Impact of Cefotaxime Non-susceptibility on the Clinical Outcomes of Bacteremic Pneumococcal Pneumonia

 ,
,
Abstract
:1. Introduction
2. Methods
2.1. Ethics Statement
2.2. Study Design and Patients
2.3. Data Collection and Evaluation
2.4. Definitions
2.5. Microbiological Evaluation and Diagnostic Criteria
2.6. Statistical Analysis
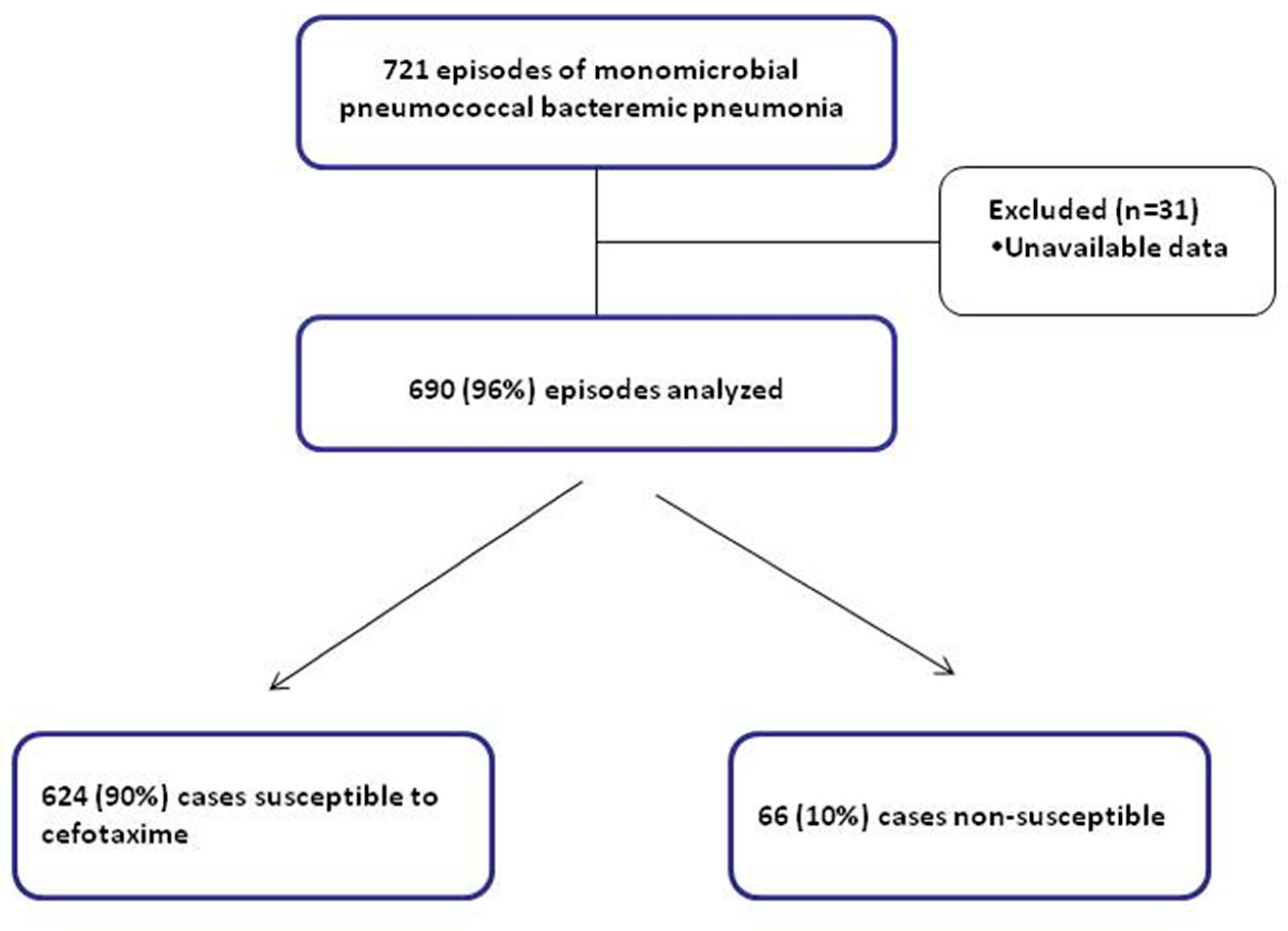
3. Results
3.1. Patients’ Characteristics
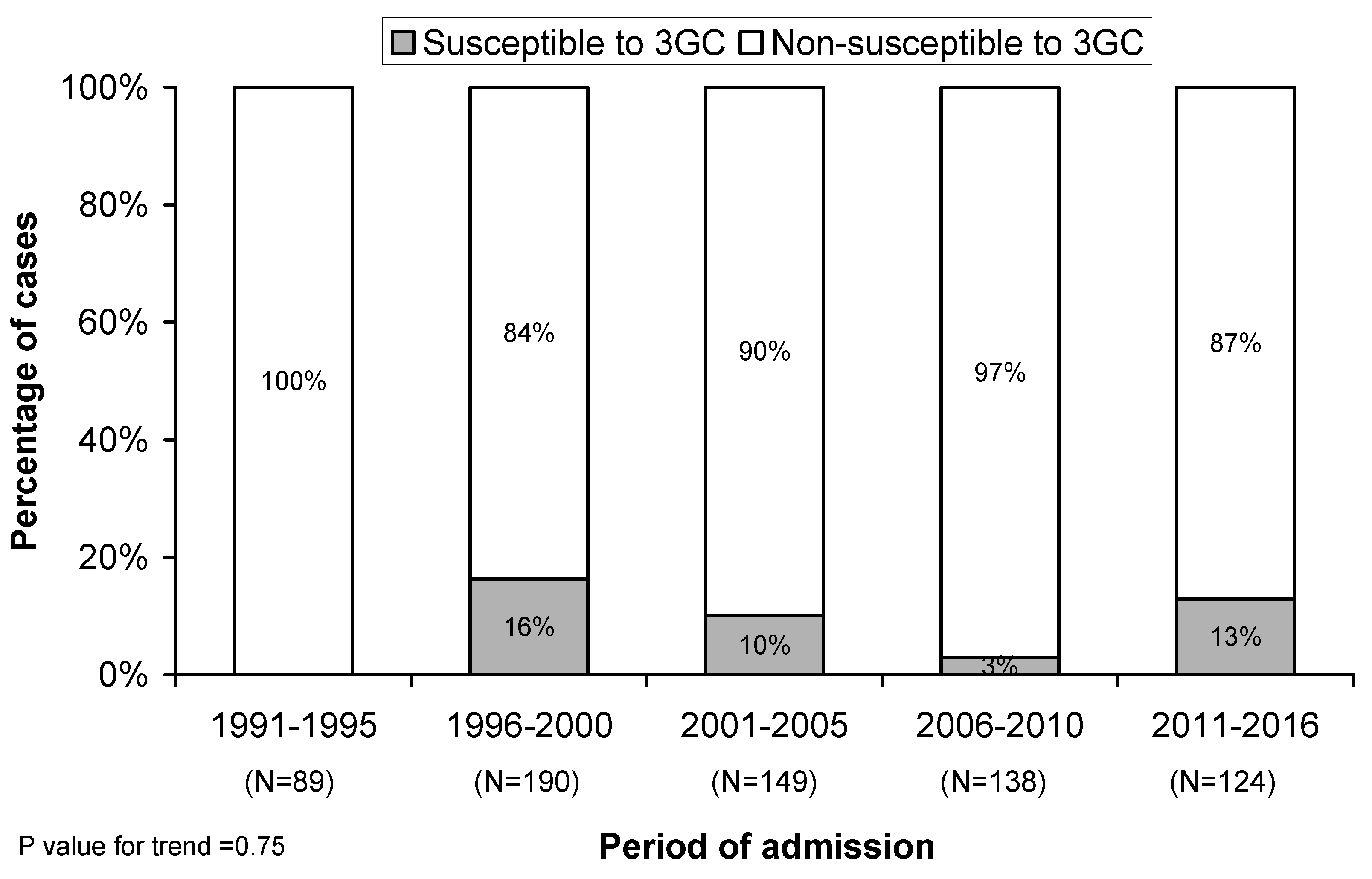
3.2. Microbiology
3.3. Clinical Outcomes
3.4. Factors Associated with 30-Day Mortality
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Feldman, C.; Anderson, R. The Role of Streptococcus pneumoniae in Community-Acquired Pneumonia. Semin. Respir. Crit. Care Med. 2016, 37, 806–818. [Google Scholar] [PubMed] [Green Version]
- Ardanuy, C.; Marimón, J.M.; Calatayud, L.; Giménez, M.; Alonso, M.; Grau, I.; Pallarés, R.; Pérez-Trallero, E.; Liñares, J. Epidemiology of invasive pneumococcal disease in older people in Spain (2007–2009): Implications for future vaccination strategies. PLoS ONE 2012, 7, e43619. [Google Scholar] [CrossRef] [PubMed]
- Feldman, C.; Anderson, R. Epidemiology, virulence factors and management of the pneumococcus. F1000Research 2016, 5, 2320. [Google Scholar] [CrossRef] [PubMed]
- Said, M.A.; Johnson, H.L.; Nonyane, B.A.S.; Deloria-Knoll, M.; O’Brien, K.L.; AGEDD Adult Pneumococcal Burden Study Team; Andreo, F.; Beovic, B.; Blanco, S.; Boersma, W.G.; et al. Estimating the burden of pneumococcal pneumonia among adults: A systematic review and meta-analysis of diagnostic techniques. PLoS ONE 2013, 8, e60273. [Google Scholar] [CrossRef] [PubMed]
- Kim, L.; McGee, L.; Tomczyk, S.; Beall, B. Biological and Epidemiological Features of Antibiotic-Resistant Streptococcus pneumoniae in Pre- and Post-Conjugate Vaccine Eras: A United States Perspective. Clin. Microbiol. Rev. 2016, 29, 525–552. [Google Scholar] [CrossRef]
- Cillóniz, C.; Ardanuy, C.; Vila, J.; Torres, A. What is the clinical relevance of drug-resistant pneumococcus? Curr. Opin. Pulm. Med. 2016, 22, 227–234. [Google Scholar] [CrossRef] [PubMed]
- Keller, L.E.; Robinson, D.A.; McDaniel, L.S. Nonencapsulated Streptococcus pneumoniae: Emergence and Pathogenesis. mBio 2016, 7, e01792. [Google Scholar] [CrossRef]
- Ciruela, P.; Izquierdo, C.; Broner, S.; Muñoz-Almagro, C.; Hernández, S.; Ardanuy, C.; Pallarés, R.; Domínguez, A.; Jané, M. Catalan Working Group on Invasive Pneumococcal Disease The changing epidemiology of invasive pneumococcal disease after PCV13 vaccination in a country with intermediate vaccination coverage. Vaccine 2018, 36, 7744–7752. [Google Scholar] [CrossRef]
- Vila-Corcoles, A.; Ochoa-Gondar, O.; Hospital, I.; de Diego, C.; Satué, E.; Bladé, J.; Ansa, X.; Guzmán, J.A.; Salsench, E.; Ramos, F. Pneumococcal vaccination coverages among low-, intermediate-, and high-risk adults in Catalonia. Hum. Vaccin. Immunother. 2016, 12, 2953–2958. [Google Scholar] [CrossRef] [Green Version]
- Tacconelli, E. Global Priority List of Antibiotic-Resistant Bacteria to Guide Research, Discovery and Development of New Antibiotics; WHO: Geneva, Switzerland, 2017; pp. 1–7.
- Cilloniz, C.; Albert, R.K.; Liapikou, A.; Gabarrus, A.; Rangel, E.; Bello, S.; Marco, F.; Mensa, J.; Torres, A. The Effect of Macrolide Resistance on the Presentation and Outcome of Patients Hospitalized for Streptococcus pneumoniae Pneumonia. Am. J. Respir. Crit. Care Med. 2015, 191, 1265–1272. [Google Scholar] [CrossRef]
- Lynch, J.P.; Zhanel, G.G. Streptococcus pneumoniae: Does antimicrobial resistance matter? Semin. Respir. Crit. Care Med. 2009, 30, 210–238. [Google Scholar] [CrossRef] [PubMed]
- McCabe, W.R.; Jackson, G.G. Gram-Negative Bacteremia: I. Etiology and Ecology. Arch. Intern. Med. 1962, 110, 847–853. [Google Scholar] [CrossRef]
- Fine, M.J.; Auble, T.E.; Yealy, D.M.; Hanusa, B.H.; Weissfeld, L.A.; Singer, D.E.; Coley, C.M.; Marrie, T.J.; Kapoor, W.N. A prediction rule to identify low-risk patients with community-acquired pneumonia. N. Engl. J. Med. 1997, 336, 243–250. [Google Scholar] [CrossRef] [PubMed]
- Dellinger, R.P.; Levy, M.M.; Carlet, J.M.; Bion, J.; Parker, M.M.; Jaeschke, R.; Reinhart, K.; Angus, D.C.; Brun-Buisson, C.; Beale, R.; et al. Surviving Sepsis Campaign: international guidelines for management of severe sepsis and septic shock: 2008. Intensive Care Med. 2008, 34, 17–60. [Google Scholar] [CrossRef] [PubMed]
- Hosmer, D.W.; Lemesshow, S.T.J. Applied Logistic Regression; Hosmer, D.W., Lemeshow, S., Eds.; Wiley: New York, NY, USA, 1989; xiii + 307. [Google Scholar]
- David, C. Modelling Binary Data; Chapman and Hall: London, UK, 1991. [Google Scholar]
- Efron, B.; Tibshirani, R.J. An Introduction to the Bootstrap; CRC Press: Boca Raton, FL, USA, 1994. [Google Scholar]
- Feldman, C.; Anderson, R. Recent advances in our understanding of Streptococcus pneumoniae infection. F1000Prime Rep. 2014, 6, 82. [Google Scholar] [CrossRef] [PubMed]
- Mandell, L.A.; Wunderink, R.G.; Anzueto, A.; Bartlett, J.G.; Campbell, G.D.; Dean, N.C.; Dowell, S.F.; File, T.M.; Musher, D.M.; Niederman, M.S.; et al. Infectious Diseases Society of America/American Thoracic Society consensus guidelines on the management of community-acquired pneumonia in adults. Clin. Infect. Dis. 2007, 44, S27–S72. [Google Scholar] [CrossRef] [PubMed]
- Lim, W.S.; Baudouin, S.V.; George, R.C.; Hill, A.T.; Jamieson, C.; Le Jeune, I.; Macfarlane, J.T.; Read, R.C.; Roberts, H.J.; Levy, M.L.; et al. BTS guidelines for the management of community acquired pneumonia in adults: Update 2009. Thorax 2009, 64, iii1–iii55. [Google Scholar] [CrossRef] [PubMed]
- Cassiolato, A.P.; Almeida, S.C.G.; Andrade, A.L.; Minamisava, R.; de Cunto Brandileone, M.C. Expansion of the multidrug-resistant clonal complex 320 among invasive Streptococcus pneumoniae serotype 19A after the introduction of a ten-valent pneumococcal conjugate vaccine in Brazil. PLoS ONE 2018, 13, e0208211. [Google Scholar] [CrossRef] [PubMed]
- Càmara, J.; Cubero, M.; Martín-Galiano, A.J.; García, E.; Grau, I.; Nielsen, J.B.; Worning, P.; Tubau, F.; Pallarés, R.; Domínguez, M.Á.; et al. Evolution of the β-lactam-resistant Streptococcus pneumoniae PMEN3 clone over a 30 year period in Barcelona, Spain. J. Antimicrob. Chemother. 2018, 73, 2941–2951. [Google Scholar] [CrossRef]
- Song, J.H.; Jung, S.I.; Ko, K.S.; Kim, N.Y.; Son, J.S.; Chang, H.H.; Ki, H.K.; Oh, W.S.; Suh, J.Y.; Peck, K.R.; et al. High prevalence of antimicrobial resistance among clinical Streptococcus pneumoniae isolates in Asia (an ANSORP study). Antimicrob. Agents Chemother. 2004, 48, 2101–2107. [Google Scholar] [CrossRef]
- Verghese, V.P.; Veeraraghavan, B.; Jayaraman, R.; Varghese, R.; Neeravi, A.; Jayaraman, Y.; Thomas, K.; Mehendale, S.M. Increasing incidence of penicillin- and cefotaxime-resistant Streptococcus pneumoniae causing meningitis in India: Time for revision of treatment guidelines? Indian J. Med. Microbiol. 2017, 35, 228–236. [Google Scholar] [PubMed]
- Mehl, A.; Åsvold, B.O.; Kümmel, A.; Lydersen, S.; Paulsen, J.; Haugan, I.; Solligård, E.; Damås, J.K.; Harthug, S.; Edna, T.H. Trends in antimicrobial resistance and empiric antibiotic therapy of bloodstream infections at a general hospital in Mid-Norway: A prospective observational study. BMC Infect. Dis. 2017, 17, 116. [Google Scholar]
- Brett, M.S. Emergence of a high-level cefotaxime-resistant Streptococcus pneumoniae strain in New Zealand. J. Med. Microbiol. 2001, 50, 173–176. [Google Scholar] [CrossRef] [Green Version]
- Moroney, J.F.; Fiore, A.E.; Harrison, L.H.; Patterson, J.E.; Farley, M.M.; Jorgensen, J.H.; Phelan, M.; Facklam, R.R.; Cetron, M.S.; Breiman, R.F.; et al. Clinical outcomes of bacteremic pneumococcal pneumonia in the era of antibiotic resistance. Clin. Infect. Dis. 2001, 33, 797–805. [Google Scholar] [CrossRef] [PubMed]
- Song, J.S.; Choe, P.G.; Song, K.H.; Park, W.B.; Park, S.W.; Kim, H.B.; Oh, M.D.; Kim, E.C.; Kim, N.J. Risk factors for 30-day mortality in adult patients with pneumococcal bacteraemia, and the impact of antimicrobial resistance on clinical outcomes. Epidemiol. Infect. 2012, 140, 1267–1276. [Google Scholar] [CrossRef] [PubMed]
- Choi, S.H.; Chung, J.W.; Sung, H.; Kim, M.N.; Kim, S.H.; Lee, S.O.; Kim, Y.S.; Woo, J.H.; Choi, S.H. Impact of penicillin nonsusceptibility on clinical outcomes of patients with nonmeningeal Streptococcus pneumoniae bacteremia in the era of the 2008 clinical and laboratory standards institute penicillin breakpoints. Antimicrob. Agents Chemother. 2012, 56, 4650–4655. [Google Scholar] [CrossRef] [PubMed]
- Craig, W.A. Interrelationship between pharmacokinetics and pharmacodynamics in determining dosage regimens for broad-spectrum cephalosporins. Diagn. Microbiol. Infect. Dis. 1995, 22, 89–96. [Google Scholar] [CrossRef]
- Beatty, J.A.; Majumdar, S.R.; Tyrrell, G.J.; Marrie, T.J.; Eurich, D.T. Prognostic factors associated with mortality and major in-hospital complications in patients with bacteremic pneumococcal pneumonia: Population-based study. Medicine (Baltimore) 2016, 95, e5179. [Google Scholar] [CrossRef]
- Fica, A.; Bunster, N.; Aliaga, F.; Olivares, F.; Porte, L.; Braun, S.; Dabanch, J.; Hormázabal, J.C.; Hernández, A.; Benavides, M.G. Bacteremic pneumococcal pneumonia: serotype distribution, antimicrobial susceptibility, severity scores, risk factors and mortality in a single center in Chile. Braz. J. Infect. Dis. 2014, 18, 115–123. [Google Scholar] [CrossRef]
- Naucler, P.; Darenberg, J.; Morfeldt, E.; Ortqvist, A.; Henriques Normark, B. Contribution of host, bacterial factors and antibiotic treatment to mortality in adult patients with bacteraemic pneumococcal pneumonia. Thorax 2013, 68, 571–579. [Google Scholar] [CrossRef] [Green Version]
- Niederman, M.S.; Bass, J.B.; Campbell, G.D.; Fein, A.M.; Grossman, R.F.; Mandell, L.A.; Marrie, T.J.; Sarosi, G.A.; Torres, A.; Yu, V.L. Guidelines for the initial management of adults with community-acquired pneumonia: diagnosis, assessment of severity and initial antimicrobial therapy. American Thoracic Society. Medical Section of the American Lung Association. Am. Rev. Respir. Dis. 1993, 148, 1418–1426. [Google Scholar] [CrossRef] [PubMed]
- Bartlett, J.G.; Breiman, R.F.; Mandell, L.A.; File, T.M. Community-acquired pneumonia in adults: Guidelines for management. The Infectious Diseases Society of America. Clin. Infect. Dis. 1998, 26, 811–838. [Google Scholar] [CrossRef] [PubMed]
- Niederman, M.S.; Mandell, L.A.; Anzueto, A.; Bass, J.B.; Broughton, W.A.; Campbell, G.D.; Dean, N.; File, T.; Fine, M.J.; Gross, P.A.; et al. Guidelines for the management of adults with community-acquired pneumonia. Diagnosis, assessment of severity, antimicrobial therapy, and prevention. Am. J. Respir. Crit. Care Med. 2001, 163, 1730–1754. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Non-Susceptible to 3GC (N = 66) | Susceptible to 3GC (N = 624) | p-Value | |
|---|---|---|---|
| Age, years, mean (SD) | 67 (20) | 59 (19) | 0.001 |
| Age > 65 years, n (%) | 42 (64) | 267 (43) | 0.001 |
| Male, gender, n (%) | 38 (58) | 401 (64) | 0.28 |
| Current alcohol user, n (%) | 4 (6) | 34 (5) | 0.78 |
| Previous antimicrobials, n (%) | 4 (6) | 19 (3) | 0.26 |
| Shock, n (%) | 8 (12) | 85 (14) | 0.73 |
| Previous systemic steroids, n (%) | 4 (6) | 50 (8) | 0.54 |
| Mechanical ventilation, n (%) | 0 | 4 (1) | >0.99 |
| Fever, n (%) | 63 (95) | 605 (97) | 0.42 |
| Comorbidities, n (%) | |||
| COPD | 17 (26) | 128 (21) | 0.32 |
| HIV | 14 (21) | 122 (20) | 0.75 |
| Neoplasm | 14 (21) | 98 (16) | 0.25 |
| Chronic cardiovascular disease | 9 (14) | 59 (9) | 0.28 |
| Diabetes mellitus | 15 (23) | 96 (15) | 0.12 |
| Chronic renal disease | 3 (5) | 30 (5) | >0.99 |
| Chronic liver disease | 10 (15) | 74 (12) | 0.44 |
| Empiric therapy | |||
| Cephalosporin monotherapy | 19 (29) | 164 (26) | |
| Cephalosporin + quinolone Cephalosporin + macrolide | 10 (15) 37 (56) | 147 (24) 313 (50) | 0.16 0.12 |
| McCabe score | 0.73 | ||
| 1 | 43 (66) | 438 (71) | |
| 2 | 21 (32) | 174 (28) | |
| 3 | 1 (2) | 7 (1) | |
| PSI score | 0.11 | ||
| PSI I–III | 8 (32) | 140 (49) | |
| PSI IV–V | 17 (68) | 147 (51) | |
| 30-day mortality, n (%) | 5 (8) | 42 (7) | 0.80 |
| Variable | Univariate a | Multivariable b,c | ||||
|---|---|---|---|---|---|---|
| OR | 95% CI | p-Value | OR | 95% CI | p-Value | |
| Non-susceptible to 3GC | 1.13 | 0.43–2.96 | 0.81 | 0.83 | 0.28–2.50 | 0.74 |
| Age (+1 year) | 1.03 | 1.01–1.05 | 0.001 | 1.04 | 1.02–1.06 | <0.001 |
| Septic shock | 13.01 | 6.89–24.59 | <0.001 | 17.54 | 8.72–35.27 | <0.001 |
| Chronic renal disease | 3.89 | 1.05–14.46 | 0.042 | - | - | - |
| Chronic liver disease | 2.37 | 1.16–4.86 | 0.019 | 2.33 | 0.94–5.75 | 0.068 |
| McCabe score d | 0.009 | 0.061 | ||||
| 1 | 1.00 | - | - | 1.00 | - | - |
| 2 | 1.45 | 0.76–2.74 | 0.26 | 1.32 | 0.60–2.89 | 0.49 |
| 3 | 9.66 | 2.20–42.51 | 0.003 | 8.72 | 1.43–53.00 | 0.019 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cillóniz, C.; de la Calle, C.; Dominedò, C.; García-Vidal, C.; Cardozo, C.; Gabarrús, A.; Marco, F.; Torres, A.; Soriano, A. Impact of Cefotaxime Non-susceptibility on the Clinical Outcomes of Bacteremic Pneumococcal Pneumonia. J. Clin. Med. 2019, 8, 1150. https://doi.org/10.3390/jcm8081150
Cillóniz C, de la Calle C, Dominedò C, García-Vidal C, Cardozo C, Gabarrús A, Marco F, Torres A, Soriano A. Impact of Cefotaxime Non-susceptibility on the Clinical Outcomes of Bacteremic Pneumococcal Pneumonia. Journal of Clinical Medicine. 2019; 8(8):1150. https://doi.org/10.3390/jcm8081150
Chicago/Turabian StyleCillóniz, Catia, Cristina de la Calle, Cristina Dominedò, Carolina García-Vidal, Celia Cardozo, Albert Gabarrús, Francesc Marco, Antoni Torres, and Alex Soriano. 2019. "Impact of Cefotaxime Non-susceptibility on the Clinical Outcomes of Bacteremic Pneumococcal Pneumonia" Journal of Clinical Medicine 8, no. 8: 1150. https://doi.org/10.3390/jcm8081150