The High-Sensitivity C-Reactive Protein/Albumin Ratio Predicts Long-Term Oncologic Outcomes after Curative Resection for Hepatocellular Carcinoma

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Surgical Management for Hepatocellular Carcinoma at SNUBH
2.3. Measurements and Outcomes
2.4. Statistical Analysis
3. Results
3.1. Cut-Off Value for hsCRP/Albumin Ratio
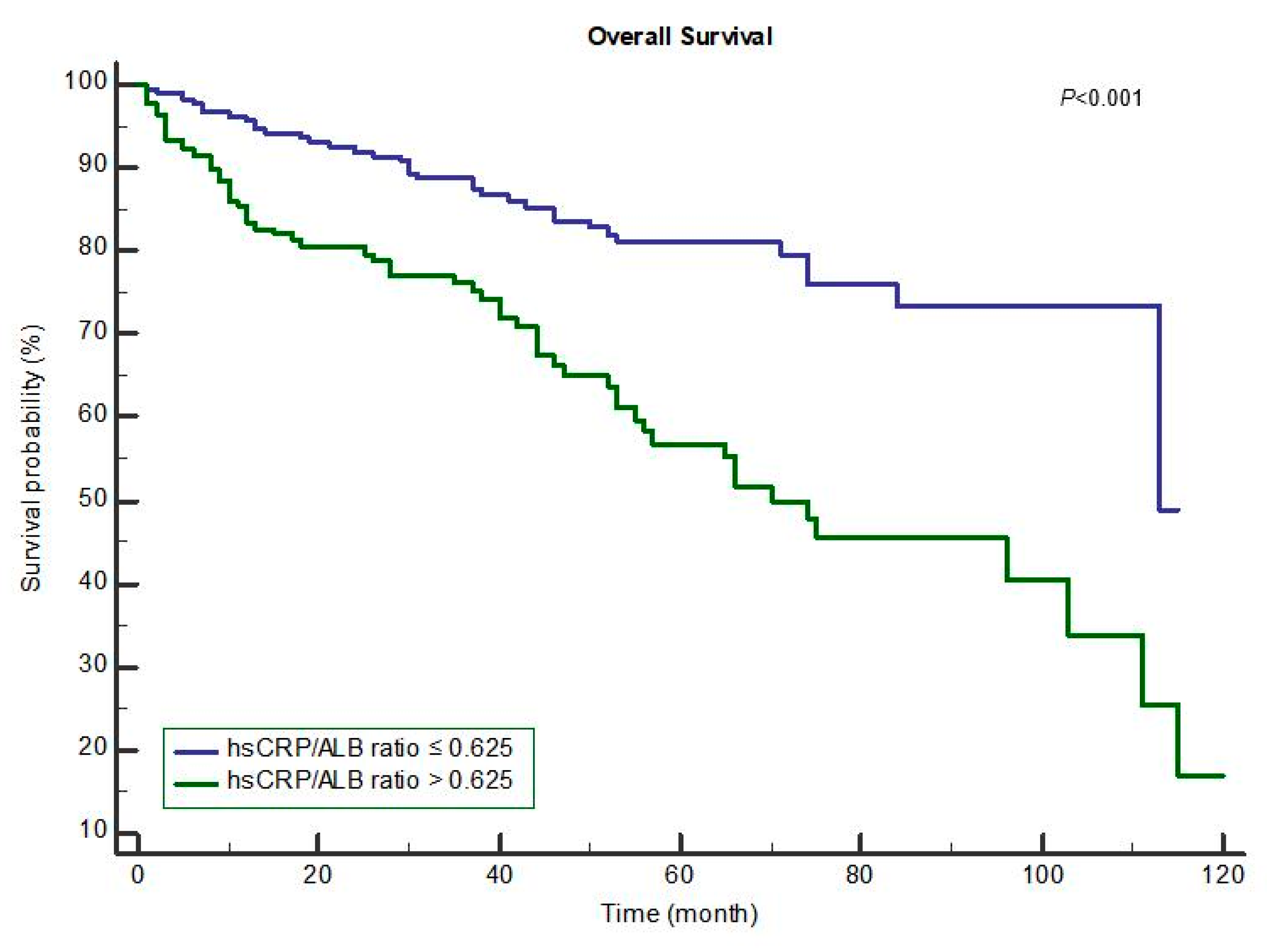
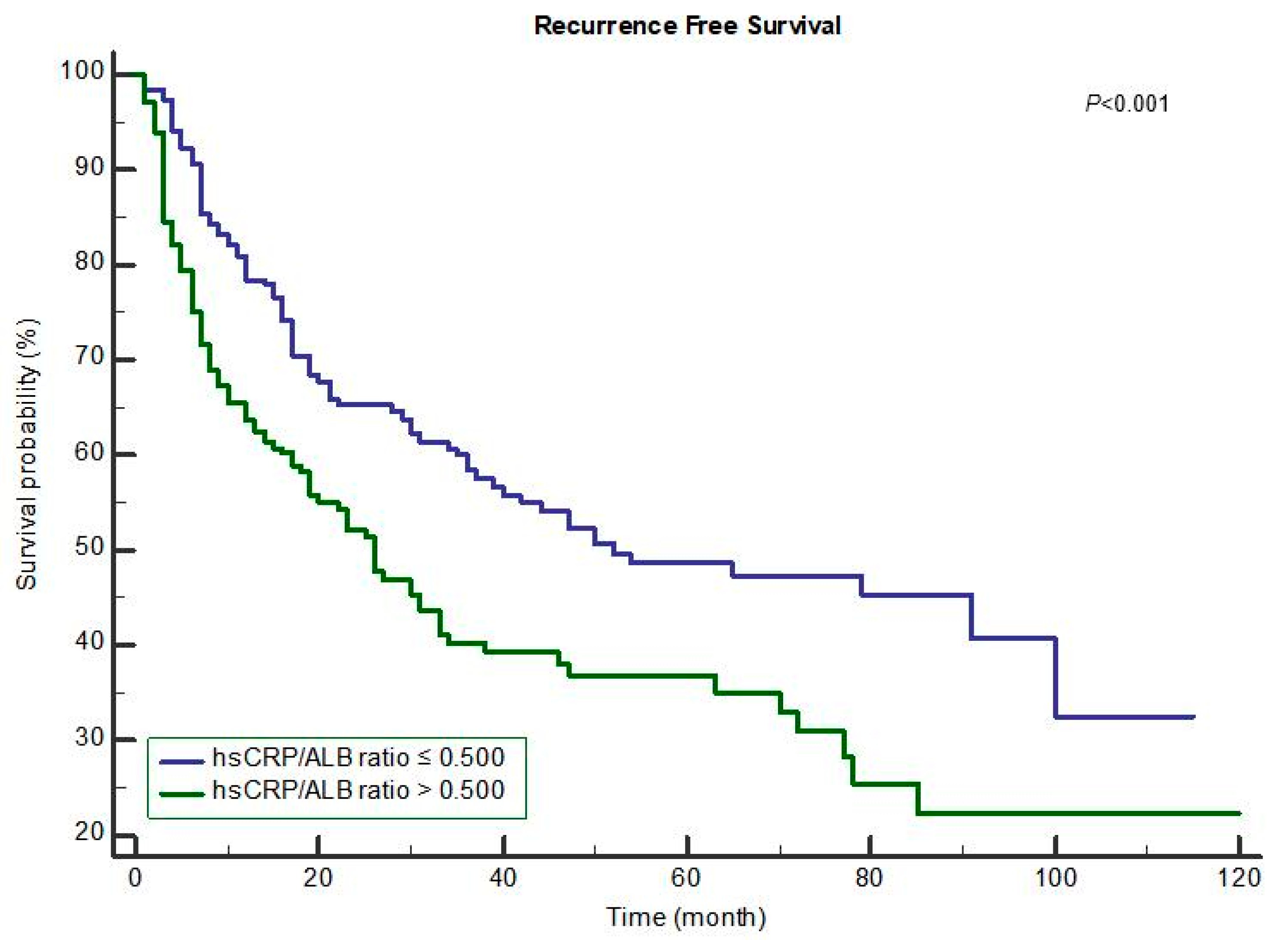
3.2. Overall Survival and Recurrence-Free Survival after HCC Surgery
3.3. Subgroup Analysis: Laparoscopy versus Laparotomy for hsCRP/Albumin Ratio
4. Discussion
Supplementary Materials
Author Contributions
Conflicts of Interest
References
- White, D.L.; Kanwal, F.; Jiao, L.; El-Serag, H.B. Epidemiology of hepatocellular carcinoma. In Hepatocellular Carcinoma; Springer: Berlin, Germany, 2016; pp. 3–24. [Google Scholar]
- Dhir, M.; Melin, A.A.; Douaiher, J.; Lin, C.; Zhen, W.K.; Hussain, S.M.; Geschwind, J.F.; Doyle, M.B.; Abou-Alfa, G.K.; Are, C. A review and update of treatment options and controversies in the management of hepatocellular carcinoma. Ann. Surg. 2016, 263, 1112–1125. [Google Scholar] [CrossRef] [PubMed]
- Forner, A.; Reig, M.E.; de Lope, C.R.; Bruix, J. Current strategy for staging and treatment: The BCLC update and future prospects. Semin. Liver Dis. 2010, 30, 61–74. [Google Scholar] [CrossRef] [PubMed]
- Kokudo, N.; Hasegawa, K.; Akahane, M.; Igaki, H.; Izumi, N.; Ichida, T.; Uemoto, S.; Kaneko, S.; Kawasaki, S.; Ku, Y.; et al. Evidence-based clinical practice guidelines for hepatocellular carcinoma: The japan society of hepatology 2013 update (3rd JSH-HCC guidelines). Hepatol. Res. 2015, 45. [Google Scholar] [CrossRef] [PubMed]
- Ettorre, G.M.; Levi Sandri, G.B.; Colasanti, M.; Masciana, G.; de Werra, E.; Santoro, R.; Lepiane, P.; Montalbano, M.; Antonini, M.; Vennarecci, G. Liver resection for hepatocellular carcinoma >/=5 cm. Transl. Gastroenterol. Hepatol. 2017, 2, 22. [Google Scholar] [CrossRef] [PubMed]
- Pamecha, V.; Sasturkar, S.V.; Sinha, P.K.; Mahansaria, S.S.; Bharathy, K.G.S.; Kumar, S.; Rastogi, A. Major liver resection for large and locally advanced hepatocellular carcinoma. Indian J. Surg. 2017, 79, 326–331. [Google Scholar] [CrossRef] [PubMed]
- Yang, H.; Xiong, F.; Qi, R.; Liu, Z.; Lin, M.; Rui, J.; Su, J.; Zhou, R. Laptm4b-35 is a novel prognostic factor of hepatocellular carcinoma. J. Surg. Oncol. 2010, 101, 363–369. [Google Scholar] [CrossRef] [PubMed]
- Poon, R.T.; Fan, S.T.; Lo, C.M.; Liu, C.L.; Wong, J. Long-term survival and pattern of recurrence after resection of small hepatocellular carcinoma in patients with preserved liver function: Implications for a strategy of salvage transplantation. Ann. Surg. 2002, 235, 373–382. [Google Scholar] [CrossRef] [PubMed]
- Casadei Gardini, A.; Carloni, S.; Scarpi, E.; Maltoni, P.; Dorizzi, R.M.; Passardi, A.; Frassineti, G.L.; Cortesi, P.; Giannini, M.B.; Marisi, G.; et al. Prognostic role of serum concentrations of high-sensitivity c-reactive protein in patients with metastatic colorectal cancer: Results from the itaca trial. Oncotarget 2016, 7, 10193–10202. [Google Scholar] [PubMed]
- Ko, Y.J.; Kwon, Y.M.; Kim, K.H.; Choi, H.C.; Chun, S.H.; Yoon, H.J.; Goh, E.; Cho, B.; Park, M. High-sensitivity c-reactive protein levels and cancer mortality. Cancer Epidemiol. Biomark. Prev. 2012, 21, 2076–2086. [Google Scholar] [CrossRef] [PubMed]
- Caras, R.J.; Lustik, M.B.; Kern, S.Q.; McMann, L.P.; Sterbis, J.R. Preoperative albumin is predictive of early postoperative morbidity and mortality in common urologic oncologic surgeries. Clin. Genitourin Cancer 2017, 15, e255–e262. [Google Scholar] [CrossRef] [PubMed]
- Lin, M.Y.; Liu, W.Y.; Tolan, A.M.; Aboulian, A.; Petrie, B.A.; Stabile, B.E. Preoperative serum albumin but not prealbumin is an excellent predictor of postoperative complications and mortality in patients with gastrointestinal cancer. Am. Surg. 2011, 77, 1286–1289. [Google Scholar] [PubMed]
- Oh, J.; Kim, S.H.; Park, K.N.; Oh, S.H.; Kim, Y.M.; Kim, H.J.; Youn, C.S. High-sensitivity c-reactive protein/albumin ratio as a predictor of in-hospital mortality in older adults admitted to the emergency department. Clin. Exp. Emerg. Med. 2017, 4, 19–24. [Google Scholar] [CrossRef] [PubMed]
- Yang, C.; Yang, Y.; Li, B.; Xu, P.; Shen, Q.; Yang, Q. The diagnostic value of high-sensitivity c-reactive protein/albumin ratio in evaluating early-onset infection in premature. Zhonghua Wei Zhong Bing Ji Jiu Yi Xue 2016, 28, 173–177. [Google Scholar] [PubMed]
- Ma, L.N.; Liu, X.Y.; Lu, Z.H.; Wu, L.G.; Tang, Y.Y.; Luo, X.; Hu, Y.C.; Yan, T.T.; Wang, Q.; Ding, X.C.; et al. Assessment of high-sensitivity c-reactive protein tests for the diagnosis of hepatocellular carcinoma in patients with hepatitis b-associated liver cirrhosis. Oncol. Lett. 2017, 13, 3457–3464. [Google Scholar] [CrossRef] [PubMed]
- Nault, J.C.; Guyot, E.; Laguillier, C.; Chevret, S.; Ganne-Carrie, N.; N’Kontchou, G.; Beaugrand, M.; Seror, O.; Trinchet, J.C.; Coelho, J.; et al. Serum proteoglycans as prognostic biomarkers of hepatocellular carcinoma in patients with alcoholic cirrhosis. Cancer Epidemiol. Biomark. Prev. 2013, 22, 1343–1352. [Google Scholar] [CrossRef] [PubMed]
- Tateishi, R.; Shiina, S.; Yoshida, H.; Teratani, T.; Obi, S.; Yamashiki, N.; Yoshida, H.; Akamatsu, M.; Kawabe, T.; Omata, M. Prediction of recurrence of hepatocellular carcinoma after curative ablation using three tumor markers. Hepatology 2006, 44, 1518–1527. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fujiwara, N.; Tateishi, R.; Nakagawa, H.; Nakagomi, R.; Kondo, M.; Minami, T.; Sato, M.; Uchino, K.; Enooku, K.; Kondo, Y.; et al. Slight elevation of high-sensitivity c-reactive protein to predict recurrence and survival in patients with early stage hepatitis c-related hepatocellular carcinoma. Hepatol. Res. 2015, 45, 645–655. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.B.; Ying, J.; Kuang, S.J.; Jin, H.S.; Yin, Z.; Chang, L.; Yang, H.; Ou, Y.L.; Zheng, J.H.; Zhang, W.D.; et al. Elevated preoperative serum hs-crp level as a prognostic factor in patients who underwent resection for hepatocellular carcinoma. Medicine (Baltimore) 2015, 94, e2209. [Google Scholar] [CrossRef] [PubMed]
- Kinoshita, A.; Onoda, H.; Imai, N.; Iwaku, A.; Oishi, M.; Tanaka, K.; Fushiya, N.; Koike, K.; Nishino, H.; Matsushima, M. The c-reactive protein/albumin ratio, a novel inflammation-based prognostic score, predicts outcomes in patients with hepatocellular carcinoma. Ann. Surg. Oncol. 2015, 22, 803–810. [Google Scholar] [CrossRef] [PubMed]
- Han, H.S.; Shehta, A.; Ahn, S.; Yoon, Y.S.; Cho, J.Y.; Choi, Y. Laparoscopic versus open liver resection for hepatocellular carcinoma: Case-matched study with propensity score matching. J. Hepatol. 2015, 63, 643–650. [Google Scholar] [CrossRef] [PubMed]
- Yoon, Y.S.; Han, H.S.; Cho, J.Y.; Ahn, K.S. Total laparoscopic liver resection for hepatocellular carcinoma located in all segments of the liver. Surg. Endosc. 2010, 24, 1630–1637. [Google Scholar] [CrossRef] [PubMed]
- Goh, B.K.; Teo, J.Y.; Chan, C.Y.; Lee, S.Y.; Jeyaraj, P.; Cheow, P.C.; Chow, P.K.; Ooi, L.L.; Chung, A.Y. Importance of tumor size as a prognostic factor after partial liver resection for solitary hepatocellular carcinoma: Implications on the current ajcc staging system. J. Surg. Oncol. 2016, 113, 89–93. [Google Scholar] [CrossRef] [PubMed]
- Pang, R.W.; Poon, R.T. Diagnosis: Novel prognostic biomarkers in hepatocellular carcinoma. Nat. Rev. Gastroenterol. Hepatol. 2012, 9, 691–692. [Google Scholar] [CrossRef] [PubMed]
- Gabay, C.; Kushner, I. Acute-phase proteins and other systemic responses to inflammation. N. Engl. J. Med. 1999, 340, 448–454. [Google Scholar] [CrossRef] [PubMed]
- Hubner, M.; Mantziari, S.; Demartines, N.; Pralong, F.; Coti-Bertrand, P.; Schafer, M. Postoperative albumin drop is a marker for surgical stress and a predictor for clinical outcome: A pilot study. Gastroenterol. Res. Pract. 2016, 2016, 8743187. [Google Scholar] [CrossRef] [PubMed]
- Li, N.; Tian, G.W.; Wang, Y.; Zhang, H.; Wang, Z.H.; Li, G. Prognostic role of the pretreatment c-reactive protein/albumin ratio in solid cancers: A meta-analysis. Sci. Rep. 2017, 7, 41298. [Google Scholar] [CrossRef] [PubMed]
- Kim, M.H.; Ahn, J.Y.; Song, J.E.; Choi, H.; Ann, H.W.; Kim, J.K.; Kim, J.H.; Jeon, Y.D.; Kim, S.B.; Jeong, S.J.; et al. The c-reactive protein/albumin ratio as an independent predictor of mortality in patients with severe sepsis or septic shock treated with early goal-directed therapy. PLoS ONE 2015, 10, e0132109. [Google Scholar] [CrossRef] [PubMed]
- Ranzani, O.T.; Zampieri, F.G.; Forte, D.N.; Azevedo, L.C.; Park, M. C-reactive protein/albumin ratio predicts 90-day mortality of septic patients. PLoS ONE 2013, 8, e59321. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Variable | Total (389) | Mean | SD | |
|---|---|---|---|---|
| Sex: male | 299 (76.9%) | |||
| Age (year) | 58.30 | 11.73 | ||
| Body Mass Index (kg m−2) | 23.86 | 3.39 | ||
| Charson Comorbidity Index | 3.08 | 1.17 | ||
| ASA class | I | 103 (26.5%) | ||
| II | 255 (65.6%) | |||
| III + IV | 31 (8.0%) | |||
| Preoperative serum bilirubin (mg dl−1) | 0.90 | 0.64 | ||
| Preoperative aFP (IU mL−1) | 926.64 | 4111.91 | ||
| Preoperative PT INR | 1.35 | 5.07 | ||
| Preoperative ALT (U L−1) | 43.37 | 41.05 | ||
| Preoperative AST (U L−1) | 43.50 | 46.17 | ||
| Procedures | Laparotomy | 232 (59.6%) | ||
| Laparoscopy | 157 (40.4%) | |||
| Operation time (min) | 295.54 | 154.33 | ||
| Estimated Blood Loss (mL) | 1071.31 | 1844.42 | ||
| Preoperative TACE | 107 (27.5%) | |||
| Preoperative RFA | 26 (6.7%) | |||
| Preoperative Child pugh class | A | 341 (87.7%) | ||
| B | 35 (9.0%) | |||
| C | 13 (3.3%) | |||
| Virology | HCV (+) | 279 (71.7%) | ||
| HBV (+) | 27 (6.9%) | |||
| Both (+) | 1 (0.3%) | |||
| Both (−) | 82 (21.1%) | |||
| Intraoperative Transfusion | 106 (27.2%) | |||
| Intraoperative Pringle manuever | 73 (18.8%) | |||
| Liver cirrhosis | 156 (40.1%) | |||
| Intraoperative Ascites | 26 (6.7%) | |||
| Tumor size (cm) * | 4.05 | 2.88 | ||
| Resection margin (R0) | 368 (94.6%) | |||
| Pathologic Tumor stage | 1 | 194 (49.9%) | ||
| 2 | 141 (36.2%) | |||
| 3 | 40 (10.3%) | |||
| 4 | 14 (3.6%) | |||
| Postoperative complication | 87 (22.4%) | |||
| Postoperative hsCRP (mg L−1) | 32.16 | 41.40 | ||
| Postoperative albumin (g L−1) | 38.00 | 7.76 | ||
| Postoperative hsCRP/ALB ratio | 0.97 | 1.46 | ||
| Death | 98 (25.2%) | |||
| Recurrence | 193 (49.6%) | |||
| Variables | Univariate Analysis | Multivariate Analysis | |||
|---|---|---|---|---|---|
| Hazard Ratio (95% CI) | p-Value | Hazard Ratio (95% CI) | p-Value | ||
| Age | 1.015 (0.998–1.033) | 0.090 | 1.008 (0.990–1.026) | 0.372 | |
| Sex: Female (Ref: Male) | 0.887 (0.542–1.451) | 0.633 | |||
| Body Mass Index | 0.915 (0.856–0.979) | 0.008 | 0.901 (0.837–0.970) | 0.005 | |
| ASA class (Ref: I) | II | 1.176 (0.743–1.860) | 0.489 | ||
| III + IV | 1.472 (0.689–3.142) | 0.318 | |||
| Charson Comorbidity Index score | 0.969 (0.805–1.166) | 0.738 | |||
| Preoperative_TACE | 1.051 (0.810–1.365) | 0.707 | |||
| Preoperative_RFA | 1.230 (0.537–2.815) | 0.624 | |||
| Child_pugh_class B + C (Ref: A) | 1.599 (1.125–2.275) | 0.009 | 1.270 (0.794–2.029) | 0.319 | |
| Preoperative serum bilirubin | 0.883 (0.621–1.256) | 0.490 | |||
| Preoperative PT INR | 0.503 (0.082–3.083) | 0.457 | |||
| Preoperative alanine aminotransferase | 1.001 (0.997–1.006) | 0.551 | |||
| Preoperative aspartate aminotransferase | 0.999 (0.994–1.004) | 0.759 | |||
| Preop Virology | HBV (Ref: HCV) | 1.126 (0.670–1.890) | 0.655 | ||
| Both Positive (Ref: HCV) | 1.082 (0.40–2.601) | 0.861 | |||
| Both Negative (Ref: HCV) | 3.314 (0.441–24.89) | 0.244 | |||
| Preoperative serum aFP | 1.00 (1.00–1.00) | 0.632 | |||
| Laparoscopy (Ref: Laparotomy) | 2.118 (1.411–3.179) | <0.001 | 1.270 (0.794–2.029) | 0.319 | |
| Intraoperative RFA | 0.860 (0.398–1.859) | 0.701 | |||
| Major resection (ref: minor resection) * | 1.972 (1.324–2.938) | 0.001 | 1.134 (0.688–1.869) | 0.621 | |
| Intraoperative ascites | 1.671 (0.890–3.138) | 0.110 | |||
| Intraoperative Pringle manuever | 1.068 (0.956–1.194) | 0.242 | |||
| Operation time (min) | 1.001 (0.999–1.002) | 0.322 | |||
| Estimated Blood Loss (mL) | 1.00 (1.00–1.00) | 0.095 | |||
| Intraoperative Transfusion | 0.655 (0.434–0.989) | 0.044 | |||
| Preoperative Liver Cirrhosis | 1.258 (0.822–1.924) | 0.291 | 1.015 (0.612–1.681) | 0.955 | |
| Pathologic Tumor Size (mm) ** | 1.119 (1.060–1.182) | <0.001 | 1.064 (0.993–1.139) | 0.079 | |
| Tumor number | 1.138 (0.843–1.537) | 0.398 | |||
| Resection margin R1 (Ref: R0) | 2.477 (1.244–4.931) | 0.010 | 1.822 (0.790–4.198) | 0.159 | |
| Pathologic Tumor stage (1 increase in 1–4) | 1.448 (1.226–1.709) | <0.001 | 1.365 (1.134–1.643) | 0.001 | |
| Postoperative Complication | 1.708 (1.119–2.607) | 0.013 | 1.239 (0.743–2.067) | 0.411 | |
| hsCRP/ALB ratio (continous) *** | 1.202 (1.116–1.294) | <0.001 | 1.171 (1.072–1.278) | <0.001 | |
| hsCRP/ALB ratio >0.625 (dichotomous) | 2.671 (1.769–4.034) | <0.001 | 2.257 (1.470–3.466) | <0.001 | |
| Variables | Univariate Analysis | Multivariate Analysis | |||
|---|---|---|---|---|---|
| Hazard Ratio (95% CI) | p-Value | Hazard Ratio (95% CI) | p-Value | ||
| Age | 0.990 (0.978–1.002) | 0.093 | 0.983 (0.970–0.995) | 0.006 | |
| Sex: Female (Ref: Male) | 0.662 (0.459–0.955) | 0.027 | 0.741 (0.504–1.088) | 0.126 | |
| Body Mass Index | 0.953 (0.911–0.997) | 0.036 | 0.932 (0.887–0.978) | 0.004 | |
| ASA class (Ref: I) | II | 1.240 (0.888–1.732) | 0.206 | ||
| III + IV | 1.388 (0.775–2.486) | 0.270 | |||
| Charson Comorbidity Index score | 0.99 (0.874–1.121) | 0.873 | |||
| Preoperative_TACE | 0.858 (0.639–1.151) | 0.306 | |||
| Preoperative_RFA | 0.680 (0.418–1.106) | 0.120 | |||
| Child_pugh_class B + C (Ref: A) | 1.185 (0.879–1.597) | 0.265 | |||
| Preoperative serum bilirubin | 1.028 (0.862–1.225) | 0.759 | |||
| Preoperative PT INR | 0.964 (0.844–1.101) | 0.587 | |||
| Preoperative alanine aminotransferase | 1.003 (1.00–1.006) | 0.028 | 1.003 (1.000–1.005) | 0.058 | |
| Preoperative aspartate aminotransferase | 1.001 (0.999–1.003) | 0.473 | |||
| Preop Virology | HBV (Ref: HCV) | 1.015 (0.713–1.445) | 0.934 | ||
| Both Positive (Ref: HCV) | 1.398 (0.801–2.440) | 0.239 | |||
| Both Negative (Ref: HCV) | 0.00 (0.00–4.99 × 107) | 0.951 | |||
| Preoperative serum AFP | 1.00 (1.00–1.00) | 0.374 | |||
| laparoscopy (Ref: laparotomy) | 1.291 (0.973–1.714) | 0.077 | 0.970 (0.745–1.433) | 0.844 | |
| Intraoperative RFA | 0.534 (0.328–0.870) | 0.012 | |||
| Intraoperative ascites | 1.364 (0.817–2.276) | 0.235 | |||
| Major resection (ref: minor resection) * | 0.980 (0.719–1.335) | 0.897 | |||
| Intraoperative Pringle manuever | 0.936 (0.780–1.123) | 0.478 | |||
| Operation time (min) | 1.00 (1.00–1.001) | 0.362 | |||
| Estimated Blood Loss (ml) | 1.00 (1.00–1.00) | 0.520 | |||
| Intraoperative Transfusion | 0.800 (0.590–1.084) | 0.150 | |||
| Preoperative Liver Cirrhosis | 1.160 (0.866–1.553) | 0.319 | |||
| Pathologic Tumor Size (cm) ** | 1.082 (1.035–1.131) | 0.001 | 1.049 (0.995–1.106) | 0.079 | |
| Tumor number | 1.391 (1.158–1.670) | <0.001 | 1.126 (1.000–1.478) | 0.050 | |
| Resection margin R1 (Ref:R0) | 2.312 (1.361–3.927) | 0.002 | 2.418 (1.381–4.234) | 0.002 | |
| Pathologic Tumor stage (1 increase in 1–4) | 1.281 (1.118–1.468) | <0.001 | 1.248 (0.981–1.367) | 0.083 | |
| Postoperative Complication | 1.412 (1.026–1.941) | 0.034 | 1.114 (0.797–1.558) | 0.528 | |
| hsCRP/ALB ratio (continous) *** | 1.210 (1.136–1.289) | <0.001 | 1.190 (1.108–1.278) | <0.001 | |
| hsCRP/ALB ratio > 0.500 (dichotomous) | 1.652 (1.240–2.199) | 0.001 | 1.518 (1.125–2.050) | 0.006 | |
| Variables | Mortality | |
|---|---|---|
| Hazard Ratio (95% CI) | p-Value * | |
| Laparoscopy (hsCRP/ALB ratio >0.625) | 4.581 (2.445–8.584) | <0.001 |
| Laparotomy (hsCRP/ALB ratio >0.625) | 4.646 (2.082–10.366) | <0.001 |
| Recurrence | ||
| Hazard ratio (95% CI) | p-value * | |
| Laparoscopy (hsCRP/ALB ratio >0.500) | 1.483 (1.003–2.193) | 0.048 |
| Laparotomy (hsCRP/ALB ratio >0.500) | 1.995 (1.307–3.045) | 0.001 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Oh, T.K.; Choi, Y.-R.; Cho, J.Y.; Yoon, Y.-S.; Han, H.-S.; Park, I.S.; Ryu, J.-H. The High-Sensitivity C-Reactive Protein/Albumin Ratio Predicts Long-Term Oncologic Outcomes after Curative Resection for Hepatocellular Carcinoma. J. Clin. Med. 2018, 7, 139. https://doi.org/10.3390/jcm7060139
Oh TK, Choi Y-R, Cho JY, Yoon Y-S, Han H-S, Park IS, Ryu J-H. The High-Sensitivity C-Reactive Protein/Albumin Ratio Predicts Long-Term Oncologic Outcomes after Curative Resection for Hepatocellular Carcinoma. Journal of Clinical Medicine. 2018; 7(6):139. https://doi.org/10.3390/jcm7060139
Chicago/Turabian StyleOh, Tak Kyu, Young-Rok Choi, Jai Young Cho, Yoo-Suk Yoon, Ho-Seong Han, In Sun Park, and Jung-Hee Ryu. 2018. "The High-Sensitivity C-Reactive Protein/Albumin Ratio Predicts Long-Term Oncologic Outcomes after Curative Resection for Hepatocellular Carcinoma" Journal of Clinical Medicine 7, no. 6: 139. https://doi.org/10.3390/jcm7060139