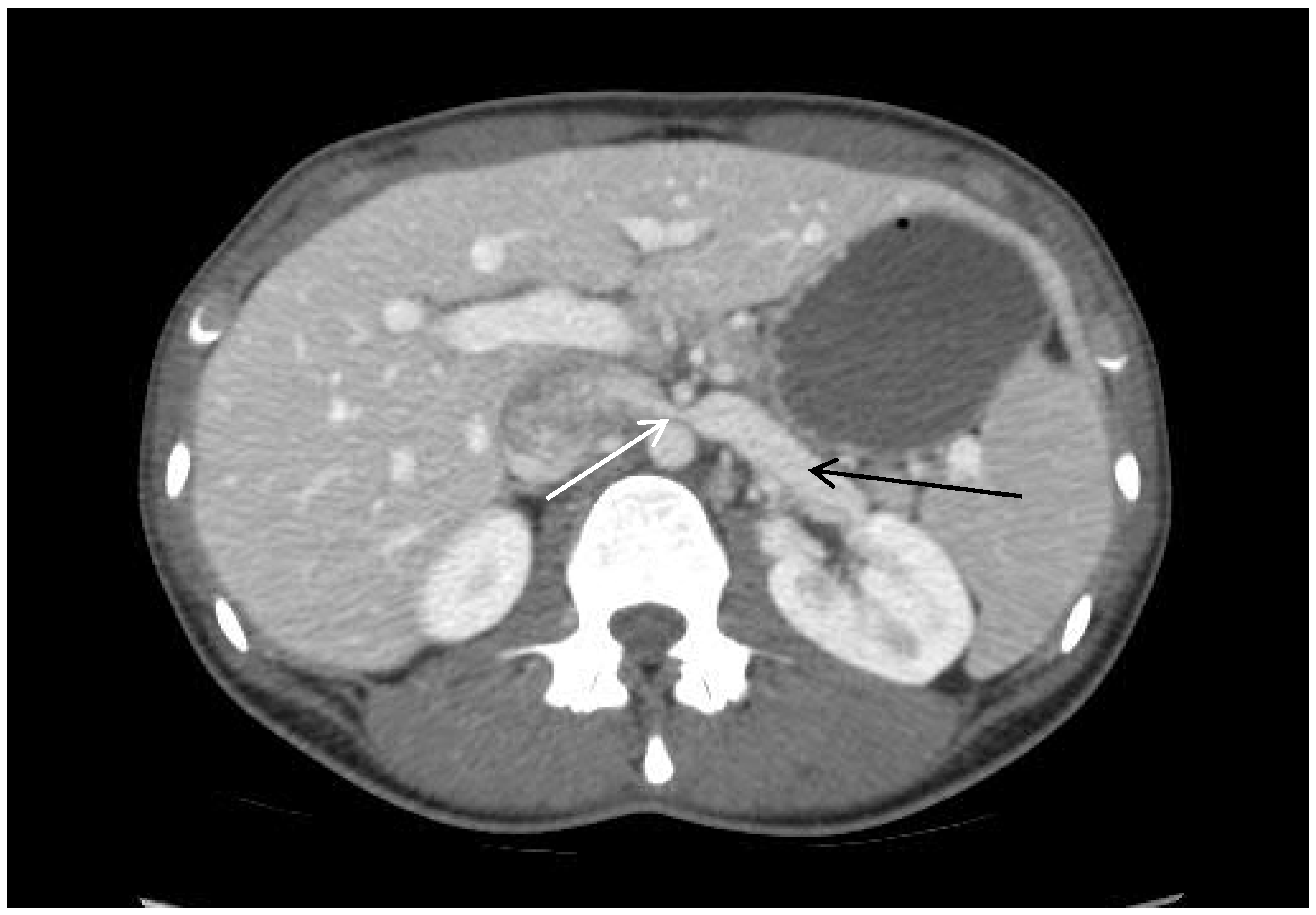
2.1. Image Analysis, Patient Presentation
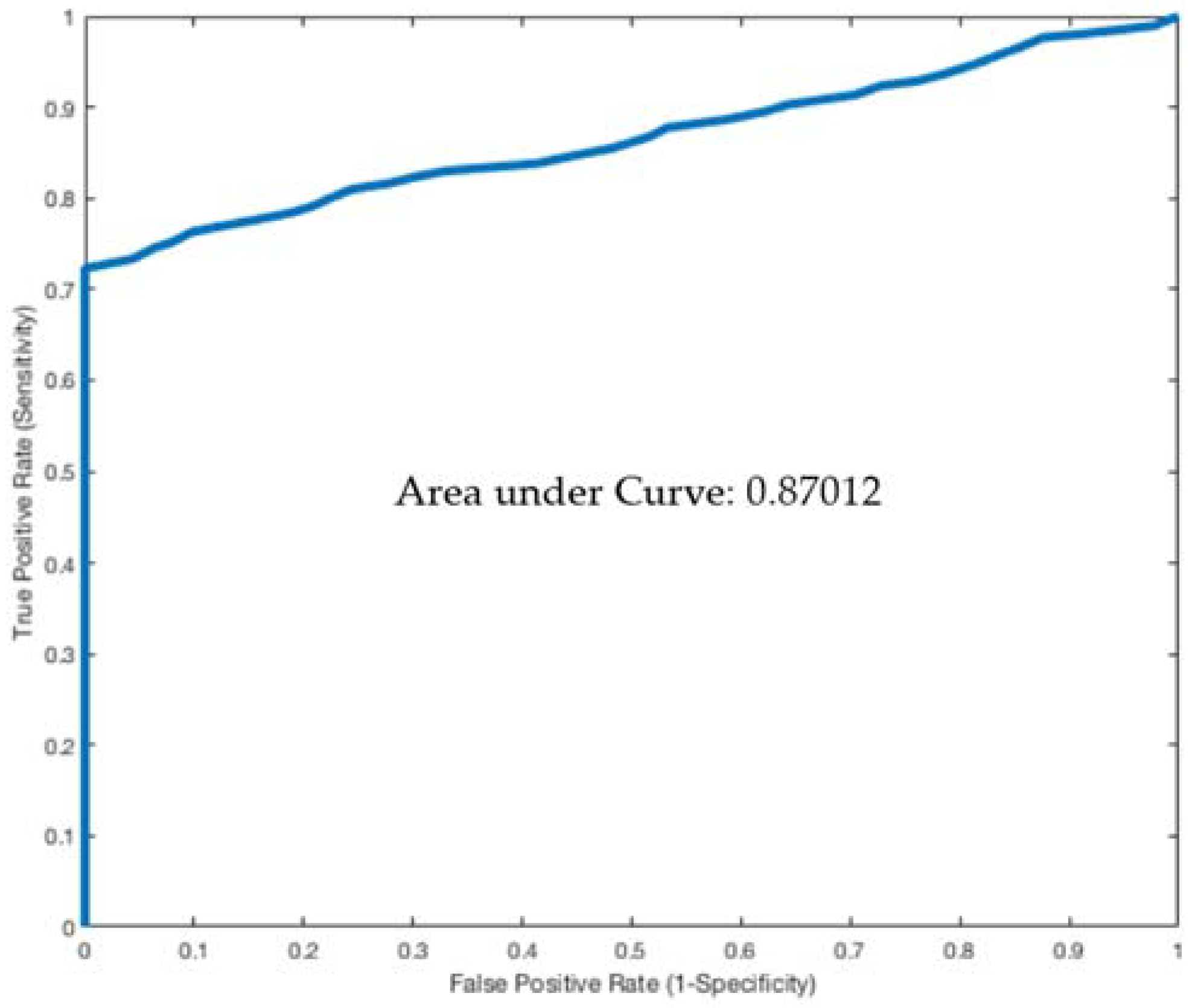
2.2. Statistical Analysis
3. Results
3.1. Patient Characteristics and Symptoms
3.2. Imaging Characteristics
4. Discussion
5. Conclusions
Author Contributions
Acknowledgments
Conflicts of Interest
References
- He, Y.; Wu, Z.; Chen, S.; Tian, L.; Li, D.; Li, M.; Jin, W.; Zhang, H. Nutcracker syndrome—How well do we know it? Urology 2014, 83, 12–17. [Google Scholar] [CrossRef] [PubMed]
- Zhang, H.; Li, M.; Jin, W.; San, P.; Xu, P.; Pan, S. The left renal entrapment syndrome: Diagnosis and treatment. Ann. Vasc. Surg. 2007, 21, 198–203. [Google Scholar] [CrossRef] [PubMed]
- Kurklinsky, A.K.; Rooke, T.W. Nutcracker phenomenon and nutcracker syndrome. Mayo Clin. Proc. 2010, 85, 552–559. [Google Scholar] [CrossRef] [PubMed]
- El-Sadr, A.R.; Mina, E. Anatomical and surgical aspects in the operative management of varicocele. Urol. Cutaneous. Rev. 1950, 54, 257–262. [Google Scholar] [PubMed]
- Polguj, M.; Topol, M.; Majos, A. An unusual case of left venous renal entrapment syndrome: A new type of nutcracker phenomenon? Surg. Radiol. Anat. 2013, 35, 263–267. [Google Scholar] [CrossRef] [PubMed]
- Grimm, L.J.; Engstrom, B.I.; Nelson, R.C.; Kim, C.Y. Incidental detection of nutcracker phenomenon on multidetector CT in an asymptomatic population: Prevalence and associated findings. J. Comput. Assist. Tomogr. 2013, 37, 415–418. [Google Scholar] [CrossRef] [PubMed]
- Velasquez, C.A.; Saeyeldin, A.; Zafar, M.A.; Brownstein, A.J.; Erben, Y. A systematic review on management of nutcracker syndrome. J. Vasc. Surg. Venous Lymphat. Disord. 2018, 6, 271–278. [Google Scholar] [CrossRef] [PubMed]
- Ahmed, K.; Sampath, R.; Khan, M.S. Current trends in the diagnosis and management of renal nutcracker syndrome: A review. Eur. J. Vasc. Endovasc. Surg. 2006, 31, 410–416. [Google Scholar] [CrossRef] [PubMed]
- Rudloff, U.; Holmes, R.J.; Prem, J.T.; Faust, G.R.; Moldwin, R.; Siegel, D. Mesoaortic Compression of the Left Renal Vein (Nutcracker Syndrome): Case Reports and Review of the Literature. Ann. Vasc. Surg. 2006, 20, 120–129. [Google Scholar] [CrossRef] [PubMed]
- Menard, M.T. Nutcracker syndrome: When should it be treated and how? Perspect. Vasc. Surg. Endovasc. Ther. 2009, 21, 117–124. [Google Scholar] [CrossRef] [PubMed]
- Kibbe, M.R.; Ujiki, M.; Goodwin, A.L.; Eskandari, M.; Yao, J.; Matsumura, J. Iliac vein compression in an asymptomatic patient population. J. Vasc. Surg. 2004, 39, 937–943. [Google Scholar] [CrossRef] [PubMed]
- McDermott, S.; Oliveira, G.; Ergul, E.; Brazeau, N.; Wicky, S.; Oklu, R. May-Thurner syndrome: Can it be diagnosed by a single MR venography study? Diagn. Interv. Radiol. 2013, 19, 44–48. [Google Scholar] [PubMed]
- Kim, K.W.; Cho, J.Y.; Kim, S.H.; Yoon, J.H.; Kim, D.S.; Chung, J.W.; Park, J.H. Diagnostic value of computed tomographic findings of nutcracker syndrome: Correlation with renal venography and renocaval pressure gradients. Eur. J. Radiol. 2011, 80, 648–654. [Google Scholar] [CrossRef] [PubMed]
- Fong, J.K.; Poh, A.C.; Tan, A.G.; Taneja, R. Imaging findings and clinical features of abdominal vascular compression syndromes. AJR Am. J. Roentgenol. 2014, 203, 29–36. [Google Scholar] [CrossRef] [PubMed]
- Venkatachalam, S.; Bumpus, K.; Kapadia, S.R.; Gray, B.; Lyden, S.; Shishehbor, M.H. The nutcracker syndrome. Ann. Vasc. Surg. 2011, 25, 1154–1164. [Google Scholar] [CrossRef] [PubMed]
- Pascarella, L.; Penn, A.; Schmid-Schonbein, G.W. Venous hypertension and the inflammatory cascade: Major manifestations and trigger mechanisms. Angiology 2005, 56 (Suppl. 1), S3–S10. [Google Scholar] [CrossRef] [PubMed]
- Takebayashi, S.; Ueki, T.; Ikeda, N.; Fujikawa, A. Diagnosis of the nutcracker syndrome with color Doppler sonography: Correlation with flow patterns on retrograde left renal venography. AJR Am. J. Roentgenol. 1999, 172, 39–43. [Google Scholar] [CrossRef] [PubMed]
- Pytel, A. Renal fornical hemorrhages: Their pathogenesis and treatment. J. Urol. 1960, 83, 783–789. [Google Scholar] [CrossRef]
- Shin, J.I.; Park, J.M.; Lee, J.S.; Kim, M.J. Effect of renal Doppler ultrasound on the detection of nutcracker syndrome in children with hematuria. Eur. J. Pediatr. 2007, 166, 399–404. [Google Scholar] [CrossRef] [PubMed]
- Stapleton, F.B.; Roy, S., 3rd; Noe, H.N.; Jerkins, G. Hypercalciuria in children with hematuria. N. Engl. J. Med. 1984, 310, 1345–1348. [Google Scholar] [CrossRef] [PubMed]
- Stavros, A.T.; Sickler, K.J.; Menter, R.R. Color duplex sonography of the nutcracker syndrome (aortomesenteric left renal vein compression). J. Ultrasound. Med. 1994, 13, 569–574. [Google Scholar] [CrossRef] [PubMed]
- Shaper, K.R.; Jackson, J.E.; Williams, G. The nutcracker syndrome: An uncommon cause of haematuria. Br. J. Urol. 1994, 74, 144–146. [Google Scholar] [CrossRef] [PubMed]
- Hanna, H.E.; Santella, R.N.; Zawada, E.T., Jr.; Masterson, T.E. Nutcracker syndrome: An underdiagnosed cause for hematuria? S. D. J. Med. 1997, 50, 429–436. [Google Scholar] [PubMed]



{kind=link}
{kind=link}
| Nutcracker (n = 33) | Controls (n = 103) | p-Value | |
|---|---|---|---|
| Female (%) | 32 (97.0%) | 60 (58.2%) | 0.001 |
| Age, years | 46.2 ± 3.3 | 46.7 ± 1.7 | 0.5 |
| BMI | 21.4 ± 0.7 | 27.2 ± 0.5 | <0.0001 |
| Hematuria | 19 (57.6%) | 12 (11.7%) | <0.0001 |
| Left Flank Pain | 10 (30.3%) | 2 (1.9%) | <0.0001 |
| Abdominal Pain | 24 (72.7%) | 11 (10.6%) | <0.0001 |
| Proteinuria | 13 (39.4%) | 7 (6.8%) | 0.001 |
| Nutcracker | Controls | p-Value | |
|---|---|---|---|
| Compression Percentage | 74.5 ± 1.9 | 25.2 ± 2.4 | <0.0001 |
| Diameter Pre-Compression (mm) | 10.7 ± 0.4 | 10.2 ± 0.4 | 0.42 |
| Diameter at Compression (mm) | 2.6 ± 0.2 | 7.0 ± 0.4 | <0.0001 |
| Ratio of Diameter at Compression vs. Pre-Compression | 4.6 ± 0.3 | 1.6 ± 0.1 | <0.0001 |
| Hematuria | Proteinuria | Abdominal Pain | Left Flank Pain | |||||
|---|---|---|---|---|---|---|---|---|
| Coeff (SD) | p-Val | Coeff (SD) | p-Val | Coeff (SD) | p-Val | Coeff (SD) | p-Val | |
| Age | 0.01 (0.01) | 0.31 | 0.01 (0.01) | 0.67 | 0.01 (0.01) | 0.27 | 0.004 (0.02) | 0.82 |
| Gender | −0.64 (0.63) | 0.31 | −0.83 (0.83) | 0.32 | 0.64 (0.60) | 0.28 | 1.0 (1.1) | 0.38 |
| BMI | −0.07 (0.06) | 0.23 | 0.07 (0.89) | 0.34 | −0.19 (0.07) | 0.005 | 0.004 (0.09) | 1.0 |
| Percent LRV Compression | −0.02 (0.01) | 0.01 | −0.04 (0.01) | 0.002 | −0.03 (0.01) | 0.007 | 0.03 (0.02) | 0.06 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hangge, P.T.; Gupta, N.; Khurana, A.; Quencer, K.B.; Albadawi, H.; Alzubaidi, S.J.; Knuttinen, M.-G.; Naidu, S.G.; Oklu, R. Degree of Left Renal Vein Compression Predicts Nutcracker Syndrome. J. Clin. Med. 2018, 7, 107. https://doi.org/10.3390/jcm7050107
Hangge PT, Gupta N, Khurana A, Quencer KB, Albadawi H, Alzubaidi SJ, Knuttinen M-G, Naidu SG, Oklu R. Degree of Left Renal Vein Compression Predicts Nutcracker Syndrome. Journal of Clinical Medicine. 2018; 7(5):107. https://doi.org/10.3390/jcm7050107
Chicago/Turabian StyleHangge, Patrick T., Nikhil Gupta, Aditya Khurana, Keith B. Quencer, Hassan Albadawi, Sadeer J. Alzubaidi, M-Grace Knuttinen, Sailendra G. Naidu, and Rahmi Oklu. 2018. "Degree of Left Renal Vein Compression Predicts Nutcracker Syndrome" Journal of Clinical Medicine 7, no. 5: 107. https://doi.org/10.3390/jcm7050107