
The NERSH International Collaboration on Values, Spirituality and Religion in Medicine: Development of Questionnaire, Description of Data Pool, and Overview of Pool Publications

 , , ,
, , ,  ,
, 
 add
Show full author list
add
Show full author list
Abstract
:
1. Introduction
2. Methods and Materials
2.1. Development of the RSMPP
- Physician perspectives on religion/spirituality (R/S) and health containing 50 items. The items were written by Curlin and colleagues after thorough review of relevant literature and data gathered from qualitative pilot interviews. Items were subsequently revised for clarity and cogency through multiple expert panel reviews [2].
- Religious Characteristics consisting of 21 questions based on existing religiosity measures: 3A Religious affiliation, 3B Intrinsic religiosity, 3C Frequency of religious service attendance, 3D Beliefs, 3E Spirituality vs. Religiosity, 3F Religious Coping [1], and
- Demographics containing 18 items.
2.2. International Translations and Validations of the RSMPP
2.3. Development of the NERSH Instrument
2.3.1. Expert Round Table Meetings with NGT
2.3.2. Internal Reliability
2.3.3. Face Validation
2.4. Characteristics of NERSH Questionnaire
2.5. Identification of Eligible Datasets for Inclusion in NERSH International Data Pool on Values in Medicine
2.5.1. Personal Contacts
2.5.2. Citation Search
2.5.3. Systematic Search
2.6. Description of Pool of Data Harvested with Versions of the RSMPP and the NERSH Instruments
3. Results
3.1. Chronological Overview of Existing Studies Using the Original RSMPP
3.2. Chronological Overview of Articles Using Translations of the RSMPP
3.3. Glimpse of Trends in the NERSH Data Pool of Physician Values
4. Summary
- In the eyes of HPs, R/S is an important element of the life of patients. R/S may help patients cope with their disease and may positively influence their health. However, HPs also report various barriers for engaging their patients on R/S themes. These are mainly centred on lack of training, lack of time and fear of offending patients or imposing own beliefs on them.
- The idea that health care is a value neutral sphere, mainly driven by a scientifically neutral and “objective” approach, is challenged by research. HP values (both R/S and atheistic) are subjective, personal, and deep. They have a profound influence on communication with patients, in particular when it comes to existential and R/S issues, controversial issues in Health Care, and understanding of one’s own professional identity.
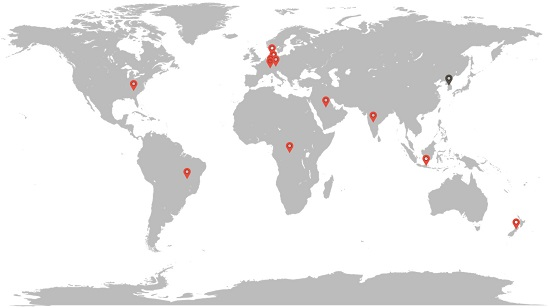
- Just as HPs’ personal values impact health care (communication, ethics and professional identity), so are the same values highly impacted by culture. This is clear in the enormous differences in R/S when comparing for instance Denmark with Brazil and the impact these differences have on HPs evaluation of patient R/S. This insight might help HPs to adopt a humble attitude while reflecting on the context of their own values, which may lead to improved attention to the particular values and needs of patients, be they atheist or R/S. Such reflecting may improve critical ethical reflection, increase respect for both religious and agnostic worldviews and improve communication with patients in their search for resources for dealing with their illness.
5. Invitation for Researchers to Join and Availability of Questionnaire
6. Limitations
Supplementary Materials
Acknowledgments
Author Contributions
Conflicts of Interest
Abbreviations
| ASP | Aspects of Spirituality |
| DUREL | Duke Religiosity Index |
| FRIAS | Freiburg Institute for Advanced Studies |
| HPs | Health Professionals |
| IRG | Interdisciplinary Research Group |
| NERSH | Network for Research in Spirituality and Health |
| NGT | Nominal Group Technique |
| R/S | R/s understood as a unit of both, although they conceptually and phenomenologically have different traits |
| RSMPP | Questionnaire Religion and Spirituality in Medicine: Physicians’ Perspectives |
| SpREUK | Spiritual and Religious Attitudes in Dealing with Illness |
| TCAM | Traditional Complementary and Alternative Medicine |
Appendix A
- Item complex #20: Positive experience of r/s in the clinical practice (i.e., helps patients to cope with and endure illness and suffering; causes guilt, anxiety, or other negative emotions that lead to increased patient suffering; gives patients a positive, hopeful state of mind; leads patients to refuse, delay, or stop medically indicated therapy; helps to prevent severe consequences of disease, etc.). Cronbach´s alphas ranged from 0.60 to 0.79 between the four samples. This indicates that the putative scale is of questionable to acceptable internal validity. Therefore, we added additional items as used in the Freiburg sample that had the best internal reliability with a 6-item version of the scale (i.e., adding: patients receive emotional or practical support from their religious community; religiosity/spirituality in general influences the health of patients/relatives positively; is strengthened or deepened through the experience of illness).
- Item complex # 21: Inquiry about religious/spiritual issues in specific situations (i.e., When a patient presents with a minor illness or injury; faces a frightening diagnosis or crisis; faces the end of life; suffers from anxiety or depression; comes for a history and physical; faces an ethical quandary). This topic was addressed in four datasets; Cronbach´s alpha ranged from 0.83 to 0.90 which indicates a good to very good internal reliability of this putative scale.
- Item complex #22: Frequency of specific responses when religious/spiritual issues come up in discussions with patients (i.e., listen carefully and empathetically; try to change the subject in a tactful way; encourage patients in their own religious/spiritual beliefs and practices; respectfully share my own religious ideas and experiences; pray with the patient). This topic was addressed in five datasets, but was found to be of questionable to acceptable internal validity (Cronbach´s alpha ranged from 0.61 to 0.74).
- Item complex #28: Controversial Issues in Medicine (i.e., Physician assisted suicide; Sedation to unconsciousness in dying patients; Withdrawal of artificial life support; Abortion for congenital abnormalities; Abortion for failed contraception; Prescription of birth control to teenagers between the age of 14 and 16 if their parents do not approve). This topic was addressed in four datasets, and was found to be of questionable to acceptable internal validity (Cronbach´s alpha ranged from 0.62 to 0.78).
Appendix B—Citation Search in Web of Science

{kind=link}
{kind=link}
| ID | Term(s) | Results |
|---|---|---|
| 1 | Religious characteristics of US physicians–A national survey [1] | 1 |
| 2 | Citing articles | 85 |
| ID | Term(s) | Results |
|---|---|---|
| 1 | The association of physicians’ religious characteristics with their attitudes and self-reported behaviors regarding religion and spirituality in the clinical encounter [2] | 1 |
| 2 | Citing articles | 59 |
| ID | Term(s) | Results |
|---|---|---|
| 1 | Do religious physicians disproportionately care for the underserved? [3] | 1 |
| 2 | Citing articles | 15 |
| ID | Term(s) | Results |
|---|---|---|
| 1 | Religion, conscience, and controversial clinical practices AND Curlin [4] | 1 |
| 2 | Citing articles | 131 |
| ID | Term(s) | Results |
|---|---|---|
| 1 | Religion, spirituality, and medicine: Psychiatrists’ and other physicians’ differing observations, interpretations, and clinical approaches [5] | 1 |
| 2 | Citing articles | 46 |
| ID | Term(s) | Results |
|---|---|---|
| 1 | The relationship between psychiatry and religion among US physicians [6] | 1 |
| 2 | Citing articles | 32 |
| ID | Term(s) | Results |
|---|---|---|
| 1 | Physicians’ observations and interpretations of the influence of religion and spirituality on health [7] | 1 |
| 2 | Citing articles | 43 |
| ID | Term(s) | Results |
|---|---|---|
| 1 | To die, to sleep: US physicians’ religious and other objections to physician-assisted suicide, terminal sedation, and withdrawal of life support [8] | 1 |
| 2 | Citing articles | 34 |
Appendix C—Literature Search
| Database | Interface | Date of Search |
|---|---|---|
| Google Scholar | Internet | 12-04-16 |
| Web of Science | Internet | 13-04-16 |
| Embase | Ovid | 12-04-16 |
| Medline | Ovid | 13-04-16 |
| PsychInfo | Ovid | 13-04-16 |
| ID | Term(s) | Results |
|---|---|---|
| 1 | “Religion and Spirituality in Medicine: Physicians’ Perspectives” | 8 |
| ID | Term(s) | Results |
|---|---|---|
| 1 | TOPIC:(((questionn * OR survey * OR cross-section * OR national sample *) AND (religious OR religio * OR spiritual * OR religiosity) near/3 (professional * OR physician * OR psychiatris * OR doctor * OR staff * OR ((nurs * or medic *) near/3 (professor *))))) | 308 |
| 2 | Refined by: LANGUAGES: ( ENGLISH OR DANISH OR SPANISH OR FRENCH OR GERMAN ) Timespan: All years. Search language = Auto | 305 |
| ID | Term(s) | Results |
|---|---|---|
| 1 | (((questionn * or survey * or cross-section * or national sample *) and (religious or religio * or spiritual * or religiosity)) adj3 (professional * or physician * or psychiatris * or doctor * or staff * or ((nurs * or medic *) adj3 professor *))).mp. [mp = title, abstract, heading word, drug trade name, original title, device manufacturer, drug manufacturer, device trade name, keyword] | 1431 |
| 2 | limit 1 to (danish or english or french or german or italian or norwegian or spanish or swedish) | 1400 |
| ID | Term(s) | Results |
|---|---|---|
| 1 | ((questionn * or survey * or cross-section * or national sample *) and (religious or religio * or spiritual * or religiosity)) adj3 (professional * or physician * or psychiatris * or doctor * or staff * or ((nurs * or medic *) adj3 professor *))).mp. [mp = title, abstract, original title, name of substance word, subject heading word, keyword heading word, protocol supplementary concept word, rare disease supplementary concept word, unique identifier] | 1021 |
| 2 | limit 1 to (danish or english or french or german or italian or norwegian or spanish or swedish) | 998 |
| ID | Term(s) | Results |
|---|---|---|
| 1 | (((questionn * or survey * or cross-section * or national sample *) and (religious or religio * or spiritual * or religiosity)) adj3 (professional * or physician * or psychiatris * or doctor * or staff * or ((nurs * or medic *) adj3 professor *))).mp. [mp = title, abstract, heading word, table of contents, key concepts, original title, tests & measures] | 829 |
| 2 | limit 1 to (danish or english or french or german or italian or norwegian or spanish or swedish) | 804 |
Appendix D
| Country | Location | Sampling Year(s) | Occupation | n | Specialties | n | % | Religious Affiliation (%) | n | % | ntotal | RR* | Gender | n | % | Mean Age (CI95%) | ||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| USA | Nationwide | 2002 | All physicians | Anesthesiology | 39 | 3.4 | None | 80 | 7.0 | 1144 | 63% | Male | 842 | 73.6 | 49.0 (48.5-49.5) | |||
| General Pract | 17 | 1.5 | Atheist | 19 | 1.7 | Female | 300 | 26.2 | ||||||||||
| Neuro | 18 | 1.6 | Agnostic | 18 | 1.6 | n/a | 2 | 0.2 | ||||||||||
| OB/GYN | 80 | 7.0 | Buddhist | 13 | 1.1 | |||||||||||||
| Optho | 18 | 1.6 | Hindu | 54 | 4.7 | |||||||||||||
| Pathology | 20 | 1.7 | Jewish | 181 | 15.8 | |||||||||||||
| Peds - General | 87 | 7.6 | Mormon | 17 | 1.5 | |||||||||||||
| Physiatry | 16 | 1.4 | Muslim | 33 | 2.9 | |||||||||||||
| Psych | 100 | 8.7 | Protestants | 428 | 37.4 | |||||||||||||
| Ped Subspec. | 60 | 5.2 | Catholic | 244 | 21.3 | |||||||||||||
| Gen Med | 129 | 11.3 | Orthodox | 22 | 1.9 | |||||||||||||
| FP | 158 | 13.8 | Other | 18 | 1.6 | |||||||||||||
| EM | 15 | 1.3 | Unanswered | 17 | 1.5 | |||||||||||||
| Dermathology | 11 | 1.0 | ||||||||||||||||
| Med Subspec. | 231 | 20.2 | ||||||||||||||||
| Radiology | 25 | 2.2 | ||||||||||||||||
| Unanswered | 2 | 0.2 | ||||||||||||||||
| General Surgery | 23 | 2.0 | ||||||||||||||||
| Surg Subsp. | 77 | 6.7 | ||||||||||||||||
| Other | 18 | 1.6 | ||||||||||||||||
| Germany | Freiburg. University clinic | 2008–2009 | Mixed psychiatric staff | Physicians | 18 | 21.1 | Protestants | 30 | 34.9 | 87 | 44% | Male | 38 | 43.2 | 41.5 | |||
| Psychologists and psychotherapists | 11 | 12.9 | Catholics | 28 | 32.5 | Female | 49 | 56.8 | ||||||||||
| Nursing staff | 39 | 44.7 | No affiliation | 23 | 26.5 | |||||||||||||
| Other psychiatric staff | 18 | 21.2 | ||||||||||||||||
| Saudi Arabia | Riyadh, King Abdul-Aziz Medical City | 2009–2010 | All physicians | Family medicine | 73 | 32.4 | Muslim | 225 | 100 | 225 | 64% | Male | 128 | 56.9 | 36.6 (35.4–37.6) | |||
| Internal med. and subspec. | 38 | 16.9 | Female | 97 | 43.1 | |||||||||||||
| OB/GYN | 31 | 13.8 | ||||||||||||||||
| Pediatrics | 21 | 9.3 | ||||||||||||||||
| Surgical subspec. | 30 | 13.3 | ||||||||||||||||
| Emergency med. | 9 | 4 | ||||||||||||||||
| Oncology and palliative care | 19 | 8.4 | ||||||||||||||||
| ICU and anaesthesia | 4 | 1.8 | ||||||||||||||||
| Indonesia | Dr. Soetomo General Hospital, Surabaya, East Java | 2010 | All physicians | Anatomy | 1 | None | 2 | 1,6 | 122 | 99% | Male | 55 | 45.1 | 29.2 (28.4–29.9) | ||||
| Microbiology | 1 | 0.8 | Other | 7 | 5.7 | Female | 65 | 53.3 | ||||||||||
| Pathology | 3 | 2.5 | Hindu | 2 | 1.6 | n/a | 2 | 1.6 | ||||||||||
| Forensic | 1 | 0.88 | Christian | 7 | 5.7 | |||||||||||||
| Ophtalmology | 10 | 8.2 | Muslim | 104 | 85.2 | |||||||||||||
| ENT | 1 | 0.8 | ||||||||||||||||
| Pediatric | 2 | 1.6 | ||||||||||||||||
| General medicine | 23 | 18.9 | ||||||||||||||||
| Surgery | 14 | 11.5 | ||||||||||||||||
| OBG | 7 | 5.7 | ||||||||||||||||
| Psychiatry/neurology | 17 | 13.9 | ||||||||||||||||
| Radiology | 8 | 6.6 | ||||||||||||||||
| Anesthesiology | 8 | 6.6 | ||||||||||||||||
| Psychotherapist | 1 | 0.8 | ||||||||||||||||
| Unanswered | 14 | 11.5 | ||||||||||||||||
| Brazil | São Paulo | 2010 | Teachers | 30 | Nursing | Teachers | 148 | 99% | Male | 15 | 10.1 | Teachers 41.4 (38.6–44.2) Students 28.4 (27.0–29.8) | ||||||
| Students | 118 | Catholics | 25 | 16.7 | Female | 133 | 89.9 | |||||||||||
| Spiritists | 20 | 13.3 | ||||||||||||||||
| Evangelical | 20 | 13.3 | ||||||||||||||||
| Students | ||||||||||||||||||
| Catholics, 30.8% | 46 | 30.8 | ||||||||||||||||
| Evangelicals, 11.1% | 16 | 11.1 | ||||||||||||||||
| None or others | 22 | 14.8 | ||||||||||||||||
| Germany, Freiburg | Nationwide. Departments of psychiatry and psychotherapy in university clinics + faith based clinics. | 2010–2011 | Psychiatrist | 121 | All psychiatry | No affiliation | 88 | 21.8 | 404 | 24% | Male | 145 | 35.9 | 39.9 (38.8–41) | ||||
| Psychotherapist | 16 | Catholic | 115 | 28.5 | Female | 252 | 62.4 | |||||||||||
| Other therapeut | 25 | Protestant | 128 | 31.7 | n/a | 7 | 1.7 | |||||||||||
| Psychologist | 32 | Free Church | 10 | 2.5 | ||||||||||||||
| Nurse or assistant | 160 | Orthodox | 1 | 0.2 | ||||||||||||||
| Other | 32 | Muslim | 5 | 1,2 | ||||||||||||||
| Buddhist | 7 | 1,7 | ||||||||||||||||
| Agnostic/Atheist | 34 | 8,4 | ||||||||||||||||
| Other | 9 | 2,2 | ||||||||||||||||
| India | Selected hospitals | 2010–2012 | TCAM | 192 | Anatomy | 8 | 2 | None or others | 11 | 3.7 | 394 | 50% | Male | 148 | 37.6 | 31.6 (30.5–32.8) | ||
| -Physicians | 79 | Physiology | 15 | 3.8 | Hindu | 257 | 65.2 | Female | 230 | 58.4 | ||||||||
| -Nurses | 0 | Biochemisty | 5 | 1.3 | Christian | 54 | 13.7 | n/a | 16 | 4 | ||||||||
| -Residents | 48 | Pharmacology | 23 | 5.8 | Muslim | 58 | 14.7 | |||||||||||
| -Interns | 0 | Microbiology | 4 | 1 | ||||||||||||||
| -Students | 36 | Pathology | 7 | 1.8 | ||||||||||||||
| -All-Therapists | 0 | Forensic | 6 | 1.5 | ||||||||||||||
| -Non-clinical physicians | 13 | Opthalmoloy | 1 | 0.3 | ||||||||||||||
| -Unknown | 16 | ENT | 11 | 2.8 | ||||||||||||||
| PSM | 12 | 3.0 | ||||||||||||||||
| Allopaths | 201 | Gen medicine | 49 | 12.4 | ||||||||||||||
| -Physicians | 54 | Surgery | 4 | 1.0 | ||||||||||||||
| -Nurses | 29 | OBG | 16 | 4.0 | ||||||||||||||
| -Residents | 44 | Psychiatry+neuro | 57 | 14.5 | ||||||||||||||
| -Interns | 0 | Pediatrics | 26 | 6.6 | ||||||||||||||
| -Students | 33 | Radiology | 0 | 0 | ||||||||||||||
| -All-Therapists | 0 | Anesthesiology | 18 | 4.6 | ||||||||||||||
| -Non-clinical physicians | 35 | Psychotherapist | 16 | 4.1 | ||||||||||||||
| -Unknown | 6 | Physical medicine and rehab +spec. | 18 | 4.6 | ||||||||||||||
| Denmark | Nationwide, selection criteria? | 2011–2012 | All physicians | General practitioner | 261 | 28.6 | Missing 8 (0.9) | 8 | 0.9 | 911 | 61% | Male | 524 | 57.5 | 48.9 (48.0–49.8) | |||
| Mixed hospital physicians | 650 | 71.4 | Do not wish to answer | 4 | 0.4 | Female | 387 | 42.5 | ||||||||||
| No affiliation | 183 | 20.1 | ||||||||||||||||
| Other | 20 | 2.2 | ||||||||||||||||
| Buddhist | 2 | 0.2 | ||||||||||||||||
| Hindu | 1 | 0.1 | ||||||||||||||||
| Muslim | 6 | 0.7 | ||||||||||||||||
| The Orthodox Church | 11 | 1.2 | ||||||||||||||||
| Roman Catholic Church | 29 | 3.2 | ||||||||||||||||
| Danish National Church | 647 | 71.0 | ||||||||||||||||
| Other | 4 | 0.4 | ||||||||||||||||
| New Zealand | Psychiatry | 2012 | Psychiatrists | 91 | All psychiatry | No affiliation | 53 | 45.7 | 116 | 18% | Male | 73 | 62.9 | Agegroups (n) | ||||
| Non specialists | 25 | Christian | 42 | 36.2 | Female | 39 | 33.6 | 20-29 | 4 | |||||||||
| Buddhist | 3 | 2.6 | Trans-gender | 1 | 0.9 | 40-49 | 32 | |||||||||||
| Hindu | 4 | 3.4 | n/a | 3 | 2.6 | 30-39 | 19 | |||||||||||
| Other | 4 | 3.4 | 50-59 | 43 | ||||||||||||||
| Object to answer | 3 | 2.6 | 60-69 | 14 | ||||||||||||||
| Unanswered | 7 | 6.0 | 70+ | 3 | ||||||||||||||
| Brazil | Marilia - Marília University Hospital | 2012 | Physicians | 81 | Internal Med. | 146 | 75.3 | None | 9 | 7.4 | 194 | 95% | Male | 145 | 74.7 | 37.7 (36.1–39.3) | ||
| Residents | 113 | Pediatricians | 12 | 6.2 | Other | 0 | 0 | Female | 49 | 25.3 | ||||||||
| Surgeons/surgical physicians | 26 | 13.4 | Hindu | 0 | 0 | |||||||||||||
| OB/GYN | 10 | 5.2 | Christian | 166 | 94.9 | |||||||||||||
| Muslim | 0 | 0 | ||||||||||||||||
| Congo R.D. | University Hospital of Kinshasa | 2012 | Mixed hospital physicians | No data | No affiliation | 12 | 11 | 112 | 82% | Male | 84 | 75 | 35 (33.5–36.8) | |||||
| Roman Catholics | 43 | 38 | Female | 28 | 25 | |||||||||||||
| Orthodox Christians | 1 | 1 | ||||||||||||||||
| Protestant Christians | 22 | 10 | ||||||||||||||||
| Others | 34 | 30 | ||||||||||||||||
| Germany, Munich | Nationwide Perinatal | 2013–2014 | Physicians | 482 | Perinatal hospital professionals | Does not apply | 115 | 7 | 1,637 | 82% | Male | 192 | 11.7 | 39.1 (38.6–39.6) | ||||
| Midwife | 257 | No response | 15 | 0.9 | Female | 1312 | 80.1 | |||||||||||
| Nurses | 529 | None | 409 | 25.0 | n/a | 133 | 8.1 | |||||||||||
| Psychologist | 18 | Roman | 639 | 39.0 | ||||||||||||||
| Others | 351 | Orthodox | 8 | 0.5 | ||||||||||||||
| Protestant (without Free-Church) | 409 | 25.0 | ||||||||||||||||
| Other Christian denominations | 21 | 1.3 | ||||||||||||||||
| Islam | 13 | 0.8 | ||||||||||||||||
| Jewish | 1 | 0.1 | ||||||||||||||||
| Buddhist | 6 | 0.4 | ||||||||||||||||
| Other non-Christian denominations | 1 | 0.1 | ||||||||||||||||
| Germany, Munich | Transplantation medicine | 2014 | Physician | 48 | Internal med. | 3 | 1.6 | 187 | 64% | Male | 53 | 28.3 | 34.6 (32.9–36.3) | |||||
| Nurse | 127 | Intensive care | 88 | 47.1 | Female | 134 | 71.7 | |||||||||||
| Other | 12 | Surgery | 38 | 20.3 | ||||||||||||||
| Neurology | 7 | 3.7 | ||||||||||||||||
| Anesthesiology | 19 | 10.2 | ||||||||||||||||
| Other | 32 | 17.1 | ||||||||||||||||
| Austria, Salzburg | Brothers of Mercy hospital | 2014 | Physician | 28 | Internal medicine | 54 | 23 | Not religious | 29 | 13 | 231 | 52% | Male | 54 | 23 | 39.3 (37.7–41.0) | ||
| Nursing care | 114 | Surgery | 37 | 16 | Catholic | 143 | 62 | Female | 133 | 58 | ||||||||
| Other | 29 | Anesthetics | 12 | 5 | Protestant | 8 | 3 | n/a | 44 | 19 | ||||||||
| Unanswered | 60 | Others | 62 | 27 | Others | 6 | 8 | |||||||||||
| Unanswered | 66 | 29 | Unanswered, | 45 | 19 | |||||||||||||
| Switzerland | Region of Bale and Aarau | 2015–2016 | All physicians, practicing outside the hospital | General practitioner | 104 | 100 | Christian | 80 | 76.2 | 104 | 75% | Male | 73 | 70.5 | 53.8 (51.9–55.7) | |||
| Jewish | 2 | 1.9 | Female | 31 | 29.5 | |||||||||||||
| Islam | 2 | 1.9 | ||||||||||||||||
| No affiliation | 19 | 18.1 | ||||||||||||||||
| Unanswered | 2 | 1.9 | ||||||||||||||||
| Germany, Munich | Turkish physicians | 2016 | All physicians | Psychiatry + psychotherapists | 9 | 7.4 | Muslim | 79 | 65.3 | 121 | 22% | Male | 42 | 34.8 | 33.2 (31.7–34.7) | |||
| Anesthetics | 1 | 0.8 | No affiliation | 21 | 17.4 | Female | 79 | 65.3 | ||||||||||
| Orthopedics | 4 | 3.3 | Exited a religious community | 1 | 0.8 | |||||||||||||
| Intensive care | 3 | 2.5 | Roman catholic | 1 | 0.8 | |||||||||||||
| OB/GYN | 5 | 4.1 | Other | 1 | 0.8 | |||||||||||||
| Internal medicine | 16 | 13.2 | Unanswered | 18 | 14.9 | |||||||||||||
| Surgery | 17 | 14 | ||||||||||||||||
| Neurology | 10 | 8.3 | ||||||||||||||||
| Pediatric | 9 | 7.4 | ||||||||||||||||
| Other 28 | 28 | 23.1 | ||||||||||||||||
| Unanswered | 19 | 15.7 | ||||||||||||||||
References
- Farr A. Curlin, John D. Lantos, Chad J. Roach, Sarah A. Sellergren, and Marshall H. Chin. “Religious Characteristics of U.S. Physicians: A National Survey.” Journal of General Internal Medicine 20 (2005): 629–34. [Google Scholar] [CrossRef] [PubMed]
- Farr A. Curlin, Marshall H. Chin, Sarah A. Sellergren, Chad J. Roach, and John D. Lantos. “The Association of Physicians’ Religious Characteristics with Their Attitudes and Self-Reported Behaviors Regarding Religion and Spirituality in the Clinical Encounter.” Medical Care 44 (2006): 446–53. [Google Scholar] [CrossRef] [PubMed]
- Farr A. Curlin, Lydia S. Dugdale, John D. Lantos, and Marshall H. Chin. “Do religious physicians disproportionately care for the underserved? ” The Annals of Family Medicine 5 (2007): 353–60. [Google Scholar] [CrossRef] [PubMed]
- Farr A. Curlin, Ryan E. Lawrence, Marshall H. Chin, and John D. Lantos. “Religion, Conscience, and Controversial Clinical Practices.” New England Journal of Medicine 356 (2007): 593–600. [Google Scholar] [CrossRef] [PubMed]
- Farr A. Curlin, Ryan E. Lawrence, Shaun Odell, Marshall H. Chin, John D. Lantos, Harold G. Koenig, and Keith G. Meador. “Religion, Spirituality, and Medicine: Psychiatrists’ and Other Physicians’ Differing Observations, Interpretations, and Clinical Approaches.” American Journal of Psychiatry 164 (2007): 1825–31. [Google Scholar] [CrossRef] [PubMed]
- Farr A. Curlin, Shaun V. Odell, Ryan E. Lawrence, Marshall H. Chin, John D. Lantos, Keith G. Meador, and Harold G. Koenig. “The Relationship between Psychiatry and Religion among U.S. Physicians.” Psychiatric Services 58 (2007): 1193–208. [Google Scholar] [CrossRef] [PubMed]
- Farr A. Curlin, Sarah A. Sellergren, John D. Lantos, and Marshall H. Chin. “Physicians’ Observations and Interpretations of the Influence of Religion and Spirituality on Health.” Archives of Internal Medicine 167 (2007): 649–54. [Google Scholar] [CrossRef] [PubMed]
- Farr A. Curlin, Chinyere Nwodim, Jennifer L. Vance, Marshall H. Chin, and John D. Lantos. “To Die, to Sleep: Us Physicians’ Religious and Other Objections to Physician-Assisted Suicide, Terminal Sedation, and Withdrawal of Life Support.” American Journal of Hospice and Palliative Medicine 25 (2008): 112–20. [Google Scholar] [CrossRef] [PubMed]
- Robert M. Stern, Kenneth A. Rasinski, and Farr A. Curlin. “Jewish Physicians’ Beliefs and Practices Regarding Religion/Spirituality in the Clinical Encounter.” Journal of Religion and Health 50 (2011): 806–17. [Google Scholar] [CrossRef] [PubMed]
- Aaron B. Franzen. “Physicians in the USA: Attendance, Beliefs and Patient Interactions.” Journal of Religion and Health 54 (2015): 1886–900. [Google Scholar] [CrossRef] [PubMed]
- Klaus Baumann, Eunmi Lee, and Anne Zahn. “‘Religion in Psychiatry and Psychotherapy?’ A Pilot Study: The Meaning of Religiosity/Spirituality from Staff’s Perspective in Psychiatry and Psychotherapy.” Religions 2 (2011): 525–35. [Google Scholar]
- Claudia de Souza Tomasso, Ideraldo Luiz Beltrame, and Giancarlo Lucchetti. “Knowledge and Attitudes of Nursing Professors and Students Concerning the Interface between Spirituality, Religiosity and Health.” Revista Latino-Americana De Enfermagem 19 (2011): 1205–13. [Google Scholar] [CrossRef]
- Nada A. Al-Yousefi. “Observations of Muslim Physicians Regarding the Influence of Religion on Health and Their Clinical Approach.” Journal of Religion and Health 51 (2012): 269–80. [Google Scholar] [CrossRef] [PubMed]
- Eunmi Lee, and Klaus Baumann. “German Psychiatrists’ Observation and Interpretation of Religiosity/Spirituality.” Evidence-Based Complementary and Alternative Medicine 2013 (2013): article 280168. [Google Scholar] [CrossRef] [PubMed]
- P. Ramakrishnan, A. Dias, A. Rane, A. Shukla, S. Lakshmi, B. K. Ansari, R. S. Ramaswamy, A. R. Reddy, A. Tribulato, A. K. Agarwal, and et al. “Perspectives of Indian Traditional and Allopathic Professionals on Religion/Spirituality and Its Role in Medicine: Basis for Developing an Integrative Medicine Program.” Journal of Religion and Health 53 (2013): 1161–75. [Google Scholar] [CrossRef] [PubMed]
- P. Ramakrishnan, A. Rane, A. Dias, J. Bhat, A. Shukla, S. Lakshmi, B. K. Ansari, R. S. Ramaswamy, R. A. Reddy, A. Tribulato, and et al. “Indian Health Care Professionals’ Attitude Towards Spiritual Healing and Its Role in Alleviating Stigma of Psychiatric Services.” Journal of Religion and Health 53 (2014): 1800–14. [Google Scholar] [CrossRef] [PubMed]
- P. Ramakrishnan, A. Karimah, K. Kuntaman, A. Shukla, B. K. Ansari, P. H. Rao, M. Ahmed, A. Tribulato, A. K. Agarwal, H. G. Koenig, and et al. “Religious/Spiritual Characteristics of Indian and Indonesian Physicians and Their Acceptance of Spirituality in Health Care: A Cross-Cultural Comparison.” Journal of Religion and Health 54 (2014): 649–63. [Google Scholar] [CrossRef] [PubMed]
- Eunmi Lee, Anne Zahn, and Klaus Baumann. “Religiosity/Spirituality and Mental Health: Psychiatric Staff’s Attitudes and Behaviors.” Open Journal of Social Sciences 2 (2014): 7. [Google Scholar] [CrossRef]
- Eunmi Lee, Anne Zahn, and Klaus Baumann. “How Do Psychiatric Staffs Approach Religiosity/Spirituality in Clinical Practice? Differing Perceptions among Psychiatric Staff Members and Clinical Chaplains.” Religions 6 (2015): 930–47. [Google Scholar] [CrossRef]
- Giancarlo Lucchetti, Parameshwaran Ramakrishnan, Azimatul Karimah, Gabriela R. Oliveira, Amit Dias, Anil Rane, A. Shukla, S. Lakshmi, B. K. Ansari, R. S. Ramaswamy, and et al. “Spirituality, Religiosity, and Health: A Comparison of Physicians’ Attitudes in Brazil, India, and Indonesia.” International Journal of Behavioral Medicine 23 (2016): 63–70. [Google Scholar] [CrossRef] [PubMed]
- Wyatt Butcher. “Spirituality, Religion and Psychiatric Practice in New Zealand: A Survey of Psychiatrists in New Zealand.” 2013. Available online: https://ourarchive.otago.ac.nz/handle/10523/242/browse?value=Butcher%2C+Wyatt+Hillary&type=author (accessed on 5 April 2016).
- Eunmi Lee. Religiosität Bzw. Spiritualität in Psychiatrie Und Psychotherapie. Ihre Bedeutung Für Psychiatrisches Wirken Aus Der Sicht Des Psychiatrischen Personals Anhand Einer Bundesweiten Personalbefragung. Studien Zur Theologie Und Praxis Der Caritas Und Sozialen Pastoral, 28. Würzburg: Echter, 2014. [Google Scholar]
- Can Kuseyri. “Spiritualität Türkischstämmiger Ärzte in Deutschland.” MD Thesis (German Dr.med.), Ludwig Maximilian University, 2016. Available online: http://www.nersh.org (accessed on 6 August 2016). [Google Scholar]
- Tryphon Mukwayakala-Kisamba. “Spiritualität Bei Ärzten Im Kongo.” MD Thesis (German Dr.med.), Ludwig Maximilian University, 2016. Available online: http://www.nersh.org (accessed on 6 August 2016). [Google Scholar]
- Esther Schouten. “Spiritualität in Der Perinatologie.” MD Thesis (German Dr.med.), Ludwig Maximilian University, 2016. Available online: http://www.nersh.org (accessed on 6 August 2016). [Google Scholar]
- Christian Balslev Van Randwijk. “Faith and Values of Danish Physicians.” Ph.D. Dissertation, University of Southern Denmark, 2016. Available online: http://www.nersh.org (accessed on 6 August 2016). [Google Scholar]
- Micha Eglin. “Religious Beliefs and Patient Observation in Swiss General Practitioners.” MD Thesis (Swiss Dr.Med.), University of Basel, 2016. Available online: http://www.nersh.org (accessed on 6 August 2016). [Google Scholar]
- Miriam Wey. “Religious Beliefs and Medical Practice in Swiss General Practitioners.” MD Thesis (Swiss Dr.Med.), University of Basel, 2016. Available online: http://www.nersh.org (accessed on 6 August 2016). [Google Scholar]
- Daniel E. Hall, Harold G. Koenig, and Keith G. Meador. “Conceptualizing ‘Religion’.” Perspectives in Biology and Medicine 47 (2004): 386–401. [Google Scholar] [CrossRef] [PubMed]
- Peter C. Hill, Kenneth Pargament II, Ralph W. Hood Jr., Michael E. McCullough, James P. Swyers, David B. Larson, and Brian J. Zinnbauer. “Conceptualizing Religion and Spirituality: Points of Commonality, Points of Departure.” Journal for the Theory of Social Behaviour 30 (2000): 51–77. [Google Scholar] [CrossRef]
- Peter La Cour, and Niels Christian Hvidt. “Research on Meaning-Making and Health in Secular Society: Secular, Spiritual and Religious Existential Orientations.” Social Science & Medicine 71 (2010): 1292–99. [Google Scholar] [CrossRef] [PubMed]
- Amanda Porterfield. Healing in the History of Christianity. New York: Oxford University Press, 2005. [Google Scholar]
- “Lancet Series on Faith-Based Health Care.” Available online: http://www.thelancet.com/series/faith-based-health-care (accessed on 6 April 2016).
- Sigmund Freud. Civilizations and Its Discontents. New York: W. W. Norton, 1959. [Google Scholar]
- Klaus Baumann. “The Birth of Human Sciences, Especially Psychology.” In L’uomo Moderno E La Chiesa—Atti Del Congresso (Analecta Gregoriana, 317). Edited by Paul Gilbert. Rome: Gregorian & Biblical Press, 2012, pp. 391–408. [Google Scholar]
- Harold G. Koenig, Dana E. King, and Verna Benner Carson. Handbook of Religion and Health, 2nd ed. Oxford and New York: Oxford University Press, 2012. [Google Scholar]
- Ryan E. Lawrence, and Farr A. Curlin. “Physicians’ Beliefs About Conscience in Medicine: A National Survey.” Academic Medicine 84 (2009): 1276–82. [Google Scholar] [CrossRef] [PubMed]
- Ryan E. Lawrence, and Farr A. Curlin. “Autonomy, Religion and Clinical Decisions: Findings from a National Physician Survey.” Journal of Medical Ethics 35 (2009): 214–18. [Google Scholar] [CrossRef] [PubMed]
- Ryan E. Lawrence, Kenneth A. Rasinski, John D. Yoon, and Farr A. Curlin. “Obstetrician-Gynecologist Physicians’ Beliefs About Emergency Contraception: A National Survey.” Contraception 82 (2010): 324–30. [Google Scholar] [CrossRef] [PubMed]
- Ryan E. Lawrence, Kenneth A. Rasinski, John D. Yoon, and Farr A. Curlin. “Obstetrician-Gynecologists’ Beliefs About Assisted Reproductive Technologies.” Obstetrics & Gynecology 116 (2010): 127–35. [Google Scholar] [CrossRef] [PubMed]
- Debra B. Stulberg, Ryan E. Lawrence, Jason Shattuck, and Farr A. Curlin. “Religious Hospitals and Primary Care Physicians: Conflicts over Policies for Patient Care.” Journal of General Internal Medicine 25 (2010): 725–30. [Google Scholar] [CrossRef] [PubMed]
- John D. Yoon, Kenneth A. Rasinski, and Farr A. Curlin. “Conflict and Emotional Exhaustion in Obstetrician-Gynaecologists: A National Survey.” Journal of Medical Ethics 36 (2010): 731–35. [Google Scholar] [CrossRef] [PubMed]
- John D. Yoon, Kenneth A. Rasinski, and Farr A. Curlin. “Moral Controversy, Directive Counsel, and the Doctor’s Role: Findings from a National Survey of Obstetrician-Gynecologists.” Academic Medicine 85 (2010): 1475–81. [Google Scholar] [CrossRef] [PubMed]
- Ryan E. Lawrence, Kenneth A. Rasinski, John D. Yoon, and Farr A. Curlin. “Adolescents, Contraception and Confidentiality: A National Survey of Obstetrician-Gynecologists.” Contraception 84 (2011): 259–65. [Google Scholar] [CrossRef] [PubMed]
- Ryan E. Lawrence, Kenneth A. Rasinski, John D. Yoon, and Farr A. Curlin. “Obstetrician-Gynecologists’ Beliefs About Safe-Sex and Abstinence Counseling.” International Journal of Gynecology & Obstetrics 114 (2011): 281–85. [Google Scholar] [CrossRef] [PubMed]
- Ryan E. Lawrence, Kenneth A. Rasinski, John D. Yoon, and Farr A. Curlin. “Obstetrician-Gynecologists’ Views on Contraception and Natural Family Planning: A National Survey.” American Journal of Obstetrics and Gynecology 204 (2011): 124.e1–e7. [Google Scholar] [CrossRef] [PubMed]
- R. E. Lawrence, K. A. Rasinski, J. D. Yoon, and F. A. Curlin. “Factors Influencing Physicians’ Advice About Female Sterilization in USA: A National Survey.” Human Reproduction 26 (2011): 106–11. [Google Scholar] [CrossRef] [PubMed]
- Kenneth A. Rasinski, Youssef G. Kalad, John D. Yoon, and Farr A. Curlin. “An Assessment of Us Physicians’ Training in Religion, Spirituality, and Medicine.” Medical Teacher 33 (2011): 944–45. [Google Scholar] [CrossRef] [PubMed]
- Kenneth A. Rasinski, John D. Yoon, Youssef G. Kalad, and Farr A. Curlin. “Obstetrician-Gynaecologists’ Opinions About Conscientious Refusal of a Request for Abortion: Results from a National Vignette Experiment.” Journal of Medical Ethics 37 (2011): 711–14. [Google Scholar] [CrossRef] [PubMed]
- Debra B. Stulberg, Annie M. Dude, Irma Dahlquist, and Farr A. Curlin. “Abortion Provision among Practicing Obstetrician-Gynecologists.” Obstetrics & Gynecology 118 (2011): 609–14. [Google Scholar] [CrossRef] [PubMed]
- Ryan E. Lawrence, Kenneth A. Rasinski, John D. Yoon, Harold G. Koenig, Keith G. Meador, and Farr A. Curlin. “Physicians’ Beliefs About Faith-Based Treatments for Alcoholism.” Psychiatric Services 63 (2012): 597–604. [Google Scholar] [CrossRef] [PubMed]
- R. E. Lawrence, K. A. Rasinski, J. D. Yoon, K. G. Meador, H. G. Koenig, and F. A. Curlin. “Primary Care Physicians’ and Psychiatrists’ Approaches to Treating Mild Depression.” Acta Psychiatrica Scandinavica 126 (2012): 385–92. [Google Scholar] [CrossRef] [PubMed]
- Kenneth A. Rasinski, Ryan E. Lawrence, John D. Yoon, and Farr A. Curlin. “A Sense of Calling and Primary Care Physicians’ Satisfaction in Treating Smoking, Alcoholism, and Obesity.” Archives of Internal Medicine 172 (2012): 1423–24. [Google Scholar] [CrossRef] [PubMed]
- Debra B. Stulberg, Annie M. Dude, Irma Dahlquist, and Farr A. Curlin. “Obstetrician-Gynecologists, Religious Institutions, and Conflicts Regarding Patient-Care Policies.” American Journal of Obstetrics & Gynecology 207 (2012): 73e1–e5. [Google Scholar] [CrossRef] [PubMed]
- Ryan E. Lawrence, Kenneth A. Rasinski, John D. Yoon, and Farr A. Curlin. “Religion and Anxiety Treatments in Primary Care Patients.” Anxiety Stress Coping 26 (2013): 526–38. [Google Scholar] [CrossRef] [PubMed]
- Ryan E. Lawrence, Kenneth A. Rasinski, John D. Yoon, and Farr A. Curlin. “Religion and Beliefs About Treating Medically Unexplained Symptoms: A Survey of Primary Care Physicians and Psychiatrists.” The International Journal of Psychiatry in Medicine 45 (2013): 31–44. [Google Scholar] [CrossRef] [PubMed]
- Ryan E. Lawrence, Kenneth A. Rasinski, John D. Yoon, and Farr A. Curlin. “Physicians’ Beliefs About the Nature of Addiction: A Survey of Primary Care Physicians and Psychiatrists.” The American Journal on Addictions 22 (2013): 255–60. [Google Scholar] [CrossRef] [PubMed]
- M. S. Putman, and F. A. Curlin. “Authors’ Reply to Dirksen et al.” Journal of Pain and Symptom Management 45 (2013): e2–e3. [Google Scholar] [CrossRef] [PubMed]
- Michael S. Putman, John D. Yoon, Kenneth A. Rasinski, and Farr A. Curlin. “Intentional Sedation to Unconsciousness at the End of Life: Findings from a National Physician Survey.” Journal of Pain and Symptom Management 46 (2013): 326–34. [Google Scholar] [CrossRef] [PubMed]
- Kelly M. Wolenberg, John D. Yoon, Kenneth A. Rasinski, and Farr A. Curlin. “Religion and United States Physicians’ Opinions and Self-Predicted Practices Concerning Artificial Nutrition and Hydration.” Journal of Religion and Health 52 (2013): 1051–65. [Google Scholar] [CrossRef] [PubMed]
- Ryan E. Lawrence, Kenneth A. Rasinski, John D. Yoon, and Farr A. Curlin. “Physician Race and Treatment Preferences for Depression, Anxiety, and Medically Unexplained Symptoms.” Ethnicity & Health 20 (2015): 354–64. [Google Scholar] [CrossRef] [PubMed]
- Ryan E. Lawrence, Kenneth A. Rasinski, John D. Yoon, and Farr A. Curlin. “Primary Care Physicians’ and Psychiatrists’ Willingness to Refer to Religious Mental Health Providers.” International Journal of Social Psychiatry 60 (2014): 627–36. [Google Scholar] [CrossRef] [PubMed]
- Michael S. Putman, John D. Yoon, Kenneth A. Rasinski, and Farr A. Curlin. “Directive Counsel and Morally Controversial Medical Decision-Making: Findings from Two National Surveys of Primary Care Physicians.” Journal of General Internal Medicine 29 (2014): 335–40. [Google Scholar] [CrossRef] [PubMed]
- Ryan E. Lawrence, Kenneth A. Rasinski, John D. Yoon, and Farr A. Curlin. “Psychiatrists’ and Primary Care Physicians’ Beliefs About Overtreatment of Depression and Anxiety.” The Journal of Nervous and Mental Disease 203 (2015): 120–25. [Google Scholar] [CrossRef] [PubMed]
- Krishna C. Ravella, Farr A. Curlin, and John D. Yoon. “Medical School Ranking and Medical Student Vocational Identity.” Teaching and Learning in Medicine 27 (2015): 123–29. [Google Scholar] [CrossRef] [PubMed]
- John D. Yoon, Jiwon H. Shin, Andy L. Nian, and Farr A. Curlin. “Religion, Sense of Calling, and the Practice of Medicine: Findings from a National Survey of Primary Care Physicians and Psychiatrists.” Southern Medical Journal 108 (2015): 189–95. [Google Scholar] [CrossRef] [PubMed]
- Klaus Baumann, Arndt Büssing, and Niels Chrsitian Hvidt. “Geisteswissenschaftliches Kolloquium Klaus Baumann (Freiburg)/Arndt Büssing (Witten/Herdecke)/Niels Hvidt (Odense): Empirische Forschung Über Religiöse Und Spirituelle Aspekte Bei Patientinnen Und Ärztinnen.” Freiburg Institute for Advanced Studies. Available online: https://www.frias.uni-freiburg.de/en/events/humanities-and-social-sciences-colloquium/geisteswissenschaftliches-kolloquium-klaus-baumann-freiburg-arndt-bussing-witten-herdecke-niels-hvidt-odense-empirische-forschung-uber-religiose-und-spirituelle-aspekte-bei-patientinnen-und-arztinnen (accessed on 6 April 2016).
- Arndt Büssing, Klaus Baumann, Niels Christian Hvidt, Harold G. Koenig, Christina M. Puchalski, and John Swinton. “Spirituality and Health. Editorial.” Evidence-Based Complementary and Alternative Medicine 2014 (2014): article 682817. [Google Scholar] [CrossRef] [PubMed]
- A. Büssing, A. T. Hirdes, K. Baumann, Niels Christian Hvidt, and P. Heusser. “Aspects of Spirituality in Medical Doctors and Their Relation to Specific Views of Illness and Dealing with Their Patients’ Individual Situation.” Evidence-Based Complementary and Alternative Medicine 2013 (2013): article 734392. [Google Scholar] [CrossRef] [PubMed]
- Edgar Voltmer, Arndt Büssing, HaroldG Koenig, and Faten Al Zaben. “Religiosity/Spirituality of German Doctors in Private Practice and Likelihood of Addressing R/S Issues with Patients.” Journal of Religion and Health 53 (2013): 1741–52. [Google Scholar] [CrossRef] [PubMed]
- Andre L. Delbecq, Andrew H. Van de Ven, and David H. Gustafson. Group Techniques for Program Planning: A Guide to Nominal Group and Delphi Processes. Glenview: Scott Foresman, 1975. [Google Scholar]
- Jeremy Jones, and Duncan Hunter. “Consensus Methods for Medical and Health Services Research.” British Medical Journal 311 (1995): 376–80. [Google Scholar] [CrossRef] [PubMed]
- Arndt Büssing, Thomas Ostermann, and Peter F. Matthiessen. “Distinct Expressions of Vital Spirituality ‘the Asp Questionnaire as an Explorative Research Tool‘.” Journal of Religion and Health 46 (2007): 267–86. [Google Scholar] [CrossRef]
- A Büssing, D. R. Recchia, J. Surzykiewicz, and K. Baumann. “Ausdrucksformen Der Spiritualität Bei Schülern Und Jungen Erwachsenen.” Spiritual Care. forthcoming.
- Arndt Bussing, Thomas Ostermann, and Peter Matthiessen. “Role of Religion and Spirituality in Medical Patients: Confirmatory Results with the Spreuk Questionnaire.” Health and Quality of Life Outcomes 3 (2005): 10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Arndt Büssing. “Spirituality as a Resource to Rely on in Chronic Illness: The Spreuk Questionnaire.” Religions 1 (2010): 9–17. [Google Scholar] [CrossRef]

| Indonesia | Brazil | Austria | USA | Denmark | Congo | |
|---|---|---|---|---|---|---|
| Do you believe there is a life after death? (%) Yes | 95.9% | 23.7% | 64.3% | 58.5% | 20.3% | - |
| My whole approach to life is based on my religion (%) Agree or Strongly Agree | 92.6% | 36.1% | - | 41.1% | 10.6% | 51.8% |
| When r/s topics come up in conversation, I pray with the patient (%) Never | 39.5% | 7.2% | 71.4% | 43.7% | 90.5% | 28.6% |
| When r/s topics come up in the conversation, I respectfully share my own religious ideas and experiences (%) Never | 11.4% | 6.2% | 32.1% | 25.2% | 55.2% | 0.0% |
| In general is it appropriate or inappropriate for a physician to discuss religious/spiritual issues when a patient brings them up? (%) Always appropriate + Usually appropriate | 90.2% | 99.0% | 96.0% | 92.2% | 83.3% | 67.0% |
© 2016 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hvidt, N.C.; Kappel Kørup, A.; Curlin, F.A.; Baumann, K.; Frick, E.; Søndergaard, J.; Nielsen, J.B.; DePont Christensen, R.; Lawrence, R.; Lucchetti, G.; et al. The NERSH International Collaboration on Values, Spirituality and Religion in Medicine: Development of Questionnaire, Description of Data Pool, and Overview of Pool Publications. Religions 2016, 7, 107. https://doi.org/10.3390/rel7080107
Hvidt NC, Kappel Kørup A, Curlin FA, Baumann K, Frick E, Søndergaard J, Nielsen JB, DePont Christensen R, Lawrence R, Lucchetti G, et al. The NERSH International Collaboration on Values, Spirituality and Religion in Medicine: Development of Questionnaire, Description of Data Pool, and Overview of Pool Publications. Religions. 2016; 7(8):107. https://doi.org/10.3390/rel7080107
Chicago/Turabian StyleHvidt, Niels Christian, Alex Kappel Kørup, Farr A. Curlin, Klaus Baumann, Eckhard Frick, Jens Søndergaard, Jesper Bo Nielsen, René DePont Christensen, Ryan Lawrence, Giancarlo Lucchetti, and et al. 2016. "The NERSH International Collaboration on Values, Spirituality and Religion in Medicine: Development of Questionnaire, Description of Data Pool, and Overview of Pool Publications" Religions 7, no. 8: 107. https://doi.org/10.3390/rel7080107