Health Outcomes Associated with Adherence to Antidepressant Use during Acute and Continuation Phases of Depression Treatment among Older Adults with Dementia and Major Depressive Disorder

 , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
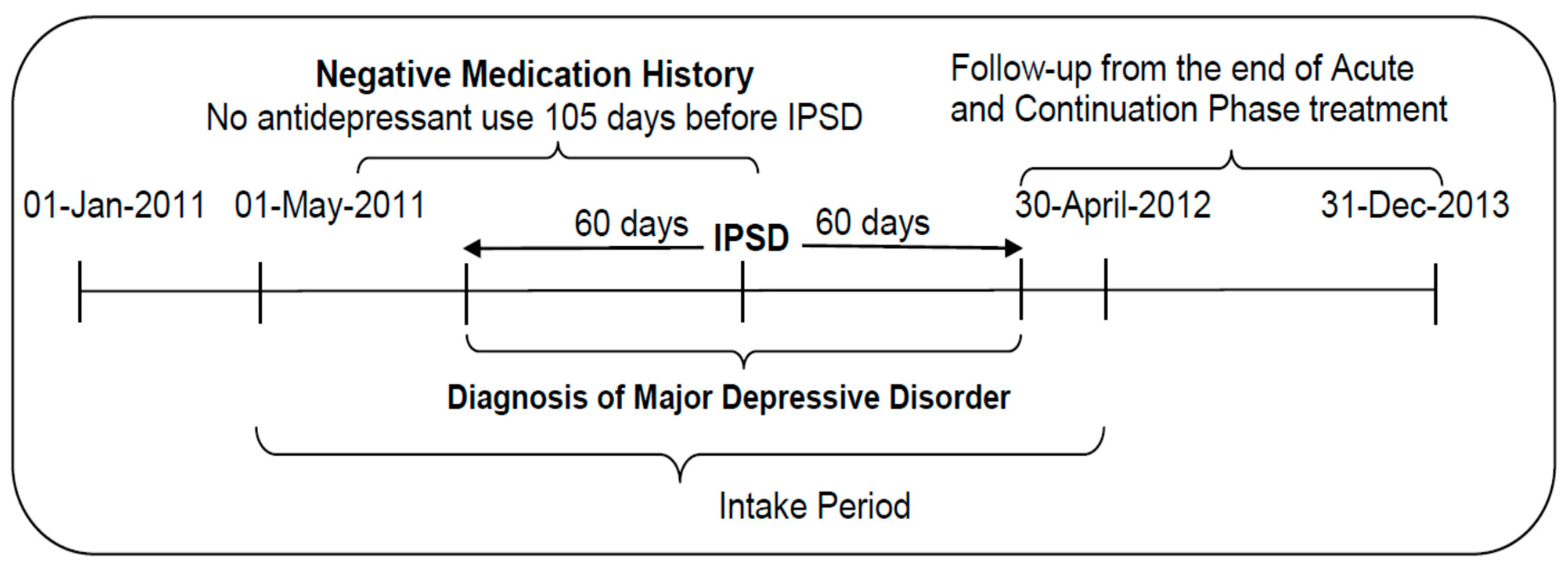
2.1. Study Design
2.2. Data Sources
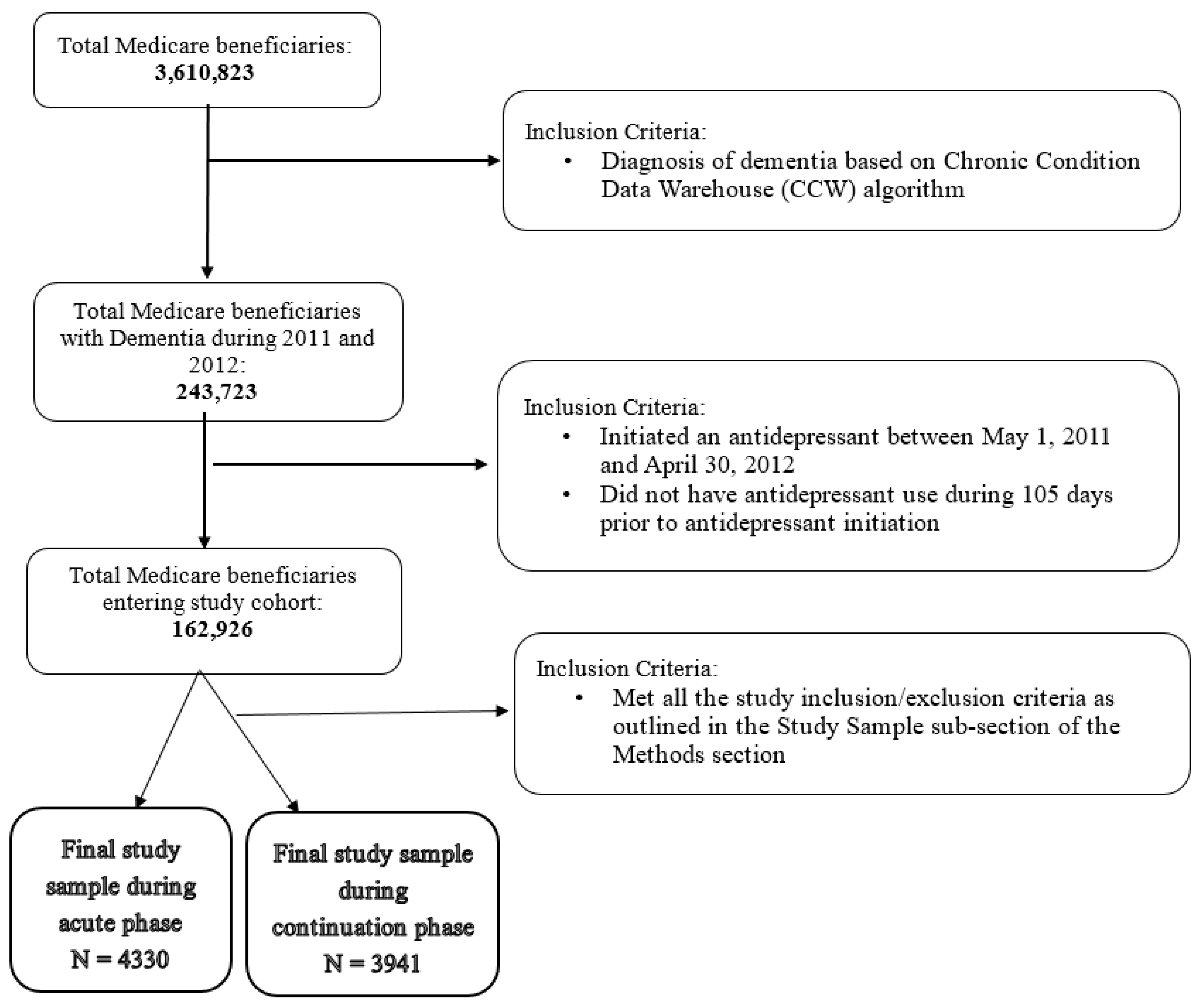
2.3. Study Sample
2.4. Key Independent Variables
2.5. Outcomes of Interest
2.6. Inverse Probability of Treatment Weighting (IPTW)
2.7. Statistical Analysis
2.8. Sensitivity Analysis
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Alzheimer’s Association. 2019 Alzheimer’s Disease Facts and Figures. 2018. Available online: https://www.alz.org/media/documents/alzheimers-facts-and-figures-2019-r.pdf (accessed on 21 June 2020).
- Steinberg, M.; Shao, H.; Zandi, P.; Lyketsos, C.G.; Welsh-Bohmer, K.A.; Norton, M.C.; Breitner, J.C.; Steffens, D.C.; Tschanz, J.T.; Cache County Investigators. Point and 5-year period prevalence of neuropsychiatric symptoms in dementia: The Cache County Study. Int. J. Geriatr. Psychiatry 2008, 23, 170–177. [Google Scholar] [CrossRef] [Green Version]
- Kales, H.C.; Chen, P.; Blow, F.C.; Welsh, D.E.; Mellow, A.M. Rates of clinical depression diagnosis, functional impairment, and nursing home placement in coexisting dementia and depression. Am. J. Geriatr. Psychiatry 2005, 13, 441–449. [Google Scholar] [CrossRef]
- Lyketsos, C.G.; DelCampo, L.; Steinberg, M.; Miles, Q.; Steele, C.D.; Munro, C.; Baker, A.S.; Sheppard, J.M.; Frangakis, C.; Brandt, J.; et al. Treating depression in Alzheimer disease: Efficacy and safety of sertraline therapy, and the benefits of depression reduction: The DIADS. Arch. Gen. Psychiatry 2003, 60, 737–746. [Google Scholar] [CrossRef]
- Wei, Y.J.; Simoni-Wastila, L.; Zuckerman, I.H.; Huang, T.Y.; Brandt, N.; Moyo, P.; Lucas, J.A. Quality of psychopharmacological medication prescribing and mortality in Medicare beneficiaries in nursing homes. J. Am. Geriatr. Soc. 2014, 62, 1490–1504. [Google Scholar] [CrossRef]
- Thompson, S.; Herrmann, N.; Rapoport, M.J.; Lanctôt, K.L. Efficacy and safety of antidepressants for treatment of depression in Alzheimer’s disease: A metaanalysis. Can. J. Psychiatry 2007, 52, 248–255. [Google Scholar] [CrossRef] [Green Version]
- Su, J.A.; Chang, C.C.; Wang, H.M.; Chen, K.J.; Yang, Y.H.; Lin, C.Y. Antidepressant treatment and mortality risk in patients with dementia and depression: A nationwide population cohort study in Taiwan. Ther. Adv. Chronic Dis. 2019. [Google Scholar] [CrossRef]
- Dudas, R.; Malouf, R.; McCleery, J.; Dening, T. Antidepressants for treating depression in dementia. Cochrane Database Syst. Rev. 2018, 8, CD003944. [Google Scholar] [CrossRef]
- Banerjee, S.; Hellier, J.; Dewey, M.; Romeo, R.; Ballard, C.; Baldwin, R.; Bentham, P.; Fox, C.; Holmes, C.; Katona, C; et al. Sertraline or mirtazapine for depression in dementia (HTA-SADD): A randomised, multicentre, double-blind, placebo-controlled trial. Lancet 2011, 378, 403–411. [Google Scholar] [CrossRef]
- Farina, N.; Morrell, L.; Banerjee, S. What is the therapeutic value of antidepressants in dementia? A narrative review. Int. J. Geriatr. Psychiatry 2017, 32, 32–49. [Google Scholar] [CrossRef]
- National Committee for Quality Assurance’s (NCQA). Healthcare Effectiveness Data and Information Set (HEDIS) Technical Specifications; National Committee for Quality Assurance: Washington, DC, USA, 2016; Volume 2, pp. 160–163. [Google Scholar]
- By the American Geriatrics Society 2015 Beers Criteria Update Expert Panel. American Geriatrics Society 2015 Updated Beers Criteria for Potentially Inappropriate Medication Use in Older Adults. J. Am. Geriatr. Soc. 2015, 63, 2227–2246. [Google Scholar] [CrossRef] [PubMed]
- O’Mahony, D.; O’Sullivan, D.; Byrne, S.; O’Connor, M.N.; Ryan, C.; Gallagher, P. STOPP/START criteria for potentially inappropriate prescribing in older people: Version 2. Age Ageing 2015, 44, 213–218. [Google Scholar] [CrossRef] [Green Version]
- Bhattacharjee, S.; Lee, J.K.; Patanwala, A.E.; Vadiei, N.; Malone, D.C.; Knapp, S.M.; Lo-Ciganic, W.H.; Burke, W.J. Extent and Predictors of Potentially Inappropriate Antidepressant Use Among Older Adults With Dementia and Major Depressive Disorder. Am. J. Geriatr. Psychiatry 2019, 27, 794–805. [Google Scholar] [CrossRef]
- Centers for Medicare and Medicaid Services. Chronic Conditions Data Warehouse: Condition Categories. 2015. Available online: https://www.ccwdata.org/web/guest/condition-categories (accessed on 30 June 2020).
- Wei, W.; Sambamoorthi, U.; Olfson, M.; Walkup, J.T.; Crystal, S. Use of psychotherapy for depression in older adults. Am. J. Psychiatry 2005, 162, 711–717. [Google Scholar] [CrossRef]
- Crystal, S.; Sambamoorthi, U.; Walkup, J.T.; Akincigil, A. Diagnosis and treatment of depression in the elderly medicare population: Predictors, disparities, and trends. J. Am. Geriatr. Soc. 2003, 51, 1718–1728. [Google Scholar] [CrossRef]
- Sambamoorthi, U.; Olfson, M.; Walkup, J.T.; Crystal, S. Diffusion of new generation antidepressant treatment among elderly diagnosed with depression. Med. Care 2003, 41, 180–194. [Google Scholar] [CrossRef]
- Sambamoorthi, U.; Shen, C.; Findley, P.; Frayne, S.; Banerjea, R. Depression treatment patterns among women veterans with cardiovascular conditions or diabetes. World Psychiatry 2010, 9, 177–182. [Google Scholar] [CrossRef]
- Perez, A.; Anzaldua, M.; McCormick, J.; Fisher-Hoch, S. High frequency of chronic end-stage liver disease and hepatocellular carcinoma in a Hispanic population. J. Gastroenterol. Hepatol. 2004, 19, 289–295. [Google Scholar] [CrossRef]
- Bhattacharjee, S.; Patanwala, A.E.; Lo-Ciganic, W.H.; Malone, D.C.; Lee, J.K.; Knapp, S.M.; Warholak, T.; Burke, W.J. Alzheimer’s disease medication and risk of all-cause mortality and all-cause hospitalization: A retrospective cohort study. Alzheimer’s Dement. 2019, 5, 294–302. [Google Scholar] [CrossRef]
- Tseng, V.L.; Yu, F.; Lum, F.; Coleman, A.L. Risk of fractures following cataract surgery in Medicare beneficiaries. JAMA 2012, 308, 493–501. [Google Scholar] [CrossRef] [Green Version]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences, 2nd ed.; Lawrence Erlbaum Associates: Mahwah, NJ, USA, 1988. [Google Scholar]
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2018. [Google Scholar]
- Davydow, D.S.; Zivin, K.; Langa, K.M. Hospitalization, depression and dementia in community-dwelling older Americans: Findings from the national health and aging trends study. Gen. Hosp. Psychiatry 2014, 36, 135–141. [Google Scholar] [CrossRef] [Green Version]
- Davydow, D.S.; Zivin, K.; Katon, W.J.; Pontone, G.M.; Chwastiak, L.; Langa, K.M.; Iwashyna, T.J. Neuropsychiatric disorders and potentially preventable hospitalizations in a prospective cohort study of older Americans. J. Gen. Intern. Med. 2014, 29, 1362–1371. [Google Scholar] [CrossRef] [PubMed]
- Davydow, D.S.; Hough, C.L.; Zivin, K.; Langa, K.M.; Katon, WJ. Depression and risk of hospitalization for pneumonia in a cohort study of older Americans. J. Psychosom. Res. 2014, 77, 528–534. [Google Scholar] [CrossRef] [Green Version]
- Ma, C.; Bao, S.; Dull, P.; Wu, B.; Yu, F. Hospital readmission in persons with dementia: A systematic review. Int. J. Geriatr. Psychiatry 2019, 34, 1170–1184. [Google Scholar] [CrossRef]
- Wang, H.H.; Sheu, J.T.; Shyu, Y.I.; Chang, H.Y.; Li, C.L. Geriatric conditions as predictors of increased number of hospital admissions and hospital bed days over one year: Findings of a nationwide cohort of older adults from Taiwan. Arch. Gerontol. Geriatr. 2014, 59, 169–174. [Google Scholar] [CrossRef]
- Boström, G.; Hörnsten, C.; Brännström, J.; Conradsson, M.; Nordström, P.; Allard, P.; Gustafson, Y.; Littbrand, H. Antidepressant use and mortality in very old people. Int. Psychogeriatr. 2016, 28, 1201–1210. [Google Scholar] [CrossRef]
- Enache, D.; Fereshtehnejad, S.M.; Kåreholt, I.; Cermakova, P.; Garcia-Ptacek, S.; Johnell, K.; Religa, D.; Jelic, V.; Winblad, B.; Ballard, C.; et al. Antidepressants and mortality risk in a dementia cohort: Data from SveDem, the Swedish Dementia Registry. Acta Psychiatr. Scand. 2016, 134, 430–440. [Google Scholar] [CrossRef]
- Sobieraj, D.M.; Baker, W.L.; Martinez, B.K.; Hernandez, A.V.; Coleman, C.I.; Ross, J.S.; Berg, K.M.; Steffens, D.C. AHRQ Comparative Effectiveness Reviews. In Adverse Effects of Pharmacologic Treatments of Major Depression in Older Adults; Agency for Healthcare Research and Quality: Rockville, MD, USA, 2019. [Google Scholar]
- Macri, J.C.; Iaboni, A.; Kirkham, J.G.; Maxwell, C.; Gill, S.S.; Vasudev, A.; Whitehead, M.; Seitz, D.P. Association between Antidepressants and Fall-Related Injuries among Long-Term Care Residents. Am. J. Geriatr. Psychiatry 2017, 25, 1326–1336. [Google Scholar] [CrossRef]
- Bakken, M.S.; Engeland, A.; Engesæter, L.B.; Ranhoff, A.H.; Hunskaar, S.; Ruths, S. Increased risk of hip fracture among older people using antidepressant drugs: Data from the Norwegian Prescription Database and the Norwegian Hip Fracture Registry. Age Ageing 2013, 42, 514–520. [Google Scholar] [CrossRef] [Green Version]
- Marcum, Z.A.; Perera, S.; Thorpe, J.M.; Switzer, G.E.; Castle, N.G.; Strotmeyer, E.S.; Simonsick, E.M.; Ayonayon, H.N.; Phillips, C.L.; Rubin, S.; et al. Antidepressant Use and Recurrent Falls in Community-Dwelling Older Adults: Findings From the Health ABC Study. Ann. Pharm. 2016, 50, 525–533. [Google Scholar] [CrossRef] [Green Version]
- Coupland, C.; Dhiman, P.; Morriss, R.; Arthur, A.; Barton, G.; Hippisley-Cox, J. Antidepressant use and risk of adverse outcomes in older people: Population based cohort study. BMJ 2011, 343, d4551. [Google Scholar] [CrossRef] [Green Version]
- Bohlken, J.; Jacob, L.; Schaum, P.; Rapp, M.A.; Kostev, K. Hip fracture risk in patients with dementia in German primary care practices. Dementia 2017, 16, 853–864. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Allan, L.M.; Ballard, C.G.; Burn, D.J.; Kenny, R.A. Prevalence and severity of gait disorders in Alzheimer’s and non-Alzheimer’s dementias. J. Am. Geriatr. Soc. 2005, 53, 1681–1687. [Google Scholar] [CrossRef] [PubMed]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | Adherent | Non-Adherent | Unweighted | Weighted | Unweighted | Weighted | |||
|---|---|---|---|---|---|---|---|---|---|
| N | % | N | % | χ2 | χ2 | df | p-Value | p-Value | |
| Age group | 0.283 | 0.019 | 1 | 0.595 | 0.891 | ||||
| 65–74 years | 537 | 71.13 | 218 | 28.87 | |||||
| 75+ years | 2577 | 72.08 | 998 | 27.92 | |||||
| Gender | 2.592 | 0.067 | 1 | 0.107 | 0.796 | ||||
| Male | 821 | 70.11 | 350 | 29.89 | |||||
| Female | 2293 | 72.59 | 866 | 27.41 | |||||
| Race/Ethnicity | 13.083 | 0.014 | 1 | <0.001 * | 0.906 | ||||
| White | 2725 | 72.90 | 1013 | 27.10 | |||||
| Others | 389 | 65.71 | 203 | 34.29 | |||||
| Public Assistance | 0.096 | 0.004 | 1 | 0.757 | 0.948 | ||||
| Yes | 1152 | 71.64 | 456 | 28.36 | |||||
| No | 1962 | 72.08 | 760 | 27.92 | |||||
| Region | 4.275 | 0.015 | 3 | 0.233 | 1.000 | ||||
| Northeast | 629 | 71.80 | 247 | 28.20 | |||||
| South | 1275 | 71.83 | 500 | 28.17 | |||||
| Midwest | 835 | 73.63 | 299 | 26.37 | |||||
| West | 375 | 68.81 | 170 | 31.19 | |||||
| Metropolitan status | 0.132 | 0.010 | 1 | 0.716 | 0.922 | ||||
| Yes | 2413 | 72.05 | 936 | 27.95 | |||||
| No | 701 | 71.46 | 280 | 28.54 | |||||
| Baseline PD | 0.267 | 0.046 | 1 | 0.605 | 0.831 | ||||
| No | 179 | 73.36 | 65 | 26.64 | |||||
| Yes | 2935 | 71.83 | 1151 | 28.17 | |||||
| Provider Specialty | 6.790 | 0.151 | 4 | 0.147 | 0.997 | ||||
| General/Family | 2284 | 72.60 | 862 | 27.40 | |||||
| Neurology | 64 | 67.37 | 31 | 32.63 | |||||
| Psychiatry | 163 | 73.09 | 60 | 26.91 | |||||
| Unknown | 234 | 72.90 | 87 | 27.10 | |||||
| Other | 369 | 67.71 | 176 | 32.29 | |||||
| Density of Neurologists | 9.269 | 0.023 | 3 | 0.026 * | 0.999 | ||||
| 0 | 634 | 71.00 | 259 | 29.00 | |||||
| 1 | 844 | 73.58 | 303 | 26.42 | |||||
| 2 | 793 | 68.96 | 357 | 31.04 | |||||
| 3 | 843 | 73.95 | 297 | 26.05 | |||||
| Density of Psychiatrists | 0.324 | 0.037 | 3 | 0.955 | 0.998 | ||||
| 0 | 507 | 71.81 | 199 | 28.19 | |||||
| 1 | 866 | 71.81 | 340 | 28.19 | |||||
| 2 | 850 | 71.49 | 339 | 28.51 | |||||
| 3 | 891 | 72.50 | 338 | 27.50 | |||||
| ELX Index | 9.101 | 0.052 | 3 | 0.028 * | 0.997 | ||||
| 0 | 565 | 71.25 | 228 | 28.75 | |||||
| 1 | 512 | 69.10 | 229 | 30.90 | |||||
| 2 | 448 | 69.46 | 197 | 30.54 | |||||
| 3 | 1589 | 73.87 | 562 | 26.13 | |||||
| Baseline medication use | |||||||||
| ACE Inhibitor | 0.317 | 0.006 | 1 | 0.573 | 0.938 | ||||
| Yes | 862 | 71.30 | 347 | 28.70 | |||||
| No | 2252 | 72.16 | 869 | 27.84 | |||||
| Anticoagulant | 0.481 | 0.007 | 1 | 0.488 | 0.935 | ||||
| Yes | 383 | 70.66 | 159 | 29.34 | |||||
| No | 2731 | 72.10 | 1057 | 27.90 | |||||
| Antidiabetic | 0.728 | 0.004 | 1 | 0.394 | 0.950 | ||||
| Yes | 622 | 70.76 | 257 | 29.24 | |||||
| No | 2492 | 72.21 | 959 | 27.79 | |||||
| Antiparkinsonian | 0.721 | 0.013 | 1 | 0.396 | 0.908 | ||||
| Yes | 209 | 74.11 | 73 | 25.89 | |||||
| No | 2905 | 71.76 | 1143 | 28.24 | |||||
| Antipsychotic | 6.969 | 0.003 | 1 | 0.008 * | 0.955 | ||||
| Yes | 577 | 75.82 | 184 | 24.18 | |||||
| No | 2537 | 71.08 | 1032 | 28.92 | |||||
| ARB | 1.446 | 0.000 | 1 | 0.229 | 0.998 | ||||
| Yes | 395 | 74.11 | 138 | 25.89 | |||||
| No | 2719 | 71.61 | 1078 | 28.39 | |||||
| Anxiolytic | 5.783 | 0.049 | 1 | 0.016 * | 0.825 | ||||
| Yes | 395 | 67.75 | 188 | 32.25 | |||||
| No | 2719 | 72.56 | 1028 | 27.44 | |||||
| Betablocker | 0.290 | 0.007 | 1 | 0.590 | 0.934 | ||||
| Yes | 1275 | 72.36 | 487 | 27.64 | |||||
| No | 1839 | 71.61 | 729 | 28.39 | |||||
| CCB | 0.100 | 0.041 | 1 | 0.752 | 0.840 | ||||
| Yes | 754 | 71.54 | 300 | 28.46 | |||||
| No | 2360 | 72.04 | 916 | 27.96 | |||||
| PPI | 0.141 | 0.001 | 1 | 0.708 | 0.982 | ||||
| Yes | 940 | 72.31 | 360 | 27.69 | |||||
| No | 2174 | 71.75 | 856 | 28.25 | |||||
| Diuretic | 1.531 | 0.000 | 1 | 0.216 | 0.989 | ||||
| Yes | 1164 | 73.02 | 430 | 26.98 | |||||
| No | 1950 | 71.27 | 786 | 28.73 | |||||
| Statin | 2.647 | 0.007 | 1 | 0.104 | 0.934 | ||||
| Yes | 1197 | 73.35 | 435 | 26.65 | |||||
| No | 1917 | 71.05 | 781 | 28.95 | |||||
| Characteristics | Adherent | Non-Adherent | Unweighted | Weighted | Unweighted | Weighted | |||
|---|---|---|---|---|---|---|---|---|---|
| N | % | N | % | χ2 | χ2 | df | p-Value | p-Value | |
| Age group | 2.298 | 0.001 | 1 | 0.130 | 0.9715 | ||||
| 65–74 years | 411 | 58.55 | 291 | 41.45 | |||||
| 75+ years | 1996 | 61.62 | 1243 | 38.38 | |||||
| Gender | 2.855 | 0.012 | 1 | 0.091 | 0.9146 | ||||
| Male | 613 | 58.89 | 428 | 41.11 | |||||
| Female | 1794 | 61.86 | 1106 | 38.14 | |||||
| Race/Ethnicity | 38.713 | 0.000 | 1 | <0.001 * | 0.9841 | ||||
| White | 2141 | 63.01 | 1257 | 36.99 | |||||
| Others | 266 | 48.99 | 277 | 51.01 | |||||
| Public Assistance | 0.416 | 0.000 | 1 | 0.519 | 0.9867 | ||||
| Yes | 1523 | 61.46 | 955 | 38.54 | |||||
| No | 884 | 60.42 | 579 | 39.58 | |||||
| Region | 15.483 | 0.007 | 3 | 0.001 * | 0.9999 | ||||
| Northeast | 507 | 63.45 | 292 | 36.55 | |||||
| South | 940 | 58.86 | 657 | 41.14 | |||||
| Midwest | 674 | 64.81 | 366 | 35.19 | |||||
| West | 286 | 56.63 | 219 | 43.37 | |||||
| Metropolitan status | 0.579 | 0.001 | 1 | 0.447 | 0.9716 | ||||
| Yes | 1850 | 60.76 | 1195 | 39.24 | |||||
| No | 557 | 62.17 | 339 | 37.83 | |||||
| Baseline PD | 1.254 | 0.000 | 1 | 0.263 | 0.9965 | ||||
| Yes | 146 | 64.60 | 80 | 35.40 | |||||
| No | 2261 | 60.86 | 1454 | 39.14 | |||||
| Provider Specialty | 19.464 | 0.059 | 4 | 0.001 * | 0.9996 | ||||
| General/Family | 1766 | 61.92 | 1086 | 38.08 | |||||
| Neurology | 37 | 44.05 | 47 | 55.95 | |||||
| Other | 284 | 55.91 | 224 | 44.09 | |||||
| Psychiatry | 132 | 62.86 | 78 | 37.14 | |||||
| Unknown | 188 | 65.51 | 99 | 34.49 | |||||
| Density of Neurologists | 4.547 | 0.038 | 3 | 0.208 | 0.9981 | ||||
| 0 | 494 | 60.76 | 319 | 39.24 | |||||
| 1 | 638 | 60.99 | 408 | 39.01 | |||||
| 2 | 617 | 58.99 | 429 | 41.01 | |||||
| 3 | 658 | 63.51 | 378 | 36.49 | |||||
| Density of Psychiatrists | 7.664 | 0.008 | 3 | 0.054 | 0.9998 | ||||
| 0 | 406 | 63.84 | 230 | 36.16 | |||||
| 1 | 654 | 59.19 | 451 | 40.81 | |||||
| 2 | 641 | 59.13 | 443 | 40.87 | |||||
| 3 | 706 | 63.26 | 410 | 36.74 | |||||
| ELX Index | 10.949 | 0.017 | 3 | 0.012 * | 0.9994 | ||||
| 0 | 441 | 59.12 | 305 | 40.88 | |||||
| 1 | 393 | 56.79 | 299 | 43.21 | |||||
| 2 | 363 | 61.01 | 232 | 38.99 | |||||
| 3 | 1210 | 63.42 | 698 | 36.58 | |||||
| Baseline medication use | |||||||||
| ACE Inhibitor | 0.232 | 0.012 | 1 | 0.630 | 0.914 | ||||
| Yes | 676 | 61.68 | 420 | 38.32 | |||||
| No | 1731 | 60.84 | 1114 | 39.16 | |||||
| Anticoagulant | 0.008 | 0.002 | 1 | 0.930 | 0.9650 | ||||
| Yes | 299 | 60.90 | 192 | 39.10 | |||||
| No | 2108 | 61.10 | 1342 | 38.90 | |||||
| Antidiabetic | 3.372 | 0.000 | 1 | 0.066 | 0.9853 | ||||
| Yes | 466 | 58.25 | 334 | 41.75 | |||||
| No | 1941 | 61.80 | 1200 | 38.20 | |||||
| Antiparkinsonian | 0.838 | 0.000 | 1 | 0.360 | 0.9879 | ||||
| Yes | 167 | 63.74 | 95 | 36.26 | |||||
| No | 2240 | 60.89 | 1439 | 39.11 | |||||
| Antipsychotic | 14.386 | 0.004 | 1 | <0.001 * | 0.9478 | ||||
| Yes | 463 | 67.49 | 223 | 32.51 | |||||
| No | 1944 | 59.72 | 1311 | 40.28 | |||||
| ARB | 0.167 | 0.008 | 1 | 0.683 | 0.9276 | ||||
| Yes | 300 | 60.24 | 198 | 39.76 | |||||
| No | 2107 | 61.20 | 1336 | 38.80 | |||||
| Anxiolytic | 6.626 | 0.036 | 1 | 0.010 * | 0.849 | ||||
| Yes | 298 | 56.02 | 234 | 43.98 | |||||
| No | 2109 | 61.87 | 1300 | 38.13 | |||||
| Betablocker | 2.952 | 0.001 | 1 | 0.086 | 0.9802 | ||||
| Yes | 992 | 62.71 | 590 | 37.29 | |||||
| No | 1415 | 59.98 | 944 | 40.02 | |||||
| CCB | 1.145 | 0.012 | 1 | 0.285 | 0.9138 | ||||
| Yes | 565 | 59.60 | 383 | 40.40 | |||||
| No | 1842 | 61.54 | 1151 | 38.46 | |||||
| Diuretic | 0.169 | 0.004 | 1 | 0.681 | 0.9504 | ||||
| Yes | 888 | 61.50 | 556 | 38.50 | |||||
| No | 1519 | 60.83 | 978 | 39.17 | |||||
| PPI | 0.301 | 0.005 | 1 | 0.583 | 0.9416 | ||||
| Yes | 729 | 61.73 | 452 | 38.27 | |||||
| No | 1678 | 60.80 | 1082 | 39.20 | |||||
| Statin | 0.264 | 0.010 | 1 | 0.607 | 0.9211 | ||||
| Yes | 925 | 61.58 | 577 | 38.42 | |||||
| No | 1482 | 60.76 | 957 | 39.24 | |||||
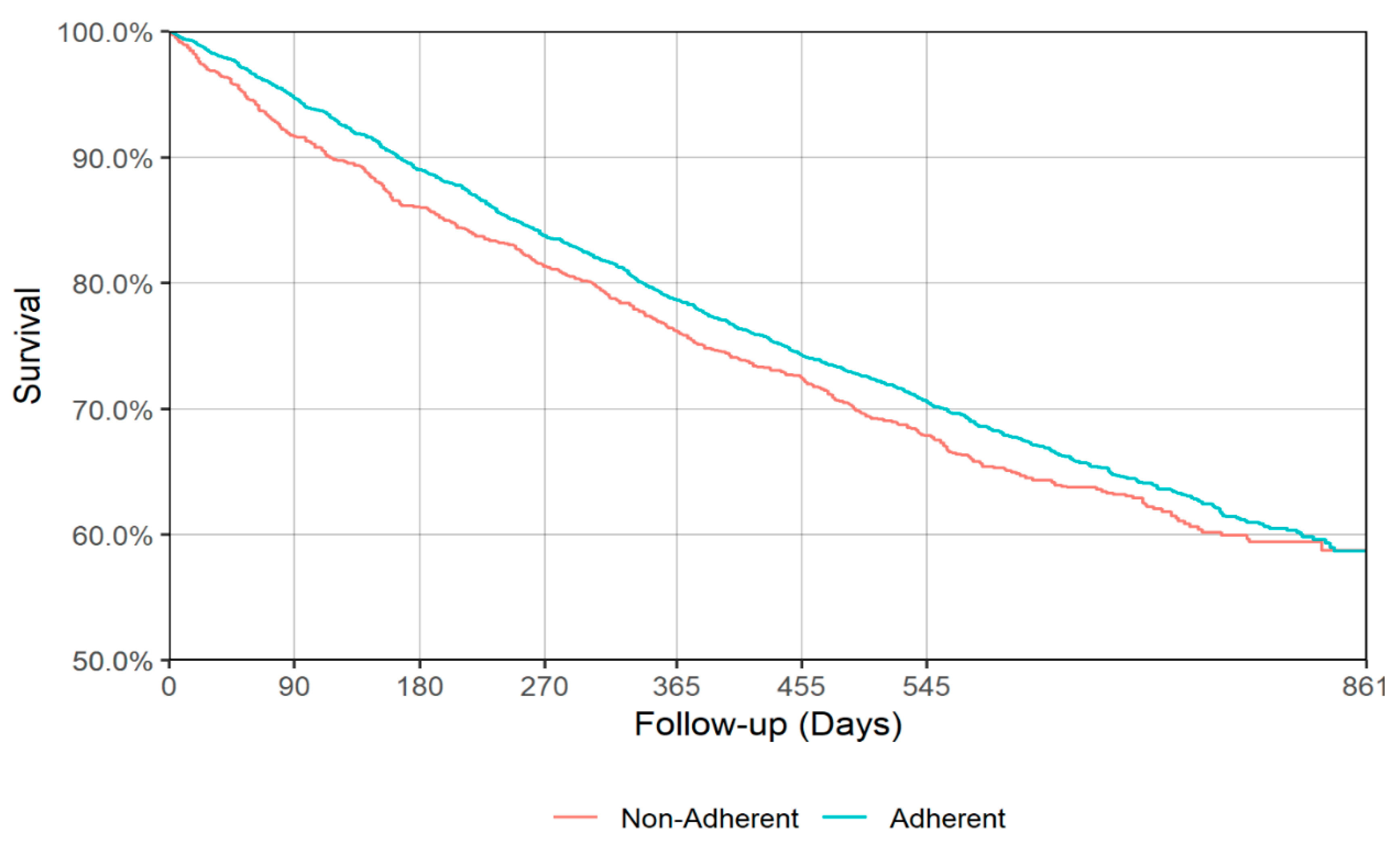
| Acute Depression Treatment Phase | ||||
|---|---|---|---|---|
| All-cause mortality | ||||
| Adherent | Non-adherent | |||
| 90 days | 0.9463 | (0.9377–0.9537) | 0.9164 | (0.8990–0.9310) |
| 180 days | 0.8891 | (0.8775–0.8997) | 0.8607 | (0.8395–0.8794) |
| 270 days | 0.8367 | (0.8232–0.8493) | 0.8134 | (0.7898–0.8346) |
| 365 days | 0.7857 | (0.7708–0.7999) | 0.7617 | (0.7362–0.7851) |
| 455 days | 0.7418 | (0.7259–0.7570) | 0.7240 | (0.6974–0.7488) |
| 545 days | 0.7050 | (0.6883–0.7209) | 0.6785 | (0.6507–0.7046) |
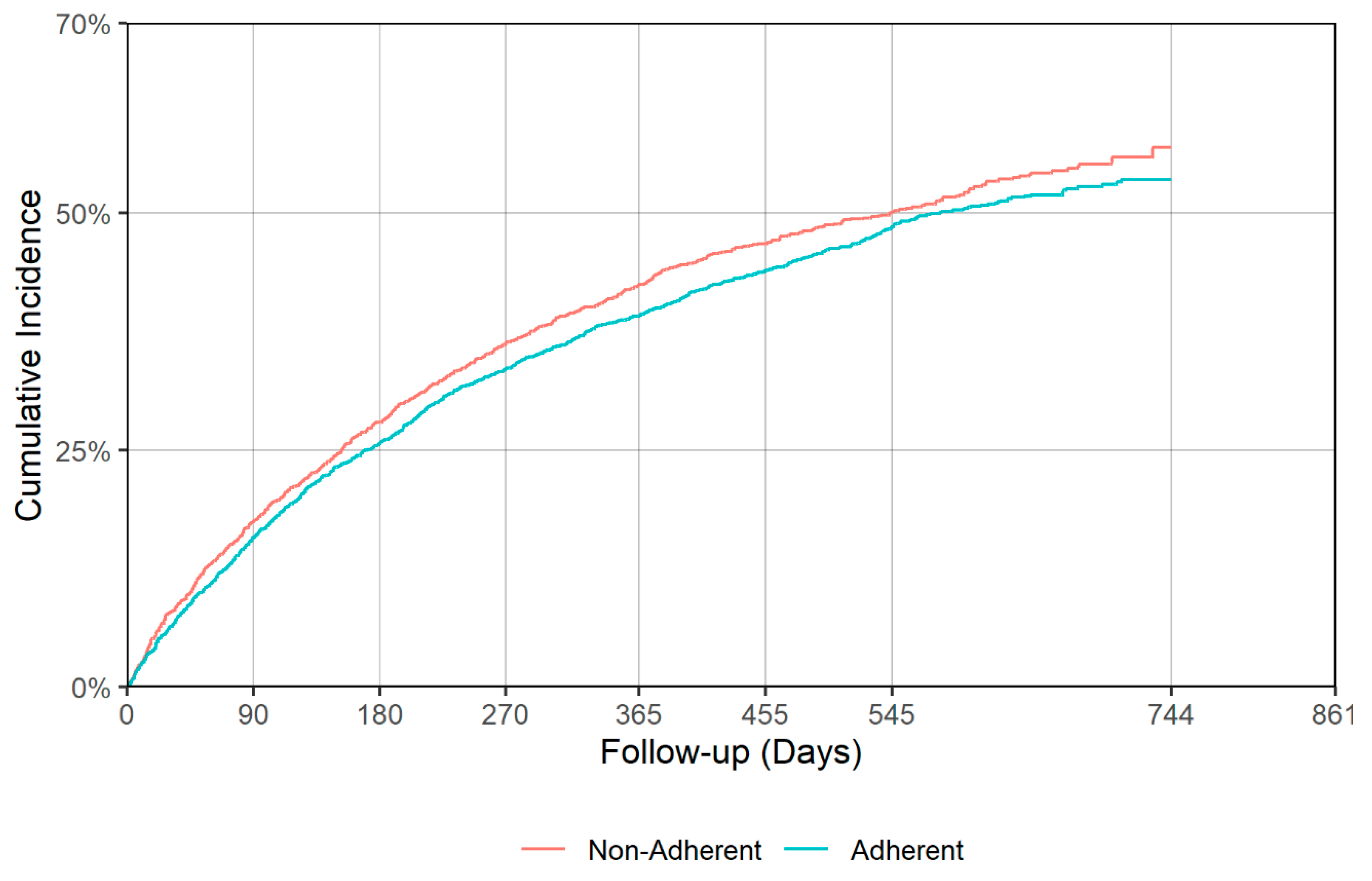
| All-cause hospitalization | ||||
| Adherent | Non-adherent | |||
| 90 days | 0.1702 | (0.1571–0.1840) | 0.1998 | (0.1762–0.2232) |
| 180 days | 0.2736 | (0.2573–0.2893) | 0.3209 | (0.2933–0.3486) |
| 270 days | 0.3603 | (0.3430–0.3775) | 0.3910 | (0.3626–0.4191) |
| 365 days | 0.4190 | (0.4013–0.4362) | 0.4667 | (0.4370–0.4980) |
| 455 days | 0.4643 | (0.4470–0.4813) | 0.5077 | (0.4765–0.5362) |
| 545 days | 0.5042 | (0.4869–0.5216) | 0.5438 | (0.5127–0.5731) |
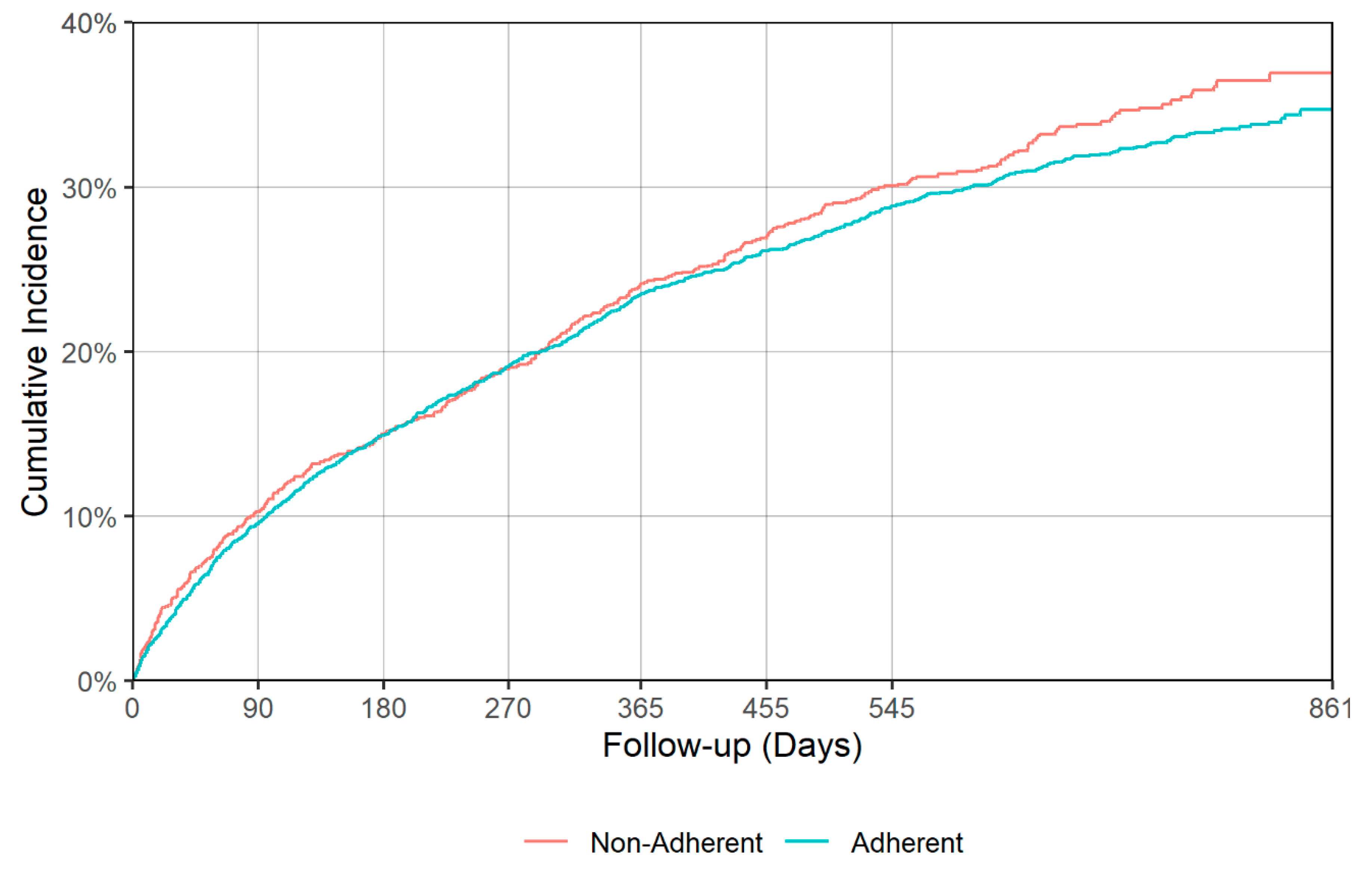
| Falls and Fractures | ||||
| Adherent | Non-adherent | |||
| 90 days | 0.0953 | (0.0849–0.1058) | 0.1027 | (0.0852–0.1203) |
| 180 days | 0.1491 | (0.1366–0.1616) | 0.1500 | (0.1290–0.1699) |
| 270 days | 0.1911 | (0.1766–0.2044) | 0.1897 | (0.1687–0.2109) |
| 365 days | 0.2351 | (0.2192–0.2493) | 0.2412 | (0.2167–0.2650) |
| 455 days | 0.2611 | (0.2453–0.2771) | 0.2689 | (0.2425–0.2944) |
| 545 days | 0.2883 | (0.2727–0.3044) | 0.3008 | (0.2731–0.3266) |
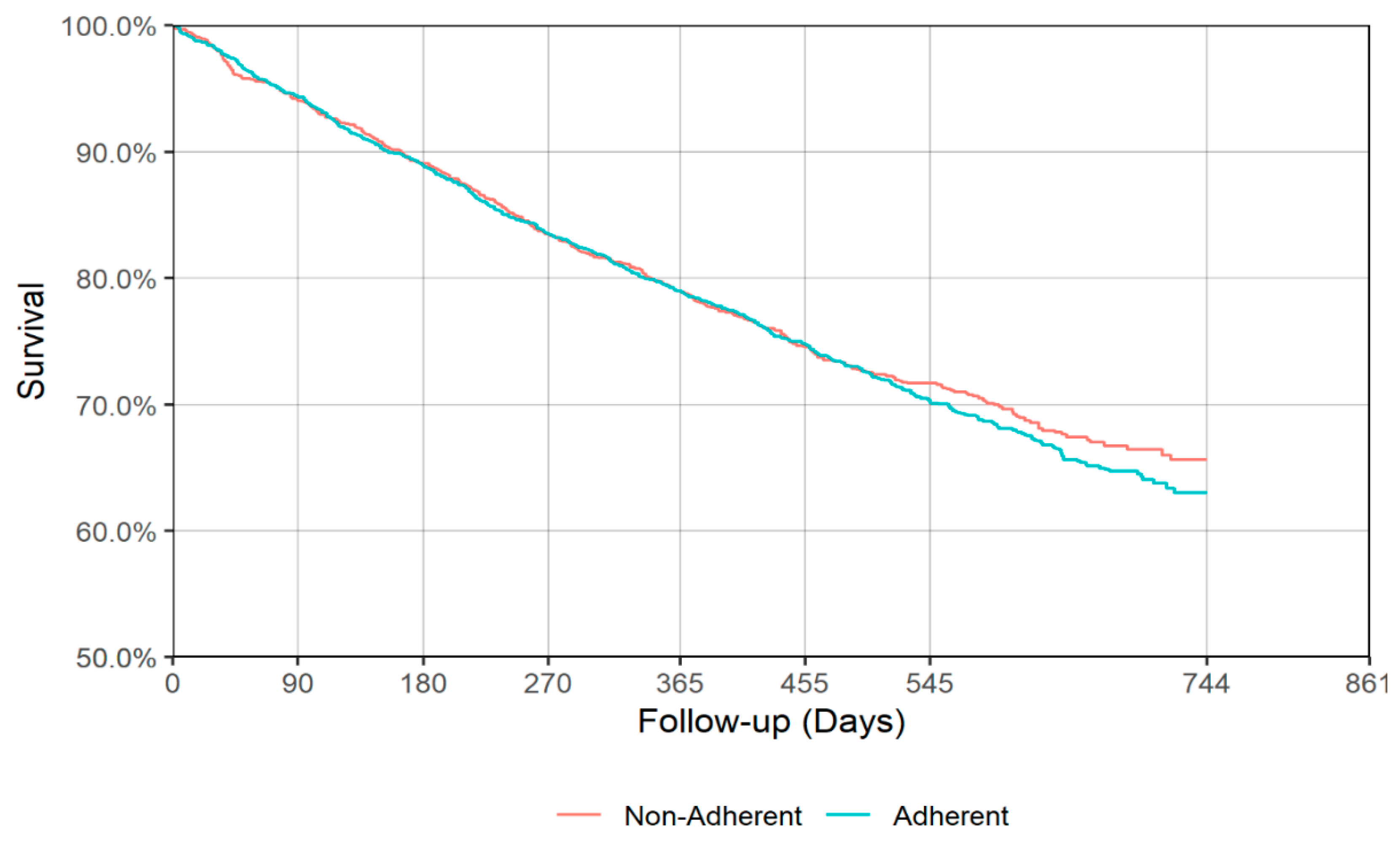
| Continuation Depression Treatment Phase | ||||
| All-cause mortality | ||||
| Adherent | Non-adherent | |||
| 90 days | 0.9430 | (0.9328–0.9517) | 0.9398 | (0.9263–0.9509) |
| 180 days | 0.8887 | (0.8753–0.9008) | 0.8899 | (0.8726–0.9049) |
| 270 days | 0.8344 | (0.8187–0.8490) | 0.8343 | (0.8141–0.8525) |
| 365 days | 0.7895 | (0.7723–0.8055) | 0.7888 | (0.7668–0.8090) |
| 455 days | 0.7473 | (0.7289–0.7647) | 0.7447 | (0.7210–0.7666) |
| 545 days | 0.7014 | (0.6811–0.7207) | 0.7161 | (0.6912–0.7394) |
| All-cause hospitalization | ||||
| Adherent | Non-adherent | |||
| 90 days | 0.1574 | (0.1427–0.1728) | 0.1739 | (0.1565–0.1929) |
| 180 days | 0.2569 | (0.2382–0.2752) | 0.2796 | (0.2579–0.3031) |
| 270 days | 0.3354 | (0.3159–0.3552) | 0.3619 | (0.3385–0.3876) |
| 365 days | 0.3914 | (0.3723–0.4119) | 0.4243 | (0.4011–0.4510) |
| 455 days | 0.4391 | (0.4185–0.4601) | 0.4674 | (0.4437–0.4951) |
| 545 days | 0.4847 | (0.4632–0.5056) | 0.5012 | (0.4772–0.5293) |
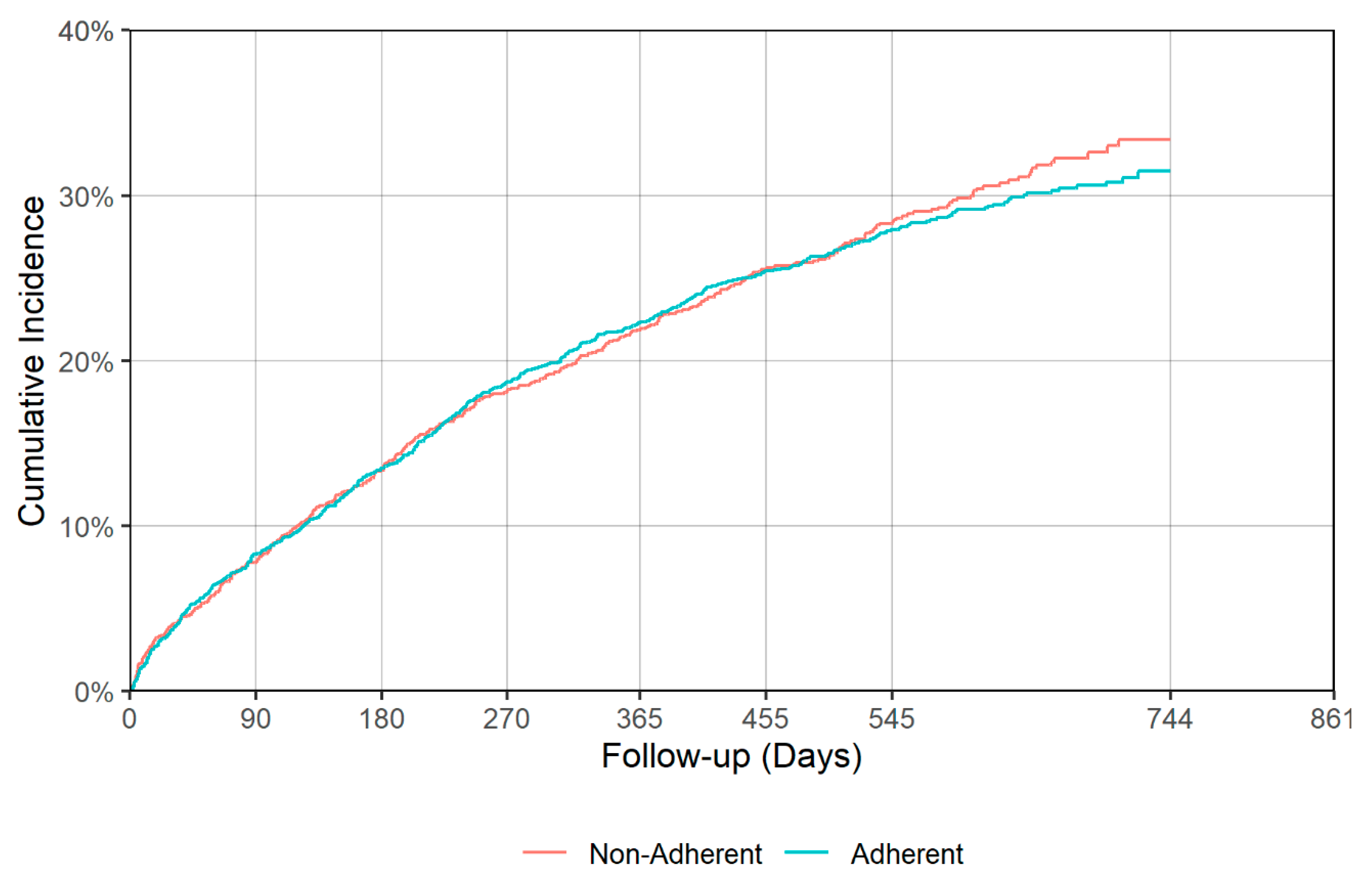
| Falls and Fractures | ||||
| Adherent | Non-adherent | |||
| 90 days | 0.0826 | (0.0718–0.0937) | 0.0778 | (0.0651–0.0936) |
| 180 days | 0.1348 | (0.1214–0.1491) | 0.1338 | (0.1162–0.1526) |
| 270 days | 0.1872 | (0.1722–0.2043) | 0.1815 | (0.1620–0.2009) |
| 365 days | 0.2231 | (0.2068–0.2407) | 0.2187 | (0.1981–0.2396) |
| 455 days | 0.2543 | (0.2368–0.2725) | 0.2555 | (0.2336–0.2786) |
| 545 days | 0.2794 | (0.2606–0.2979) | 0.2829 | (0.2600–0.3074) |
| Acute Depression Treatment Phase | ||||
|---|---|---|---|---|
| Mortality | ||||
| Adherent | Non-adherent | |||
| 1st Quartile | 441 | (406–474) | 385 | (342–455) |
| Median | NA | NA | NA | NA |
| Hospitalization | ||||
| Adherent | Non-adherent | |||
| 1st Quartile | 153 | (140–171) | 122 | (103–139) |
| Median | 530 | (499–587) | 425 | (364–492) |
| Falls and Fractures | ||||
| Adherent | Non-adherent | |||
| 1st Quartile | 424 | (364–471) | 403 | (336–459) |
| Median | NA | NA | NA | NA |
| Continuation Depression Treatment Phase | ||||
| Mortality | ||||
| Adherent | Non-adherent | |||
| 1st Quartile | 445 | (415–483) | 443 | (397–492) |
| Median | NA | NA | NA | NA |
| Hospitalization | ||||
| Adherent | Non-adherent | |||
| 1st Quartile | 169 | (146–191) | 152 | (135–170) |
| Median | 578 | (536–666) | 543 | (463–599) |
| Falls and Fractures | ||||
| Adherent | Non-adherent | |||
| 1st Quartile | 436 | (387–510) | 440 | (384–516) |
| Median | NA | NA | NA | NA |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bhattacharjee, S.; Naeem, S.; Knapp, S.M.; Lee, J.K.; Patanwala, A.E.; Vadiei, N.; Malone, D.C.; Lo-Ciganic, W.-H.; Burke, W.J. Health Outcomes Associated with Adherence to Antidepressant Use during Acute and Continuation Phases of Depression Treatment among Older Adults with Dementia and Major Depressive Disorder. J. Clin. Med. 2020, 9, 3358. https://doi.org/10.3390/jcm9103358
Bhattacharjee S, Naeem S, Knapp SM, Lee JK, Patanwala AE, Vadiei N, Malone DC, Lo-Ciganic W-H, Burke WJ. Health Outcomes Associated with Adherence to Antidepressant Use during Acute and Continuation Phases of Depression Treatment among Older Adults with Dementia and Major Depressive Disorder. Journal of Clinical Medicine. 2020; 9(10):3358. https://doi.org/10.3390/jcm9103358
Chicago/Turabian StyleBhattacharjee, Sandipan, Suniya Naeem, Shannon M. Knapp, Jeannie K. Lee, Asad E. Patanwala, Nina Vadiei, Daniel C. Malone, Wei-Hsuan Lo-Ciganic, and William J Burke. 2020. "Health Outcomes Associated with Adherence to Antidepressant Use during Acute and Continuation Phases of Depression Treatment among Older Adults with Dementia and Major Depressive Disorder" Journal of Clinical Medicine 9, no. 10: 3358. https://doi.org/10.3390/jcm9103358