Brace Treatment for Adolescent Idiopathic Scoliosis

Department of Orthopaedic Surgery, National Hospital Organization Miyazaki Higashi Hospital, Miyazaki 880-0911, Japan
J. Clin. Med. 2018, 7(6), 136; https://doi.org/10.3390/jcm7060136
Submission received: 29 April 2018
/
Revised: 23 May 2018
/
Accepted: 29 May 2018
/
Published: 4 June 2018
(This article belongs to the Special Issue Spinal Deformity)
Abstract
:In the past, numerous non-operative treatments for adolescent idiopathic scoliosis (AIS), including exercise, physical therapy, electrical stimulation, and brace treatment, have been tried to delay or prevent the curve progression. Of these, brace treatment is the only option that is widely accepted and has demonstrated the efficacy to alter the natural history of AIS. Recently, the importance of brace treatment for AIS has been increasing since the efficacy was objectively established by the BrAIST (Bracing in Adolescent Idiopathic Scoliosis Trial) study in 2013. This editorial article summarizes the current status of brace treatment in patients with AIS and discusses future prospects on the basis of our clinical experiences.
1. Introduction
Scoliosis is a lateral curvature of the spine measuring at least 10° on an X-ray as determined by the Cobb method. Structural scoliosis is characterized by vertebral and trunk rotation [1]. Untreated cases of adolescent idiopathic scoliosis (AIS) may progress, and severe cases are at an increased risk for various morbidity problems and mortality [2]. In numerous non-operative treatments for AIS, brace treatment is the only potentially effective method in preventing curve progression and the subsequent need for surgery [3]. Various types of braces have been invented and were practically used in the past. In this editorial article, the current status and future prospects of brace treatment in patients with AIS will be summarized and discussed.
2. Aim of Brace Treatment
The goal of brace treatment for AIS is to halt the progression of a curve and to improve cosmetic appearance in accordance with maintaining whole body alignment and balance during a period of growth. Efficacy of brace treatment in AIS has continued to be controversial, with some authors reporting control of curve progression with bracing and others reporting that bracing fails to alter the natural history [4]. However, this is no longer true as evidence from the BrAIST (Bracing in Adolescent Idiopathic Scoliosis Trial) study [3] has established the effectiveness of bracing as early, non-operative care, that can statistically reduce the number of patients with AIS that progress to high-risk curves and the threshold for surgery [5]. In this study, 242 AIS patients were assigned to bracing and observation. Patients in the bracing group were instructed to wear the brace for at least 18 h per day. The rate of treatment success (skeletal maturity without 50 degrees of curve progression) was 72% after bracing, as compared with 48% after observation in the primary analysis. With the results of the BrAIST multicenter National Institute of Health (NIH) trial, there is level I evidence to support the efficacy of brace treatment in AIS [6].
3. History of Brace Treatment
The history of brace treatment began in the 16th century when Paré advocated metal braces made by an armorer for scoliosis; however, these braces were not used generally [7]. Before this, traction was a popular technique for correcting spinal deformities since Hippocrates’ time. In 1946, Blount and Schmidt theoretically developed the Milwaukee brace (CTLSO: cervico-thoraco-lumbo-sacro orthosis) for postoperative poliomyelitis and subsequently adopted it for treatment of AIS [8]. After that, brace treatment became popular, and various different thoraco-lumbo-sacro orthoses (TLSOs) were designed and practically utilized in place of CTLSO, which has some shortcomings; such as conspicuous design, difficulty to wear, compression of the mandible, and so on.
4. Type of Brace
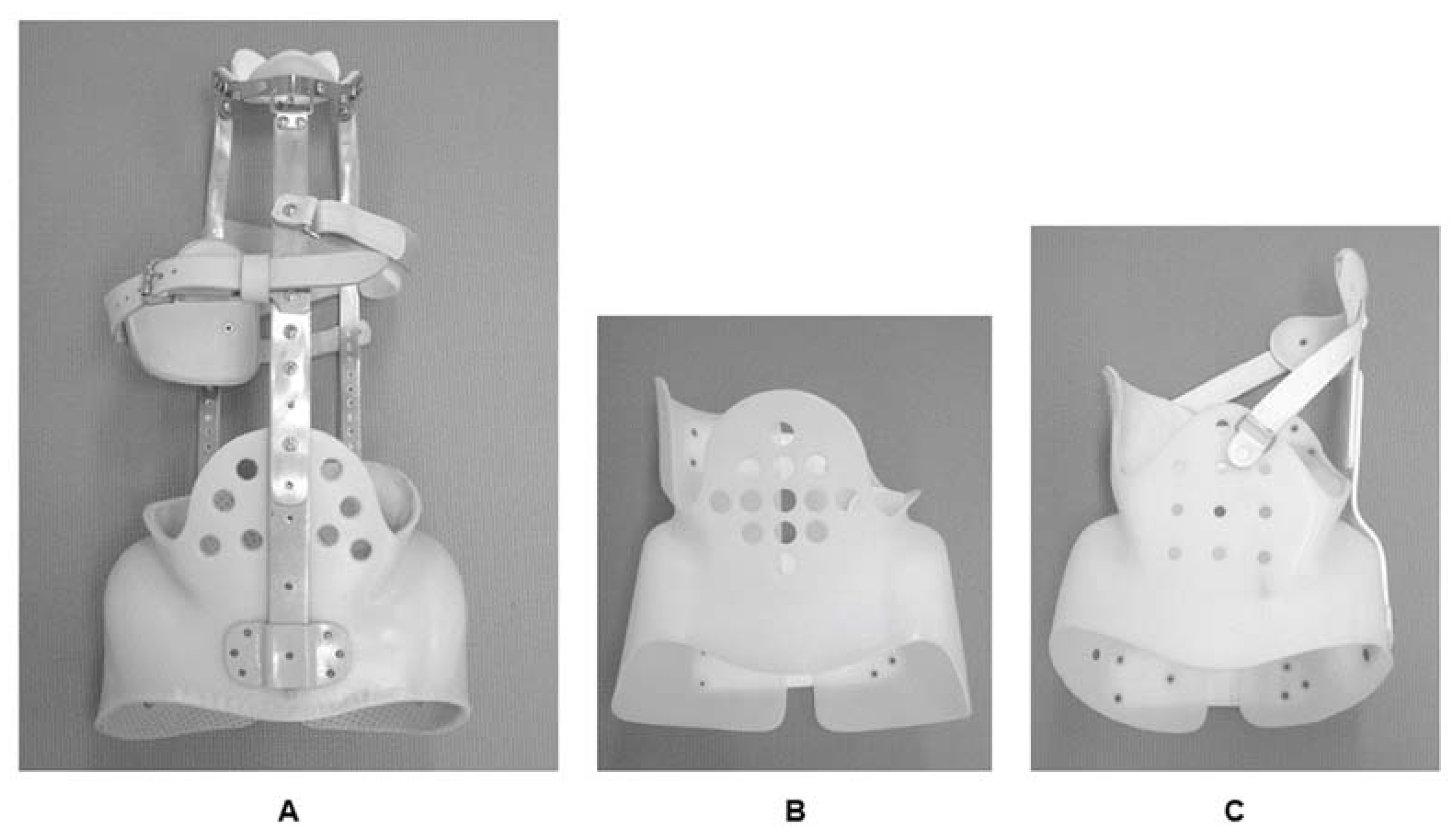
Braces employed for the treatment of spinal deformity are divided into CTLSO and TLSO. They are implemented depending on the location of curves, that is, the CTLSO is appropriate for the upper thoracic curve, where its apex is over T7 and would be difficult to correct using the TLSO. However, patient acceptance is poorer with CTLSO because of the visible neck ring [7]. The only CTLSO is the Milwaukee brace (Figure 1A). On the other hand, various different TLSOs have been manufactured around the world, for example: Boston (Figure 1B), Wilmington, Providence, and Rosenberg braces in North America, Chêneau and Sforzesco braces in Europe, and OMC (Osaka Medical College) brace (Figure 1C), CBH (Chiba brace high type), and TLSO Hiroshima in Japan. One of the specific TLSOs is the Charleston bending brace. This brace is worn on the inside of the bending position of the convex side during only sleeping hours as a night brace in expectation of excessive correction.
5. Theory of Curve Correction
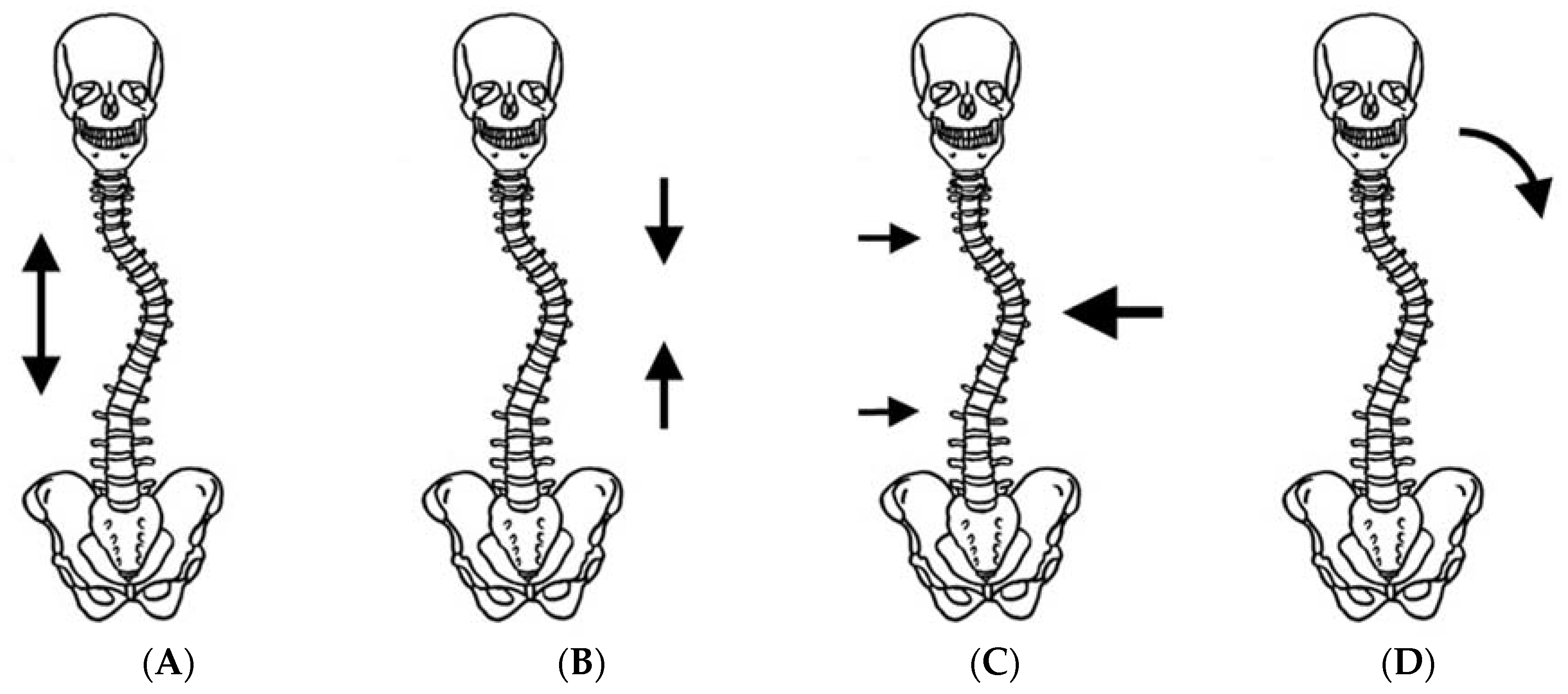
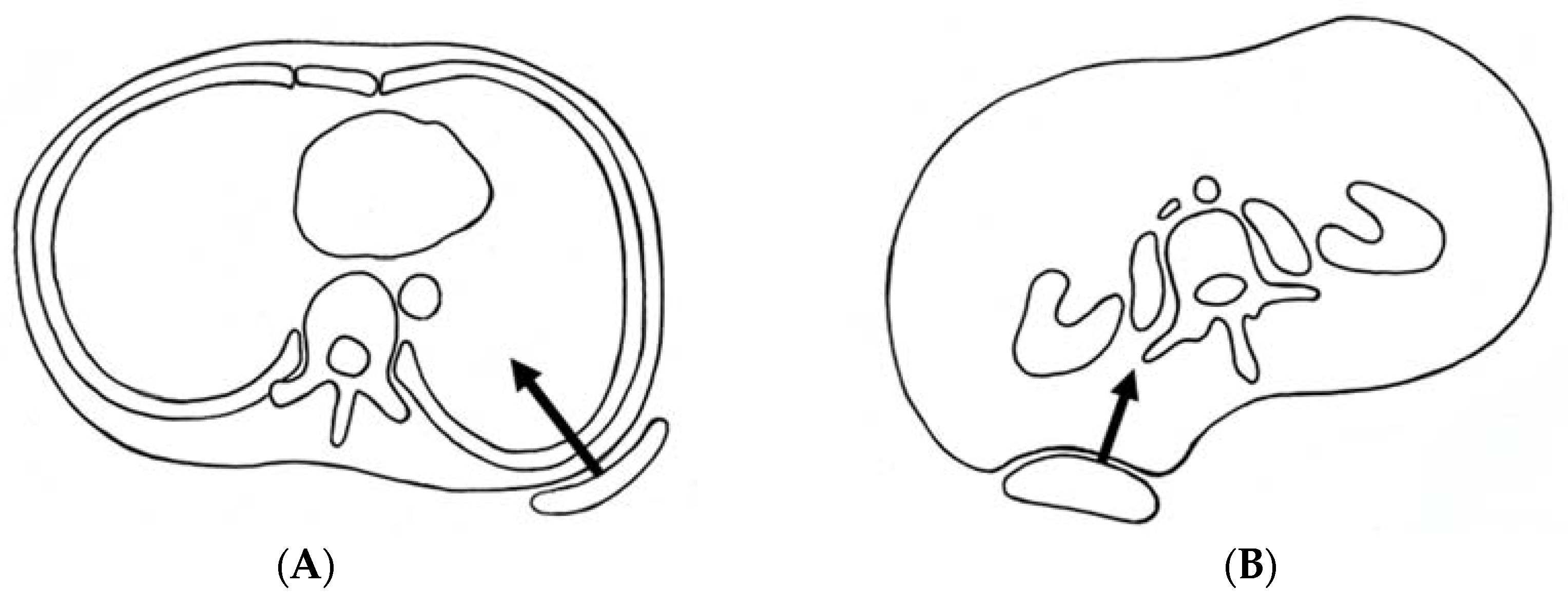
The main mechanical forces to correct spinal deformity consist of distraction forces on the concave side, compression forces on the convex side, transverse forces from both sides, and side bending for the convex side (Figure 2). Of these, longitudinal forces are most efficient for larger curves. However, transverse forces at the apex of the scoliotic curve are more efficient than longitudinal forces when correcting a spinal deformity of less than approximately 50°, which is the common indicator for brace treatment [9]. Basically, longitudinal forces cannot be applied for patients in TLSO. However, a biomechanical study proved that 2.5 times (about 5 kg) longitudinal forces could be created by CTLSO in the recumbent position compared with an upright position [10]. Only CTLSO can control the upper thoracic curve at its apex when over T7. Whereas, the active correction of the upper thoracic curve by righting reflex may be expected with TLSO. The position of the pads is also very important to properly correct spinal deformity, especially in cases with over a 40° curvature, because deformity of the thoracic cage may deteriorate from compression forces. In such cases, angles between the vertebral column and the ribs at the apex are ordinarily acute. If the thoracic pad comes closer to the midline, the anterior force is increased, and it will facilitate thoracic hypokyphosis that originally exists in AIS. If the thoracic pad is in a lateral position, the straight lateral force may further rotate the spine in an undesirable direction. Therefore, the location of the pad should be adjusted meticulously to provide optimal anterior and transverse forces in the thoracic spine (Figure 3A). Similarly, in the lumbar spine, the lumbar pad should be located at the level of the apex to push the transverse process from the posterolateral direction and create bending and derotational forces (Figure 3B). To do so, reduction of lumbar lordosis in brace wear is absolutely required.
6. Complications
There exist some potential complications and problems in brace treatment. They consist of two major elements, that is, physical changes by compression of the body and psychological disturbance by the appearance of wearing a brace. The onset of a pressure sore, skin color change, and cutaneous nerve involvement are common side effects in most patients during brace treatment. Prolonged TLSO wearing may produce a tubular thorax deformity [7]. The temporomandibular joint disorder by the mandibular pad was a serious issue of the original Milwaukee brace. Reflex esophagitis due to increased intragastric pressure; decrease in glomerular filtration rate and total lung capacity has also been noted [7]. These physical changes by compression of the body trunk can be mostly controlled by meticulous modifications of the brace and skin hygiene. Whereas, management of psychological disturbance by the appearance of brace wearing is extremely difficult. Matsunaga et al. [11] reported that the rate of patients with psychological problems increased from 7.6% to 82.1% one month after the start of brace treatment. MacLean et al. [12] mentioned the psychological effects of brace treatment for, not only the patients themselves, but also their parents.
It is important to provide the patients, their parents, and nursing teachers with a better understanding of the significance of brace treatment. Further, it is needless to say that the emotional stress during brace treatment should be relieved as much as possible by mental support for the patients with brace treatment with frequent and periodic consultation.
7. Brace Management Protocol
We usually use the OMC brace for the treatment of AIS. The OMC brace is one of the popular custom-made TLSOs in Japan and was developed by Onomura in the 1970s [13]. The characteristics of the OMC brace are represented by its inconspicuous design, lightweight, reduction of restriction on chest wall movement, and ability to correct the high thoracic curve by righting reflex [13]. The concept of this brace is the maintenance of the whole body alignment and balance. For the achievement of these goals, step-by-step molding from pelvic girdle to high thoracic level with correcting lumbar and main thoracic curves is important to generate desirable mechanical force based on the principle of three points lateral compression.
We prescribe the OMC brace to patients who meet certain requirements as follows; still growing, a Cobb angle of between 25 and 50°, and an apex of caudad to T7, with the expectation to halt the progression of the curve and to improve cosmetic appearance. However, we have practically recommended brace treatment for immature (premenarche) AIS patients with Cobb angle of between 20 and 25° in accordance with the principles of Weinstein et al. [14].
All OMC braces were fabricated by the certified orthotist. Each OMC brace was customized for the patient from a molding box, which was directly created relative to each patient’s body. The appropriate application and fit of the brace was confirmed to ensure an accurate reflection bringing forces that were employed to reduce the size of the curve in each patient. In addition, standing anteroposterior and lateral spine X-rays were used to document the amount of curve correction and maintenance of the preferable spinal alignment while the brace was being worn. It is indisputable that extra consideration should be given to brace wear comfort and secure decompression of the bone prominences.
Patients were instructed to wear the brace for a minimum of 20 h per day at the beginning of brace treatment. We periodically followed up with patients every three to eight months depending on the maturity of the patient, to document any adverse events during brace treatment (posture, skin trouble, breakage of brace) in addition to brace wear compliance (actual brace wear time). When skeletal maturity was noted, that is, all of the following three criteria were fulfilled; a Risser stage of four, at least two years passed since the onset of menstruation (for girls), two consecutive visits over a time period of at least one year with no more than a 1-cm increase in height, brace weaning was started and advanced step by step during one year. Then, the patients were weaned off the brace a year after skeletal maturity. During brace treatment, we always spent substantial time trying to recognize the patients that brace treatment was effective but required daily effort for long periods of time.
We found that compliance of brace wearing had a tendency to diminish with time, especially in periods when changes in environment, such as the time proceeding the next stage of the education process, as an example [15]. Therefore, encouragement of patients at this period is important to maintain brace wearing as scheduled.
The response of scoliotic deformity to initial brace wearing is essential to determine positive outcomes of brace treatment. The initial in-brace corrections are commonly different among patients due to spinal flexibility and curve patterns. Until now, various types of stress radiographs to evaluate spinal flexibility in patients with AIS have been reported; supine position, prone position, and lateral bending position. We evaluated the flexibility of the spine in patients with AIS by hanging total spine X-ray before the OMC brace treatment and assess if an appropriate correction by brace is achieved (Figure 4) [16]. This radiograph is easily taken in the outpatient clinic without any expensive equipment, extra-time, and extra-workforce. Cobb angles in hanging position were closely correlated with those on initial brace wearing, independent of curve patterns, except some curves in multiple curve patterns, and were useful for the confirmation of adequate correction by the brace. We basically aim smaller Cobb angles on initial brace wear than those in hanging position, particularly in immature patients.
8. Clinical Results of Brace Treatment (under SRS Criteria)
The efficacy of brace treatment for AIS continues to be controversial by reasons of the lack of consistency of both the inclusion criteria of subjects and the definition of brace effectiveness. To make the comparison among studies more valid and reliable, the Scoliosis Research Society (SRS) has standardized criteria for brace studies in patients with AIS. The SRS criteria consist of; age is 10 years or older when the brace is prescribed, Risser 0–2, primary curve angles 25–40°, no prior treatment, and if female, either premenarche or less than one year postmenarchal [17].
We previously attempted the clinical study to evaluate the efficacy of OMC brace for AIS in accordance with the modified SRS criteria (immature AIS patients who have a progressive curve from 20 to 24° were included as subjects) and compared our results with other previous reports.
In our previous study [18], 67.7% of patients achieved curve progression of less than 6° at skeletal maturity. Further, only 9.7% of patients reached Cobb angle of more than 45° which meant surgical indication. These results verified that OMC brace treatment could change the natural history of AIS just like other TLSOs [3,14,18,19,20,21,22,23,24,25,26] (Table 1). With regard to the ability of curve correction, the average initial in-brace correction of the OMC brace was 46.8%. This was inferior to the Charleston bending brace but almost the same as the other TLSOs [18,26,27,28,29,30,31,32,33,34,35,36,37] (Table 2). As previously mentioned, although the OMC brace is a TLSO, correction and controlling of the upper thoracic curve in double thoracic scoliosis could be achieved by utilizing the righting reflex that was generated by the active bending for the high thoracic curve under bracing [13].
9. Future Prospects
Our clinical experiences identified that maintenance of compliance, avoidance of dropout, and support for emotional burden were essential factors during brace treatments. In particular, maintenance of compliance was directly associated with clinical results. However, in brace treatment, there exists an inevitable issue of over-treatment for AIS patients, who may be free from the possibility of progress. Recently, prediction of curve progression has been made possible by the advancement of genetic testing [38,39]. Bohl et al. [40] reported that a genetic test with Scoliscore could anticipate Providence brace success. This problem may be solved by categorizing AIS patients according to the level of potential for deterioration, utilizing genetic diagnosis, so that the most appropriate treatment can be provided to each AIS patient.
10. Summary
Brace treatment is indispensable for AIS management as conservative care because it can alter the natural history of AIS and significantly decrease the progression of curve in skeletally-immature patients. However, it is not easy to smoothly accomplish brace treatment, since brace wearing must be, not only physically, but also emotionally, burdensome for adolescent patients. In the future, not only the development or improvement of more effective braces, and reinforcement of patient support, but also the introduction of a tailor-made treatment in which each patient can utilize genetic diagnosis and are expected to maintain motivation for brace wearing and to avoid dropouts relative to treatment success.
Conflicts of Interest
The author declares no conflicts of interest.
References
- Bunnell, W.P. Selective screening for scoliosis. Clin. Orthop. Relat. Res. 2005, 434, 40–45. [Google Scholar] [CrossRef]
- Fong, D.Y.T.; Lee, C.F.; Cheung, K.M.C.; Cheng, J.C.Y.; Ng, B.K.W.; Lam, T.P.; Mak, K.H.; Yip, P.S.F.; Luk, K.D.K. A meta-analysis of the clinical effectiveness of school scoliosis screening. Spine 2010, 35, 1061–1071. [Google Scholar] [CrossRef] [PubMed]
- Weinstein, S.L.; Dolan, L.A.; Wright, J.G.; Dobbs, M.B. Effects of bracing in adolescents with idiopathic scoliosis. N. Engl. J. Med. 2013, 369, 1512–1521. [Google Scholar] [CrossRef] [PubMed]
- Katz, D.E.; Herring, J.A.; Browne, R.H.; Kelly, D.M.; Birch, J.G. Brace wear control of curve progression in adolescent idiopathic scoliosis. J. Bone Jt. Surg. 2010, 92, 1343–1352. [Google Scholar] [CrossRef] [PubMed]
- Grivas, T.B.; Hresko, M.T.; Labelle, H.; Price, N.; Kotwicki, T.; Maruyama, T. The pendulum swings back to scoliosis screening: Screening policies for early detection and treatment of idiopathic scoliosis—Current concepts and recommendations. Scoliosis 2013, 8, 16. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Labelle, H.; Richards, B.S.; Kleuver, M.D.; Grivas, T.B.; Luk, K.D.K.; Wong, H.K.; Thometz, J.; Beauséjour, M.; Turgeon, I.; Fong, D.Y. Screening for adolescent idiopathic scoliosis: An information statement by the scoliosis research society international task force. Scoliosis 2013, 8, 17. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Oglivie, J.W. Historical aspect of scoliosis. In Moe’s Textbook of Scoliosis and Other Spinal Deformities, 3rd ed.; Lonstein, J.E., Bradford, D.S., Winter, R.B., Oglivie, J.W., Eds.; WB Saunders Company: Tokyo, Japan, 1994; pp. 1–5. [Google Scholar]
- Blount, W.P.; Schmidt, A.C.; Keever, E.D.; Leonard, E.T. The Milwaukee brace in the operative treatment of scoliosis. J. Bone Jt. Surg. 1958, 40, 511–525. [Google Scholar] [CrossRef]
- White, A.A.; Panjabi, M.M. Practical Biomechanics of Scoliosis and Kyphosis, Clinical Biomechanics of the Spine, 2nd ed.; Lippincott Williams & Wilkins: Philadelphia, PA, USA, 1990; pp. 127–168. [Google Scholar]
- Galante, J.; Schultz, A.; Dewald, R.L.; Ray, R.D. Forces acting in the Milwaukee brace on patients undergoing treatment for idiopathic scoliosis. J. Bone Jt. Surg. 1970, 52, 498–506. [Google Scholar] [CrossRef]
- Matsunaga, S.; Hayashi, K.; Naruo, T.; Nozoe, S.; Komiya, S. Psychologic management of brace therapy for patients with idiopathic scoliosis. Spine 2005, 30, 547–550. [Google Scholar] [CrossRef] [PubMed]
- MacLean, W.E.; Green, N.E.; Pierre, C.B.; Ray, D.C. Stress and coping with scoliosis: Psychological effects on adolescents and their families. J. Pediatr. Orthop. 1989, 9, 257–261. [Google Scholar] [CrossRef] [PubMed]
- Endo, O.; Onomura, T.; Yamamoto, S.; Yamaguchi, R.; Kato, M.; Watanabe, H.; Oota, K. Scoliosis treatment with the Osaka Medical College type brace (OMC-brace). In Seikeigeka Mook 18; Itami, Y., Nishio, A., Eds.; Kanehara syuppan Inc.: Tokyo, Japan, 1981; pp. 134–149, (In Japanese, the title is literally translated). [Google Scholar]
- Weinstein, S.L.; Dolan, L.A.; Wright, J.G.; Dobbs, M.B. Design of the bracing in adolescent idiopathic trial (BrAIST). Spine 2013, 38, 1832–1841. [Google Scholar] [CrossRef] [PubMed]
- Kuroki, H.; Kubo, S.; Chosa, E.; Tajima, N. Compliance of brace treatment for patients with idiopathic scoliosis. J. Jpn. Scoliosis Soc. 2007, 22, 42–46. (In Japanese) [Google Scholar]
- Kuroki, H.; Inomata, N.; Hamanaka, H.; Chosa, E.; Tajima, N. Significance of hanging total spine x-ray to estimate the indicative correction angle by brace wearing in idiopathic scoliosis patients. Scoliosis 2012, 7, 8. [Google Scholar] [CrossRef] [PubMed]
- Richards, B.S.; Bernstein, R.M.; D’Amato, C.R.; Thompson, G.H. Standardization of criteria for adolescent idiopathic scoliosis brace studies: SRS Committee on Bracing and Nonoperative Management. Spine 2005, 30, 2068–2075. [Google Scholar] [CrossRef] [PubMed]
- Kuroki, H.; Inomata, N.; Hamanaka, H.; Higa, K.; Chosa, E.; Tajima, N. Efficacy of the Osaka Medical College (OMC) brace in the treatment of adolescent idiopathic scoliosis following Scoliosis Research Society brace studies criteria. Scoliosis 2015, 10, 12. [Google Scholar] [CrossRef] [PubMed]
- Coillard, C.; Vachon, V.; Circo, A.B.; Beauséjour, M.; Rivard, C.H. Effectiveness of the SpineCor brace based on the new standardized criteria proposed by the Scoliosis Research Society for adolescent idiopathic scoliosis. J. Pediatr. Orthop. 2007, 27, 375–379. [Google Scholar] [CrossRef] [PubMed]
- Janicki, J.A.; Poe-Kochert, C.; Armstrong, D.G.; Thompson, G.H. A comparison of the thoracolumbosacral orthoses and Providence orthosis in the treatment of adolescent idiopathic scoliosis: Results using the new SRS inclusion and assessment criteria for bracing studies. J. Pediatr. Orthop. 2007, 27, 369–374. [Google Scholar] [CrossRef] [PubMed]
- Negrini, S.; Atanasio, S.; Fusco, C.; Zaina, F. Effectiveness of complete conservative treatment for adolescent idiopathic scoliosis (bracing and exercises) based on SOSORT management criteria: Results according to the SRS criteria for bracing studies—SOSORT award 2009 winner. Scoliosis 2009, 4, 19. [Google Scholar] [CrossRef] [PubMed]
- Aulisa, A.G.; Guzzanti, V.; Galli, M.; Perisano, C.; Falciglia, F.; Aulisa, L. Treatment of thoraco-lumbar curves in adolescent females affected by idiopathic scoliosis with a progressive action short brace (PASB): Assessment of results according to the SRS committee on bracing and nonoperative management standardization criteria. Scoliosis 2009, 4, 21. [Google Scholar] [CrossRef] [PubMed]
- Zaborowska-Sapeta, K.; Kowalski, I.M.; Kotwicki, T.; Protasiewicz-Faldowska, H.; Kiebzak, W. Effectiveness of Chêneau brace treatment for idiopathic scoliosis: Prospective study in 79 patients followed to skeletal maturity. Scoliosis 2011, 6, 2. [Google Scholar] [CrossRef] [PubMed]
- Lee, C.S.; Hwang, C.J.; Kim, D.J.; Kim, J.H.; Kim, Y.T.; Lee, M.Y.; Yoon, S.J.; Lee, D.H. Effectiveness of the Charleston night-time bending brace in the treatment of adolescent idiopathic scoliosis. J. Pediatr. Orthop. 2012, 32, 368–372. [Google Scholar] [CrossRef] [PubMed]
- Maruyama, T.; Yamada, H.; Kobayashi, Y.; Nakao, Y.; Sakai, H. Outcomes of Rigo-Chêneau type brace treatment for adolescent idiopathic scoliosis: Using the Scoliosis Research Society brace studies standardization protocol. J. Jpn. Orthop. Assoc. 2013, 87, S99. (In Japanese) [Google Scholar]
- Yamazaki, K.; Murakami, H.; Yoshida, S.; Kikuchi, T.; Shimamura, T. Outcome of brace treatment for adolescent idiopathic scoliosis. Orthop. Surg. 2013, 64, 806–811. (In Japanese) [Google Scholar]
- Watts, H.G.; Hall, J.E.; Stanish, W. The Boston brace system for the treatment of low thoracic and lumbar scoliosis by the use of a girdle without superstructure. Clin. Orthop. 1977, 126, 87–92. [Google Scholar] [CrossRef]
- Udén, A.; Willner, S.; Pettersson, H. Initial correction with the Boston thoracic brace. Acta Orthop. Scand. 1982, 53, 907–911. [Google Scholar] [CrossRef] [PubMed]
- Jonasson-Rajala, E.; Josefsson, E.; Lundberg, B.; Nilsson, H. Boston thoracic brace in the treatment of idiopathic scoliosis: Initial correction. Clin. Orthop. 1984, 183, 7–41. [Google Scholar] [CrossRef]
- Ohta, K.; Ikata, T.; Shinohara, K.; Teramae, T.; Nishioka, T.; Kasai, T. An active corrective brace for early idiopathic scoliosis. J. Jpn. Scoliosis Soc. 1988, 3, 196–199. (In Japanese) [Google Scholar]
- Kawakami, N.; Mimatsu, K.; Katoh, F.; Saito, H.; Satou, K.; Yagi, R. Evaluation of the Cobb angle and vertebral rotation in brace treatment of idiopathic scoliosis. J. Jpn. Scoliosis Soc. 1991, 6, 31–34. (In Japanese) [Google Scholar]
- Asazuma, T.; Suzuki, N.; Ono, T.; Tezuka, M.; Hijikata, S.; Hirabayashi, K. Follow-up study of under-arm brace treatment to adolescent idiopathic scoliosis. J. Jpn. Scoliosis Soc. 1991, 6, 22–26. (In Japanese) [Google Scholar]
- Arai, S.; Ootsuka, Y.; Kitahara, H.; Minami, S.; Moriya, H.; Nakata, Y.; Matsumoto, T. Brace treatment for idiopathic scoliosis: Followed over 10 years. J. Jpn. Scoliosis Soc. 1992, 7, 83–87. (In Japanese) [Google Scholar]
- Iwaya, D.; Ohtake, S.; Harata, S.; Ueyama, K.; Itoh, J.; Nitobe, T. Treatment for idiopathic scoliosis with Charleston bending brace: Preliminary study. J. Jpn. Scoliosis Soc. 1997, 12, 30–33. (In Japanese) [Google Scholar]
- Semoto, Y.; Kosaka, R.; Yamada, M.; Abe, M. Osaka medical college type brace for idiopathic scoliosis. J. Jpn. Orthop. Assoc. 1999, 73, S146. (In Japanese) [Google Scholar]
- Spoonamore, M.J.; Dolan, L.A.; Weinstein, S.L. Use of the Rosenberger brace in the treatment of progressive adolescent idiopathic scoliosis. Spine 2004, 29, 1458–1464. [Google Scholar] [CrossRef] [PubMed]
- D’Amato, C.R.; Griggs, S.; McCoy, B. Nighttime bracing with the Providence brace in adolescent girls with idiopathic scoliosis. Spine 2001, 26, 2006–2012. [Google Scholar] [CrossRef] [PubMed]
- Ward, K.; Ogilvie, J.W.; Singleton, M.V.; Chettier, R.; Engler, G.; Nelson, L.M. Validation of DNA-based prognostic testing to predict spinal curve progression in adolescent idiopathic scoliosis. Spine 2010, 35, E1455–E1464. [Google Scholar] [CrossRef] [PubMed]
- Roye, B.D.; Wright, M.L.; Williams, B.A.; Matsumoto, H.; Corona, J.; Hyman, J.E.; Roye, D.P., Jr.; Vitale, M.G. Does ScoliScore provide more information than traditional clinical estimates of curve progression? Spine 2012, 37, 2099–2103. [Google Scholar] [CrossRef] [PubMed]
- Bohl, D.D.; Telles, C.J.; Ruiz, F.K.; Badrinath, R.; DeLuca, P.A.; Grauer, J.N. A genetic test predicts Providence brace success for adolescent idiopathic scoliosis when failure is defined as progression to greater than 45 degrees. Clin. Spine Surg. 2016, 29, E146–E150. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Various types of brace. (A) CTLSO (Milwaukee brace); (B) TLSO (Boston brace); (C) TLSO (Osaka Medical College: OMC brace).
Figure 1.
Various types of brace. (A) CTLSO (Milwaukee brace); (B) TLSO (Boston brace); (C) TLSO (Osaka Medical College: OMC brace).

Figure 2.
Mechanical forces to correct spinal deformity. (A) Distraction force; (B) compression force; (C) transverse force; and (D) bending force.
Figure 2.
Mechanical forces to correct spinal deformity. (A) Distraction force; (B) compression force; (C) transverse force; and (D) bending force.

Figure 3.
Optimal position of pads to add proper mechanical forces. (A) Thoracic spine; (B) lumbar spine.
Figure 3.
Optimal position of pads to add proper mechanical forces. (A) Thoracic spine; (B) lumbar spine.

Figure 4.
Position of hanging total spine X-ray. Hanging total spine X-ray was taken in a position that the patient is hanging onto the bar, stretching the back, and touching the toes lightly to the floor, not to sway the body under the instruction of making a great effort to stretch their back as much as possible [16] (licensed under CC BY).
Figure 4.
Position of hanging total spine X-ray. Hanging total spine X-ray was taken in a position that the patient is hanging onto the bar, stretching the back, and touching the toes lightly to the floor, not to sway the body under the instruction of making a great effort to stretch their back as much as possible [16] (licensed under CC BY).


{kind=link}
{kind=link}
{kind=link}
{kind=link}
Table 1.
Literature review of the clinical results under SRS criteria.
| Author (Year) | Treatment Period | Type of Brace | Success Rate | Progression Rate for Surgical Indication |
|---|---|---|---|---|
| Coillard C et al. (2007) [19] | ? | SpineCor Brace | 89.4% ** | 24.1% † |
| Janicki JA et al. (2007) [20] | 1y5m | TLSO | 85.4% * | 62.4% † |
| 1y4m | Providence | 68.6% * | 42.9% † | |
| Negrini S et al. (2009) [21] | 4y2m | Lyon, SPoRT | 95.8% ** | 0.0% † |
| Aulisa AG et al. (2009) [12] | 4y11m | Progressive Action Short Brace | 100% * | 0.0% † |
| Zaborowaka-Sapeta K et al. (2011) [23] | 2y8m | Chêneau brace | 48.1% * | 12.7% ‡ |
| Lee CS et al. (2012) [24] | 2y9m | Charleston Bending Brace | 84.2% ** | 12.6% † |
| Weinstein SL et al. (2013) [3,14] | ? | TLSO | — | 28.1% ‡ |
| Maruyama T et al. (2013) [25] | 1y9m | Rigo-Chêneau brace | 70.8% ** | 18.2% † |
| Yamazaki K et al. (2013) [26] | 6y5m | Under Arm Brace | 59% ** | 13.6% † |
| Kuroki H et al. (2015) [18] | 3y4m | Osaka Medical College Brace | 67.7% ** | 9.7% † |
y, year; m, month; ?, unknown; * Progress < 5°; ** Progression < 6°; † Progression ≥ 45°; ‡ Progression ≥ 50°.
Table 2.
Literature review of the initial correction rate.
| Author (Year) | Apex | Type of Brace | Correction Rate |
|---|---|---|---|
| Watts HG et al. (1977) [27] | below T10 | Boston Brace | 54.7% |
| Uden A et al. (1982) [28] | below T7 | Boston Brace | 41.0% |
| Milwaukee Brace | 10.0% | ||
| Jonasson-Rajala E et al. (1984) [29] | below T8 | Boston Thoracic Brace | 46.2% |
| Boston Milwaukee Brace | 29.3% | ||
| Boston Brace | 36.9% | ||
| Ohta K et al. (1988) [30] | — | Active Corrective Brace | 53.8% |
| Kawakami N et al. (1991) [31] | — | Active Corrective Brace | 17.6% |
| Asazuma T et al. (1991) [32] | below T7 | Under Arm Brace | 23.0% * |
| Arai S et al. (1992) [33] | — | Milwaukee Brace | 44.2% * |
| Iwaya D et al. (1997) [34] | below T7 | Charleston Bending Brace | 75.0% |
| Semoto Y et al. (1999) [35] | below T7 | OMC Brace | 35.5% |
| Spoonamore MJ et al. (2001) [36] | — | Rosenberger Brace | 30.0% |
| D’Amato CR et al. (2004) [37] | — | Providence Brace | 96.0% |
| Yamazaka K et al. (2013) [26] | — | Under Arm Brace | 38.7% |
| Kuroki H et al. (2015) [18] | below T8 | OMC Brace | 46.8% |
* Maximum Correction Rate.
© 2018 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Kuroki, H. Brace Treatment for Adolescent Idiopathic Scoliosis. J. Clin. Med. 2018, 7, 136. https://doi.org/10.3390/jcm7060136
AMA Style
Kuroki H. Brace Treatment for Adolescent Idiopathic Scoliosis. Journal of Clinical Medicine. 2018; 7(6):136. https://doi.org/10.3390/jcm7060136
Chicago/Turabian StyleKuroki, Hiroshi. 2018. "Brace Treatment for Adolescent Idiopathic Scoliosis" Journal of Clinical Medicine 7, no. 6: 136. https://doi.org/10.3390/jcm7060136
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.