Religious and Spiritual Biomarkers in Both Health and Disease

Postgraduate and Doctoral School named after St Cyril and Methodius, Russian Orthodox Church, Cathedral of the Mother of God of Kazan on the Red Square, Moscow, Ulitsa Gerasima Kurina 16/174, Moscow 121108, Russia
Religions 2012, 3(2), 467-497; https://doi.org/10.3390/rel3020467
Submission received: 6 February 2012
/
Revised: 11 May 2012
/
Accepted: 29 May 2012
/
Published: 6 June 2012
Abstract
:Religious thought and spirituality can be considered as a part of natural human capacities. There is an exponential rise in clinical research in the relationship between religion, spirituality and positive health outcomes. Most of these studies, however, have been primarily descriptive, rather than explanatory, focusing on identifying their underlying mechanisms. Almost no attempts have been made to find novel methods to mirror and monitor positive, and possibly negative, reactions related to the local and general effects of religion and spirituality in healthy subjects and patients. As this area of interest is rather new, we propose to put forward a new hypothesis that effects of religion and spirituality can be objectively studied by various exhaled biomarkers, some of which have already been developed and tested in health and disease. The lungs are particularly well suited for this purpose, as we have easy access to exhaled air and thereby a possibility to develop methods that measure compounds directly released from them. This work is the first step in the convergence of medical and theological research by linking various biomarkers and physiological measures with indicators of individual belief systems, religiosity and spirituality.
Keywords:
religion; spirituality; prayer; exhaled biomarkers; inflammation; nitric oxide; volatile compounds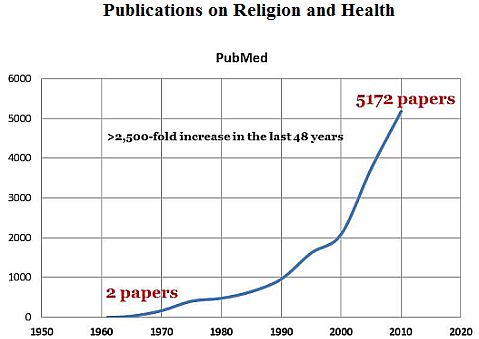
{kind=link}
{kind=link}
{kind=link}
1. Introduction
Research within the field of religion and spirituality in health and disease is expanding rapidly. It has been shown that religiosity is an effective coping resource for people with health related problems, and it has been correlated with better health outcomes. Considering the consistency of the findings and the diversity of the methodological approaches used, it is unlikely that the salutary effects of religiosity and spirituality are solely attributable to chance or biased methods.
However the processes by which religiosity and spirituality are utilized and their effects on various biochemical, inflammatory and immune parameters of both healthy individuals and patients have not been adequately explored. This may be the reason that not all of the evidence is conclusive. Thus, the efficacy of religious practice relative to health outcomes, with religiosity measured as religious attendance in the subset of 27 studies has been inconclusive at best [1,2]. Almost no attempts have been made to find novel methods to mirror and monitor positive, and possibly negative, reactions related to the local and general effects of religion and spirituality in healthy subjects and patients.
As this area of interest is rather new, we propose to put forward a new hypothesis that the effects of religion and spirituality can be objectively studied by various exhaled biomarkers, some of which have already been developed and tested in healthy individuals and patients. The lungs are particularly well suited for this purpose, as we have easy access to exhaled air and thereby a possibility to develop methods that measure compounds directly released from them.
This work is the first step in the convergence of medical and theological research by linking various biomarkers and physiological measures with indicators of individual belief systems, religiosity and spirituality.
2. Results and Discussion
2.1. Rationale for New Category of Religious and Spiritual Biomarkers
The current focus on the relationship of religion and spirituality with healing is a remarkable and unanticipated current developed within academic medicine [3].
Most medical schools in the 1990s dropped religious and spiritual dimension from their vocabulary. This was partially due to an increasing emphasis on the scientific basis for medical practice, e.g. “evidence-based” medicine. This inattention inadvertently undermined the medical student's own spiritual growth [4], and it certainly inhibited the development of a clinical facility when confronting spiritual issues.
However, medicine as a “sacred vocation” [5] is coming back. Religious or spiritual problems were recognized as a new diagnostic category (Code V62.89)1: the Diagnostic and Statistical Manual of Mental Disorders acknowledged that crises that challenged a person's spiritual composure or the emergence or maturation of one's spiritual identity could present times of psychic-spiritual and even physical distress [6]. The validity of this category has been further improved, so that more subtle distinctions can be made, differentiating mental disorders and religious or spiritual problems from "pure" religious problems [7].
Approximately 70% of U.S. medical schools now include spiritual dimension (religion and spirituality) in their curricula [8] as a component in the Medical School Objectives Project for medical schools, this represents an approximately 33-fold rise over the last 15 years. The new curricular guidelines of the American Association of Medical Colleges [9] reads: “In all their interactions with patients, physicians must seek to understand the meaning of the patient's stories in the context of the patient's beliefs, family, and cultural values” [5].
Patient centeredness is now considered as a central component of high-quality health care [10,11]. This is to help practitioners provide care that is concordant with the patient's values, needs and preferences, including their religiosity and spirituality. In fact, in a 2011 GALLUP Poll2, most of the US adults believed in God (no change since the 1940s), and 79% believed that faith can help people recover from disease.
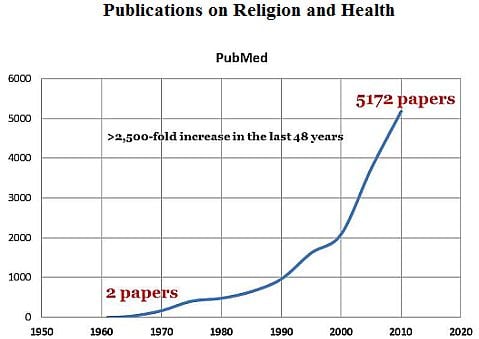
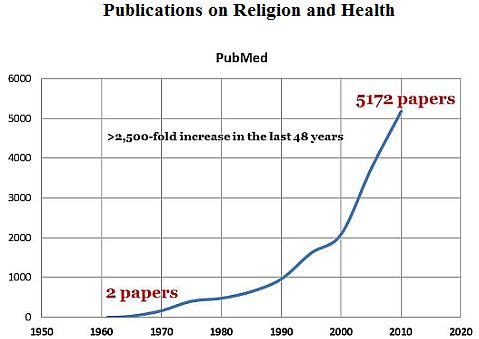
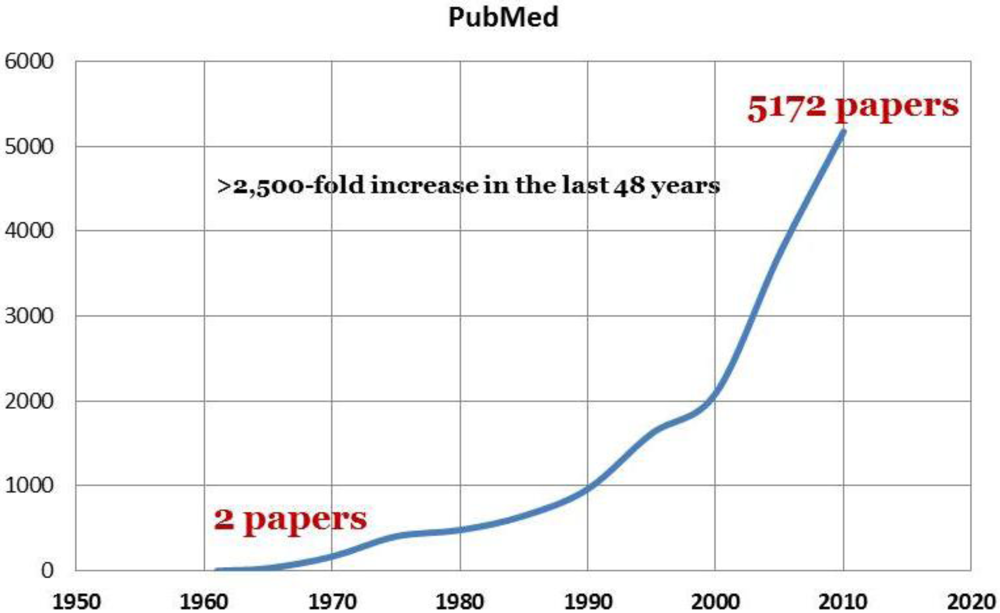
There is a considerable number of clinical trials, including children, adults and elderly patients, in which significant positive responses to various spiritual and religious means have been observed, and some mechanisms of their actions have been suggested. This is reflected by an exponential rise in research in the relationship between religion, spirituality and health outcomes [8,12] with a >2,500-fold increase in the number of articles in the last 48 years (Figure 1).
Figure 1.
Publications on religion and health (PubMed).

Most of these studies, however, have been primarily descriptive, investigating associations between spirituality and health, rather than explanatory, focusing on identifying their underlying mechanisms [13]. Earlier and current research is also limited by the failure to use simple non-invasive biomarker measurements that have been recently developed [14,15,16] and validated [17,18,19].
The research focus now is turning to examining not only whether religious factors are relevant to human health, but also how spirituality may functionally impact medical and psychological wellbeing [20] and illness. A combined approach, treating the human person as a single, united whole3 and the sacred in medicine raise a new set of medical, theological and ethical questions, which are discussed in this article. The spiritual dimension may restore the historically close relationship between medicine and religion, the twin traditions of healing [21].
This is of particular importance in an era of patient dissatisfaction with a technologically advanced, but increasingly impersonal form of medical care [22]. Research in religion and spirituality in health and disease will benefit from the existing arsenal of simple, non-invasive exhaled biomarker assessments. Creating personal bio-medical and spiritual patients profiles may offer personalization of medical care and significant benefits to the patient at little cost.
2.2. Understanding Its Potential Health Effect, not Trivializing Religion
There is a certain danger of religious activities being “prescribed” by either clerical staff or medical doctors, because of the growing number of research studies demonstrating a positive link between religion and health outcomes. We agree with the concern expressed by Sloan et al. [23], that “an instrumental approach” to religion, derived from the need to define variables for use in scientific studies, or to validate religion by its effects on health, should not be used to trivialize religion. Although it is agreeable that religion does not need science to justify its existence or appeal [23], it can be argued that medical science needs to be able to quantify its effect in health and disease.
2.3. Religiosity vs. Spirituality
Spirituality is often confused with religiosity, as the two constructs are closely related, but are not synonymous. Both of them deal with the divine and can involve practices aimed at increasing feelings of connection with a higher power [24]. There are important differences, however:
- a) Religiosity is seen as more of a public, formal, and socialized practice; spirituality is characterized as more private, naturally occurring [24]
These differences between religiosity and spirituality may not be simply academic. Medical cancer, cardiac and HIV patients, when they were not provided with specific definitions, differentiated easily between the two constructs [27]. It is not surprising, perhaps, that “spiritual individuals” reported that their spirituality helped them to heal themselves, and self-identified religious patients reported that their healing was the direct result of divine intervention.
Older adults who reported attending religious services more frequently had better functional 1st and 7th-month recovery following an acute myocardial infarction (AMI) than those who considered themselves more spiritual [28].
Therefore, religiosity and spirituality, although often overlapping, should be investigated separately.
Human beings’ relation to that which they regard as holy, absolute, spiritual, divine, or worthy of special reverence (definition of religion in Encyclopaedia Britannica)4, is both difficult to describe and to measure. Therefore, assessment of the potential effect of religiosity and spirituality on health by investigating the existing and discovering novel biomarkers, may not be simply academic, but can be used in the clinic in the future. In medicine, a biomarker can be considered as anything that may be used as an indicator of a particular physiological or psychological state of a human being. A number of biomarkers have been shown to be affected by psychological stress [29,30]. “Spiritual biomarker”, can be defined as any physiological and/or psychological biomarker that is capable to reflect the changing state of a human being involved in a certain religious and/or spiritual activity. Spiritual biomarkers can help characterize and quantify the biological and psychological impact of religion, religiosity and spirituality on health and disease.
2.4. Healing vs. Cure
There is a tendency to equate healing with cure. When an illness is incurable, there is a common misperception that healing is not possible either. Yet there is an opportunity for healing, even in the midst of an incurable illness. Healing can be manifested as inner peace; peace and reconciliation with God, self, and others; acceptance; letting go; and, finally, a peaceful death [31,32].
2.5. Integrated Approach to a Patient as a Whole Person
Western philosophy, beginning with Plato, describes the human being as consisting of two separate parts—the body and the mind [31]. This division was further widened as medicine became more scientific, and religion was seen as a barrier to progress. Eventually, the realm of the body was delegated to physicians, whereas the care of the soul remained with religious leaders [31].
Early Christian sources assumed a similar dichotomy between body and soul, although St. Irenaeus wrote that “the union of these (soul, the spirit and the body) constitutes the perfect man” [33]. And for this cause Apostle Paul made it clear that the saved man is a complete man as well as a spiritual man; saying thus in the first Epistle to the Thessalonians, “And the very God of peace sanctify you wholly; and I pray God your whole spirit and soul and body be preserved blameless unto the coming of our Lord Jesus Christ” (1 Thes 5:23).
Just spiritual or physical medical care alone is not enough. The Jewish tradition asserts that humans are integrated wholes, that body, mind, emotions and will all are connected and that these faculties all affect one another [31]. The traditional Jewish prayer for the sick asks God to grant “healing of body and healing of soul” because it recognizes that the two are intertwined. Similarly, Islam teaches that God created the whole person as one unit and in a perfect form, and that the healing process must deal with all aspects of the human being [31].
In the Second Vatican Council, the first chapter of the Pastoral Constitution of the Church in the Modern World noted, “the human person, though made of body and soul is a unity” [34].
Therefore, whether from a Christian, Jewish, or Muslim perspective, this view of human beings as a whole has immediate implications for how patients must be treated. Furthermore, this approach makes an integrated approach of creating an individual, but integrated breath profile of a patient as a whole subject, extremely attractive.
2.6. General Effects of Religion and Spirituality
Positive association of religion and spirituality with physical and mental health, as it is judged, for example, by the frequency of church (synagogue, or mosque) attendance [1,21], has been demonstrated in many studies, and has been known since the Biblical times5.
Spiritual and religious practices appear to positively influence medical outcomes and coping [35,36]. A National Health Interview Survey of 21,204 adults has demonstrated better physical and mental health outcomes, as well as increased longevity in those who attended church weekly [37].
Most of these studies, however, have used cross-sectional designs, and very few of them used any objective measurements of biological parameters. In fact, it has been suggested that frequent religious attendance is simply a proxy for functional ability, especially in older adults whose health may prevent them from regular religious attendance [21].
2.7. Mortality
Religious commitment may increase longevity, starting with clergy. Thus, 12 studies, published between 1959 and 2000, examined mortality among American and European clergy [38]. All but one of the reports found lower all-cause death rates for clergy compared to the people of similar age in the general population. Protestant ministers consistently were found to have more than a 25% mortality advantage in various studies. Catholic nuns had a mortality advantage of roughly 20%–25%, whereas the mortality advantage of Catholic priests was just over 10%.
In a nationwide cohort of Americans, predominantly Christians, analyses demonstrated a lower risk of death independent of confounders among those reporting religious attendance at least weekly compared to never. The association did not differ by gender or ethnicity [39].
Attendance at religious services (at least weekly compared to never [39]) and prayer were strongly connected to reduced mortality [40,41], and a lower risk of death in a nationwide cohort of 8,450 Americans6, predominantly Christians. People (n = 10,059) who attended religious services ≥40 (40.8%), or <40 times (22.4%) were less likely to have elevated levels of inflammatory markers of cardiovascular disease than non-attendees (36.8%) [42].
The risk of dying from arteriosclerotic heart disease for men who attended church at least once a week was only 60% of the risk of men who attended church infrequently [43]. The same study also found that death rates from pulmonary emphysema were more than twice as high and that liver cirrhosis was almost four times higher for white men who attended church infrequently compared with white men who attended church at least once a week [43].
A 12-year follow up study in industrial 3,638 Jewish Israeli males demonstrated that religiosity had a protective effect on mortality in younger employees, but the reverse was true for older employees (total number) [44].
The lack of objective and non-invasive measurements in this study, however, may be the reason that the mechanisms of these associations were not fully elucidated. Future research should examine methodological and substantive explanations for the discrepancies among these studies.
2.8. Religiosity and Spirituality in Aging
Older adults who reported attending religious services more frequently had better functional recovery following an acute myocardial infarction (AMI) [28] and a more active communal life. In fact, spiritual participation and community involvement were associated with volunteering among adults 60 years or older [45].
Interestingly, rates of volunteering varied by race/ethnicity: Bivariate analyses showed that non-Hispanic white older adults were more likely to participate in formal volunteering activities, while their African American and Hispanic counterparts tended to participate in informal volunteering activities [45]. There is evidence that African Americans rated their private religiosity higher and attended religious services more frequently than Whites [46].
Medically ill older adults, a population of high users of health care services, who attended church weekly or more often were significantly less likely to have been admitted to hospital in the year prior to the study, had fewer hospital admissions, and spent fewer days in the hospital than those attending less often [47]. Patients unaffiliated with a religious community, while not using more acute hospital services in the year before admission, had significantly longer index hospital stays than those affiliated. Unaffiliated patients spent an average of 25 days in hospital, compared with 11 days for affiliated patients; this association strengthened when physical health and other covariates were controlled.
There is the need for objective empirical examinations of these issues in countries other than the United States [48]. Given the positive associations of mental health, spirituality and social engagement with volunteering among older adults, they can be also involved in helping their physicians to use simple exhaled biomarkers measurements (e.g., exhaled NO measurements by a portable analyzer NIOX MINO). The latter was successfully used in general practice in older patients with chronic lung diseases [49].
2.9. Cardio-Vascular Diseases
There is a link between religious commitment and blood pressure, in that more religiously committed patients had lower blood pressures [50]. In fact, blood pressure among the nuns living in a secluded order in six nunneries in Umbria, central Italy, remained remarkably stable during the 30 years’ observation period [51]. None showed a rise in diastolic blood pressure to above 90 mm Hg, in contrast to the laywomen from the same region and similar demographic details. There were also much lower fatal and non-fatal cardiovascular events in the nuns [51].
Re-education in religious and spiritual matters that would involve motivational reorientation of both, public and medical professionals, might revolve around a message that ideal cardiovascular health is much more than crisis intervention and beneficial lifestyle.
A holistic cardiac rehabilitation intervention focusing on several psychosocial and biological predictors of coronary heart disease including depression, low spirituality and others was highly effective in lowering levels of depression and perceived stress, increasing levels of life satisfaction and spirituality upon program completion [52]. Future studies utilizing exhaled biomarker profiling are necessary to determine whether holistic programs are more effective than traditional programs in the reduction of cardiac risk factors.
It has been suggested that a salutary effect of religion on blood pressure can be explained by the combination of the following correlates of religion: the promotion of health-related behavior; hereditary predispositions in particular groups; the healthful psychosocial effects of religious practice; and, the beneficial psychodynamics of belief systems, religious rites, and faith [53].
In addition, it has been found that the rates of hypertension-related morbidity and mortality were significantly lower in typically conservative religious groups than in compared populations [21]. Spiritual wellbeing may be cardio protective, as it has been significantly related to lower systolic and diastolic BP, hs-C-reactive protein, fasting glucose, and marginally lower triglycerides [54].
Little research has focused on the relationship between religious attendance and inflammatory markers of cardiovascular risk. A national representative sample of adults aged ≥40 derived from the National Health and Nutrition Examination Survey III 1988–1994 (n = 10,059) has demonstrated that 40.8% of the population attended religious services 40 or more times in the previous year while 22.4% attended services less than 40 times and 36.8% attended no religious services at all [42]. Non-attendees of religious services were more likely than attendees to have elevated white blood cell counts, highly elevated C-reactive protein, and elevated fibrinogen.
These findings suggest that people who have attended religious services in the previous year are less likely to have elevated levels of certain inflammatory markers, however, current smoking has significant shared variance with religious attendance.
2.10. Diabetes
Diabetes affects 2.8 million people in the UK and 26 million people in the U.S.7 The majority of sufferers have type II of the condition. Spiritual care is an important component of providing culturally sensitive health care to African Americans [55] and Hispanic adults in the USA, 78% of whom believed they had diabetes because it was God's will [56], and other patients [57] with diabetes, facilitating their self-management.
Mormons in Utah may have lower cardiac mortality than other people living in the same State and the US population. A population of 448 patients was surveyed (2004 to 2006) for the association of behavioral factors with coronary artery disease (CAD), with routine fasting (i.e., abstinence from food and drink) as the primary variable [58].
Routine periodic religious fasting in a representative group (n = 448) of Mormons of Utah has been shown to be associated with lower diabetes prevalence [58].
Although diabetics may be exempted from Ramadan fasting, many patients still insist on this worship. In fact, there was no significant change from pre-Ramadan in fasting blood glucose, post-prandial blood glucose, and HbA1c variables in fasting diabetics at post-Ramadan and one-month post-Ramadan [59].
There are several exhaled biomarkers that potentially may be used to monitor the effect of religiosity and spirituality on diabetes, including exhaled carbon monoxide [60], carbon dioxide [61] and hydrocarbons [62,63]. A novel non-invasive method has been developed analyzing human tear proteins enabled by an alkaline microfluidic homogeneous immunoassay [64]. Thus it may be possible to measure tear glucose levels multiple times per day to monitor blood glucose changes without the potential pain from repeated invasive blood drawing methods.
2.11. Asthma
2.11.1. Psychological and Socioeconomic Stress, Inflammatory Biomarkers
Asthmatic airways constrict in response to emotion and stress, and asthma symptoms are less severe in patients with higher religiosity and spirituality. However, the underlying mechanisms, potential extra thoracic contributions, and associations with airway pathophysiology in emotion-induced or spiritual-relieved airway responses have not been elucidated. Psychosocial stress and socioeconomic status (SES) are known to influence the pathophysiology of asthma, including serum inflammatory markers and exaggerated allergen response. Lower SES and related higher levels of stress and threat perception were associated with higher chronic stress and perceived threat, heightened production of IL-5 and IL-13 and higher eosinophil counts in children with asthma [29]. It has been confirmed that chronic stress and threat perception represented statistically significant overlapping pathways between SES and immune processes in children with asthma. Associations among SES, psychological stress, and immune pathways suggest that the experience of stress, particularly among lower SES children, has implications for childhood asthma morbidity [29].
The link between the perceived psychological triggers and stress in patients' daily lives suggests a physiological basis for emotion-induced asthma, as it has been demonstrated by the increased respiratory resistance and exhaled NO during unpleasant films in asthma patients [65,66]. Exhaled NO (FeNO) was a significant mediator of the association of both negative affect and daily hassles with lung function changes, confirming the pathophysiological link between stress and airway inflammation in asthma [66]. Interestingly, this response was blocked by ipratropium bromide and was not substantially associated with asthma severity, airway inflammation, hyper-reactivity and reversibility.
There are several novel biomarkers measured in exhaled breath condensate in asthma, including microsatellite alterations [67] suggestive of organ-specific asthma and atopy, exhaled IL-4 and pH [68].
Furthermore, an inverse association of SES with changes in FeNO levels in response to the conflict task, meaning that as SES declined, greater increases in FeNO were observed [69]. This study suggests that lower SES children with asthma may be more vulnerable to heightened airway inflammation in response to stress.
In asthma elevated rates of exhaled breath temperature changes and bronchial blood flow may be due to increased vascularity of the airway mucosa as a result of inflammation [70,71].
Recent studies have demonstrated lower levels or reactivity of endogenous cortisol in asthma [72]. Indeed, elevated exhaled NO was further increased and low salivary cortisol levels became highly elevated in patients with asthma after the stress protocol [73]. Acute psychosocial stress alone increases airway inflammatory markers in asthma and this increase is attenuated by stronger stress-related activity of the hypothalamic-pituitary-adrenal axis in asthma [73].
2.11.2. Effect of Worship and Lifestyle
It has been shown that engagement in Pentecostal worship is associated with reductions in circulatory salivary cortisol and enhancements in α-amylase activity, reflecting the expected reduction of stress after a day of worship [74]. Religious coping with stress has been shown to be closely related to problem-focused coping [75].
The anthroposophic8 family lifestyle reduces the level of stress and allergic diseases in infants [76]. Salivary samples of 330 infants and their parents demonstrated that low salivary cortisol levels in infants from anthroposophic families vs. families with more conventional lifestyles, may be related to an environment with a lower degree of exposure to stress, which could influence the development of allergic diseases [76].
Although the positive role of religion and spirituality on psychosocial stress and clinical asthma outcomes has been demonstrated, controlled, laboratory paradigms that test associations between religion and spirituality and markers of airway inflammation in asthma are lacking. We speculate that investigating the role of religious coping in asthma may require more complex approaches, including exhaled NO and salivary cortisol measurements.
2.12. Smoking and Chronic Obstructive Pulmonary Disease (COPD)
There are important issues, especially with patients diagnosed with life-limiting illnesses (e.g., COPD). Despite the fact that end-of-life topics are important to patients, most clinicians focus on life-preserving treatments and avoid conversations about end-of-life care. A recent cross-sectional study of COPD outpatients (n = 376) who completed the Quality of Communication (QOC) questionnaire (outcome measure) demonstrated that all end-of-life communication topics were under-addressed by clinicians, regardless of their training [77].
Religious commitment prevents health problems even among people who engage in religiously disapproved behaviors such as smoking. Thus “religious smokers” who attended church at least once a week were four times less likely to have an abnormal diastolic pressure than “less religious smokers” who attended church infrequently [78]. This difference was seven times more evident between “religious” vs. “non-religious” smokers.
A recent study has shown that one session of water pipe smoking (WPS) causes acute biologic potentially harmful changes that might result in marked health problems. These included - increased blood pressure, heart rate, exhaled carbon monoxide (CO) and decreased FEV1, exhaled Feno and 8-isoprostane levels in exhaled breath condensate (EBC) and eosinophils in peripheral blood [79]. Potentially, impulse oscillometry can be used to differentiate patients with asthma from those with COPD [80].
An acute [81] and chronic [82] effect of smoking on exhaled NO, exhaled CO [83] and exhaled 8-isoprostanes [84] have been described. We suggest that monitoring these exhaled biomarkers (NO, CO, 8-isoprostane) might be useful to assess the effect of religiosity in smokers with cardio-vascular problems.
2.13. Depression and Stress
Spiritual and/or religious individuals may experience a protective effect against the neuroendocrine consequences of stress. Young adults with higher composite religiosity/spirituality scores, religiosity, levels of forgiveness and frequency of prayer showed lower cortisol responses to stress [85]. Religiosity may have a protective effect on the physiological effects of stress among women with fibromyalgia [86].
Hyperactivity of the hypothalamic-pituitary-adrenal (HPA)-axis is a common finding in major depressive disorder. Chemokines, in addition to their traditional inflammatory functions, also have neuromodulatory effects, e.g., they are expressed in dopaminergic neurons and affect dopamine turnover [87,88]. Chemokines are also involved in CNS development and in the maintenance of normal brain homeostasis [89].
A few recent studies have shown increased levels of certain chemokines in the blood of depressed patients [88,90].
2.13.1. Chemokines, Cytokines, Neuropeptide Hormones, Matrix Metalloproteinases
Recently, 20 cerebrospinal fluid (CSF) biomarkers were measured in 124 drug-free suicide attempters: kynurenic acid, orexin, homovanillic acid (HVA), 5-hydroxyindoleacetic acid (5-HIAA), 3-methoxy-4-hydroxyphenylglycol, chemokines, matrix metalloproteases and cytokines [88]. Consequently, principal component analysis identified four factors explaining 52.4% of the total variance: factors 1 and 2 were characterized by high loadings of chemokines and cytokines, respectively, and were both associated with severe depressive symptoms; factor 2 was also associated with a high suicidal intent; factor 4 was characterized by strong loadings of the monoamine metabolites 5-HIAA and HVA, as well as orexin and interleukin-6. High scores on this factor were found in patients who performed a violent suicide attempt and in patients who subsequently completed suicide [88].
Concentration of eotaxin in serum was almost 10 times higher in patients with major depressive disorder (MDD) compared to controls [90]. Depressive symptoms were highly associated with high loadings of eotaxins [88], other study also reported low serum levels of the chemokines MCP-1 and MIP-1b in patients with MDD [91].
Recent technological advances in exhaled breath biomarkers measurements offer an opportunity to further elucidate the complex chemokine/cytokine network in MDD and their potential “spiritual modulation”.
We speculate that measuring several inflammatory mediators simultaneously [17], such as eotaxins [92], cytokines and chemokines [93,94,95] levels in exhaled breath condensate may be used to monitor the modulating effect of religiosity and spirituality in patients with depression.
Significant elevations of multiple pro-inflammatory and anti-inflammatory cytokines in patients with depression support a generalized chronic inflammatory state in MDD [88]. Therefore, and implicate additional cytokines and chemokines previously linked to cardiovascular disease.
While the etiology of cytokine elevations in MDD remains unknown and significantly more work is needed, the growing understanding of cytokines in individuals with MDD suggests the intriguing possibility that early intervention, perhaps with anti-inflammatory agents and/or antioxidants, might reduce or prevent downstream medical consequences of MDD.
Corticotrophin-releasing hormone (CRH) in CSF, urinary and salivary cortisol were monitored in the suicide attempters for approximately 12 years after the index admission [96]. Low cortisol levels were associated with severe psychiatric symptoms, and lower evening salivary cortisol was found in suicide attempters compared to controls. Among women, repeated suicide attempts were associated with low morning and lunch salivary and urinary cortisol and CRH levels.
Therefore, easily detectable (salivary or exhaled breath condensate) hypocortisolism may serve not only as a predictor of a suicidal attempt, but also of the potential positive role of religion in these patients.
Religious commitment has been associated with a decreased prevalence of depression [97,98]. Higher levels of religiosity may protect against one of the most severe outcomes of depression: suicide [99].
The reported results suggest that specific combinations of CSF and, potentially exhaled, biomarkers may discriminate between types of suicidal behavior and indicate an increased risk for future suicide and the role of religiosity and spirituality as a preventing means.
2.14. Lifestyle and Nutrition
Mormons in Utah may have lower cardiac mortality than other people in the same State and the US population. A population of 448 patients was surveyed (2004 to 2006) for the association of behavioral factors with coronary artery disease (CAD), with routine fasting (i.e., abstinence from food and drink) as the primary variable [58]. Routine periodic fasting was associated with lower risk of CAD (64% vs. 76%), and this remained after adjustment for traditional risk factors. Fasting was also associated with lower diabetes prevalence. Therefore, not only proscription of tobacco, but also routine periodic fasting was associated with a lower risk of CAD.
Future research should include an examination of the links between religious involvement and other important lifestyle factors that may influence maternal and child health. Thus, pregnant and postpartum women frequently (more than once a week) and regularly (once a week) attending church services had 80% and 60%, respectively, lower odds of drinking alcohol compared to women who attended less than once a week [100]. Similar patterns surfaced with regard to smoking tobacco, with the odds of smoking being roughly 85% lower among frequent attenders, and nearly 65% lower among regular attenders.
Various health effects of religious activities of different religions and religious groups have been described. Thus, fasting during the holy month, Ramadan, is a religious obligation for all adult healthy Muslims. During this month, Muslims are allowed to eat and drink between sunset and dawn. However, they are not allowed to eat and drink after dawn. Indeed, beneficial effects of fasting during Ramadan on neutrophil phagocytic function biomarkers have been included [101].
There is only one published paper investigating a link between religious style of life and exhaled breath analysis using thermal desorption gas chromatography mass spectrometry (TD-GC-MS) [102]. Male monks fasting for 63 hours9 were examined as a group that simulates the medical status of victims entrapped under the ruins of collapsed buildings after an earthquake to be found by their exhaled breath. Religious fast resulted in a 30-fold increase of acetone concentration (5.8 ppm) which was similar to the reported 15-fold increase after 24-hour fasting [103], and to the levels in diabetes (1.7–3.7 ppm) [62]. A significant number of hydrocarbons has also been identified, suggesting high levels of oxidative stress in fasting monks.
2.15. Complementary and Alternative Medicine (CAM) Phenomenon
The search for the spiritual a dimension in their medical care may be behind the recent and strong trend towards the use of complementary and alternative medicine (CAM)10 in conjunction with conventional medicine: According to the 2002 National Health Interview Survey based on 31,044 interviews [104], 54.9% individuals seek the help of CAM. It has been reported that some forms of CAM were used by 36% of U.S. adults aged 18 years, or by 62% when prayer specifically for health reasons was included in the definition of CAM [104].
The prevalence of CAM use for treatment remains high (2007 U.S. National Health Interview Survey, n = 20,710) among adults (86.9%), regardless of their functional status, although mind-body therapies (MBT) (39.3% versus 17.4%, p < 0.001) were prevalent in patients with functional limitations. Moreover, the belief in miracles is found to be common in the U.S., and it is an important determinant of how decisions are made for those with advanced illness [104].
A recent cross-sectional survey of 328 patients attending an urban general practice in the Republic of Ireland demonstrated that 27% of the patients had visited a CAM practitioner within the past 12 months [105]. A significant positive association was found between CAM use and female gender, middle-aged, private health insurance and full time employment, and the most common reason for use was “to treat an illness for which conventional medicine was already sought” (42%). Interestingly, a high rate of non-disclosure to GPs was found (41% patients) and personal recommendation was the most important source of information (53.2%).
One of the reasons for patients turning to CAM treatment is the eroding the state of the art of medicine when medical scientists set themselves apart from the doctor-patient relationship in order to obtain a knowledge that is stripped of personal elements [106].
Religious and spirituality research offers promise in breaking down the dichotomy between the art of medicine and science by directing scientific investigations to techniques of ameliorating illness, thus enhancing the art of medicine and patient care [106].
The prevalence of CAM use for treatment, including combination of CAM and prayer for health, is high. Public health strategies are needed to promote increased screening for spirituality use in CAM by health care providers, promote increased use of objective non-invasive means, i.e., exhaled biomarkers to monitor therapeutic effects of CAM which will promote health care interactions and facilitate communication about CAM safety and efficacy [107].
This also indicates that the current popularity of an alternative healthcare system and the extent to which modern patients have turned to “spirituality in treatment” are approached with the hope that they would help treat and prevent disease and enhance quality of life.
Many important questions remain to be answered in pursuit of the goal of individualized medicine via therapeutically-oriented research on the religion/spirituality effect. Constructing individual and objective patient profiles and their changes in the course of treatment by using non-invasive exhaled biomarkers might be of great value for physicians necessarily relying on individualized judgments about how to relate to particular patients. It is reasonable to suppose that the interaction between clinicians and patients is more or less likely to promote optimal therapeutic outcomes; and these interactions can be evaluated by exhaled biomarkers.
2.16. Religious, Ethnic and Behavioral Differences in Health
The role of religion in the patterning of health inequities and how this is related to ethnicity and socioeconomic status has been studied in 14,924 Christians, 4,337 Muslims, 656 Sikhs, 1,197 Hindus and 2,682 people reporting not to identify with any religion with different ethnic backgrounds, who were interviewed as part of the Health Survey for England in either 1999 or 2004, adjusted for age, gender and socioeconomic status and periodicity [108]. Multivariate analyses using nationally representative data were performed on self-assessed fair or poor health, longstanding limiting illness, diagnosed diabetes, diagnosed hypertension, waist–hip ratio, body mass index, current tobacco use and participation in no regular physical activity.
As expected, the odds ratios for general health, hypertension, diabetes, waist-hip ratio, tobacco use and physical activity stressed the importance of ethnicity in the patterning of health inequalities. Unexpectedly, however, there was strong evidence of an important, independent role for religion, with risks for the different health indicators varying between people with the same ethnic, but different religious, identifications [108].
Non-Christians were more likely to report activity-limiting illnesses than Christians, regardless of ethnicity. More importantly, the risks for the different health outcomes often varied between groups with the same ethnic, but different religious, associations. The ethnic/religious patterning of health also varied considerably by gender, supporting the need to explore the health risks of men and women separately [108].
Several non-invasive exhaled biomarkers were successfully used for recognition of ethnic differences in both adults and children. Differences in FeNO and forced expiratory lung volumes between South Asian and white children were found to be evident and existed from a very young age [109], also reference ranges for FeNO in healthy Japanese adults were similar to those of Caucasians [110]. Immigrant children of Turkish and Moroccan origin showed a higher prevalence of allergic sensitization and FeNO compared to Dutch children [111].
These findings show important differences in the health of people of different religions, suggesting that our understanding of health inequalities can be further enhanced by relevant non-invasive biomarkers that measure the impact of this underlying heterogeneity.
The effect of closely intertwined social and religious ideologies on health risk behaviors in sexual minority youths in the United States has been recently reported by Hatzenbuehler et al. [112]. The central finding of this study is that the religious climate surrounding lesbian, gay, and bisexual (LGB) youths serves as a determinant of their health risk behaviors. Although a similar influence was found among heterosexual youths, it was more strongly associated with the health behaviors of LGB youths [112].
Contrasting results have been recently reported of a protective effect of religion on health in heterosexual youths and its lack among LGB youths [113], vs. the data that showed that LGB youths living in counties with more supportive religious climates exhibited fewer health risk behaviors, indicating that religion can be protective for LGB youths [112]. An objective measure of the religious climate assessed at the ecological level in the latter study, vs. an individual-level measurements of the environment (e.g., perceived discrimination) used in the latter study, provided the methodological limitations of existing studies on environmental risk factors and health risk behaviors among LGB individuals, which have relied on individual-level measurements of the environment (e.g., perceived discrimination).
Therefore, further research is needed, exploring novel objective biomarkers that are not confounded with health status that, potentially, may lead to biased estimates of the association between religion and health of members of socially disadvantaged groups.
2.17. The Efficacy of Prayer11
C.S. Lewis wrote:
[“Medicine, as all true doctors admit, is not an exact science. You need not, unless you choose, believe in a causal connection between the prayers and the recovery. For prayer is request. The essence of request is that it may or may not be granted”][114]
Although the majority of studies reviewed rely on correlational data, there is nevertheless considerable evidence that prayer, religiosity, and spirituality can be associated with health benefits. This is the case despite the fact that the correlations between prayer and other religious behaviors are rarely reported or controlled statistically (or experimentally) to understand the unique contribution of prayer to health [2].
The empirical results from recent randomized controlled studies on remote, intercessory prayer remain mixed.
Several studies have, however, appeared in prestigious medical journals, and it is believed by many researchers, including apparent skeptics, that it makes sense to study intercessory prayer (IP) as if it were just another experimental drug treatment [115]. Among the many recent attempts to demonstrate the medical benefits of religious activity, the methodologically strongest seem to be studies of the effects of distant IP. There are several studies ranging from highly critical [116,117], to moderately positive [118,119,120] and highly positive [121,122].
Generally, claims of benefits of IP are not well supported by well-controlled clinical trials. It is still unclear whether prayer itself or knowledge that IP is being provided may influence outcome [123]. Periodic reassessment of epistemological assumptions on which the majority of research domains are based is important, because they influence our interpretation of experimental outcomes, especially in the studies of IP.
Some of the early IP studies claimed that the “randomized double-blind design” was used, when one hospitalized group of patients received IP by participating Christians praying outside the hospital, and the control group did not [124]. Indeed, it was observed that the IP group of cardiac patients had a significantly lower severity score compared with the control patients who required ventilator assistance, antibiotics, and diuretics more frequently [124].
Intercessory prayer did not significantly decrease the odds of cardiac patients experiencing a bad or intermediate outcome, nor did it affect their mortality rate [125]. This, however, may be due to the inclusion of an assumption of poor outcome for those not accounted for in the final analyses. Although based on heterogeneous data, another Cochrane review (10 studies, 7,646 patients) reported no statistically significant effect of intercessory prayer for re-admission to a Coronary Care Unit [126].
A more recent study (Study on the Therapeutic Effects of intercessory Prayer, STEP) was conducted at six US hospitals to evaluate whether receiving IP or being certain of receiving IP was associated with uncomplicated recovery after coronary artery bypass graft (CABG) surgery [123]. It was concluded that IP itself had no effect on complication-free recovery from CABG, but certainty of receiving intercessory prayer was associated with a higher incidence of complications.
The paper by Schwartz and Dossey [127] argues that the dose-dependent design characteristic of drug trials, and the adopted use in the STEP and other studies concerning blindness and randomization, is not the optimal model for intention-healing research and must be reappraised. New lines of research linking belief and intention with novel informative biomarkers may be important for an accurate and meaningful study outcome. Major problems with the data on IP are the lack of objective outcome variables, raising problems of multiple comparisons. Apart from the need of more rigorous experimental, longitudinal protocols and comparisons of prayer with known treatments, future studies need to be based on investigations with proper measures of control variables.
Integration of religious or spiritual dimensions of an individual's life into therapeutic activities raises important ethical considerations. Prayer may be considered as either alternative or as an adjunct to conventional medical therapy. Most of the physicians and clerics will strongly discourage the former and the majority of patients will desire the adjunct model. In the future, a helpful principle may be to inform but not to recommend [5].
Before the gap between prayerful and medical practice can be bridged, research into the efficacy of prayer and religiosity might need to be reconstructed, considering humans as integrated, multifactorial beings living within a complex milieu [2]. Then, prayer, religiosity, and spirituality might be assessed and understood better, and the influence of spirituality and prayer within humans' daily lives might be more accepted.
The use of prayer as a therapeutic resource and the means of its assessment in published peer reviewed journals are the focus of this review. No attempt will be made to advocate prayer as a therapeutic supplement to any therapy, or to validate prayer purely scientifically. It is agreeable, however, that the self-reported frequency of prayer may be superficially related to the personal and underlying meaning of religion [23].
This work may also represent an important step in the convergence of multiple realms of research by linking various biomarkers and physiological measures with indicators of individual belief systems.
2.17.1. Prayer and Various Clinical Conditions
2.17.1.1. Stress
Engagement in church worship is associated with reduction in stress. Salivary cortisol, as a biomarker of stress and sympathetic nervous system activity, was measured in a group (n = 52) of Apostolic Pentecostals in New York's mid-Hudson Valley [74]. Saliva samples were collected at four predetermined times on consecutive Sundays and Mondays to establish diurnal profiles and compare days of worship and non-worship.
A significant decrease in cortisol and an increase in α-amylase on a non-worship day compared with a service day were demonstrated [74]. This suggests that engaging in religious worship activities would reduce baseline stress levels after a day of worship among Pentecostals, and may be monitored by simple non-invasive salivary biomarkers. Greater composite religiosity/spirituality, religiosity, frequency of prayer and attendance at services of young adults were associated with lower blood pressure in males, elevated blood pressure in females, and lower cortisol responses to stress [85].
2.17.1.2. Cancer
Spiritual healing practices such as faith healing and prayer have been found to be some of the most common strategies used by patients with various types of cancer [24,128].
The recent advances in the psycho-oncological and psycho-neuroimmunological investigations of cancer patients has allowed the rediscovery of the importance of spiritual faith in influencing the clinical course of neoplastic disease, not only in terms of supportive care but also as a potential prognostic variable [129]. The tumor response rate and three-year survival achieved in a group of 50 metastatic non-small cell lung cancer (NSCLC) patients with a high degree of faith was significantly higher than in the other group of patients [129]. Moreover, the mean post-chemotherapeutic lymphocyte number was significantly higher in the patients with evident spiritual faith than in the other patients. This study also suggests that the effect of faith may be assessed by various lymphocyte-mediated biomarkers.
There are several non-invasive biomarkers measurable in exhaled breath condensate, such as ferritin and superoxide dismutase [130], LTB-4 and IL-8 [131], microsatellite alterations (MAs) at the long arm of chromosome 19 [132], cyclooxygenase (COX-2) and survivin [133], IL-2, TNF-alpha and leptin [134], which, if deemed feasible, have clinical implications in the monitoring of lung cancer and as an religious outcome predictor.
2.17.1.3. Arthritis
Patients with long-standing moderately severe rheumatoid arthritis (RA) were shown to derive significant short- and long-term physical benefits (pain and functional impairment, physical signs, erythrocyte sedimentation rate and C-reactive protein) from in-person intercessory prayer ministry [22]. The specific therapeutic agent of prayer could not be proven definitively, because the intervention was multimodal, combining the putative factor of prayer ministry with group education and counseling. Increased hydrogen peroxide in RA [135] may be used to monitor the effect of intercessory prayer in the treatment of these patients.
2.17.1.4. Open-heart Surgery
The major finding of this paper of 295 middle age patients undergoing open-heart surgery was unexpected. Of the four major types, only the use of “petitionary” prayer was related to better postoperative well-being, mediated through optimism, whereas “conversational” prayer was associated with poor outcomes, mediated through acute stress [136].
The results of another trial in IP were less optimistic: IP itself had no effect on complication-free recovery from coronary artery bypass graft (CABG), but certainty of receiving intercessory prayer was associated with a higher incidence of complications [123].
Lower pre-operative exhaled NO and its reduced response to nitroglycerin accompanied pulmonary vascular dysfunction in patients after open-heart surgery [137]. The possibility of using exhaled nitric oxide dynamics to investigate the effect of prayer in cardiac patients with pulmonary endothelial dysfunction merits further studies.
2.17.1.5. Alzheimer’s Disease
Spiritual practices are meaningful activities to connect with patients’ personal faith, important memories, and present support. Prayer was the most important spiritual practice used for coping by patients with Alzheimer’s disease (AD) [138]. Prayer provided a personal connection with God, produced beneficial effects of emotional healing, reassurance, and hope, and was important to persons with Alzheimer’s disease because it provides a sense of control over the progressive cognitive impairment [139].
Another important spiritual practice used for coping was engagement in church activities, which provided vital connections with other people and possibly a sense of belonging and identity for the individual with AD. Since AD interferes with verbal communication and comprehension of conversations, individuals with AD often become socially isolated. In addition, losing one’s memory also means losing one’s self-identity. Being a member of a faith community is an identity; therefore, it may provide a sense of belonging and offer opportunities to break the social isolation.
Interestingly, the two participants in this study who spoke of feeling isolated also no longer attended the churches that they had attended for many years. Notably over half of the study participants continued to serve in church roles fulfilling their need to be useful and productive [138], differing from Snyder’s participants [140] who reported decreased attendance.
2.18. Belief and Expectation: Their Role in Health and Disease, Placebo Effect
An objective identification of a potential religious placebo effect and its extent are extremely important. It is likely that religious/spiritual activities may provide a greater placebo effect than conventional medicine, but at present there is little empirical supporting evidence. There are certain similarities between the placebo and religion/spirituality effects in health and disease. These include the ritual of treatment (vs. the ritual of a religious service, regular treatment vs. regular spiritual practice), the clinician-patient (clergy-patient) relationship, and the hope for relief that requires either a self-generated cognitive/emotional response (vs.intercessory prayer) or the intervention of others (physicians vs. clericals). Although there is no "real" drug involved in both (placebo and religion/spirituality), the actual positive consequences of their “administration” may well be physiological, emotional, behavioral, and/or cognitive, and real.
Both of them need the emotional trigger of hope for relief in order to activate internal healing mechanisms; and both of them require the intervention of others, rather than self-generated cognitive/emotional responses, additionally, the spiritual effect can be generated independently of other people. Part of why the phenomenon of the spiritual effect on disease and illness has been relatively neglected within biomedicine is that the latter focuses on a biological conception of disease that is treated by technological interventions (drugs, medical procedures, implanted devices, and surgery). The doctor-patient relationship, as a means of treatment, has also been largely ignored by scientific medicine [141].
We suggest that a new way of thinking and considering the therapeutic equality of words and rituals and real drugs may have profound implications both for clinical trials and for medical practice. Indeed, recent research has revealed that words and ritual-induced biochemical and cellular changes in a patient's brain are very similar to those induced by drugs [142].
The “spiritual placebo effects” are not chemically generated and are due only to the subject's optimistic belief and expectation that the spiritual interactions will produce positive consequences. It has been shown that the expectation of reward (in this case, the expectation of clinical benefit) [143] influences the clinical benefit associated in both verum and placebo groups [144].
The major mechanism of the placebo effect is the patient’s belief/expectation that this medication or procedure will help them with their disease [145,146].
The placebo effect also depends on the informational context. Lower expectations, when patients are told that they may get either a drug or a masked placebo [147], will reduce its effect. In contrast, higher expectations, when placebos are presented deceptively as a known beneficial [148,149,150] or more expensive [151] treatment, increase its effect.
Spiritual experiences and practices involve a variety of physiological mechanisms that are comparable if not identical to those engaged in placebo responses. It has been suggested that meaningfulness seems to be both a hallmark of spirituality and placebo reactions [152], suggesting that spirituality, under certain conditions, may be a predictor of placebo response and effect. Therefore, it may be regarded as an overarching psychological concept that is important in engaging and facilitating psychophysiological mechanisms that are involved in health-related effects of spirituality.
Development of novel objective techniques of religiosity and spirituality assessment, is not merely of theoretical interest, but may also be clinically relevant. Caution needs to be exercised before applying these techniques in patients, for both secular and religious orientation, as for some patients, focusing upon their spirituality may become an additional source of distress and anxiety.
3. Conclusions
Research increasingly demonstrates that religiosity and spirituality are associated with measurable and clinically significant impacts on people’s health. The majority of end-of-life communication between the physicians and patients, especially with those diagnosed with life-limiting illnesses, are under-addressed by clinicians [77].
There are well more than 100 instruments in the published literature to study religion and spirituality [153,154]. A total of 564 research studies were identified in nursing research journals for the period 1995–1999, of which 12% included at least one measure of spirituality or religiousness [154]. The majority of these studies (although only 19.3%) were qualitative and contained a measure of religion or spirituality, compared to 9.9% quantitative studies.
There are several major and common limitations of these developed tests:
- Influenced by culture, ethnic and other factors. Thus, the psychometric properties of the STS [160], SELF [161], SOI [157] tests have been shown to be reliable with American, but not with the samples outside of American culture (in Indian students and teachers, for example, due to a mixture of Hindu, Christian, and Muslim participants).
- Lack of standardization, reliability and validity studies, including cross-cultural and language validation.
However, there is little convergence of tests used across studies and the absence of any objective non-invasive biomarkers assessments.
This is the case despite the fact that most patients desire to be offered basic spiritual care by their clinicians.
The vast majority of the studies investigating the connection between religious involvement and good health are correlational, use inadequate measures of religious commitment (e.g., religious denomination or other single-item measures), and seldom assess the intensity of religious commitment [4]. Nevertheless, a beneficial, or salutary, effect for religious or spiritual involvement on physical and mental health status is clearly shown. Professional medical and clerical associations and educational institutions are beginning to provide clinicians information on how to incorporate spirituality into practice [162]. Deistic, agnostic and atheistic people may have various and quite different lifestyles and moralities compared to their Christian counterparts.
In fact, it has been shown that a Christian and an atheist would react differently when presented with a concept like God, and this will be paralleled with brain activation [163]. The results indicate that the anxiolytic power of religion, as reflected by the reduction of the error-related negativity (ERN), a neural signal biomarker derived from anterior cingulate cortex, is clearly seen in believers.
In contrast, priming non-believers with religious concepts causes an increase in ERN amplitude [163]. This would seem to suggest, from an atheistic point of view, as it was expressed by Stenger in his book “God the failed hypothesis” [164], a power of the mind that goes beyond known physical capabilities. It is agreeable that this would also emphasize the need for a series of quantitative, repeatable (under similar conditions and by different and independent investigators), performing the study without any prejudgment of how the results should come out [164].
To conclude, we identified several religious and spiritual factors and mechanisms, associated with different human conditions and symptoms in health and disease. This review is the first attempt to identify several potential “religious and spiritual” non-invasive biomarkers in different patients and healthy subjects.
Considering that the multidimensional character of most concepts and phenomena in spiritual and religious matters are complex, one-dimensional instruments/approaches may not be sufficient for most research purposes.
Research into spiritual and religious profiles by using multiple exhaled biomarkers is at its early stage. Although there is a clear increase of the number of publications on religion-mortality, new research should include the analysis of more dimensions of religious involvement, including religious life histories; different race, ethnic and socioeconomic groups; correlation with a wider set of social, psychological, and behavioral mechanisms by which religion and spirituality may be related to health and disease. We also suggest that such an approach may lead to more individualized treatment options in the future.
Therefore, the following may be recommended:
- Within a single study, use multiple biomarkers to build up an individual “spiritual profile” of a patient.
- Considering that the multidimensional character of most concepts and phenomena in spiritual and religious matters are complex, one-dimensional instruments/approaches that assess these constructs as a global entity may not be sufficient for most research purposes.
- Investigating spiritual and religious profiles by using multiple exhaled biomarkers and integrative approaches, such as metabolomics for the systematic study of the unique chemical fingerprints found in specific cellular processes, should be considered.
- Considering the need to study fast changes in spiritual and religious profiles of patients receiving treatments, a single marker, for example exhaled nitric oxide, can be used and measured on-line with an individual portable instrument, for example with NIOX MINO.
- If an investigator is going to use tests in a study, then consideration should be given to using multidimensional measurements. Ideally, profiles of exhaled biomarkers should be combined with psychometric tests and with other operational measures (e.g., behavioral observation, structured or semi-structured interviews) so that studies utilize a multidimensional approach to gather data for any given construct.
Acknowledgments
I am grateful to Bulgakova Alvira and Kharitonova Irina who assisted me in shaping this work.
- 1 ICD-9-CM V62.89 is a billable medical code that can be used to specify a diagnosis on a reimbursement claim. The Web's Free Medical Coding Resource (http://www.icd9data.com/2012/Volume1/V01-V91/V60-V69/V62/V62.89.htm).
- 3 Not only the human mind, but the whole person was created in the image of God, according to the Biblical doctrine and teaching of St. Gregory Palamas (Homily 16, P.G. cli, 193B).
- 5 The Hebrew word for healing (napha, רָפָא) can refer not just to physical healing, but to spiritual healing: Ps. 41:4 - "Heal my soul, for I have sinned"; Isa. 6:10 - "repent and be healed".
- 6 The Third National Health and Nutrition Examination Survey (NHANES III) is one of the largest studies to provide population-based data on the association of attendance at religious services and survival in a nation-wide representative sample of Americans and the first to incorporate physical examinations and biochemical data.
- 8 Anthroposophy, a philosophy founded by Rudolf Steiner, postulates the existence of an objective, intellectually comprehensible spiritual world accessible to direct experience through inner development.
- 9 As part of the religious tradition, all the monasteries located in Mount Athos (Chalkidiki, Greece) abstain from food and water for three days at the onset of the Easter fast in order to cleanse body and spirit.
- 10 CAM is defined as a group of diverse medical and health care systems, practices, and products that are not presently considered to be part of conventional medicine.
- 11 “The efficacy of prayer” is an essay written by Clive Staples Lewis who was a novelist, academic, medievalist, literary critic, essayist, lay theologian and Christian apologist.
References and Notes
- J. Levin, and H. Vanderpool. “Is frequent religious attendance really conducive to better health? Toward an epidemiology of religion.” Soc. Sci. Med. 24 (1987): 589–600. [Google Scholar] [CrossRef]
- D.P. O'Hara. “Is there a role for prayer and spirituality in health care? ” Med. Clin. North. Am. 86 (2002): 33–46. [Google Scholar] [CrossRef]
- C.M. Puchalski. “Spirituality and medicine: Curricula in medical education.” J. Cancer. Educ. 21 (2006): 14–18. [Google Scholar] [CrossRef]
- S. Waldfogel. “Spirituality in medicine.” Prim. Care 24 (1997): 963–976. [Google Scholar] [CrossRef]
- J.W. Lomax, R.S. Karff, and G.P. McKenny. “Ethical considerations in the integration of religion and psychotherapy: Three perspectives.” Psychiatr. Clin. North Am. 25 (2002): A547–A559. [Google Scholar] [CrossRef]
- D. Lukoff, F. Lu, and R. Turner. “From spiritual emergency to spiritual problem: The transpersonal roots of the new dsm-iv category.” J. Hum. Psychol. 38 (1998): 21–50. [Google Scholar] [CrossRef]
- G. Milstein, E. Mildarsky, B.G. Link, P.J. Raue, and M.L. Bruce. “Assessing problems with religious content: A comparison of rabbis and psychologists.” J. Nerv. Ment. Dis. 188 (2000): 608–615. [Google Scholar] [CrossRef]
- H.G. Koenig. “Religion, spirituality, and medicine: How are they related and what does it mean? ” Mayo Cli. Proc. 76 (2001): 1189–1191. [Google Scholar] [CrossRef]
- AAMC American Association of Medical Colleges, Medical School Objectives Projects Report 1, Learning Objectives for Medical School Education, Guidelines for Medical Schools, Washington, DC, USA: AAMC, 1998.
- M.E. Ronald, F. Peter, F. Kevin, G.S. Cleveland, C.M. Sean, L.K. Richard, and R.D. Paul. “Measuring patient-centered communication in patient-physician consultations: Theoretical and practical issues.” Soc. Sci. Med. 61 (2005): 1516–1528. [Google Scholar] [CrossRef]
- C. Zimmermann, H. de Haes, and A. Visser. “Enhancing the patient position in the world of health care: Contributions from the each conference 2010 in Verona.” Pat. Educ. Couns. 84 (2011): 283–286. [Google Scholar] [CrossRef]
- J.M. Bredle, J.M. Salsman, S.M. Debb, B.J. Arnold, and D. Cella. “Spiritual well-being as a component of health-related quality of life: The functional assessment of chronic illness therapy—spiritual well-being scale (facit-sp).” Religions 2 (2011): 77–94. [Google Scholar] [CrossRef]
- D. Rosmarin, A. Wachholtz, and A. Ai. “Beyond descriptive research: Advancing the study of spirituality and health.” J. Behav. Med. 34 (2011): 409–413. [Google Scholar] [CrossRef]
- M. Corradi, P. Gergelova, E. Di Pilato, G. Folesani, M. Goldoni, R. Andreoli, L. Selis, and A. Mutti. “Effect of exposure to detergents and other chemicals on biomarkers of pulmonary response in exhaled breath from hospital cleaners: A pilot study.” Int. Arch. Occup. Environ. Health., 2011, 1–8. [Google Scholar]
- A. Amann, M. Corradi, P. Mazzone, and A. Mutti. “Lung cancer biomarkers in exhaled breath.” Expert. Rev. Mol. Diagn. 11 (2011): 207–217. [Google Scholar] [CrossRef]
- S.A. Kharitonov, F. Gonio, C. Kelly, S. Meah, and P.J. Barnes. “Reproducibility of exhaled nitric oxide measurements in healthy and asthmatic adults and children.” Eur. Respir. J. 21 (2003): 433–438. [Google Scholar] [CrossRef]
- S.A. Kharitonov, and P.J. Barnes. “Exhaled biomarkers.” Chest 130 (2006): 1541–1546. [Google Scholar] [CrossRef]
- T. D. Robin. “Using biomarkers in the assessment of airways disease.” J. Allergy. Clin. Immunol. 128 (2011): 927–934. [Google Scholar] [CrossRef]
- R.A. Dweik, P.B. Boggs, S.C. Erzurum, C.G. Irvin, M.W. Leigh, J.O. Lundberg, A.-C. Olin, A.L. Plummer, and D.R. Taylor. “On behalf of the American Thoracic Society Committee on Interpretation of Exhaled Nitric Oxide Levels for Clinical Applications. An official ats clinical practice guideline: Interpretation of exhaled nitric oxide levels (feno) for clinical applications.” Am. J. Respir. Crit. Care Med. 184 (2011): 602–615. [Google Scholar] [CrossRef]
- B. Waldron-Perrine, L.J. Rapport, R.A. Hanks, M. Lumley, S.-J. Meachen, and P. Hubbarth. “Religion and spirituality in rehabilitation outcomes among individuals with traumatic brain injury.” Rehabil. Psychol. 56 (2011): 107–116. [Google Scholar] [CrossRef]
- D.A. Matthews, M.E. McCullough, D.B. Larson, H.G. Koenig, J.P. Swyers, and M.G. Milano. “Religious commitment and health status: A review of the research and implications for family medicine.” Arch. Fam. Med. 7 (1998): 118–124. [Google Scholar] [CrossRef]
- D.A. Matthews. “Prayer and spirituality.” Rheum. Dis. Clin. North Am. 26 (2000): 177–187. [Google Scholar] [CrossRef]
- R.P. Sloan, E. Bagiella, L. VandeCreek, M. Hover, C. Casalone, T.J. Hirsch, Y. Hasan, R. Kreger, and P. Poulos. “Should physicians prescribe religious activities? ” NEJM 342 (2000): 1913–1916. [Google Scholar]
- E.D. Boudreaux, E. O'Hea, and R. Chasuk. “Spiritual role in healing: An alternative way of thinking.” Prim. Care 29 (2002): 439–454. [Google Scholar] [CrossRef]
- S.G. Post, C.M. Puchalski, and D.B. Larson. “Physicians and patient spirituality: Professional boundaries, competency, and ethics.” Ann. Intern. Med. 132 (2000): 578–583. [Google Scholar]
- W.R.T. Miller, and E. Carl. “Spirituality, religion, and health: An emerging research field.” Am. Psychol. 58 (2003): 24–35. [Google Scholar] [CrossRef]
- T.E. Woods, and G.H. Ironson. “Religion and spirituality in the face of illness.” J. Health. Psychol. 4 (1999): 393–412. [Google Scholar] [CrossRef]
- K. Martin, and B. Levy. “Opposing trends of religious attendance and religiosity in predicting elders’ functional recovery after an acute myocardial infarction.” J. Relig. Health 45 (2006): 440–451. [Google Scholar] [CrossRef]
- E. Chen, M.D. Hanson, L.Q. Paterson, M.J. Griffin, H.A. Walker, and G.E. Miller. “Socioeconomic status and inflammatory processes in childhood asthma: The role of psychological stress.” J. Allergy Clin. Immunol. 117 (2006): 1014–1020. [Google Scholar]
- Z. Djuric, C.E. Bird, A. Furumoto-Dawson, G.H. Rauscher, M.T. Ruffin, R.P. Stowe, K.L. Tucker, and C.M. Masi. “Biomarkers of psychological stress in health disparities research.” Open Biomark J. 1 (2010): 7–19. [Google Scholar]
- C.M. Puchalski, R.E. Dorff, and I.Y. Hendi. “Spirituality, religion, and healing in palliative care.” Clin. Geriatr. Med. 20 (2004): 689–714. [Google Scholar] [CrossRef]
- I. Tuck, S.C. Johnson, M. Kuznetsova, C. McCrocklin, M. Baxter, and L.K. Bennington. “Sacred healing stories told at the end of life.” J. Holist. Nurs. 30 (2011): 69–80. [Google Scholar]
- A. Roberts, J. Donaldson, A.C. Coxe, A. Menzies, E.C. Richardson, and B. Pick. Against heresies (St Irenaeus). The Ante-nicene Fathers. Translations of the Writings of the Fathers down to A.D. 325. Buffalo, NY, USA: The Christian Literature Publishing Company, 1885, Chapter 6. [Google Scholar]
- A. Flannery. The Conciliar and Post Conciliar Documents, Vatican Council II. Dublin, Ireland: Dominican Publications, 1975, p. 1062. [Google Scholar]
- A.B. Astrow, C.M. Puchalski, and D.P. Sulmasy. “Religion, spirituality, and health care: Social, ethical, and practical considerations.” Am. J. Med. 110 (2001): 283–287. [Google Scholar] [CrossRef]
- P.S. Mueller, D.J. Plevak, and T.A. Rummans. “Religious involvement, spirituality, and medicine: Implications for clinical practice.” Mayo. Clin. Proc. 76 (2001): 1225–1235. [Google Scholar] [CrossRef]
- R.A. Hummer, C.G. Ellison, R.G. Rogers, B.E. Moulton, and R.R. Romero. “Religious involvement and adult mortality in the united states: Review and perspective.” South. Med. J. 97 (2004): 1223–1230. [Google Scholar] [CrossRef]
- K.J. Flannelly, A.J. Weaver, D.B. Larson, and H.G. Koenig. “A review of mortality research on clergy and other religious professionals.” J. Relig. Health 41 (2002): 57–68. [Google Scholar] [CrossRef]
- R.F. Gillum, D.E. King, T.O. Obisesan, and H.G. Koenig. “Frequency of attendance at religious services and mortality in a u.S. National cohort.” Ann. Epidemiol. 18 (2008): 124–129. [Google Scholar]
- L.H. Powell, S. Leila, and C.E. Thoresen. “Religion and spirituality. Linkages to physical health.” Am. Psychol. 58 (2003): 36–52. [Google Scholar] [CrossRef]
- E. Bagiella, V. Hong, and R.P. Sloan. “Religious attendance as a predictor of survival in the epese cohorts.” Int. J. Epidemiol. 34 (2005): 443–451. [Google Scholar] [CrossRef]
- D.E. King, A.G. Mainous, T.E. Steyer, and W. Pearson. “The relationship between attendance at religious services and cardiovascular inflammatory markers.” Int. J. Psychiatr. Med. 31 (2001): 415–425. [Google Scholar]
- G.W. Comstock, and K. Partridg. “Church attendance and health.” J. Chronic. Dis. 25 (1972): 665–672. [Google Scholar] [CrossRef]
- A. Kraut, S. Melamed, D. Gofer, and P. Froom. “Association of self-reported religiosity and mortality in industrial employees: The CORDIS study.” Soc. Sci. Med. 58 (2004): 595–602. [Google Scholar] [CrossRef]
- S. Ahn, K.L. Phillips, M.L. Smith, and M.G. Ory. “Correlates of volunteering among aging texans: The roles of health indicators, spirituality, and social engagement.” Maturitas 69 (2011): 257–262. [Google Scholar] [CrossRef]
- R.J. Taylor, L.M. Chatters, and J.S. Jackson. “Religious and spiritual involvement among older african americans, caribbean blacks, and non-hispanic whites: Findings from the national survey of american life.” J. Gerontol. B Psychol. Sci. Soc. Sci. 62 (2007): S238–S250. [Google Scholar] [CrossRef]
- H.G. Koenig, and D.B. Larson. “Use of hospital services, religious attendance, and religious affiliation.” South Med. J. 91 (1998): 925–932. [Google Scholar] [CrossRef]
- M.A. Musick, J.W. Traphagan, H.G. Koeing, and D.B. Larson. “Spirituality in physical health and aging.” J. Adult Dev. 7 (2000): 73–86. [Google Scholar] [CrossRef]
- O. Torre, D. Olivieri, P.J. Barnes, and S.A. Kharitonov. “Feasibility and interpretation of feno measurements in asthma patients in general practice.” Respir. Med. 102 (2008): 1417–1424. [Google Scholar]
- B. Kaplan. “Social health and the forgiving heart: The type b story.” J. Behav. Med. 15 (1992): 3–14. [Google Scholar] [CrossRef]
- M. Timio, G. Lippi, S. Venanzi, S. Gentili, G. Quintaliani, C. Verdura, C. Monarca, P. Saronio, and F. Timio. “Blood pressure trend and cardiovascular events in nuns in a secluded order: A 30-year follow-up study.” Blood Press. 6 (1997): 81–87. [Google Scholar] [CrossRef]
- S. Kreikebaum, E. Guarneri, G. Talavera, H. Madanat, and T. Smith. “Evaluation of a holistic cardiac rehabilitation in the reduction of biopsychosocial risk factors among patients with coronary heart disease.” Psychol. Health Med. 16 (2011): 276–290. [Google Scholar] [CrossRef]
- J. Levin, and H. Vanderpool. “Is religion therapeutically significant for hypertension? ” Soc. Sci. Med. 29 (1989): 69–78. [Google Scholar] [CrossRef]
- J. Holt-Lunstad, P.R. Steffen, J. Sandberg, and B. Jensen. “Understanding the connection between spiritual well-being and physical health: An examination of ambulatory blood pressure, inflammation, blood lipids and fasting glucose.” J. Behav. Med. 34 (2011): 477–488. [Google Scholar] [CrossRef]
- R.L. Polzer. “African americans and diabetes: Spiritual role of the health care provider in self-management.” Res. Nurs. Health 30 (2007): 164–174. [Google Scholar] [CrossRef]
- A. Zaldívar, and J. Smolowitz. “Perceptions of the importance placed on religion and folk medicine by non-mexican-american hispanic adults with diabetes.” Diabetes Educ. 20 (1994): 303–306. [Google Scholar] [CrossRef]
- V. Green. “Understanding different religions when caring for diabetes patients.” Br. J. Nurs. 13 (2004): 658–662. [Google Scholar]
- B.D. Horne, H.T. May, J.L. Anderson, A.G. Kfoury, B.M. Bailey, B.S. McClure, D.G. Renlund, D.L. Lappé, J.F. Carlquist, P.W. Fisher, R.R. Pearson, T.L. Bair, T.D. Adams, and J.B. Muhlestein. “Usefulness of routine periodic fasting to lower risk of coronary artery disease in patients undergoing coronary angiography.” Am. J. Cardiol. 102 (2008): 814–819. [Google Scholar]
- M. Cesur, D. Corapcioglu, A. Gursoy, S. Gonen, M. Ozduman, R. Emral, A.R. Uysal, V. Tonyukuk, A.E. Yilmaz, F. Bayram, and N. Kamel. “A comparison of glycemic effects of glimepiride, repaglinide, and insulin glargine in type 2 diabetes mellitus during ramadan fasting.” Diabetes Res. Clin. Pract. 75 (2007): 141–147. [Google Scholar] [CrossRef]
- P. Paredi, W. Biernacki, G. Invernizzi, S.A. Kharitonov, and P.J. Barnes. “Exhaled carbon monoxide levels elevated in diabetes and correlated with glucose concentration in blood: A new test for monitoring the disease? ” Chest 116 (1999): 1007–1011. [Google Scholar] [CrossRef]
- A. Ivlev, N. Panteleev, I. Kniazev, M. Logachev, and I. Miller. “Daily changes in the carbon isotope composition of co2 in expired air of persons with various metabolic disorders.” Biofizika 39 (1994): 393–399. [Google Scholar]
- N. Nelson, V. Lagesson, A.R. Nostratabadi, J. Ludvigsson, and C. Tagesson. “Exhaled isoprene and acetone in newborn infants and in children with diabetes mellitus.” Pediatr. Res. 44 (1998): 363–367. [Google Scholar] [CrossRef]
- V. Kulikov, L. Ruiatkina, M. Sorokin, E. Shabanova, M. Baldin, V. Gruznov, A. Efimenko, D. Petrovskiĭ, E. Shnaĭder, and M. Moshkin. “Concentration of light hydrocarbons in exhaled air depending on the risk factors of metabolic disorder.” Fiziol. Cheloveka. 37 (2011): 70–75. [Google Scholar]
- K. Karns, and A.E. Herr. “Human tear protein analysis enabled by an alkaline microfluidic homogeneous immunoassay.” Anal. Chem. 83 (2011): 8115–8122. [Google Scholar] [CrossRef]
- T. Ritz, A. Kullowatz, M.D. Goldman, H.-J. Smith, F. Kanniess, B. Dahme, and H. Magnussen. “Airway response to emotional stimuli in asthma: The role of the cholinergic pathway.” J. Appl. Physiol. 108 (2010): 1542–1549. [Google Scholar] [CrossRef]
- A. Kullowatz, D. Rosenfield, B. Dahme, H. Magnussen, F. Kanniess, and T. Ritz. “Stress effects on lung function in asthma are mediated by changes in airway inflammation.” Psychosom. Med. 70 (2008): 468–475. [Google Scholar] [CrossRef]
- G.E. Carpagnano, A. Spanevello, B. Beghe, R. Prato, and M.P.F. Barbaro. “Microsatellite alterations suggestive of organ-specific asthma and atopy in exhaled breath condensate.” Allergy 65 (2010): 404–405. [Google Scholar] [CrossRef]
- G.E. Carpagnano, M.P. Foschino Barbaro, O. Resta, E. Gramiccioni, N.V. Valerio, P. Bracciale, and G. Valerio. “Exhaled markers in the monitoring of airways inflammation and its response to steroid's treatment in mild persistent asthma.” Eur. J. Pharmacol. 519 (2005): 175–181. [Google Scholar] [CrossRef]
- E. Chen, R.C. Strunk, L.B. Bacharier, M. Chan, and G.E. Miller. “Socioeconomic status associated with exhaled nitric oxide responses to acute stress in children with asthma.” Brain. Behav. Immun. 24 (2010): 444–450. [Google Scholar] [CrossRef]
- P. Paredi, S.A. Kharitonov, and P.J. Barnes. “Correlation of exhaled breath temperature with bronchial blood flow in asthma.” Resp. Res. 6 (2005): 6–15. [Google Scholar] [CrossRef] [Green Version]
- P. Paredi, and P.J. Barnes. “The airway vasculature: Recent advances and clinical implications.” Thorax 64 (2009): 444–450. [Google Scholar] [CrossRef]
- J.H. Wlodarczyk, P.G. Gibson, and M. Caeser. “Impact of inhaled corticosteroids on cortisol suppression in adults with asthma: A quantitative review.” Ann. Allergy Asthma. Immunol. 100 (2008): 23–30. [Google Scholar] [CrossRef]
- T. Ritz, E.S. Ayala, A.F. Trueba, C.D. Vance, and R.J. Auchus. “Acute stress-induced increases in exhaled nitric oxide in asthma and their association with endogenous cortisol.” Am. J. Respir. Crit. Care. Med. 183 (2011): 26–30. [Google Scholar] [CrossRef]
- C.D. Lynn, J. Paris, C.A. Frye, and L.M. Schell. “Salivary alpha-amylase and cortisol among pentecostals on a worship and nonworship day.” Am. J. Hum. Biol. 22 (2010): 819–822. [Google Scholar] [CrossRef]
- C. Krägeloh, P. Chai, D. Shepherd, and R. Billington. “How religious coping is used relative to other coping strategies depends on the individual’s level of religiosity and spirituality.” J. Relig. Health 2 (2010): 1–15. [Google Scholar]
- F. Stenius, J. Swartz, F. Lindblad, G. Pershagen, A. Scheynius, J. Alm, and T. Theorell. “Low salivary cortisol levels in infants of families with an anthroposophic lifestyle.” Psychoneuroendocrinology 35 (2010): 1431–1437. [Google Scholar] [CrossRef]
- L.F. Reinke, C.G. Slatore, J. Uman, E.M. Udris, B.R. Moss, R.A. Engelberg, and D.H. Au. “Patient–clinician communication about end-of-life care topics: Is anyone talking to patients with chronic obstructive pulmonary disease? ” J. Palliat. Med. 14 (2011): 923–928. [Google Scholar] [CrossRef]
- D.B. Larson, H.G. Koenig, B.H. Kaplan, R.S. Greenberg, E. Logue, and H.A. Tyroler. “The impact of religion on men's blood pressure.” J. Relig. Health 28 (1989): 265–278. [Google Scholar] [CrossRef]
- F. Hakim, E. Hellou, A. Goldbart, R. Katz, Y. Bentur, and L. Bentur. “The acute effects of water-pipe smoking on the cardiorespiratory system.” Chest 139 (2011): 775–781. [Google Scholar] [CrossRef]
- P. Paredi, M. Goldman, A. Alamen, P. Ausin, O.S. Usmani, N.B. Pride, and P.J. Barnes. “Comparison of inspiratory and expiratory resistance and reactance in patients with asthma and chronic obstructive pulmonary disease.” Thorax 65 (2010): 263–267. [Google Scholar]
- S.A. Kharitonov, R.A. Robbins, D. Yates, V. Keatings, and P.J. Barnes. “Acute and chronic effects of cigarette smoking on exhaled nitric oxide.” Am. J. Respir. Crit. Care. Med. 152 (1995): 609–612. [Google Scholar]
- W. Maziak, S. Loukides, S. Culpitt, P. Sullivan, S.A. Kharitonov, and P.J. Barnes. “Exhaled nitric oxide in chronic obstructive pulmonary disease.” Am. J. Respir. Crit. Care. Med. 157 (1998): 998–1002. [Google Scholar]
- P. Montuschi, S.A. Kharitonov, and P.J. Barnes. “Exhaled carbon monoxide and nitric oxide in copd.” Chest 120 (2001): 496–501. [Google Scholar] [CrossRef]
- P. Montuschi, J.V. Collins, G. Ciabattoni, N. Lazzeri, M. Corradi, S.A. Kharitonov, and P.J. Barnes. “Exhaled 8-isoprostane as an in vivo biomarker of lung oxidative stress in patients with copd and healthy smokers.” Am. J. Respir. Crit. Care. Med. 162 (2000): 1175–1177. [Google Scholar]
- J. Tartaro, L.J. Luecken, and H.E. Gunn. “Exploring heart and soul: Effects of religiosity/spirituality and gender on blood pressure and cortisol stress responses.” J. Health Psychol. 10 (2005): 753–766. [Google Scholar] [CrossRef]
- E. Dedert, J. Studts, I. Weissbecker, P. Salmon, P. Banis, and S. Sephton. “Religiosity may help preserve the cortisol rhythm in women with stress-related illness.” Int. J. Psychiatr. Med. 34 (2004): 61–77. [Google Scholar] [CrossRef]
- S. Mélik-Parsadaniantz, and W. Rostène. “Chemokines and neuromodulation.” J. Neuroimmunol. 198 (2008): 62–68. [Google Scholar] [CrossRef]
- D. Lindqvist, S. Janelidze, S. Erhardt, L. Träskman-Bendz, G. Engström, and L. Brundin. “Csf biomarkers in suicide attempters—a principal component analysis.” Acta. Psychiatr. Scand. 124 (2011): 52–61. [Google Scholar] [CrossRef]
- A. Bajetto, R. Bonavia, S. Barbero, T. Florio, and G. Schettini. “Chemokines and their receptors in the central nervous system.” Front. Neuroendocrinol. 22 (2001): 147–184. [Google Scholar] [CrossRef]
- N.M. Simon, K. McNamara, C.W. Chow, R.S. Maser, G.I. Papakostas, M.H. Pollack, A.A. Nierenberg, M. Fava, and K.K. Wong. “A detailed examination of cytokine abnormalities in major depressive disorder.” Eur. Neuropsychopharmacol. 18 (2008): 230–233. [Google Scholar]
- S.M. Lehto, L. Niskanen, K.-H. Herzig, T. Tolmunen, A. Huotari, H. Viinamäki, H. Koivumaa-Honkanen, K. Honkalampi, H. Ruotsalainen, and J. Hintikka. “Serum chemokine levels in major depressive disorder.” Psychoneuroendocrinology 35 (2010): 226–232. [Google Scholar] [CrossRef]
- Z. Zietkowski, M. Tomasiak-Lozowska, R. Skiepko, E. Zietkowska, and A. Bodzenta-Lukaszyk. “Eotaxin-1 in exhaled breath condensate of stable and unstable asthma patients.” Respir. Res. 11 (2010): 110. [Google Scholar] [CrossRef]
- C.M.H.H.T. Robroeks, G.T. Rijkers, Q. Jöbsis, H.J.E. Hendriks, J.G.M.C. Damoiseaux, L.J.I. Zimmermann, O.P. Van Schayck, and E. Dompeling. “Increased cytokines, chemokines and soluble adhesion molecules in exhaled breath condensate of asthmatic children.” Clin. Exp. Allergy. 40 (2010): 77–84. [Google Scholar]
- E. Bucchioni, S.A. Kharitonov, L. Allegra, and P.J. Barnes. “High levels of interleukin-6 in the exhaled breath condensate of patients with copd.” Respir. Med. 97 (2003): 1299–1302. [Google Scholar] [CrossRef]
- G.E. Carpagnano, P.J. Barnes, D.M. Geddes, M.E. Hodson, and S.A. Kharitonov. “Increased leukotriene b4 and interleukin-6 in exhaled breath condensate in cystic fibrosis.” Am. J. Respir. Crit. Care. Med. 167 (2003): 1109–1112. [Google Scholar] [CrossRef]
- D. Lindqvist, A. Isaksson, B. Lil Träskman, and L. Brundin. “Salivary cortisol and suicidal behavior—A follow-up study.” Psychoneuroendocrinology 33 (2008): 1061–1068. [Google Scholar] [CrossRef]
- A.L. Ai, C. Peterson, S.F. Bolling, and W. Rodgers. “Depression, faith-based coping, and short-term postoperative global functioning in adult and older patients undergoing cardiac surger.” J. Psychosom. Res. 60 (2006): 21–28. [Google Scholar] [CrossRef]
- K.N. Fountoulakis, M. Siamouli, S. Magiria, and G. Kaprinis. “Late-life depression, religiosity, cerebrovascular disease, cognitive impairment and attitudes towards death in the elderly: Interpreting the data.” Med. Hypotheses 70 (2008): 493–496. [Google Scholar] [CrossRef]
- J. Gartner, D.B. Larson, and G.D. Allen. “Religious commitment and mental-health—a review of the empirical literature.” J. Psychol. Theol. 19 (1991): 6–25. [Google Scholar]
- R. Page, C. Ellison, and J. Lee. “Does religiosity affect health risk behaviors in pregnant and postpartum women? ” Matern. Child. Health. J. 13 (2009): 621–632. [Google Scholar] [CrossRef]
- A. Latifynia, M. Vojgani, M.J. Gharagozlou, and R. Sharifian. “Neutrophil function (innate immunity) during ramadan.” J. Ayub. Med. Coll. Abbottabad. 21 (209): 111–115. [Google Scholar]
- M. Statheropoulos, A. Agapiou, and A. Georgiadou. “Analysis of expired air of fasting male monks at mount athos.” J. Chromatogr. B. Analyt. Technol. Biomed. Life. Sci. 832 (2006): 274–279. [Google Scholar] [CrossRef]
- A.W. Jones. “Breath-acetone concentrations in fasting healthy men: Response of infra-red breath-alcohol analysers.” J. Anal. Toxicol. 11 (1987): 67–69. [Google Scholar]
- E.W. Widera, K.E. Rosenfeld, E.K. Fromme, D.P. Sulmasy, and R.M. Arnold. “Approaching patients and family members who hope for a miracle.” J. Pain. Manage. 42 (2011): 119–125. [Google Scholar] [CrossRef]
- F. Mc Kenna, and F. Killoury. “An investigation into the use of complementary and alternative medicine in an urban general practice.” Ir. Med. J. 103 (2010): 205–208. [Google Scholar]
- F.G. Miller, L. Colloca, and T.J. Kaptchuk. “The placebo effect: Illness and interpersonal healing.” Perspect. Biol. Med. 2 (2009): 518–539. [Google Scholar]
- C.A. Okoro, G. Zhao, C. Li, and L.S. Balluz. “Use of complementary and alternative medicine among USA adults with functional limitations: For treatment or general use? ” Complement. Ther. Med. 19 (2011): 208–215. [Google Scholar] [CrossRef]
- S. Karlsen, and J.Y. Nazroo. “Religious and ethnic differences in health: Evidence from the health surveys for england 1999 and 2004.” Ethn. Health 15 (2010): 549–568. [Google Scholar] [CrossRef]
- S. Sonnappa, C.M. Bastardo, P. Stafler, A. Bush, P. Aurora, and J. Stocks. “Ethnic differences in fraction of exhaled nitric oxide and lung function in healthy young children.” Chest 140 (2011): 1325–1331. [Google Scholar] [CrossRef]
- K. Matsunaga, T. Hirano, T. Kawayama, T. Tsuburai, H. Nagase, H. Aizawa, K. Akiyama, K. Ohta, and M. Ichinose. “Reference ranges for exhaled nitric oxide fraction in healthy japanese adult population.” Allergol. Int. 59 (2010): 363–367. [Google Scholar] [CrossRef]
- J. van Amsterdam, E. Bischoff, M. Hady, A. Opperhuizen, and P. Steerenberg. “The prevalence of allergic sensitisation in immigrant children in the netherlands.” Int. Arch. Allergy. Immunol. 133 (2004): 248–254. [Google Scholar] [CrossRef]
- M.L. Hatzenbuehler, J.E. Pachankis, and J. Wolff. “Religious climate and health risk behaviors in sexual minority youths: A population-based study.” Am. J. Public. Health 102 (2012): 657–663. [Google Scholar] [CrossRef]
- S.S. Rostosky, F. Danner, and E.D.B. Riggle. “Religiosity and alcohol use in sexual minority and heterosexual youth and young adults.” J. Youth Adolesc. 37 (2008): 552–563. [Google Scholar] [CrossRef]
- C.S. Lewis. Aspects of Faith (Essay collection. Faith, Christianity and the Church). New York, NY, USA: HarperCollins Publishers, 2002, p. 429. [Google Scholar]
- D.D. Turner. “Just another drug? A philosophical assessment of randomised controlled studies on intercessory prayer.” J. Med. Ethics 32 (2006): 487–490. [Google Scholar] [CrossRef]
- R. Sloan, and R. Ramakrishnan. “Science, medicine, and intercessory prayer.” Perspect. Biol. Med. 49 (2006): 504–514. [Google Scholar] [CrossRef]
- K. Masters, G. Spielmans, and J. Goodson. “Are there demonstrable effects of distant intercessory prayer? A meta-analytic review.” Ann. Behav. Med. 32 (2006): 21–26. [Google Scholar] [CrossRef]
- L. Roberts, I. Ahmed, and S. Hall. “Intercessory prayer for the alleviation of ill health.” Cochrane. Database. Syst. Rev. 24 (2007): CD000368. [Google Scholar]
- L.L. Rath. “Scientific ways to study intercessory prayer as an intervention in clinical research.” J. Perinat. Neonatal. Nurs. 23 (2009): 71–77. [Google Scholar]
- L. Roberts, I. Ahmed, S. Hall, and A. Davison. “Intercessory prayer for the alleviation of ill health.” Cochrane. Database Syst. Rev. 15 (2009): CD000368. [Google Scholar]
- K. Jorgensen, A. Hrobjartsson, and P. Gotzsche. “Divine intervention? A cochrane review on intercessory prayer gone beyond science and reason.” J. Negat. Results Biomed. 8 (2009): 7. [Google Scholar] [CrossRef]
- B. Çoruh, H. Ayele, M. Pugh, and T. Mulligan. “Does religious activity improve health outcomes? A critical review of the recent literature.” Explore (New York) 1 (2005): 186–191. [Google Scholar]
- H. Benson, J.A. Dusek, J.B. Sherwood, P. Lam, C.F. Bethea, W. Carpenter, S. Levitsky, P.C. Hill, D.W. Clem, M.K. Jain, D. Drumel, S.L. Kopecky, P.S. Mueller, D. Marek, S. Rollins, and P.L. Hibberd. “Study of the therapeutic effects of intercessory prayer (STEP) in cardiac bypass patients: A multicenter randomized trial of uncertainty and certainty of receiving intercessory prayer.” Am. Heart. J. 151 (2006): 934–942. [Google Scholar] [CrossRef]
- R.C. Byrd. “Positive therapeutic effects of intercessory prayer in a coronary care unit population.” South Med. J. 81 (1988): 826–829. [Google Scholar] [CrossRef]
- L. Roberts, I. Ahmed, and S. Hall. “Intercessory prayer for the alleviation of ill health.” Cochrane Database Syst. Rev. 2 (2000): CD000368. [Google Scholar]
- L. Roberts, I. Ahmed, S. Hall, and A. Davison. “Intercessory prayer for the alleviation of ill health.” Cochrane Database Syst. Rev. 15 (2009): CD000368. [Google Scholar]
- S.A. Schwartz, and L. Dossey. “Nonlocality, intention, and observer effects in healing studies: Laying a foundation for the future.” Explore J. Sci. Healing 6 (2010): 295–307. [Google Scholar] [CrossRef]
- L. VandeCreek. “Defining and advocating for spiritual care in the hospital.” J. Pastoral. Care Counsel. 64 (2010): 1–10. [Google Scholar]
- P. Lissoni, G. Messina, D. Parolini, A. Balestra, F. Brivo, L. Fumagalli, L. Vigore, and F. Rovelli. “A spiritual approach in the treatment of cancer: Relation between faith score and response to chemotherapy in advanced non-small cell lung cancer patients.” In Vivo 22 (2008): 577–581. [Google Scholar]
- G.E. Carpagnano, D. Lacedonia, G.P. Palladino, A. Koutelou, D. Martinelli, S. Orlando, and M.P. Foschino-Barbaro. “Could exhaled ferritin and sod be used as markers for lung cancer and prognosis prediction purposes? ” Eur. J. Clin. Invest. 42 (2012): 478–486. [Google Scholar] [CrossRef]
- G. Carpagnano, G. Palladino, D. Lacedonia, A. Koutelou, S. Orlando, and M. Foschino-Barbaro. “Neutrophilic airways inflammation in lung cancer: The role of exhaled LTB-4 and IL-8.” BMC Cancer 7 (2011): 226. [Google Scholar]
- G.E. Carpagnano, G.P. Palladino, C. Gramiccioni, M.P. Foschino Barbaro, and D. Martinelli. “Exhaled ERCC-1 and ERCC-2 microsatellite alterations in NSCL patients.” Lung Cancer 68 (2010): 305–307. [Google Scholar] [CrossRef]
- G.E. Carpagnano, A. Spanevello, G.P. Palladino, C. Gramiccioni, C. Ruggieri, F. Carpagnano, and M.P. Foschino Barbaro. “Cigarette smoke and increased COX-2 and survivin levels in exhaled breath condensate of lung cancer patients: How hot is the link? ” Lung Cancer 67 (2010): 108–113. [Google Scholar] [CrossRef]
- G. Carpagnano, A. Spanevello, C. Curci, F. Salerno, G. Palladino, O. Resta, G. Di Gioia, F. Carpagnano, and M. Foschino Barbaro. “IL-2, TNF-alpha, and leptin: Local versus systemic concentrations in nsclc patients.” Oncol. Res. 16 (2007): 375–381. [Google Scholar]
- T.R. Mikuls, J.R. O’Dell, R. Ertl, D.A. Bergman, and S.I. Rennard. “Examining the exhaled levels of hydrogen peroxide in rheumatoid arthritis: A pilot study.” Ann. Rheum. Dis. 65 (2006): 1252–1253. [Google Scholar] [CrossRef]
- A.L. Ai, T.N. Tice, B. Huang, W. Rodgers, and S.F. Bolling. “Types of prayer, optimism, and well-being of middle-aged and older patients undergoing open-heart surgery.” Ment. Health Relig. Cult. 11 (2008): 131–150. [Google Scholar] [CrossRef]
- D.C. Törnberg, M. Angdin, G. Settergen, J. Liska, J.O. Lundberg, and E. Weitzberg. “Exhaled nitric oxide before and after cardiac surgery with cardiopulmonary bypass—response to acetylcholine and nitroglycerin.” Br. J. Anaesth. 94 (2005): 174–180. [Google Scholar] [CrossRef]
- L. Beuscher, and V.T. Grando. “Using spirituality to cope with early-stage Alzheimer's disease.” West. J. Nurs. Res. 31 (2009): 583–598. [Google Scholar] [CrossRef]
- S.G. Post, and P.G. Whitehouse. “Spirituality, religion, and Alzheimer's disease.” J. Health Care Chaplain. 8 (1999): 45–57. [Google Scholar]
- L. Snyder. “Satisfactions and challenges in spiritual faith and practice for persons with dementia.” Dementia 2 (2003): 299–313. [Google Scholar] [CrossRef]
- J. Frank. “Interview with Jerome Frank, Ph.D., M.D. Exploring concepts of influence, persuasion, and healing.” J. Psychosoc. Nurs. Ment. Health Serv. 22 (1984): 32–34, 36–37. [Google Scholar]
- F. Benedetti, and M. Amanzio. “The placebo response: How words and rituals change the patient's brain.” Pat. Educ. Couns. 84 (2011): 413–419. [Google Scholar] [CrossRef]
- R. de la Fuentefernández, and A.J. Stoessl. “The biochemical bases for reward.” Eval. Health Prof. 25 (2002): 387–398. [Google Scholar] [CrossRef]
- K. Linde, C.M. Witt, A. Streng, W. Weidenhammer, S. Wagenpfeil, B. Brinkhaus, S.N. Willich, and D. Melchart. “The impact of patient expectations on outcomes in four randomized controlled trials of acupuncture in patients with chronic pain.” Pain 128 (2007): 264–271. [Google Scholar] [CrossRef]
- F. Benedetti, A. Pollo, L. Lopiano, M. Lanotte, S. Vighetti, and R. I. “Conscious expectation and unconscious conditioning in analgesic, motor, and hormonal placebo/nocebo responses.” J. Neurosci. 23 (2003): 4315–4323. [Google Scholar]
- R. Mercado, C. Constantoyannis, T. Mandat, A. Kumar, M. Schulzer, A.J. Stoessl, and C.R. Honey. “Expectation and the placebo effect in parkinson's disease patients with subthalamic nucleus deep brain stimulation.” Movem. Dis. 21 (2006): 1457–1461. [Google Scholar] [CrossRef]
- L. Vase, J.L. Riley, and D.D. Price. “A comparison of placebo effects in clinical analgesic trials versus studies of placebo analgesia.” Pain 99 (2002): 443–452. [Google Scholar] [CrossRef]
- A. Branthwaite, and P. Cooper. “Analgesic effects of branding in treatment of headaches.” Br. Med. J. 282 (1981): 1576–1578. [Google Scholar] [CrossRef]
- D.E. Moerman, and W.B. Jonas. “Deconstructing the placebo effect and finding the meaning response.” Ann. Intern. Med. 136 (2002): 471–476. [Google Scholar]
- A.J.M. de Craen, J.G.P. Tijssen, J. de Gans, and J. Kleijnen. “Placebo effect in the acute treatment of migraine: Subcutaneous placebos are better than oral placebos.” J. Neurol. 247 (2000): 183–188. [Google Scholar] [CrossRef]
- R.L. Waber, B. Shiv, Z. Carmon, and D. Ariely. “Commercial features of placebo and therapeutic efficacy.” JAMA 299 (2008): 1016–1017. [Google Scholar] [CrossRef]
- N. Kohls, S. Sauer, M. Offenbächer, and J. Giordano. “Spirituality: An overlooked predictor of placebo effects? ” Phil. Trans. R. Soc. B Biol. Sci. 366 (2011): 1838–1848. [Google Scholar] [CrossRef]
- M.-J.H.E. Gijsberts, M.A. Echteld, J.T. van der Steen, M.T. Muller, R.H.J. Otten, M.W. Ribbe, and L. Deliens. “Spirituality at the end of life: Conceptualization of measurable aspects—a systematic review.” J. Palliat. Med. 14 (2011): 852–863. [Google Scholar] [CrossRef]
- S.D. Kilpatrick, A.J. Weaver, M.E. McCullough, C. Puchalski, D.B. Larson, J.C. Hays, C.J. Farran, and K.J. Flannelly. “A review of spiritual and religious measures in nursing research journals: 1995–1999.” J. Relig. Health 44 (2005): 55–66. [Google Scholar] [CrossRef]
- V. Kassab, and D. MacDonald. “Examination of the psychometric properties of the spiritual fitness assessment.” J. Relig. Health 50 (2011): 975–985. [Google Scholar] [CrossRef]
- D.A. MacDonald. “Spirituality: Description, measurement, and relation to the five factor model of personality.” J. Pers. 68 (2000): 153–197. [Google Scholar]
- D. Elkins. “Toward phenomenological spirituality: Definition, description, and measurement.” J. Hum. Psychol. 28 (1988): 5–18. [Google Scholar] [CrossRef]
- C. Delgado. “Meeting clients' spiritual needs.” Nurs. Clin. North Am. 42 (2007): 279–293. [Google Scholar] [CrossRef]
- M. Wilfred, and R. Linda. “Dilemmas of spiritual assessment: Considerations for nursing practice.” J. Adv. Nurs. 38 (2002): 479–488. [Google Scholar] [CrossRef]
- D. MacDonald, and H. Friedman. “Measures of spiritual and transpersonal constructs for use in yoga research.” Int. J. Yoga 2 (2009): 2–12. [Google Scholar] [CrossRef]
- H. Friedman. “The self-expansiveness level form: A conceptualization and measurement of a transpersonal construct.” J. Transpers. Psychol. 15 (1983): 37–50. [Google Scholar]
- J.R. Mann, and W. Larimore. “Impact of religious attendance on life expectancy.” J. Am. Board Fam. Med. 19 (2006): 429–430. [Google Scholar] [CrossRef]
- M. Inzlicht, and A.M. Tullett. “Reflecting on God.” Psychol. Sci. 21 (2010): 1184–1190. [Google Scholar] [CrossRef]
- V.J. Stenger. “God: The failed hypothesis: How science shows that god does not exist.” Prometheus Books, 2007, 35–54. [Google Scholar]
© 2012 by the authors; licensee MDPI, Basel, Switzerland. This article is an open-access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/3.0/).
Share and Cite
MDPI and ACS Style
Kharitonov, S.A. Religious and Spiritual Biomarkers in Both Health and Disease. Religions 2012, 3, 467-497. https://doi.org/10.3390/rel3020467
AMA Style
Kharitonov SA. Religious and Spiritual Biomarkers in Both Health and Disease. Religions. 2012; 3(2):467-497. https://doi.org/10.3390/rel3020467
Chicago/Turabian StyleKharitonov, Sergei A. 2012. "Religious and Spiritual Biomarkers in Both Health and Disease" Religions 3, no. 2: 467-497. https://doi.org/10.3390/rel3020467