Safety and Activity of Metronomic Temozolomide in Second-Line Treatment of Advanced Neuroendocrine Neoplasms


 ,
,  , ,
, , 
Abstract
:1. Introduction
2. Experimental Section
2.1. Patients, Treatment and Disease Characteristics
2.2. Activity, Toxicity and Clinical Benefit Evaluations
2.3. Time-to-Outcome Analysis and Statistical Methods
3. Results
Efficacy and Safety
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Dasari, A.; Shen, C.; Halperin, D.; Zhao, B.; Zhou, S.; Xu, Y.; Shih, T.; Yao, J.C. Trends in the Incidence, Prevalence, and Survival Outcomes in Patients with Neuroendocrine Tumors in the United States. JAMA Oncol. 2017, 3, 1335–1342. [Google Scholar] [CrossRef] [PubMed]
- National Comprehensive Cancer Network. Neuroendocrine and Adrenal Tumor (Version 2.2018). Available online: https://www.nccn.org/professionals/physician_gls/PDF/neuroendocrine.pdf (accessed on 2 August 2019).
- Hallet, J.; Law, C.H.; Cukier, M.; Saskin, R.; Liu, N.; Singh, S. Exploring the rising incidence of neuroendocrine tumors: A population–based analysis of epidemiology, metastatic presentation, and outcomes. Cancer 2015, 121, 589–597. [Google Scholar] [CrossRef] [PubMed]
- Pavel, M.; Costa, F.; Capdevila, J.; Gross, D.; Kianmanesh, R.; Krenning, E.; Knigge, U.; Salazar, R.; Pape, U.F.; Öberg, K. ENETS Consensus Guidelines Update for the Management of Distant Metastatic Disease of Intestinal, Pancreatic, Bronchial Neuroendocrine Neoplasms (NEN) and NEN of Unknown Primary Site. Neuroendocrinology 2016, 103, 172–185. [Google Scholar] [CrossRef] [PubMed]
- Strosberg, J.R.; Halfdanarson, T.R.; Bellizzi, A.M.; Chan, J.A.; Dillon, J.S.; Heaney, A.P.; Kunz, P.L.; O’Dorisio, T.M.; Salem, R.; Segelov, E.; et al. The North American Neuroendocrine Tumor Society Consensus Guidelines for Surveillance and Medical Management of Midgut Neuroendocrine Tumors. Pancreas 2017, 46, 707–714. [Google Scholar] [CrossRef] [PubMed]
- Ekeblad, S.; Sundin, A.; Janson, E.T.; Welin, S.; Granberg, D.; Kindmark, H.; Dunder, K.; Kozlovacki, G.; Örlefors, H.; Sigurd, M.; et al. Temozolomide as monotherapy is effective in treatment of advanced malignant neuroendocrine tumors. Clin. Cancer Res. 2007, 13, 2986–2991. [Google Scholar] [CrossRef] [PubMed]
- Olsen, I.H.; Sørensen, J.B.; Federspiel, B.; Kjaer, A.; Hansen, C.P.; Knigge, U.; Langer, S.W. Temozolomide as second or third line treatment of patients with neuroendocrine carcinomas. Sci. World J. 2012, 2012, 170496. [Google Scholar] [CrossRef] [PubMed]
- Strosberg, J.R.; Fine, R.L.; Choi, J.; Nasir, A.; Coppola, D.; Chen, D.T.; Helm, J.; Kvols, L. First-line chemotherapy with capecitabine and temozolomide in patients with metastatic pancreatic endocrine carcinomas. Cancer 2011, 117, 268–275. [Google Scholar] [CrossRef]
- Welin, S.; Sorbye, H.; Sebjornsen, S.; Knappskog, S.; Busch, C.; Öberg, K. Clinical effect of temozolomide–based chemotherapy in poorly differentiated endocrine carcinoma after progression on first–line chemotherapy. Cancer 2011, 117, 4617–4622. [Google Scholar] [CrossRef]
- Saif, M.W.; Kaley, K.; Brennan, M.; Garcon, M.C.; Rodriguez, G.; Rodriguez, T. A retrospective study of capecitabine/temozolomide (CAPTEM) regimen in the treatment of metastatic pancreatic neuroendocrine tumors (pNETs) after failing previous therapy. JOP 2013, 14, 498–501. [Google Scholar]
- Fine, R.L.; Gulati, A.P.; Krantz, B.A.; Moss, R.A.; Schreibman, S.; Tsushima, D.A.; Mowatt, K.B.; Dinnen, R.D.; Mao, Y.; Stevens, P.D.; et al. Capecitabine and temozolomide (CAPTEM) for metastatic, well–differentiated neuroendocrine cancers: The Pancreas Center at Columbia University experience. Cancer Chemother. Pharmacol. 2013, 71, 663–670. [Google Scholar] [CrossRef]
- Saranga–Perry, V.; Morse, B.; Centeno, B.; Kvols, L.; Strosberg, J. Treatment of metastatic neuroendocrine tumors of the thymus with capecitabine and temozolomide: A case series. Neuroendocrinology 2013, 97, 318–321. [Google Scholar] [CrossRef] [PubMed]
- Chan, J.A.; Blaszkowsky, L.; Stuart, K.; Zhu, A.X.; Allen, J.; Wadlow, R.; Ryan, D.P.; Meyerhardt, J.; Gonzalez, M.; Regan, E.; et al. A prospective, phase 1/2 study of everolimus and temozolomide in patients with advanced pancreatic neuroendocrine tumor. Cancer 2013, 119, 3212–3218. [Google Scholar] [CrossRef] [PubMed]
- Koumarianou, A.; Antoniou, S.; Kanakis, G.; Economopoulos, N.; Rontogianni, D.; Ntavatzikos, A.; Tsavaris, N.; Pectasides, D.; Dimitriadis, G.; Kaltsas, G. Combination treatment with metronomic temozolomide, bevacizumab and long–acting octreotide for malignant neuroendocrine tumors. Endocr. Relat. Cancer 2012, 19, L1–L4. [Google Scholar] [CrossRef] [PubMed]
- Chan, J.A.; Stuart, K.; Earle, C.C.; Clark, J.W.; Bhargava, P.; Miksad, R.; Blaszkowsky, L.; Enzinger, P.C.; Meyerhardt, J.A.; Zheng, H.; et al. Prospective study of bevacizumab plus temozolomide in patients with advanced neuroendocrine tumors. J. Clin. Oncol. 2012, 30, 2963–2968. [Google Scholar] [CrossRef] [PubMed]
- Kulke, M.H.; Stuart, K.; Enzinger, P.C.; Ryan, D.P.; Clark, J.W.; Muzikansky, A.; Vincitore, M.; Michelini, A.; Fuchs, C.S. Phase II study of temozolomide and thalidomide in patients with metastatic neuroendocrine tumors. J. Clin. Oncol. 2006, 24, 401–406. [Google Scholar] [CrossRef] [PubMed]
- Kurzen, H.; Schmitt, S.; Näher, H.; Möhler, T. Inhibition of angiogenesis by non–toxic doses of temozolomide. Anticancer Drugs 2003, 14, 515–522. [Google Scholar] [CrossRef] [PubMed]
- Sun, C.; Yu, Y.; Wang, L.; Wu, B.; Xia, L.; Feng, F.; Ling, Z.; Wang, S. Additive antiangiogenesis effect of ginsenoside Rg3 with low–dose metronomic temozolomide on rat glioma cells both in vivo and in vitro. J. Exp. Clin. Cancer Res. 2016, 35, 32. [Google Scholar] [CrossRef] [PubMed]
- Woo, J.Y.; Yang, S.H.; Lee, Y.S.; Lee, S.Y.; Kim, J.; Hong, Y.K. Continuous Low–Dose Temozolomide Chemotherapy and Microvessel Density in Recurrent Glioblastoma. J. Korean Neurosurg. Soc. 2015, 58, 426–431. [Google Scholar] [CrossRef]
- Kaneno, R.; Shurin, G.V.; Tourkova, I.L.; Shurin, M.R. Chemomodulation of human dendritic cell function by antineoplastic agents in low noncytotoxic concentrations. J. Transl. Med. 2009, 7, 58. [Google Scholar] [CrossRef]
- Ghiringhelli, F.; Menard, C.; Puig, P.E.; Ladoire, S.; Roux, S.; Martin, F.; Solary, E.; Le Cesne, A.; Zitvogel, L.; Chauffert, B. Metronomic cyclophosphamide regimen selectively depletes CD4+CD25+regulatory T cells and restores T and NK effector functions in end stage cancer patients. Cancer Immunol. Immunother. 2007, 56, 641–648. [Google Scholar] [CrossRef]
- Banissi, C.; Ghiringhelli, F.; Chen, L.; Carpentier, A.F. Treg depletion with a lowdose metronomic temozolomide regimen in a rat glioma model. Cancer Immunol. Immunother. 2009, 58, 1627–1634. [Google Scholar] [CrossRef] [PubMed]
- Zhao, J.; Cao, Y.; Lei, Z.; Yang, Z.; Zhang, B.; Huang, B. Selective depletion of CD4+CD25+Foxp3+ regulatory T cells by low–dose cyclophosphamide is explained by reduced intracellular ATP levels. Cancer Res. 2010, 70, 4850–4858. [Google Scholar] [CrossRef] [PubMed]
- Kan, S.; Hazama, S.; Maeda, K.; Inoue, Y.; Homma, S.; Koido, S.; Okamoto, M.; Oka, M. Suppressive Effects of Cyclophosphamide and Gemcitabine on Regulatory T–Cell Induction In Vitro. Anticancer Res. 2012, 32, 5363–5369. [Google Scholar] [PubMed]
- National Institute of Health. Available online: https://ctep.cancer.gov/protocolDevelopment/electronic_applications/ctc.htm#ctc_40 (accessed on 2 August 2019).
- Girardi, D.M.; Silva, A.C.B.; Rêgo, J.F.M.; Coudry, R.A.; Riechelmann, R.P. Unraveling molecular pathways of poorly differentiated neuroendocrine carcinomas of the gastroenteropancreatic system: A systematic review. Cancer Treat. Rev. 2017, 56, 28–35. [Google Scholar] [CrossRef] [PubMed]
- Fidler, I.J.; Ellis, L.M. Chemotherapeutic drugs—More really is not better. Nat. Med. 2000, 6, 500–502. [Google Scholar] [CrossRef]
- Gatenby, R.A.; Silva, A.S.; Gillies, R.J.; Frieden, B.R. Adaptive Therapy. Cancer Res. 2009, 69, 4894–4903. [Google Scholar] [CrossRef]
- Scharovsky, O.G.; Mainetti, L.E.; Rozados, V.R. Metronomic chemotherapy: Changing the paradigm that more is better. Curr. Oncol. 2009, 16, 7–15. [Google Scholar] [CrossRef]
- Pasquier, E.; Kavallaris, M.; André, N. Metronomic chemotherapy: New rationale for new directions. Nat. Rev. Clin. Oncol. 2010, 7, 455–465. [Google Scholar] [CrossRef]
- Scoazec, J.Y. Angiogenesis in neuroendocrine tumors: Therapeutic applications. Neuroendocrinology 2013, 97, 45–56. [Google Scholar] [CrossRef]
- Besig, S.; Voland, P.; Baur, D.M.; Perren, A.; Prinz, C. Vascular endothelial growth factors, angiogenesis, and survival in human ileal enterochromaffin cell carcinoids. Neuroendocrinology 2009, 90, 402–415. [Google Scholar] [CrossRef]
- Zhang, J.; Jia, Z.; Li, Q.; Wang, L.; Rashid, A.; Zhu, Z.; Evans, D.B.; Vauthey, J.N.; Xie, K.; Yao, J.C. Elevated expression of vascular endothelial growth factor correlates with increased angiogenesis and decreased progression–free survival among patients with low–grade neuroendocrine tumors. Cancer 2007, 109, 1478–1486. [Google Scholar] [CrossRef] [PubMed]
- Zhou, Q.; Guo, P.; Wang, X.; Nuthalapati, S.; Gallo, J.M. Preclinical pharmacokinetic and pharmacodynamic evaluation of metronomic and conventional temozolomide dosing regimens. J. Pharmacol. Exp. Ther. 2007, 321, 265–275. [Google Scholar] [CrossRef] [PubMed]
- Lambrescu, I.; Fica, S.; Martins, D.; Spada, F.; Cella, C.; Bertani, E.; Rubino, M.; Gibelli, B.; Grana, C.; Bonomo, G.; et al. Metronomic and metronomic–like therapies in neuroendocrine tumors—Rationale and clinical perspectives. Cancer Treat. Rev. 2017, 55, 46–56. [Google Scholar] [CrossRef] [PubMed]
- André, N.; Carré, M.; Pasquier, E. Metronomics: Towards personalized chemotherapy? Nat. Rev. Clin. Oncol. 2014, 11, 413–431. [Google Scholar] [CrossRef] [PubMed]
- Figlin, R.A.; Kaufmann, I.; Brechbiel, J. Targeting PI3K and mTORC2 in metastatic renal cell carcinoma: New strategies for overcoming resistance to VEGFR and mTORC1 inhibitors. Int. J. Cancer 2013, 133, 788–796. [Google Scholar] [CrossRef] [PubMed]
- Schmitt, A.M.; Pavel, M.; Rudolph, T.; Dawson, H.; Blank, A.; Komminoth, P.; Vassella, E.; Perren, A. Prognostic and predictive roles of MGMT protein expression and promoter methylation in sporadic pancreatic neuroendocrine neoplasms. Neuroendocrinology 2014, 100, 35–44. [Google Scholar] [CrossRef] [PubMed]
- Walter, T.; van Brakel, B.; Vercherat, C.; Hervieu, V.; Forestier, J.; Chayvialle, J.A. O6–Methylguanine–DNA methyltransferase status in neuroendocrine tumors: Prognostic relevance and association with response to alkylating agents. Br. J. Cancer 2015, 112, 523–531. [Google Scholar] [CrossRef]
- Kulke, M.H.; Hornick, J.L.; Frauenhoffer, C.; Hooshmand, S.; Ryan, D.P.; Enzinger, P.C.; Meyerhardt, J.A.; Clark, J.W.; Stuart, K.; Fuchs, C.S.; et al. O6–methylguanine DNA methyltransferase deficiency and response to temozolomide–based therapy in patients with neuroendocrine tumors. Clin. Cancer Res. 2009, 15, 338–345. [Google Scholar] [CrossRef]
- Raj, N.; Klimstra, D.S.; Horvat, N.; Zhang, L.; Chou, J.F.; Capanu, M.; Basturk, O.; Do, R.K.G.; Allen, P.J.; Reidy-Lagunes, D. O6–Methylguanine DNA Methyltransferase Status Does Not Predict Response or Resistance to Alkylating Agents in Well–Differentiated Pancreatic Neuroendocrine Tumors. Pancreas 2017, 46, 758–763. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Characteristics | No. |
|---|---|
| Age, years | |
| Median | 65 |
| Range | 32–88 |
| Gender | |
| Male | 13 |
| Female | 13 |
| Grading | |
| G1 | 0 |
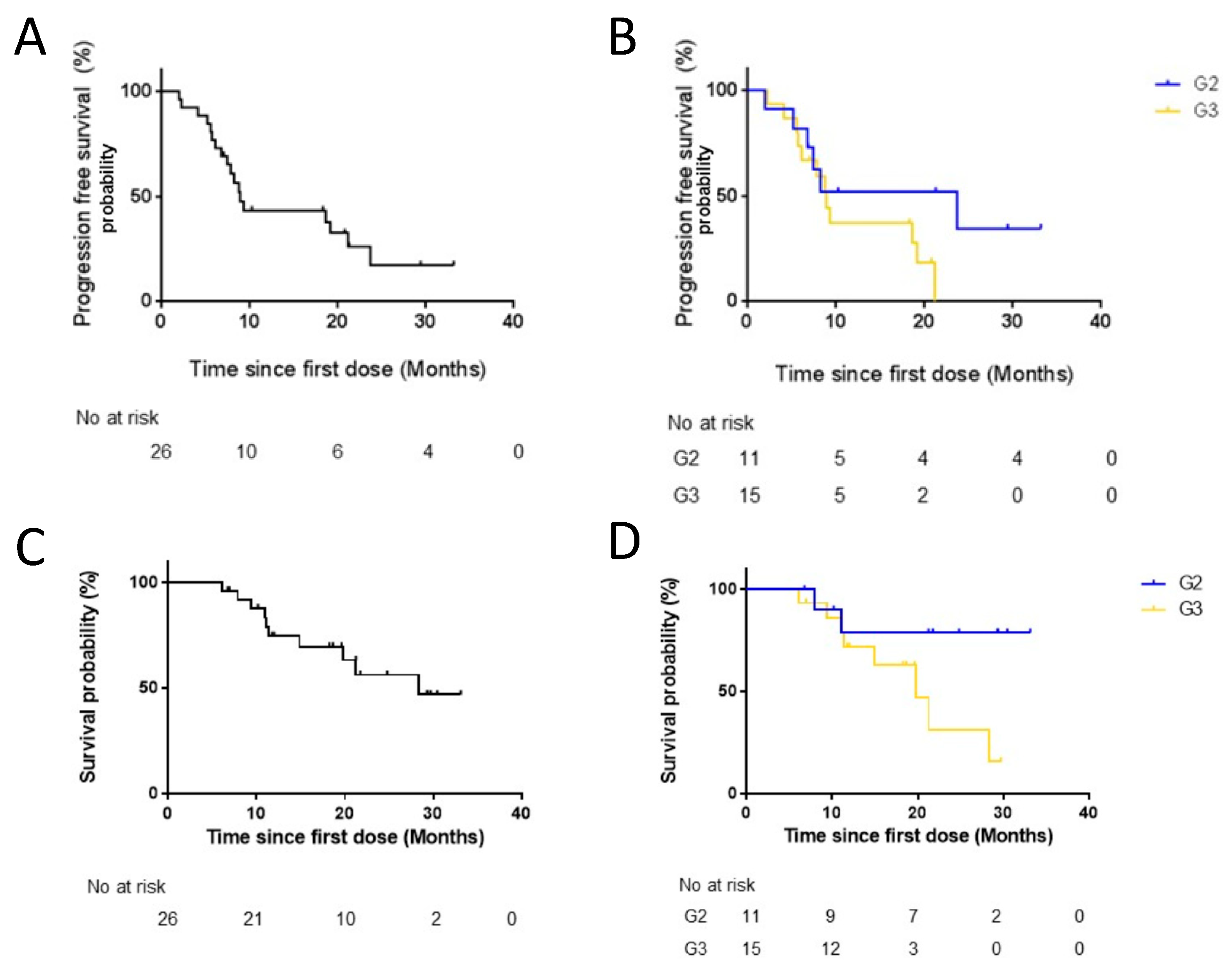
| G2 | 11 |
| G3 * | 15 |
| KI-67 level | |
| 3–20 | 11 |
| 20–55 | 10 |
| >55 | 5 |
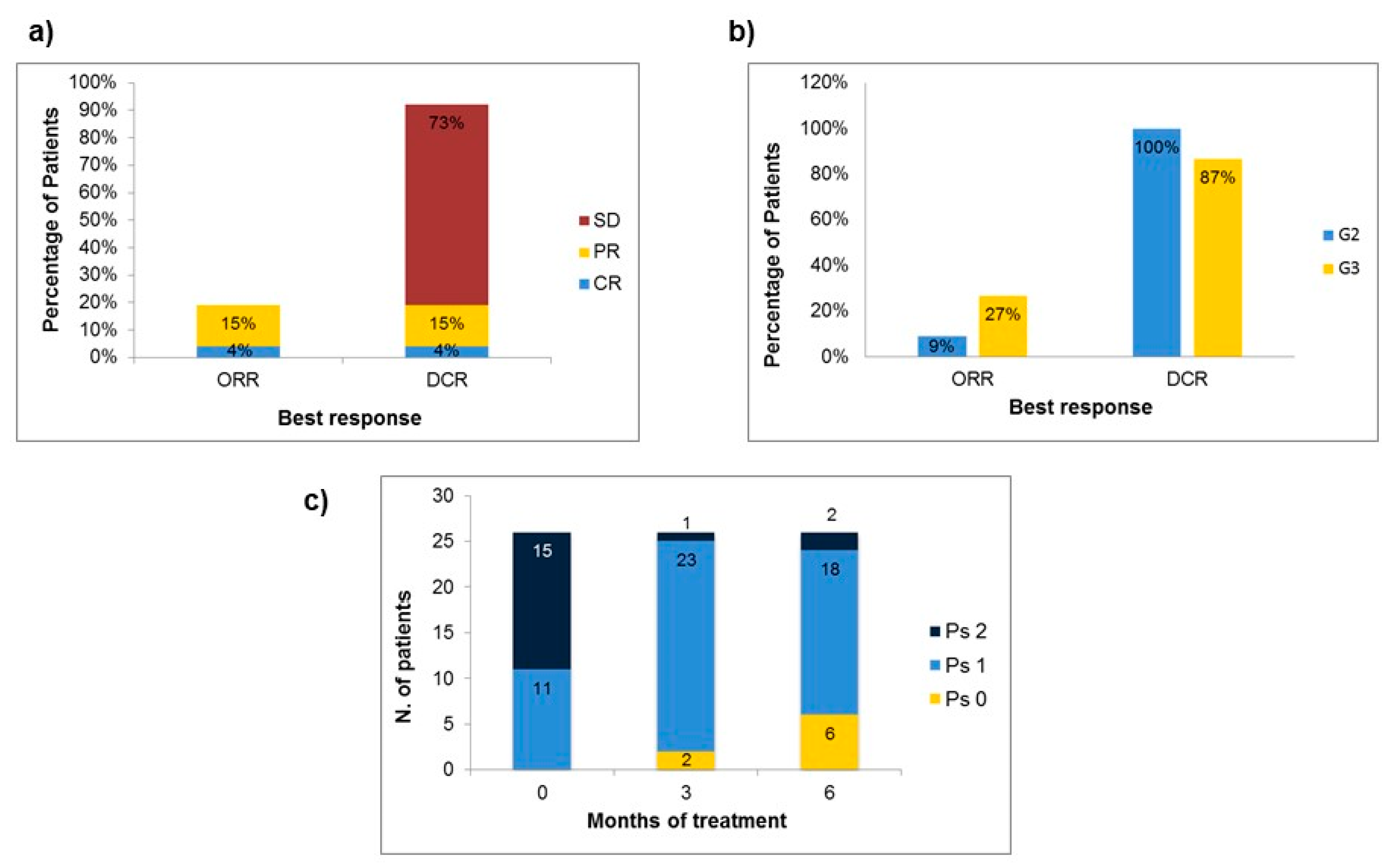
| Performance Status | |
| 0 | 0 |
| 1 | 11 |
| 2 | 15 |
| Site of primary tumor | |
| Pancreas | 5 |
| Lung | 5 |
| Stomach | 3 |
| Miscellanea | |
| Head and Neck | 2 |
| Small bowel | 3 |
| Rectum | 1 |
| Gallbladder | 1 |
| Cutaneous | 1 |
| Unknown Primary Origin | 5 |
| No. of involved metastatic sites | |
| 1 | 13 |
| 2 | 8 |
| ≥3 | 5 |
| Previous treatments | |
| Platinum-based treatments | 12 |
| Chemotherapy non-platinum based | 2 |
| Somatostatin analogues | 8 |
| Clinical trials drugs | 4 |
| Response to Therapy | No. (%) |
|---|---|
| Complete Response | 1 (3.8) |
| Partial Response | 4 (15.4) |
| Stable Disease | 19 (73.1) |
| Progressive Disease | 2 (7.6) |
| Median PFS (18 events) | 9.0 months |
| Median OS (10 events) | 28.3 months |
| Toxicity | G1 | G2 | G3/G4 | |||
|---|---|---|---|---|---|---|
| No | % | No | % | No | % | |
| Anaemia | 11 | 42.3 | 13 | 50.0 | 0 | 0.0 |
| Asthenia | 9 | 34.6 | 12 | 46.1 | 0 | 0.0 |
| Neuropathy | 8 | 30.7 | 10 | 38.4 | 0 | 0.0 |
| Neutropenia | 8 | 30.7 | 8 | 30.7 | 0 | 0.0 |
| Nausea | 7 | 26.9 | 8 | 30.7 | 0 | 0.0 |
| Hyperbilirubinemia | 7 | 26.9 | 6 | 23.1 | 0 | 0.0 |
| Alkaline phosphatase | 3 | 11.5 | 0 | 0.0 | 0 | 0.0 |
| Hyperglycaemia | 4 | 15.3 | 6 | 23.1 | 0 | 0.0 |
| Thrombocytopenia | 0 | 0.0 | 6 | 23.1 | 0 | 0.0 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tafuto, S.; von Arx, C.; Capozzi, M.; Tatangelo, F.; Mura, M.; Modica, R.; Barretta, M.L.; Di Sarno, A.; Tornesello, M.L.; Colao, A.; et al. Safety and Activity of Metronomic Temozolomide in Second-Line Treatment of Advanced Neuroendocrine Neoplasms. J. Clin. Med. 2019, 8, 1224. https://doi.org/10.3390/jcm8081224
Tafuto S, von Arx C, Capozzi M, Tatangelo F, Mura M, Modica R, Barretta ML, Di Sarno A, Tornesello ML, Colao A, et al. Safety and Activity of Metronomic Temozolomide in Second-Line Treatment of Advanced Neuroendocrine Neoplasms. Journal of Clinical Medicine. 2019; 8(8):1224. https://doi.org/10.3390/jcm8081224
Chicago/Turabian StyleTafuto, Salvatore, Claudia von Arx, Monica Capozzi, Fabiana Tatangelo, Manuela Mura, Roberta Modica, Maria Luisa Barretta, Antonella Di Sarno, Maria Lina Tornesello, Annamaria Colao, and et al. 2019. "Safety and Activity of Metronomic Temozolomide in Second-Line Treatment of Advanced Neuroendocrine Neoplasms" Journal of Clinical Medicine 8, no. 8: 1224. https://doi.org/10.3390/jcm8081224