Platelet-Rich Plasma May Offer a New Hope in Suppressed Wound Healing When Compared to Mesenchymal Stem Cells

 , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Materials
- -
- Sham-S group (vehicle group on which surgery was performed, with no experimental biological material being infused; n = 10)
- -
- Sham-M group (vehicle group on which surgery was performed following an intraperitoneal injection of corticosteroid, with no other experimental biological material being administered; n = 10)
- -
- PR group (surgery was performed following an intraperitoneal injection of corticosteroid, and then PRP was administered into the wound; n = 10)
- -
- MC group (surgery was performed following an intraperitoneal injection of corticosteroid, and then MSCs were administered into the wound; n = 10)
2.2. Surgery
2.3. Histopathological Analysis
2.4. Biochemical Analysis
2.5. Statistical Analysis
3. Results
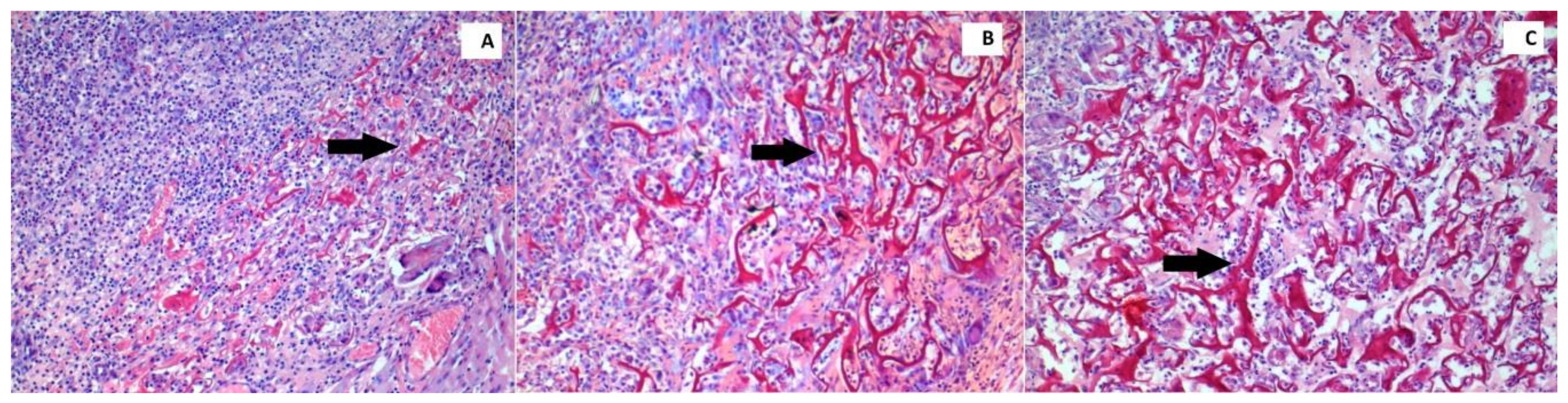
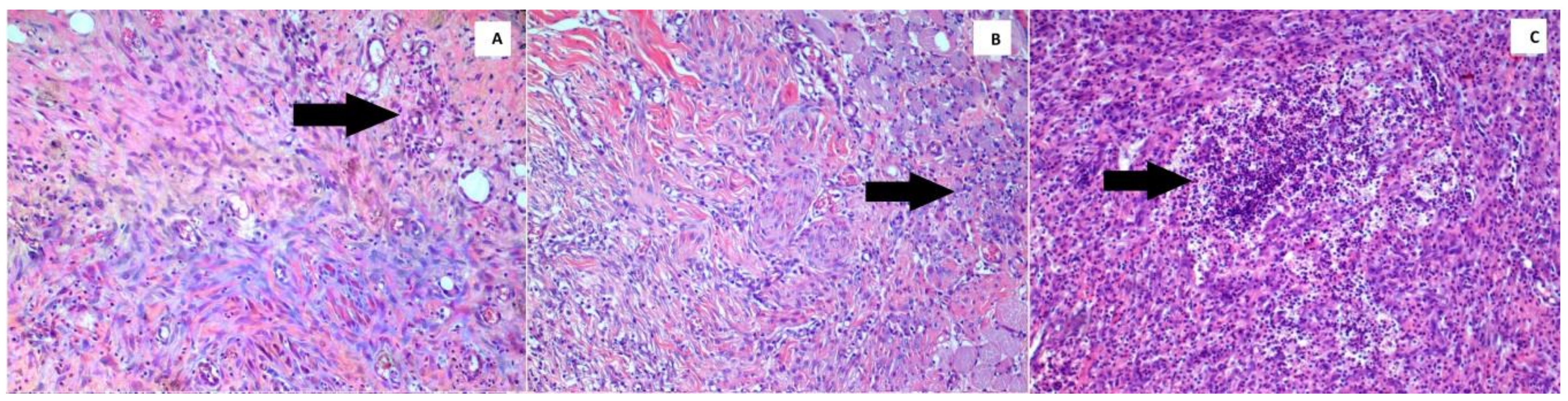
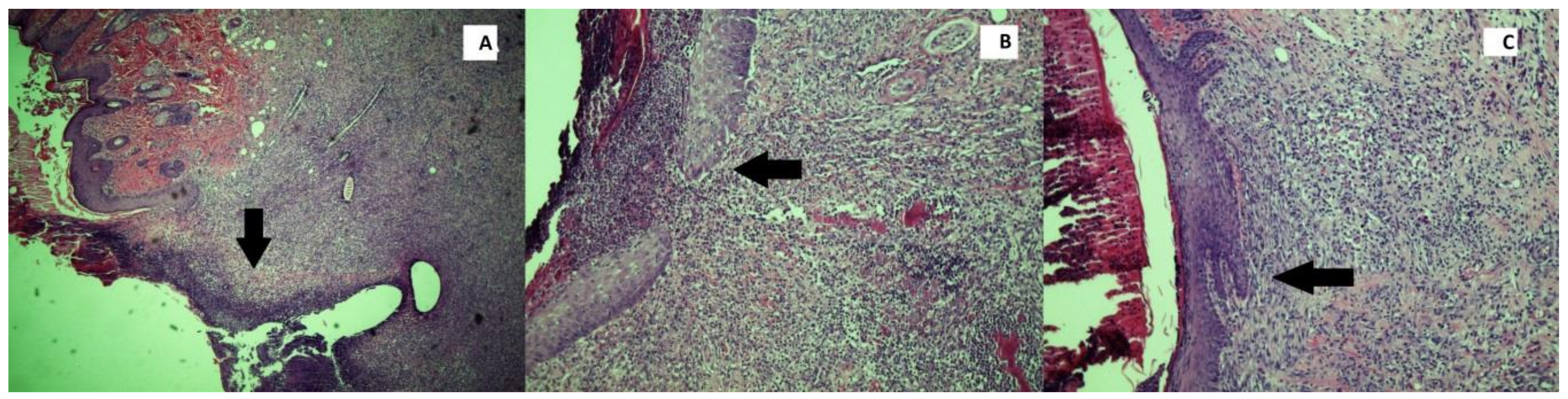
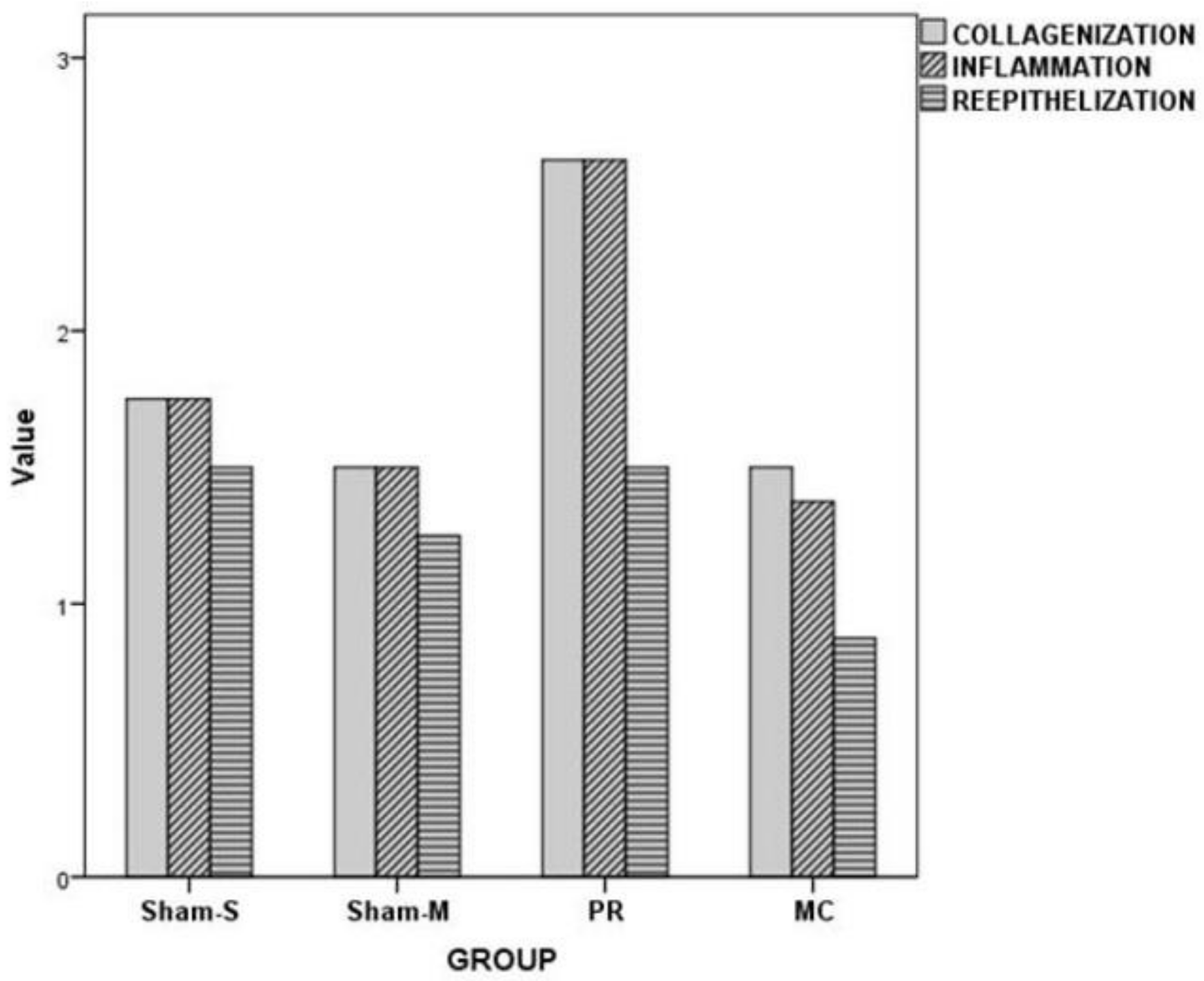
3.1. Histopathological Examination
3.2. Biochemical Examination
4. Discussion
Limitations
5. Conclusions
Author Contributions
Acknowledgments
Conflicts of Interest
References
- Nguyen, V.-L.; Truong, C.-T.; Nguyen, B.C.Q.; Van Vo, T.-N.; Dao, T.-T.; Nguyen, V.-D.; Trinh, D.T.T.; Huynh, H.K.; Bui, C.B. Anti-inflammatory and wound healing activities of calophyllolide isolated from Calophyllum inophyllum Linn. PLoS ONE 2017, 12, e0185674. [Google Scholar] [CrossRef] [PubMed]
- Eming, S.A.; Krieg, T.; Davidson, J.M. Inflammation in wound repair: Molecular and cellular mechanisms. J. Investig. Dermatol. 2007, 127, 514–525. [Google Scholar] [CrossRef] [PubMed]
- Fresno, L.; Fondevila, D.; Bambo, O.; Chacaltana, A.; Garcia, F.; Andaluz, A. Effects of platelet-rich plasma on intestinal wound healing in pigs. Vet. J. 2010, 185, 322–327. [Google Scholar] [CrossRef] [PubMed]
- Alissa, R.; Esposito, M.; Horner, K.; Oliver, R. The influence of platelet-rich plasma on the healing of extraction sockets: An explorative randomised clinical trial. Eur. J. Oral Implantol. 2010, 3, 121–134. [Google Scholar] [PubMed]
- Eppley, B.L.; Woodell, J.E.; Higgins, J. Platelet quantification and growth factor analysis from platelet-rich plasma: Implications for wound healing. Plast. Reconstr. Surg. 2004, 114, 1502–1508. [Google Scholar] [CrossRef] [PubMed]
- Karaca, G.; Aydin, O.; Pehlivanli, F.; Altunkaya, C.; Uzun, H.; Güler, O. Effectiveness of thymoquinone, zeolite, and platelet-rich plasma in model of corrosive oesophagitis induced in rats. Ann. Surg. Treat. Res. 2017, 92, 396–401. [Google Scholar] [CrossRef] [PubMed]
- Dugrillon, A.; Eichler, H.; Kern, S.; Klüter, H. Autologous concentrated platelet-rich plasma (cPRP) for local application in bone regeneration. Int. J. Oral Maxillofac. Surg. 2002, 31, 615–619. [Google Scholar] [CrossRef] [PubMed]
- Kark, L.R.; Karp, J.M.; Davies, J.E. Platelet releasate increases the proliferation and migration of bone marrow-derived cells cultured under osteogenic conditions. Clin. Oral Implants Res. 2006, 17, 321–327. [Google Scholar] [CrossRef] [PubMed]
- Ferrari, M.; Zia, S.; Valbonesi, M.; Henriquet, F.; Venere, G.; Spagnolo, S.; Grasso, M.A.; Panzani, I. A new technique for hemodilution, preparation of autologous platelet-rich plasma and intraoperative blood salvage in cardiac surgery. Int. J. Artif. Organs 1987, 10, 47–50. [Google Scholar] [CrossRef] [PubMed]
- Sampson, S.; Gerhardt, M.; Mandelbaum, B. Platelet rich plasma injection grafts for musculoskeletal injuries: A review. Curr. Rev. Musculoskelet. Med. 2008, 1, 165–174. [Google Scholar] [CrossRef] [PubMed]
- Carter, C.A.; Jolly, D.G.; Worden, C.E., Sr.; Hendren, D.G.; Kane, C.J. Platelet-rich plasma gel promotes differentiation and regeneration during equine wound healing. Exp. Mol. Pathol. 2003, 74, 244–255. [Google Scholar] [CrossRef]
- Karaca, G.; Pehlivanli, F.; Aydin, O.; Altunkaya, C.; Uzun, H.; Niyaz, M.; Özden, H.; Bulut, H. The effect of mesenchymal stem cell use on intra-abdominal adhesions in a rat model. Ann. Surg. Treat. Res. 2018, 94, 57–62. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Weissman, I.L. Stem cells: Units of development, units of regeneration, and units in evolution. Cell 2000, 100, 157–168. [Google Scholar] [CrossRef]
- Da Silva Meirelles, L.; Caplan, A.I.; Nardi, N.B. In search of the in vivo identity of mesenchymal stem cells. Stem Cells 2008, 26, 2287–2299. [Google Scholar] [CrossRef] [PubMed]
- Yoo, K.H.; Jang, I.K.; Lee, M.W.; Kim, H.E.; Yang, M.S.; Eom, Y.; Lee, J.E.; Kim, Y.J.; Yang, S.K.; Jung, H.L.; et al. Comparison of immunomodulatory properties of mesenchymal stem cells derived from adult human tissues. Cell. Immunol. 2009, 259, 150–156. [Google Scholar] [CrossRef] [PubMed]
- Hocking, A.M.; Gibran, N.S. Mesenchymal stem cells: Paracrine signaling and differentiation during cutaneous wound repair. Exp. Cell Res. 2010, 316, 2213–2219. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Smith, A.N.; Willis, E.; Chan, V.T.; Muffley, L.A.; Isik, F.F.; Gibran, N.S.; Hocking, A.M. Mesenchymal stem cells induce dermal fibroblast responses to injury. Exp. Cell Res. 2010, 316, 48–54. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, M.; Crisostomo, P.R.; Herring, C.; Meldrum, K.K.; Meldrum, D.R. Human progenitor cells from bone marrow or adipose tissue produce VEGF, HGF, and IGF-I in response to TNF by a p38 MAPK-dependent mechanism. Am. J. Physiol.-Regul. Integr. Comp. Physiol. 2006, 291, R880–R884. [Google Scholar] [CrossRef] [PubMed]
- Rehman, J.; Traktuev, D.; Li, J.; Merfeld-Clauss, S.; Temm-Grove, C.J.; Bovenkerk, J.E.; Pell, C.L.; Johnstone, B.H.; Considine, R.V.; March, K.L. Secretion of angiogenic and antiapoptotic factors by human adipose stromal cells. Circulation 2004, 109, 1292–1298. [Google Scholar] [CrossRef] [PubMed]
- Oettgen, P. Cardiac stem cell therapy. Circulation 2006, 114, 353–358. [Google Scholar] [CrossRef] [PubMed]
- Strauer, B.E.; Brehm, M.; Zeus, T.; Köstering, M.; Hernandez, A.; Sorg, R.V.; Kögler, G.; Wernet, P. Repair of infarcted myocardium by autologous intracoronary mononuclear bone marrow cell transplantation in humans. Circulation 2002, 106, 1913–1918. [Google Scholar] [CrossRef] [PubMed]
- Kwon, D.S.; Gao, X.; Liu, Y.B.; Dulchavsky, D.S.; Danyluk, A.L.; Bansal, M.; Chopp, M.; McIntosh, K.; Arbab, A.S.; Dulchavsky, S.A.; et al. Treatment with bone marrow-derived stromal cells accelerates wound healing in diabetic rats. Int. Wound J. 2008, 5, 453–463. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wahl, S.M. Glucocorticoids and Wound Healing. In Anti-Inflammatory Steroids Action: Basic and Clinical Aspects; Schleimer, R.P., Claman, H.N., Oronsky, A.L., Eds.; New York Academic Press: New York, NY, USA, 1983. [Google Scholar]
- Levenson, S.M. DA: Metabolic Factors In Wound Healing. In Wound Healing: Biochemical and Clinical Aspects; Cohen, I.K., Diegelmann, R.F., Lindblad, W.J., Eds.; W. B. Saunders: Philadelphia, PA, USA, 2001; pp. 273–284. [Google Scholar]
- Karaca, G.; Pekcici, M.; Altunkaya, C.; Fidanci, V.; Kilinc, A.; Ozer, H.; Tekeli, A.; Aydinuraz, K.; Guler, O. The effects of scalpel, harmonic scalpel and monopolar electrocautery on the healing of colonic anastomosis after colonic resection. Ann. Surg. Treat. Res. 2016, 90, 315–321. [Google Scholar] [CrossRef] [PubMed]
- Hendriks, T.; Mastboom, W.J. Healing of experimental intestinal anastomoses. Dis. Colon Rectum 1990, 33, 891–901. [Google Scholar] [CrossRef] [PubMed]
- Kimura, A.; Ogata, H.; Yazawa, M.; Watanabe, N.; Mori, T.; Nakajima, T. The effects of platelet-rich plasma on cutaneous incisional wound healing in rats. J. Dermatol. Sci. 2005, 40, 205–208. [Google Scholar] [CrossRef] [PubMed]
- Crovetti, G.; Martinelli, G.; Issi, M.; Barone, M.; Guizzardi, M.; Campanati, B.; Moroni, M.; Carabelli, A. Platelet gel for healing cutaneous chronic wounds. Transfus. Apheresis Sci. 2004, 30, 145–151. [Google Scholar] [CrossRef] [PubMed]
- Kim, Y.; Kim, H.; Cho, H.; Bae, Y.; Suh, K.; Jung, J. Direct comparison of human mesenchymal stem cells derived from adipose tissues and bone marrow in mediating neovascularization in response to vascular ischemia. Cell. Physiol. Biochem. 2007, 20, 867–876. [Google Scholar] [CrossRef] [PubMed]
- Noel, D.; Caton, D.; Roche, S.; Bony, C.; Lehmann, S.; Casteilla, L.; Jorgensen, C.; Cousin, B. Cell specific differences between human adipose-derived and mesenchymal-stromal cells despite similar differentiation potentials. Exp. Cell Res. 2008, 314, 1575–1584. [Google Scholar] [CrossRef] [PubMed]
- Lu, F.; Mizuno, H.; Uysal, C.A.; Cai, X.; Ogawa, R.; Hyakusoku, H. Improved viability of random pattern skin flaps through the use of adipose-derived stem cells. Plast. Reconstr. Surg. 2008, 121, 50–58. [Google Scholar] [CrossRef] [PubMed]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Grade | Collagenization | Inflammation | Reepithelialization |
|---|---|---|---|
| Grade 0 | None | None | No epithelization |
| Grade 1 | Minimal | Minimal | Incomplete coverage |
| Grade 2 | Moderate | Moderate | Complete reepithelization |
| Grade 3 | Severe | Severe | - |
| Group | Variable | Minimum | Maximum | Mean/Median (*) | SD |
|---|---|---|---|---|---|
| Sham-S | Collagenization | 1 | 2 | 2 * | 0.46 |
| Inflammation | 1 | 2 | 2 * | 0.46 | |
| Reepithelization | 1 | 2 | 1.5 * | 0.54 | |
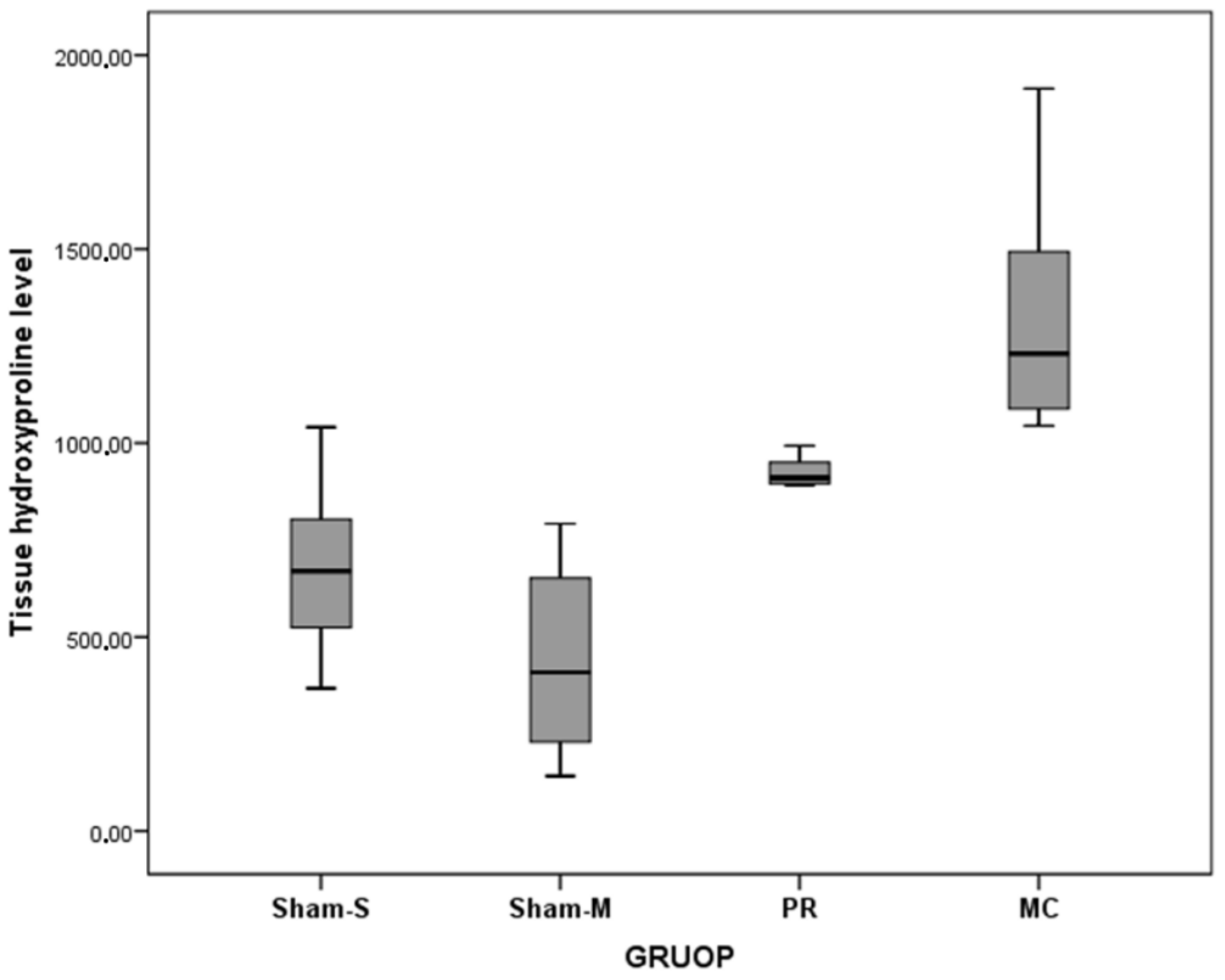
| Hydroxyproline | 367.71 | 1040.57 | 675.64 | 220.16 | |
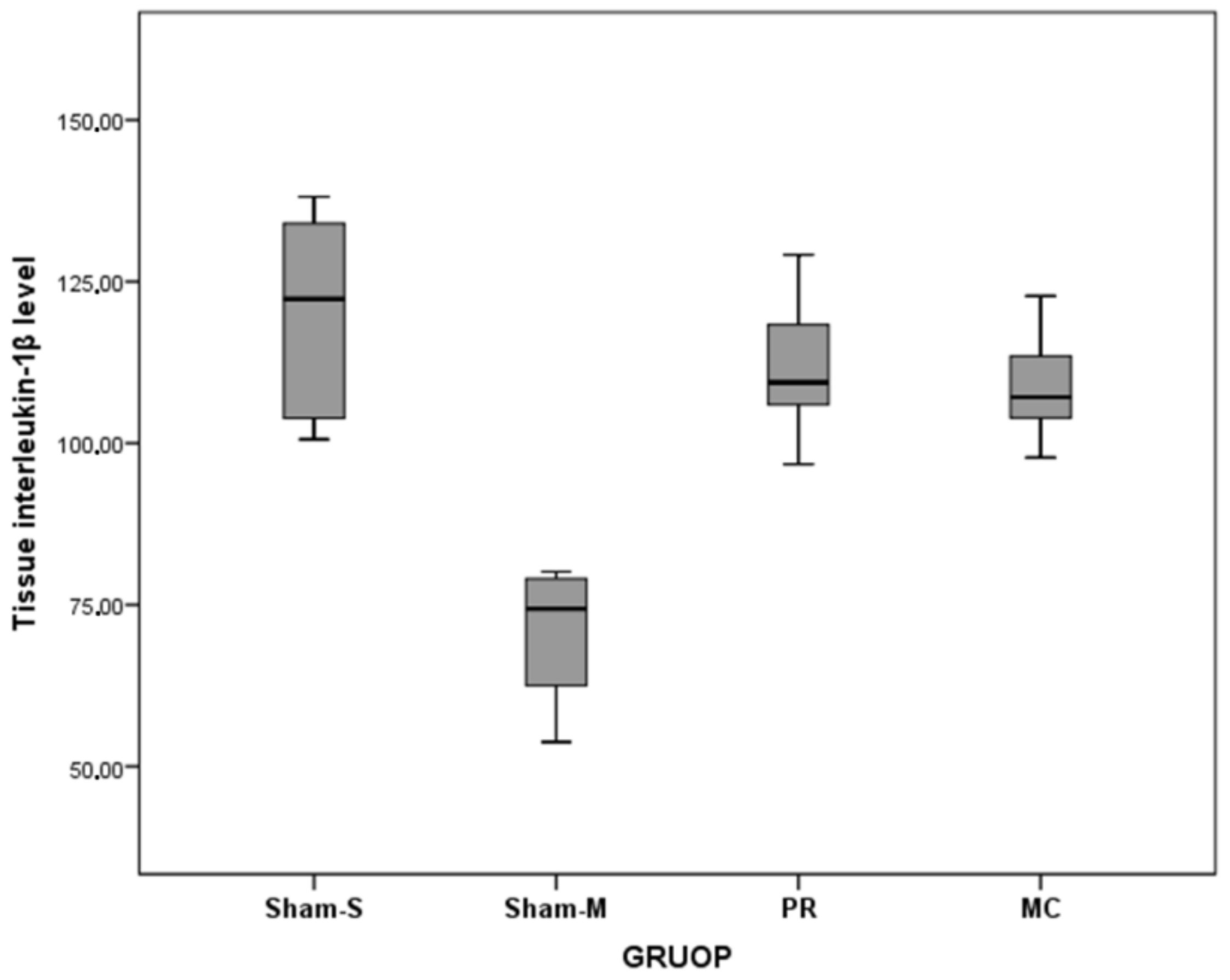
| Interleukin-1β | 100.58 | 138.14 | 119.89 | 15.48 | |
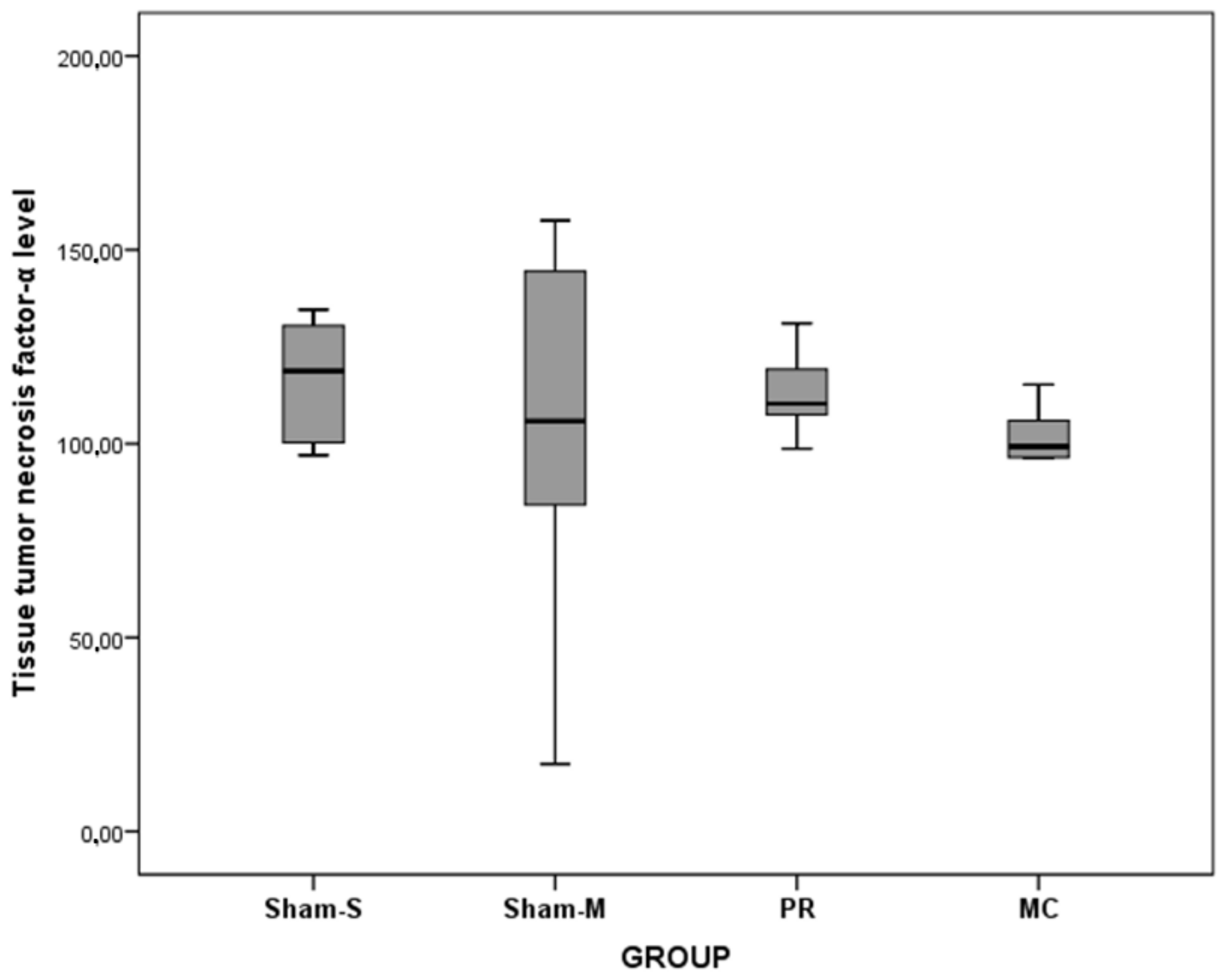
| Tumor necrosis factor-α | 97.01 | 134.57 | 118.75 * | 15.48 | |
| Sham-M | Collagenization | 1 | 2 | 1.5 * | 0.54 |
| Inflammation | 1 | 2 | 1.5 * | 0.54 | |
| Reepithelization | 1 | 2 | 1 * | 0.46 | |
| Hydroxyproline | 141.89 | 792.22 | 439.47 | 238.99 | |
| Interleukin-1β | 53.78 | 144.07 | 78.71 | 27.99 | |
| Tumor necrosis factor-α | 17.36 | 157.57 | 105.79 * | 46.80 | |
| PR | Collagenization | 2 | 3 | 3 * | 0.52 |
| Inflammation | 2 | 3 | 3 * | 0.52 | |
| Reepithelization | 1 | 2 | 1.5 * | 0.54 | |
| Hydroxyproline | 696.02 | 992.97 | 900.30 | 89.29 | |
| Interleukin-1β | 96.76 | 129.13 | 111.66 | 10.44 | |
| Tumor necrosis factor-α | 98.66 | 131.02 | 110.30 * | 10.52 | |
| MC | Collagenization | 1 | 2 | 1.5 * | 0.54 |
| Inflammation | 1 | 2 | 1 * | 0.52 | |
| Reepithelization | 0 | 2 | 1 * | 0.64 | |
| Hydroxyproline | 1044.82 | 1913.75 | 1322.80 | 298.24 | |
| Interleukin-1β | 97.78 | 122.77 | 108.71 | 8.11 | |
| Tumor necrosis factor-α | 80.26 | 115.25 | 99.24 * | 10.46 |
| Variable | F/X2 (*) | p |
|---|---|---|
| Collagenization | 13.89 * | 0.003 |
| Inflammation | 14.79 * | 0.002 |
| Reepithelization | 5.59 * | 0.134 |
| Hydroxyproline | 22.34 | <0.001 |
| Interleukin-1β | 8.64 | <0.001 |
| Tumor necrosis factor-α | 4.71 * | 0.194 |
| Variable | Group (I/J) | MD/Z (*) | p |
|---|---|---|---|
| Collagenization | Sham-S/PR | −2.71 * | 0.007 |
| Sham-M/PR | −2.92 * | 0.003 | |
| MC/PR | −2.92 * | 0.003 | |
| Inflammation | Sham-S/PR | −2.71 * | 0.007 |
| Sham-M/PR | −2.92 * | 0.003 | |
| MC/PR | −3.06 * | 0.002 | |
| Hydroxyproline | Sham-S/MC | −647.17 | <0.001 |
| Sham-M/PR | −460.82 | 0.002 | |
| Sham-M/MC | −883.33 | <0.001 | |
| Interleukin-1β | Sham-M/Sham-S | −41.17 | <0.001 |
| Sham-M/PR | −32.94 | 0.004 | |
| Sham-M/MC | −29.99 | 0.009 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Aydin, O.; Karaca, G.; Pehlivanli, F.; Altunkaya, C.; Uzun, H.; Özden, H.; Aydin, G.; Şahiner, İ.T.; Niyaz, M.; Güler, O. Platelet-Rich Plasma May Offer a New Hope in Suppressed Wound Healing When Compared to Mesenchymal Stem Cells. J. Clin. Med. 2018, 7, 143. https://doi.org/10.3390/jcm7060143
Aydin O, Karaca G, Pehlivanli F, Altunkaya C, Uzun H, Özden H, Aydin G, Şahiner İT, Niyaz M, Güler O. Platelet-Rich Plasma May Offer a New Hope in Suppressed Wound Healing When Compared to Mesenchymal Stem Cells. Journal of Clinical Medicine. 2018; 7(6):143. https://doi.org/10.3390/jcm7060143
Chicago/Turabian StyleAydin, Oktay, Gökhan Karaca, Faruk Pehlivanli, Canan Altunkaya, Hafize Uzun, Hüseyin Özden, Gülçin Aydin, İbrahim Tayfun Şahiner, Mehmet Niyaz, and Osman Güler. 2018. "Platelet-Rich Plasma May Offer a New Hope in Suppressed Wound Healing When Compared to Mesenchymal Stem Cells" Journal of Clinical Medicine 7, no. 6: 143. https://doi.org/10.3390/jcm7060143