Response-Related Factors of Bone Marrow-Derived Mesenchymal Stem Cells Transplantation in Patients with Alcoholic Cirrhosis

 ,
,  ,
,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Bone Marrow Aspiration, Isolation, and Culture
2.3. Viability, Immunophenotype, and Differential Potential of Stem Cells
2.4. Whole Transcript Expression Arrays and Data Preparation
2.5. Statistical Analysis
3. Results
3.1. Patients
3.2. Viability, Immunophenotype, and Differentiation Potential
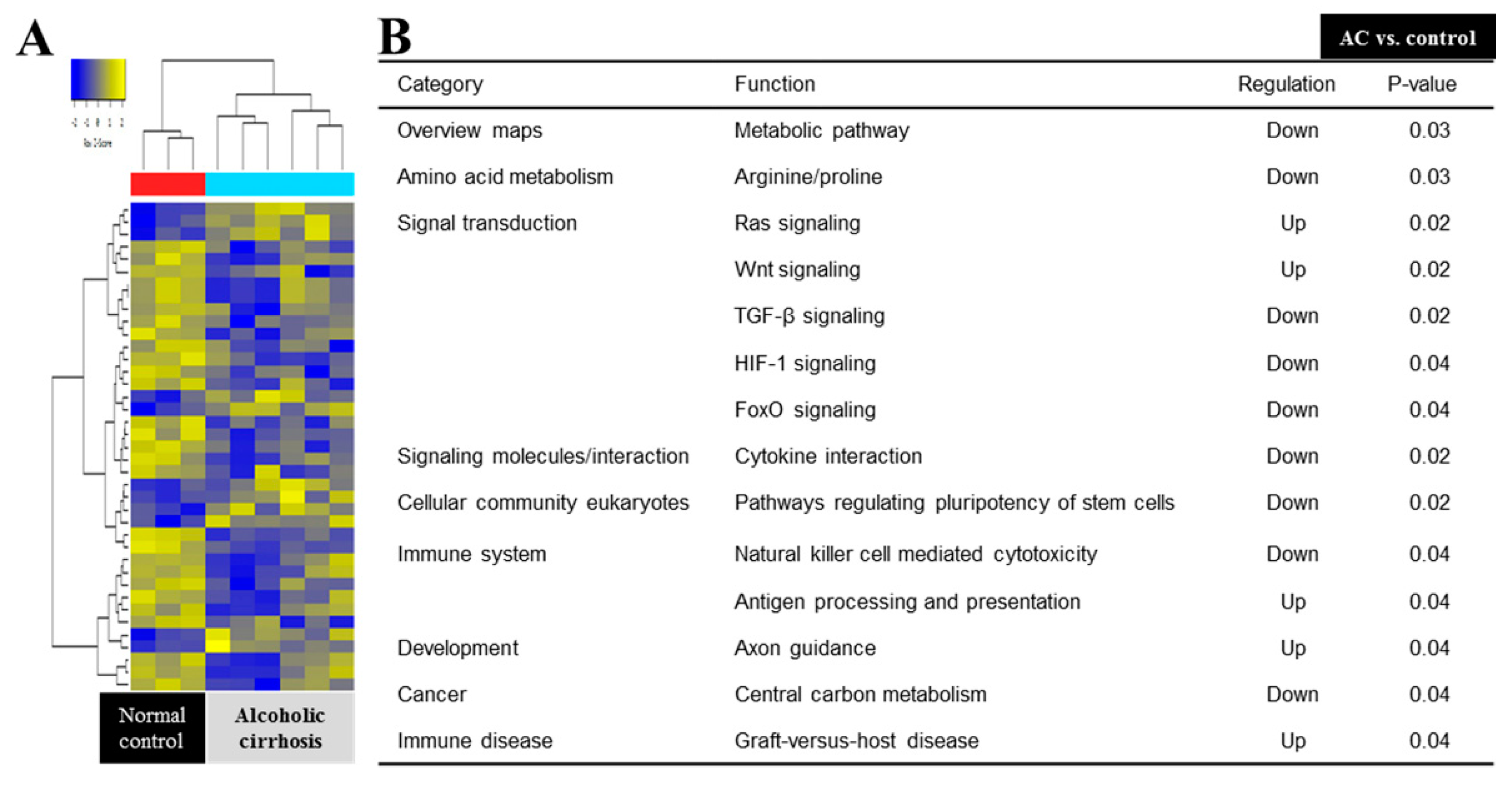
3.3. Response-Related Biological Processes and Signal Pathway
3.4. Differentially Expressed Genes
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Gao, B.; Bataller, R. Alcoholic liver disease: Pathogenesis and new therapeutic targets. Gastroenterology 2011, 141, 1572–1585. [Google Scholar] [CrossRef] [PubMed]
- Suk, K.T.; Baik, S.K.; Yoon, J.H.; Cheong, J.Y.; Paik, Y.H.; Lee, C.H.; Kim, Y.S.; Lee, J.W.; Kim, D.J.; Cho, S.W.; et al. Revision and update on clinical practice guideline for liver cirrhosis. Korean J. Hepatol. 2012, 18, 1–21. [Google Scholar] [CrossRef] [PubMed]
- Burra, P.; Senzolo, M.; Adam, R.; Delvart, V.; Karam, V.; Germani, G.; Neuberger, J.; Elita; Centers, E.L.T. Liver transplantation for alcoholic liver disease in europe: A study from the eltr (European liver transplant registry). Am. J. Transplant. 2010, 10, 138–148. [Google Scholar] [CrossRef] [PubMed]
- Lucey, M.R. Liver transplantation in patients with alcoholic liver disease. Liver transplantation: Official publication of the American Association for the Study of Liver Diseases and the International Liver Transplantation Society. Liver Transpl. 2011, 17, 751–759. [Google Scholar] [CrossRef] [PubMed]
- Khan, J.A.; Mendelson, A.; Kunisaki, Y.; Birbrair, A.; Kou, Y.; Arnal-Estape, A.; Pinho, S.; Ciero, P.; Nakahara, F.; M’ayan, A.; et al. Fetal liver hematopoietic stem cell niches associate with portal vessels. Science 2016, 351, 176–180. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ullah, I.; Subbarao, R.B.; Rho, G.J. Human mesenchymal stem cells—Current trends and future prospective. Biosci. Rep. 2015, 35, e00191. [Google Scholar] [CrossRef] [PubMed]
- Jang, Y.O.; Kim, Y.J.; Baik, S.K.; Kim, M.Y.; Eom, Y.W.; Cho, M.Y.; Park, H.J.; Park, S.Y.; Kim, B.R.; Kim, J.W.; et al. Histological improvement following administration of autologous bone marrow-derived mesenchymal stem cells for alcoholic cirrhosis: A pilot study. Liver Int. 2014, 34, 33–41. [Google Scholar] [CrossRef] [PubMed]
- Alfaifi, M.; Eom, Y.W.; Newsome, P.N.; Baik, S.K. Mesenchymal stromal cell therapy for liver diseases. J. Hepatol. 2018, 68, 1272–1285. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Suk, K.T.; Yoon, J.H.; Kim, M.Y.; Kim, C.W.; Kim, J.K.; Park, H.; Hwang, S.G.; Kim, D.J.; Lee, B.S.; Lee, S.H.; et al. Transplantation with autologous bone marrow-derived mesenchymal stem cells for alcoholic cirrhosis: Phase 2 trial. Hepatology 2016, 64, 2185–2197. [Google Scholar] [CrossRef]
- Eom, Y.W.; Kim, G.; Baik, S.K. Mesenchymal stem cell therapy for cirrhosis: Present and future perspectives. World J. Gastroenterol. 2015, 21, 10253–10261. [Google Scholar] [CrossRef]
- Shim, K.Y.; Eom, Y.W.; Kim, M.Y.; Kang, S.H.; Baik, S.K. Role of the renin-angiotensin system in hepatic fibrosis and portal hypertension. Korean J. Int. Med. 2018, 33, 453–461. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, D.L.; He, X.H.; Zhang, S.A.; Fang, J.; Chen, F.S.; Fan, J.J. Bone marrow-derived mesenchymal stem cells promote hepatic regeneration after partial hepatectomy in rats. Pathobiology 2013, 80, 228–234. [Google Scholar] [CrossRef] [PubMed]
- Wei, X.; Yang, X.; Han, Z.P.; Qu, F.F.; Shao, L.; Shi, Y.F. Mesenchymal stem cells: A new trend for cell therapy. Acta Pharmacol. Sin. 2013, 34, 747–754. [Google Scholar] [CrossRef] [PubMed]
- Kim, D.; Cho, G.S.; Han, C.; Park, D.H.; Park, H.K.; Woo, D.H.; Kim, J.H. Current understanding of stem cell and secretome therapies in liver diseases. Tissue Eng. Regen. Med. 2017, 14, 653–665. [Google Scholar] [CrossRef] [PubMed]
- Higashiyama, R.; Inagaki, Y.; Hong, Y.Y.; Kushida, M.; Nakao, S.; Niioka, M.; Watanabe, T.; Okano, H.; Matsuzaki, Y.; Shiota, G.; et al. Bone marrow-derived cells express matrix metalloproteinases and contribute to regression of liver fibrosis in mice. Hepatology 2007, 45, 213–222. [Google Scholar] [CrossRef]
- Jang, Y.O.; Jun, B.G.; Baik, S.K.; Kim, M.Y.; Kwon, S.O. Inhibition of hepatic stellate cells by bone marrow-derived mesenchymal stem cells in hepatic fibrosis. Clin. Mol. Hepatol. 2015, 21, 141–149. [Google Scholar] [CrossRef] [Green Version]
- European Association for the Study of Liver. Easl clinical practical guidelines: Management of alcoholic liver disease. J. Hepatol. 2012, 57, 399–420. [Google Scholar] [CrossRef]
- D’Amico, G.; Garcia-Tsao, G.; Pagliaro, L. Natural history and prognostic indicators of survival in cirrhosis: A systematic review of 118 studies. J. Hepatol. 2006, 44, 217–231. [Google Scholar] [CrossRef]
- Hu, Y.; Liao, L.; Wang, Q.; Ma, L.; Ma, G.; Jiang, X.; Zhao, R.C. Isolation and identification of mesenchymal stem cells from human fetal pancreas. J. Lab. Clin. Med. 2003, 141, 342–349. [Google Scholar] [CrossRef]
- Alshareeda, A.T.; Alsowayan, B.; Almubarak, A.; Alghuwainem, A.; Alshawakir, Y.; Alahmed, M. Exploring the potential of mesenchymal stem cell sheet on the development of hepatocellular carcinoma in vivo. J. Vis. Exp. 2018, 139, e57805. [Google Scholar] [CrossRef]
- Si-Tayeb, K.; Noto, F.K.; Nagaoka, M.; Li, J.; Battle, M.A.; Duris, C.; North, P.E.; Dalton, S.; Duncan, S.A. Highly efficient generation of human hepatocyte-like cells from induced pluripotent stem cells. Hepatology 2010, 51, 297–305. [Google Scholar] [CrossRef] [PubMed]
- Chamberlain, G.; Fox, J.; Ashton, B.; Middleton, J. Concise review: Mesenchymal stem cells: Their phenotype, differentiation capacity, immunological features, and potential for homing. Stem Cells 2007, 25, 2739–2749. [Google Scholar] [CrossRef] [PubMed]
- Collins, R.F.; Touret, N.; Kuwata, H.; Tandon, N.N.; Grinstein, S.; Trimble, W.S. Uptake of oxidized low density lipoprotein by cd36 occurs by an actin-dependent pathway distinct from macropinocytosis. J. Biol. Chem. 2009, 284, 30288–30297. [Google Scholar] [CrossRef] [PubMed]
- Stewart, C.R.; Stuart, L.M.; Wilkinson, K.; van Gils, J.M.; Deng, J.; Halle, A.; Rayner, K.J.; Boyer, L.; Zhong, R.; Frazier, W.A.; et al. Cd36 ligands promote sterile inflammation through assembly of a toll-like receptor 4 and 6 heterodimer. Nat. Immunol. 2010, 11, 155–161. [Google Scholar] [CrossRef] [PubMed]
- Zhou, Y.; Li, L.L.; Zhong, Z.L.; Liu, X.J.; Liu, J.L.; Shen, W.D.; Wu, G.G. Anti-cd36 mediated platelet transfusion refractoriness and related cases after stem cell transplantation. Zhongguo Shi Yan Xue Ye Xue Za Zhi 2018, 26, 541–546. [Google Scholar]
- Yang, Q.; Graham, T.E.; Mody, N.; Preitner, F.; Peroni, O.D.; Zabolotny, J.M.; Kotani, K.; Quadro, L.; Kahn, B.B. Serum retinol binding protein 4 contributes to insulin resistance in obesity and type 2 diabetes. Nature 2005, 436, 356–362. [Google Scholar] [CrossRef]
- Blaner, W.S. Retinol-binding protein: The serum transport protein for vitamin a. Endocr. Rev. 1989, 10, 308–316. [Google Scholar] [CrossRef]
- Li, X.; Fei, T.; Wang, Y.; Zhao, Y.; Pan, Y.; Li, D. Wheat starch with low retrogradation properties produced by modification of the gtfb enzyme 4,6-alpha-glucanotransferase from streptococcus thermophilus. J. Agric. Food Chem. 2018, 66, 3891–3898. [Google Scholar] [CrossRef]
- Zhuang, W.; Ge, X.; Yang, S.; Huang, M.; Zhuang, W.; Chen, P.; Zhang, X.; Fu, J.; Qu, J.; Li, B. Upregulation of lncrna meg3 promotes osteogenic differentiation of mesenchymal stem cells from multiple myeloma patients by targeting bmp4 transcription. Stem Cells 2015, 33, 1985–1997. [Google Scholar] [CrossRef]
- Deng, L.; Hong, H.; Zhang, X.; Chen, D.; Chen, Z.; Ling, J.; Wu, L. Down-regulated lncrna meg3 promotes osteogenic differentiation of human dental follicle stem cells by epigenetically regulating wnt pathway. Biochem. Biophys. Res. Commun. 2018, 503, 2061–2067. [Google Scholar] [CrossRef]
- Sun, X.; Luo, L.H.; Feng, L.; Li, D.S. Down-regulation of lncrna meg3 promotes endothelial differentiation of bone marrow derived mesenchymal stem cells in repairing erectile dysfunction. Life Sci. 2018, 208, 246–252. [Google Scholar] [CrossRef] [PubMed]
- Dozynkiewicz, M.A.; Jamieson, N.B.; Macpherson, I.; Grindlay, J.; van den Berghe, P.V.; von Thun, A.; Morton, J.P.; Gourley, C.; Timpson, P.; Nixon, C.; et al. Rab25 and clic3 collaborate to promote integrin recycling from late endosomes/lysosomes and drive cancer progression. Dev. Cell 2012, 22, 131–145. [Google Scholar] [CrossRef]
- Macpherson, I.R.; Rainero, E.; Mitchell, L.E.; van den Berghe, P.V.; Speirs, C.; Dozynkiewicz, M.A.; Chaudhary, S.; Kalna, G.; Edwards, J.; Timpson, P.; et al. Clic3 controls recycling of late endosomal mt1-mmp and dictates invasion and metastasis in breast cancer. J. Cell Sci. 2014, 127, 3893–3901. [Google Scholar] [CrossRef] [PubMed]
- Brum, A.M.; van der Leije, C.S.; Schreuders-Koedam, M.; Verhoeven, J.; Janssen, M.; Dekkers, D.H.; Demmers, J.A.; Eijken, M.; van de Peppel, J.; PTM van Leeuwen, J.; et al. Identification of chloride intracellular channel protein 3 as a novel gene affecting human bone formation. J.Bone Miner. Res. 2017, 1, 16–26. [Google Scholar] [CrossRef] [PubMed]
- Miura, N.; Sato, R.; Tsukamoto, T.; Shimizu, M.; Kabashima, H.; Takeda, M.; Takahashi, S.; Harada, T.; West, J.E.; Drabkin, H.; et al. A noncoding rna gene on chromosome 10p15.3 may function upstream of htert. BMC Mol. Biol. 2009, 10, 5. [Google Scholar] [CrossRef]
- Tsuno, S.; Wang, X.; Shomori, K.; Hasegawa, J.; Miura, N. Hsa-mir-520d induces hepatoma cells to form normal liver tissues via a stemness-mediated process. Sci. Rep. 2014, 4, 3852. [Google Scholar] [CrossRef] [PubMed]
- Tsukerman, P.; Yamin, R.; Seidel, E.; Khawaled, S.; Schmiedel, D.; Bar-Mag, T.; Mandelboim, O. Mir-520d-5p directly targets twist1 and downregulates the metastamir mir-10b. Oncotarget 2014, 5, 12141–12150. [Google Scholar] [CrossRef]
- Manh, T.H.; Young, M.K.; Dae-Yeul, Y.; Dae, H.L.; Moonjae, C.; Changlim, H. Tgf-β secreted from activated hepatic stellate cells may induce the transdifferentiation of hepatocytes into hepatocarcinoma in hbx-expressing livers. J. Korean Soc. Appl. Biol. Chem. 2014, 57, 529–538. [Google Scholar]
- Block, G.J.; Ohkouchi, S.; Fung, F.; Frenkel, J.; Gregory, C.; Pochampally, R.; DiMattia, G.; Sullivan, D.E.; Prockop, D.J. Multipotent stromal cells are activated to reduce apoptosis in part by upregulation and secretion of stanniocalcin-1. Stem Cells 2009, 27, 670–681. [Google Scholar] [CrossRef]
- Ono, M.; Ohkouchi, S.; Kanehira, M.; Tode, N.; Kobayashi, M.; Ebina, M.; Nukiwa, T.; Irokawa, T.; Ogawa, H.; Akaike, T.; et al. Mesenchymal stem cells correct inappropriate epithelial-mesenchyme relation in pulmonary fibrosis using stanniocalcin-1. Mol. Ther. 2015, 23, 549–560. [Google Scholar] [CrossRef]
- Kato, N.; Ji, G.; Wang, Y.; Baba, M.; Hoshida, Y.; Otsuka, M.; Taniguchi, H.; Moriyama, M.; Dharel, N.; Goto, T.; et al. Large-scale search of single nucleotide polymorphisms for hepatocellular carcinoma susceptibility genes in patients with hepatitis c. Hepatology 2005, 42, 846–853. [Google Scholar] [CrossRef] [PubMed]
- Chen, H.; Suzuki, M.; Nakamura, Y.; Ohira, M.; Ando, S.; Iida, T.; Nakajima, T.; Nakagawara, A.; Kimura, H. Aberrant methylation of fbn2 in human non-small cell lung cancer. Lung Cancer 2005, 50, 43–49. [Google Scholar] [CrossRef] [PubMed]
- Yeung, H.Y.; Lai, K.P.; Chan, H.Y.; Mak, N.K.; Wagner, G.F.; Wong, C.K. Hypoxia-inducible factor-1-mediated activation of stanniocalcin-1 in human cancer cells. Endocrinology 2005, 146, 4951–4960. [Google Scholar] [CrossRef] [PubMed]
- Bernard, O.; Jeny, F.; Uzunhan, Y.; Dondi, E.; Terfous, R.; Label, R.; Sutton, A.; Larghero, J.; Vanneaux, V.; Nunes, H.; et al. Mesenchymal stem cells reduce hypoxia-induced apoptosis in alveolar epithelial cells by modulating hif and ros hypoxic signaling. Am. J. Physiol. Lung Cell. Mol. Physiol. 2018, 314, L360–L371. [Google Scholar] [CrossRef] [PubMed]
- Dupuy, F.; Tabaries, S.; Andrzejewski, S.; Dong, Z.; Blagih, J.; Annis, M.G.; Omeroglu, A.; Gao, D.; Leung, S.; Amir, E.; et al. Pdk1-dependent metabolic reprogramming dictates metastatic potential in breast cancer. Cell Metab. 2015, 22, 577–589. [Google Scholar] [CrossRef] [PubMed]
- Lockyer, P.J.; Kupzig, S.; Cullen, P.J. Capri regulates Ca(2+)-dependent inactivation of the ras-mapk pathway. Curr. Biol. 2001, 11, 981–986. [Google Scholar] [CrossRef]
- Delire, B.; Starkel, P. The ras/mapk pathway and hepatocarcinoma: Pathogenesis and therapeutic implications. Eur. J. Clin. Investig. 2015, 45, 609–623. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Variables | AC Control | p | BM-MSC Transplantation | p | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Responder (n = 8) | Non-Responder (n = 10) | Responder (n = 25) | Non-Responder (n = 12) | |||||||
| Male (n, %) | 8 | (100) | 9 | (90) | NS | 21 | (84) | 9 | (82) | NS |
| Age a | 51 | (8) | 54 | (8) | NS | 54 | (8) | 55 | (9) | NS |
| Functional analysis a | ||||||||||
| CP score | 8.5 | (1.4.) | 8.0 | (1.5) | NS | 7.8 | (1.1) | 7.8 | (1.1) | NS |
| MELD score | 14.9 | (4.9) | 12.8 | (3.2) | NS | 10.3 | (3.9) | 8.3 | (4.7) | NS |
| Histologic analysis a | ||||||||||
| Laennec score | 8.9 | (1.4) | 7.5 | (1.1) | 0.029 | 7.7 | (1.2) | 6.7 | (1.2) | 0.021 |
| Biochemical analysis a | ||||||||||
| AST (IU/L) | 61 | (52) | 42 | (9) | NS | 39 | (18) | 43 | (15) | NS |
| ALT (IU/L) | 37 | (28) | 28 | (9) | NS | 23 | (10) | 22 | (13) | NS |
| Albumin (g/dL) | 3.2 | (0.6) | 3.6 | (0.5) | NS | 3.7 | (0.8) | 3.3 | (0.6) | NS |
| Bilirubin (mg/dL) | 3.5 | (2.9) | 2.4 | (1.5) | NS | 1.6 | (1.2) | 1.5 | (1.0) | NS |
| ALP (IU/L) | 169 | (66) | 97 | (35) | 0.009 | 118 | (68) | 169 | (88) | NS |
| GGT (IU/L) | 74 | (97) | 61 | (46) | NS | 69 | (68) | 78 | (53) | NS |
| Variables | Responder (n = 33) | p | Non-Responder (n = 22) | p | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Pre | Post | Pre | Post | |||||||
| Functional analysis a | ||||||||||
| Child–Pugh score | 7.7 | (1.1) | 6.7 | (1.7) | <0.001 | 8.1 | (1.4) | 7.3 | (2.1) | NS |
| Histologic analysis a | ||||||||||
| Laennec score | 8.0 | (1.3) | 6.3 | (1.3) | <0.001 | 7.1 | (1.2) | 7.4 | (1.5) | 0.031 |
| Biochemical analysis a | ||||||||||
| AST (IU/L) | 44 | (31) | 38 | (21) | 0.012 | 47 | (15) | 49 | (23) | 0.036 |
| ALT (IU/L) | 25 | (17) | 21 | (11) | NS | 28 | (12) | 30 | (14) | NS |
| Albumin (g/dL) | 3.7 | (0.7) | 4.1 | (1.9) | NS | 3.3 | (0.6) | 3.3 | (0.6) | NS |
| Bilirubin (mg/dL) | 1.8 | (1.2) | 1.8 | (1.5) | NS | 2.7 | (2.3) | 2.1 | (0.9) | NS |
| ALP (IU/L) | 118 | (59) | 104 | (35) | NS | 142 | (74) | 126 | (58) | NS |
| GGT (IU/L) | 76 | (70) | 75 | (50) | NS | 57 | (52) | 77 | (75) | NS |
| Term | p-Value | Genes |
|---|---|---|
| Lipid transport | 0.012 | ABCA9, RBP4, CD36 |
| Lipid localization | 0.015 | ABCA9, RBP4, CD36 |
| Secretion | 0.022 | MEG3, RBP4, STC1, CD36 |
| System process | 0.024 | EYA4, OR2L8, MEG3, RBP4, STC1 |
| Positive regulation: molecular mediator of immune response | 0.037 | RBP4, CD36 |
| Establishment of localization | 0.040 | ABCA9, GEM, MEG3, RBP4, STC1, CLIC3, CD36 |
| Anion transport | 0.042 | STC1, CLIC3, CD36 |
| Gene | Fold Change | Function |
|---|---|---|
| MEG3 | 2.93 | Growth suppressor in tumor cells and cell growth activator for p53 and cell apoptosis |
| RBP4 | 2.38 | Delivers retinol from the liver stores to the peripheral tissues |
| LOC101928395 | 2.22 | NA |
| SORCS2 | 2.02 | Represents the only module of the luminal/extracellular moiety Exhibit disparate functions depending on its proteolytic processing |
| LINC01111 | 1.97 | NA |
| MIR2355 | 1.91 | NA |
| MIR520D | 1.86 | Regulation of malignancy and maintaining p53 upregulation |
| ZFY | 1.80 | Function as a transcription factor |
| CD36 | 1.80 | Function as receptors engaged in platelet adhesion to collagen Initiates signal transduction and internalization of receptor–ligand complexes. |
| STC1 | 1.79 | Regulation of renal and intestinal calcium and phosphate transport, cell metabolism, or cellular calcium/phosphate homeostasis. |
| CLIC3 | −2.02 | Regulator of a recycling pathway and regulates cell migration and invasion |
| MIR4520–2 | −1.70 | NA |
| OR2L8 | −1.61 | Responsible for the recognition/G protein-mediated transduction of odorant signals. |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gupta, H.; Youn, G.S.; Han, S.H.; Shin, M.J.; Yoon, S.J.; Han, D.H.; Lee, N.Y.; Kim, D.J.; Baik, S.K.; Suk, K.T. Response-Related Factors of Bone Marrow-Derived Mesenchymal Stem Cells Transplantation in Patients with Alcoholic Cirrhosis. J. Clin. Med. 2019, 8, 862. https://doi.org/10.3390/jcm8060862
Gupta H, Youn GS, Han SH, Shin MJ, Yoon SJ, Han DH, Lee NY, Kim DJ, Baik SK, Suk KT. Response-Related Factors of Bone Marrow-Derived Mesenchymal Stem Cells Transplantation in Patients with Alcoholic Cirrhosis. Journal of Clinical Medicine. 2019; 8(6):862. https://doi.org/10.3390/jcm8060862
Chicago/Turabian StyleGupta, Haripriya, Gi Soo Youn, Sang Hak Han, Min Jea Shin, Sang Jun Yoon, Dae Hee Han, Na Young Lee, Dong Joon Kim, Soon Koo Baik, and Ki Tae Suk. 2019. "Response-Related Factors of Bone Marrow-Derived Mesenchymal Stem Cells Transplantation in Patients with Alcoholic Cirrhosis" Journal of Clinical Medicine 8, no. 6: 862. https://doi.org/10.3390/jcm8060862