Association of Cardiovascular Health with Epicardial Adipose Tissue and Intima Media Thickness: The Kardiovize Study

 , , , , ,
, , , , , 
Abstract
:1. Introduction
2. Methods
2.1. Study Design and Participants
2.2. Anthropometric Assessment
2.3. Physical Examination and Laboratory Analyses
2.4. Ideal Cardiovascular Health Score
2.5. Echocardiographic Measurement of Epicardial Fat Thickness
2.6. Measurement of Carotid Intima-Media Thickness
2.7. Statistical Analyses
3. Results
3.1. Study Population
3.2. Differences in Anthropometric Characteristics and Cardiovascular Parameters by Gender
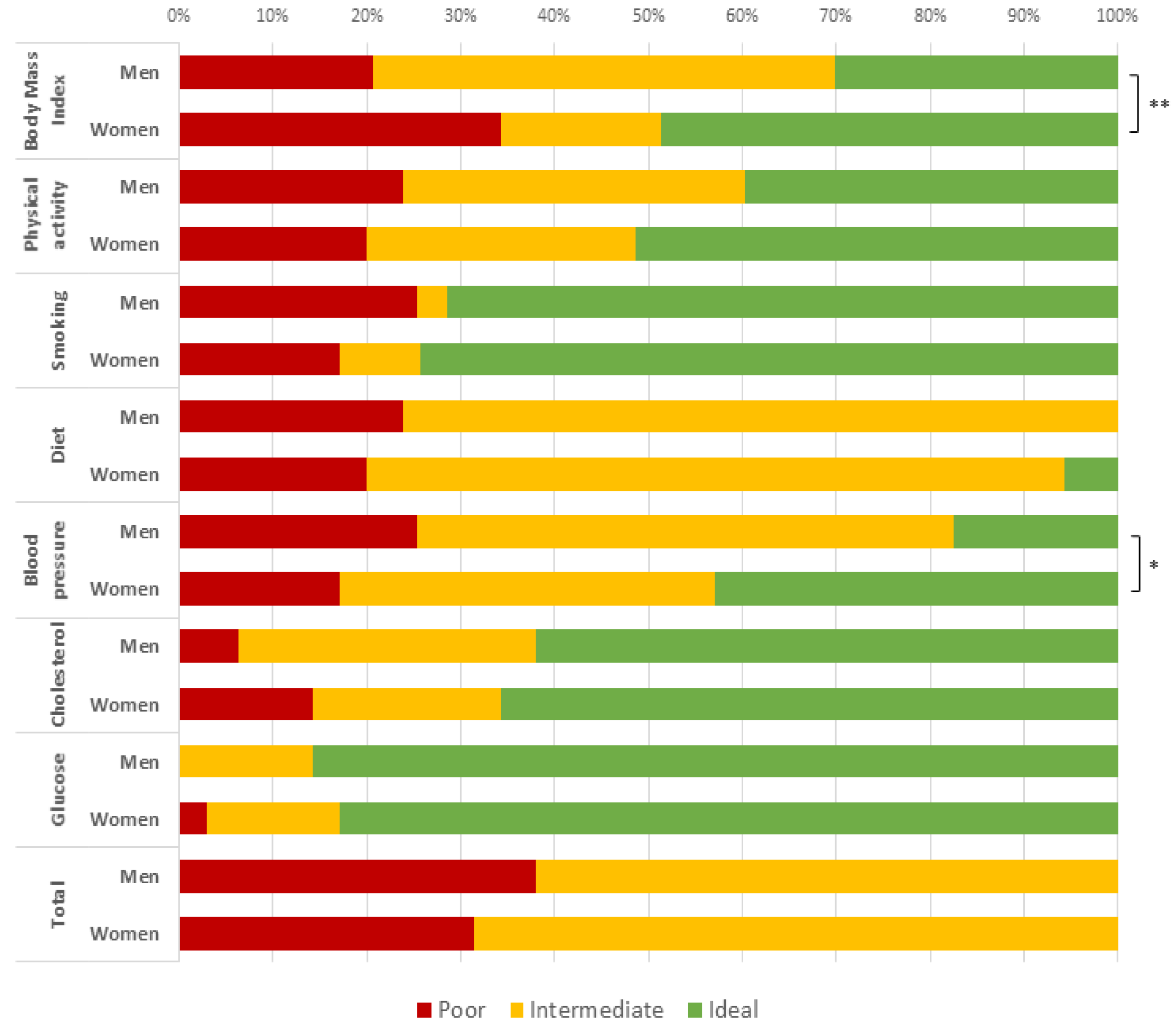
3.3. Ideal Cardiovascular Health and Score
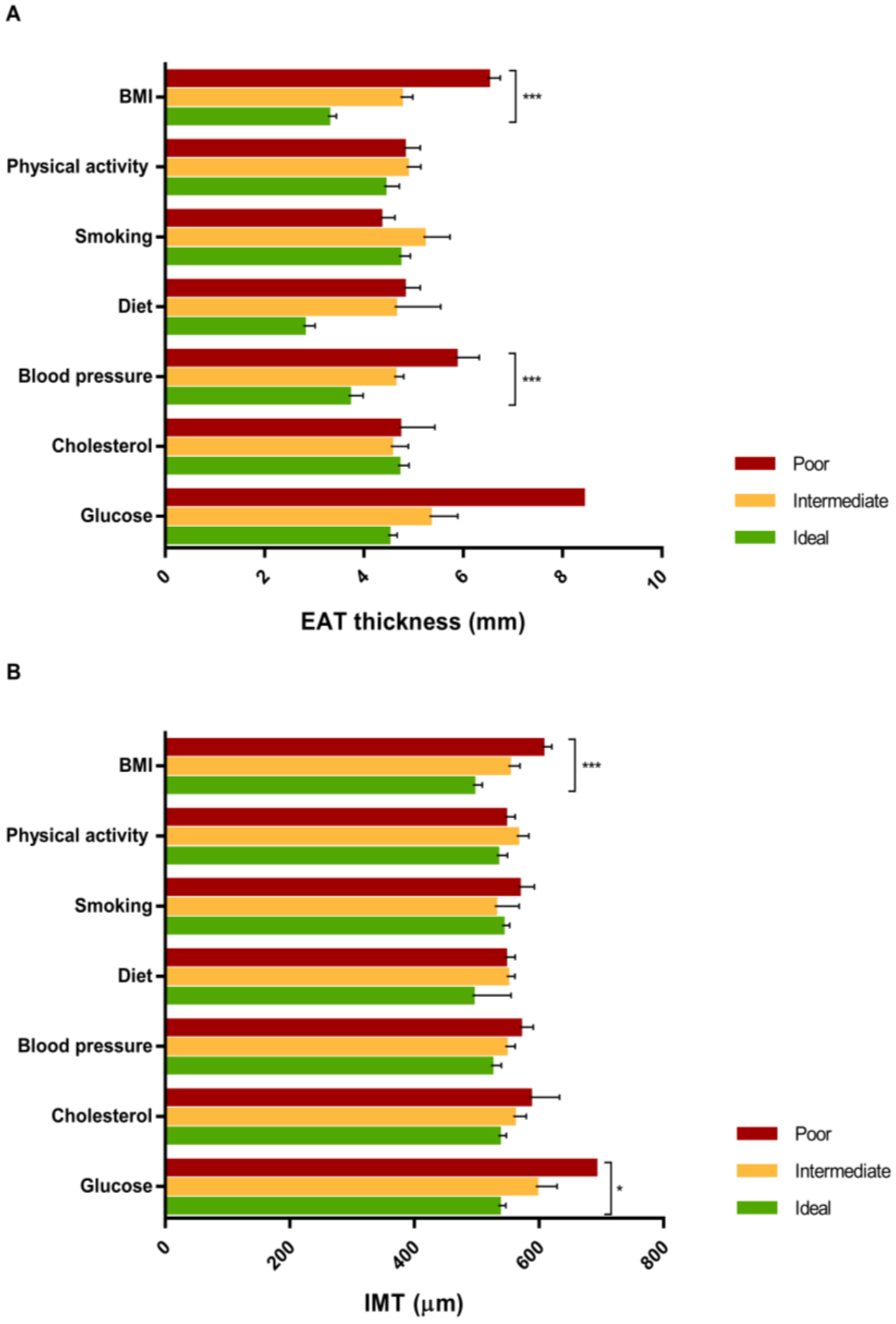
3.4. Associations of Anthropometric Measures and Cardiovascular Parameters with Epicardial Adipose Tissue (EAT) Thickness
3.5. Associations of Anthropometric Measures and Cardiovascular Parameters with Intima-Media Thickness (IMT)
3.6. The Association of Ideal Cardiovascular Health with EAT Thickness and IMT
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Acknowledgments
Conflicts of Interest
References
- Lloyd-Jones, D.M.; Hong, Y.; Labarthe, D.; Mozaffarian, D.; Appel, L.J.; Van Horn, L.; Greenlund, K.; Daniels, S.; Nichol, G.; Tomaselli, G.F.; et al. Defining and setting national goals for cardiovascular health promotion and disease reduction: The American Heart Association’s strategic Impact Goal through 2020 and beyond. Circulation 2010, 121, 586–613. [Google Scholar] [CrossRef] [PubMed]
- Stefan, N.; Schick, F.; Haring, H.U. Causes, Characteristics, and Consequences of Metabolically Unhealthy Normal Weight in Humans. Cell Metab. 2017, 26, 292–300. [Google Scholar] [CrossRef] [PubMed]
- Maffetone, P.B.; Rivera-Dominguez, I.; Laursen, P.B. Overfat Adults and Children in Developed Countries: The Public Health Importance of Identifying Excess Body Fat. Front. Public Health 2017, 5, 190. [Google Scholar] [CrossRef] [PubMed]
- Canoy, D.; Boekholdt, S.M.; Wareham, N.; Luben, R.; Welch, A.; Bingham, S.; Buchan, I.; Day, N.; Khaw, K.T. Body fat distribution and risk of coronary heart disease in men and women in the European Prospective Investigation Into Cancer and Nutrition in Norfolk cohort: A population-based prospective study. Circulation 2007, 116, 2933–2943. [Google Scholar] [CrossRef] [PubMed]
- Britton, K.A.; Fox, C.S. Ectopic fat depots and cardiovascular disease. Circulation 2011, 124, e837–e841. [Google Scholar] [CrossRef] [PubMed]
- Iacobellis, G. Local and systemic effects of the multifaceted epicardial adipose tissue depot. Nat. Rev. Endocrinol. 2015, 11, 363–371. [Google Scholar] [CrossRef] [PubMed]
- Wu, Y.; Zhang, A.; Hamilton, D.J.; Deng, T. Epicardial Fat in the Maintenance of Cardiovascular Health. Methodist DeBakey Cardiovasc. J. 2017, 13, 20–24. [Google Scholar] [CrossRef] [PubMed]
- De Matthaeis, A.; Greco, A.; Dagostino, M.P.; Paroni, G.; Fontana, A.; Vinciguerra, M.; Mazzoccoli, G.; Seripa, D.; Vendemiale, G. Effects of hypercapnia on peripheral vascular reactivity in elderly patients with acute exacerbation of chronic obstructive pulmonary disease. Clin. Interv. Aging 2014, 9, 871–878. [Google Scholar] [PubMed]
- Plichart, M.; Celermajer, D.S.; Zureik, M.; Helmer, C.; Jouven, X.; Ritchie, K.; Tzourio, C.; Ducimetiere, P.; Empana, J.P. Carotid intima-media thickness in plaque-free site, carotid plaques and coronary heart disease risk prediction in older adults. The Three-City Study. Atherosclerosis 2011, 219, 917–924. [Google Scholar] [CrossRef] [PubMed]
- Polonsky, T.S.; Ning, H.; Daviglus, M.L.; Liu, K.; Burke, G.L.; Cushman, M.; Eng, J.; Folsom, A.R.; Lutsey, P.L.; Nettleton, J.A.; et al. Association of Cardiovascular Health With Subclinical Disease and Incident Events: The Multi-Ethnic Study of Atherosclerosis. J. Am. Heart Assoc. 2017, 6, e004894. [Google Scholar] [CrossRef] [PubMed]
- Abubakar, I.I.; Tillmann, T.; Banerjee, A. Global, regional, and national age-sex specific all-cause and cause-specific mortality for 240 causes of death, 1990–2013: A systematic analysis for the Global Burden of Disease Study. Lancet 2015, 385, 117–171. [Google Scholar]
- Fuster, V.; Kelly, B.B.; Vedanthan, R. Global cardiovascular health: Urgent need for an intersectoral approach. J. Am. Coll. Cardiol. 2011, 58, 1208–1210. [Google Scholar] [CrossRef] [PubMed]
- Movsisyan, N.K.; Vinciguerra, M.; Lopez-Jimenez, F.; Kunzova, S.; Homolka, M.; Jaresova, J.; Cifkova, R.; Sochor, O. Kardiovize Brno 2030, a prospective cardiovascular health study in Central Europe: Methods, baseline findings and future directions. Eur. J. Prev. Cardiol. 2018, 25, 54–64. [Google Scholar] [CrossRef] [PubMed]
- Harris, P.A.; Taylor, R.; Thielke, R.; Payne, J.; Gonzalez, N.; Conde, J.G. Research electronic data capture (REDCap)—A metadata-driven methodology and workflow process for providing translational research informatics support. J. Biomed. Inform. 2009, 42, 377–381. [Google Scholar] [CrossRef] [PubMed]
- Folsom, A.R.; Yatsuya, H.; Nettleton, J.A.; Lutsey, P.L.; Cushman, M.; Rosamond, W.D.; Investigators, A.S. Community prevalence of ideal cardiovascular health, by the American Heart Association definition, and relationship with cardiovascular disease incidence. J. Am. Coll. Cardiol. 2011, 57, 1690–1696. [Google Scholar] [CrossRef] [PubMed]
- Iacobellis, G.; Assael, F.; Ribaudo, M.C.; Zappaterreno, A.; Alessi, G.; Di Mario, U.; Leonetti, F. Epicardial fat from echocardiography: A new method for visceral adipose tissue prediction. Obes. Res. 2003, 11, 304–310. [Google Scholar] [CrossRef] [PubMed]
- Iacobellis, G.; Willens, H.J. Echocardiographic epicardial fat: A review of research and clinical applications. J. Am. Soc. Echocardiogr. Off. Publ. Am. Soc. Echocardiogr. 2009, 22, 1311–1319. [Google Scholar] [CrossRef] [PubMed]
- Iacobellis, G.; Ribaudo, M.C.; Assael, F.; Vecci, E.; Tiberti, C.; Zappaterreno, A.; Di Mario, U.; Leonetti, F. Echocardiographic epicardial adipose tissue is related to anthropometric and clinical parameters of metabolic syndrome: A new indicator of cardiovascular risk. J. Clin. Endocrinol. Metab. 2003, 88, 5163–5168. [Google Scholar] [CrossRef] [PubMed]
- Stein, J.H.; Korcarz, C.E.; Hurst, R.T.; Lonn, E.; Kendall, C.B.; Mohler, E.R.; Najjar, S.S.; Rembold, C.M.; Post, W.S. American Society of Echocardiography Carotid Intima-Media Thickness Task Force. Use of carotid ultrasound to identify subclinical vascular disease and evaluate cardiovascular disease risk: A consensus statement from the American Society of Echocardiography Carotid Intima-Media Thickness Task Force Endorsed by the Society for Vascular Medicine. J. Am. Soc. Echocardiogr. Off. Publ. Am. Soc. Echocardiogr. 2008, 21, 93–111. [Google Scholar]
- Nambi, V.; Chambless, L.; Folsom, A.R.; He, M.; Hu, Y.; Mosley, T.; Volcik, K.; Boerwinkle, E.; Ballantyne, C.M. Carotid intima-media thickness and presence or absence of plaque improves prediction of coronary heart disease risk: The ARIC (Atherosclerosis Risk In Communities) study. J. Am. Coll. Cardiol. 2010, 55, 1600–1607. [Google Scholar] [CrossRef] [PubMed]
- Devynck, M.A.; Simon, A.; Pernollet, M.G.; Chironi, G.; Gariepy, J.; Rendu, F.; Levenson, J. Plasma cGMP and large artery remodeling in asymptomatic men. Hypertension 2004, 44, 919–923. [Google Scholar] [CrossRef] [PubMed]
- Juonala, M.; Kahonen, M.; Laitinen, T.; Hutri-Kahonen, N.; Jokinen, E.; Taittonen, L.; Pietikainen, M.; Helenius, H.; Viikari, J.S.; Raitakari, O.T. Effect of age and sex on carotid intima-media thickness, elasticity and brachial endothelial function in healthy adults: The cardiovascular risk in Young Finns Study. Eur. Heart J. 2008, 29, 1198–1206. [Google Scholar] [CrossRef] [PubMed]
- Alexopoulos, N.; McLean, D.S.; Janik, M.; Arepalli, C.D.; Stillman, A.E.; Raggi, P. Epicardial adipose tissue and coronary artery plaque characteristics. Atherosclerosis 2010, 210, 150–154. [Google Scholar] [CrossRef] [PubMed]
- Rosito, G.A.; Massaro, J.M.; Hoffmann, U.; Ruberg, F.L.; Mahabadi, A.A.; Vasan, R.S.; O’Donnell, C.J.; Fox, C.S. Pericardial fat, visceral abdominal fat, cardiovascular disease risk factors, and vascular calcification in a community-based sample: The Framingham Heart Study. Circulation 2008, 117, 605–613. [Google Scholar] [CrossRef] [PubMed]
- Mahabadi, A.A.; Massaro, J.M.; Rosito, G.A.; Levy, D.; Murabito, J.M.; Wolf, P.A.; O’Donnell, C.J.; Fox, C.S.; Hoffmann, U. Association of pericardial fat, intrathoracic fat, and visceral abdominal fat with cardiovascular disease burden: The Framingham Heart Study. Eur. Heart J. 2009, 30, 850–856. [Google Scholar] [CrossRef] [PubMed]
- Eroglu, S.; Sade, L.E.; Yildirir, A.; Bal, U.; Ozbicer, S.; Ozgul, A.S.; Bozbas, H.; Aydinalp, A.; Muderrisoglu, H. Epicardial adipose tissue thickness by echocardiography is a marker for the presence and severity of coronary artery disease. Nutr. Metab. Cardiovasc. Dis. NMCD 2009, 19, 211–217. [Google Scholar] [CrossRef] [PubMed]
- Iacobellis, G.; Barbaro, G.; Gerstein, H.C. Relationship of epicardial fat thickness and fasting glucose. Int. J. Cardiol. 2008, 128, 424–426. [Google Scholar] [CrossRef] [PubMed]
- Iacobellis, G.; Gao, Y.J.; Sharma, A.M. Do cardiac and perivascular adipose tissue play a role in atherosclerosis? Curr. Diabetes Rep. 2008, 8, 20–24. [Google Scholar] [CrossRef]
- Lorenz, M.W.; Markus, H.S.; Bots, M.L.; Rosvall, M.; Sitzer, M. Prediction of clinical cardiovascular events with carotid intima-media thickness: A systematic review and meta-analysis. Circulation 2007, 115, 459–467. [Google Scholar] [CrossRef] [PubMed]
- Iacobellis, G.; Sharma, A.M.; Pellicelli, A.M.; Grisorio, B.; Barbarini, G.; Barbaro, G. Epicardial adipose tissue is related to carotid intima-media thickness and visceral adiposity in HIV-infected patients with highly active antiretroviral therapy-associated metabolic syndrome. Curr. HIV Res. 2007, 5, 275–279. [Google Scholar] [CrossRef] [PubMed]
- Iacobellis, G.; Willens, H.J.; Barbaro, G.; Sharma, A.M. Threshold values of high-risk echocardiographic epicardial fat thickness. Obesity 2008, 16, 887–892. [Google Scholar] [CrossRef] [PubMed]
- Machann, J.; Thamer, C.; Schnoedt, B.; Haap, M.; Haring, H.U.; Claussen, C.D.; Stumvoll, M.; Fritsche, A.; Schick, F. Standardized assessment of whole body adipose tissue topography by MRI. J. Magn. Reson. Imaging 2005, 21, 455–462. [Google Scholar] [CrossRef] [PubMed]
- Rabkin, S.W. The relationship between epicardial fat and indices of obesity and the metabolic syndrome: A systematic review and meta-analysis. Metab. Syndr. Relat. Disord. 2014, 12, 31–42. [Google Scholar] [CrossRef] [PubMed]
- Rabkin, S.W.; Campbell, H. Comparison of reducing epicardial fat by exercise, diet or bariatric surgery weight loss strategies: A systematic review and meta-analysis. Obes. Rev. Off. J. Int. Assoc. Study Obes. 2015, 16, 406–415. [Google Scholar] [CrossRef] [PubMed]
- Munoz, M.J.F.; Acevedo, L.B.; Perez, N.C.; Martinez, A.L.V.; Gutierrez, N.T.; Garcia, S.V.; Cruz, A.R.; Martinez, A.D.; Garcia, R.S.; Trevino, A.Z.; et al. Epicardial adipose tissue is associated with visceral fat, metabolic syndrome, and insulin resistance in menopausal women. Rev. Esp. Cardiol. 2014, 67, 436–441. [Google Scholar]
- Ye, Z.; Lu, H.; Su, Q.; Li, L. Association between body mass index (BMI) and carotid intima media thickness in patients with type 2 diabetes mellitus: Results from the PROLOGUE study. Oncotarget 2018, 9, s508–s523. [Google Scholar] [CrossRef]
- Kulshreshtha, A.; Goyal, A.; Veledar, E.; McClellan, W.; Judd, S.; Eufinger, S.C.; Bremner, J.D.; Goldberg, J.; Vaccarino, V. Association between ideal cardiovascular health and carotid intima-media thickness: A twin study. J. Am. Heart Assoc. 2014, 3, e000282. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Linear Regression Model | EAT Thickness | IMT | ||
|---|---|---|---|---|
| B (SE) | p-Value * | B (SE) | p-Value * | |
| BMI | 0.182 (0.082) | 0.030 | 0.081 (0.095) | 0.128 |
| Total fat | 0.007 (0.027) | 0.787 | 0.005 (0.027) | 0.678 |
| BSA | 0.184 (1.234) | 0.882 | 0.126 (1.229) | 0.691 |
| WHR | 0.897 (2.154) | 0.678 | 0.876 (2.100) | 0.531 |
| LDL cholesterol | 0.022 (0.178) | 0.901 | 0.008 (0.177) | 0.987 |
| HDL cholesterol | −0.144 (0.397) | 0.719 | −0.110 (0.394) | 0.697 |
| Triglycerides | −0.051 (0.264) | 0.849 | −0.020 (0.257) | 0.902 |
| Glycated hemoglobin | −0.024 (0.034) | 0.480 | −0.023 (0.033) | 0.415 |
| Systolic blood pressure | 0.031 (0.025) | 0.221 | - | - |
| Diastolic blood pressure | −0.028 (0.034) | 0.411 | - | - |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hruskova, J.; Maugeri, A.; Podroužková, H.; Štípalová, T.; Jakubík, J.; Barchitta, M.; Medina-Inojosa, J.R.; Homolka, M.; Agodi, A.; Kunzova, S.; et al. Association of Cardiovascular Health with Epicardial Adipose Tissue and Intima Media Thickness: The Kardiovize Study. J. Clin. Med. 2018, 7, 113. https://doi.org/10.3390/jcm7050113
Hruskova J, Maugeri A, Podroužková H, Štípalová T, Jakubík J, Barchitta M, Medina-Inojosa JR, Homolka M, Agodi A, Kunzova S, et al. Association of Cardiovascular Health with Epicardial Adipose Tissue and Intima Media Thickness: The Kardiovize Study. Journal of Clinical Medicine. 2018; 7(5):113. https://doi.org/10.3390/jcm7050113
Chicago/Turabian StyleHruskova, Jana, Andrea Maugeri, Helena Podroužková, Tatiana Štípalová, Juraj Jakubík, Martina Barchitta, Jose R. Medina-Inojosa, Martin Homolka, Antonella Agodi, Sarka Kunzova, and et al. 2018. "Association of Cardiovascular Health with Epicardial Adipose Tissue and Intima Media Thickness: The Kardiovize Study" Journal of Clinical Medicine 7, no. 5: 113. https://doi.org/10.3390/jcm7050113