A Study of a Health Resources Management Platform Integrating Neural Networks and DSS Telemedicine for Homecare Assistance

 ,
, 
Abstract
:1. Introduction
- Description of the background concerning tools useful for the RMP-DSS design;
- Design and development of homecare telemedicine architecture and the integrated RMP-DSS system;
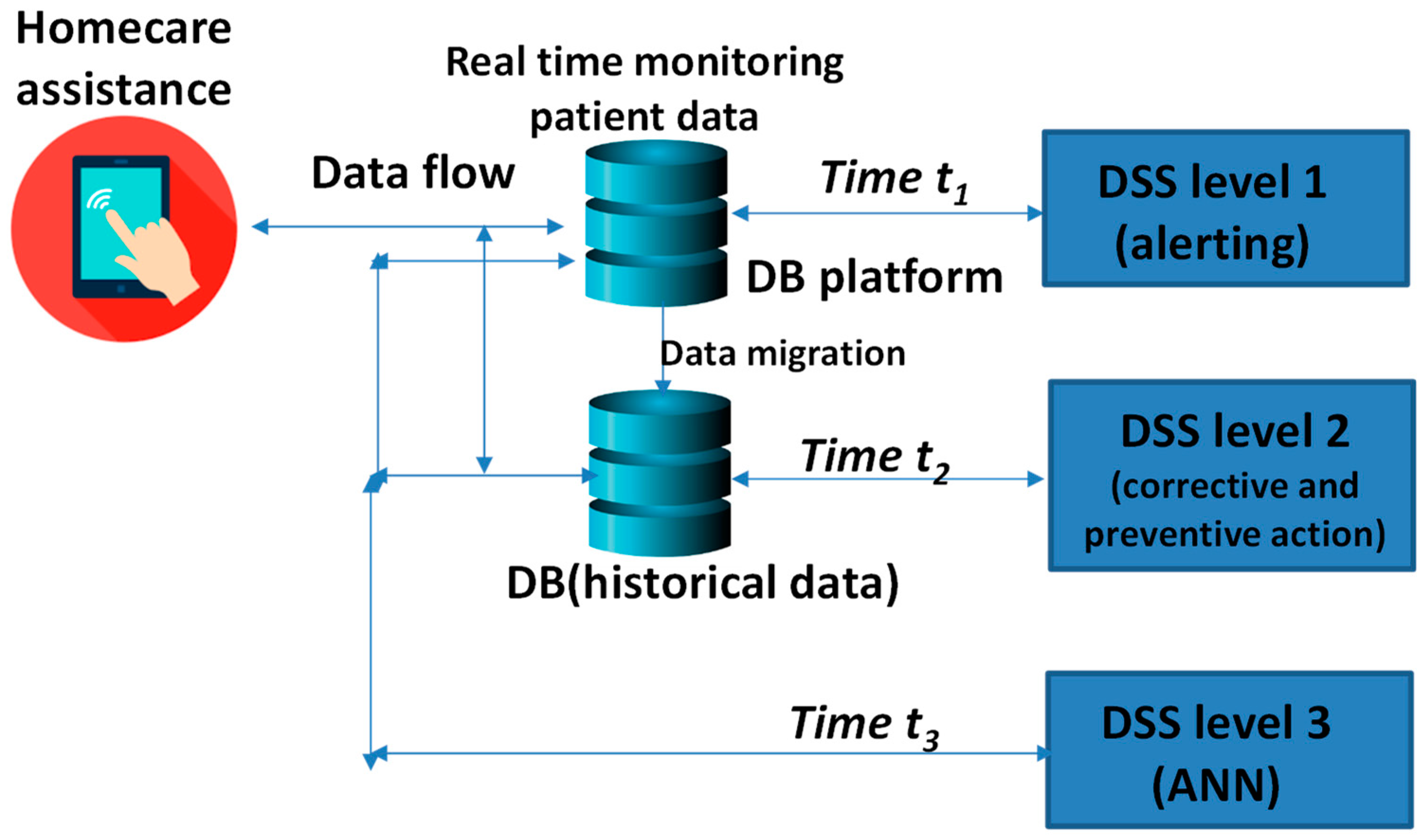
- Design and development of the innovative multi-level DSS system;
- Design, development, and testing of a multilayer perceptron (MLP) artificial neural network (ANN) able to predict patient status about high-pressure and hypertension conditions;
- Definition of correct procedures suited for MLP ANN data processing;
- Discussions and conclusions.
1.1. Background: Tools and Specifications Useful for RMP-DSS Design
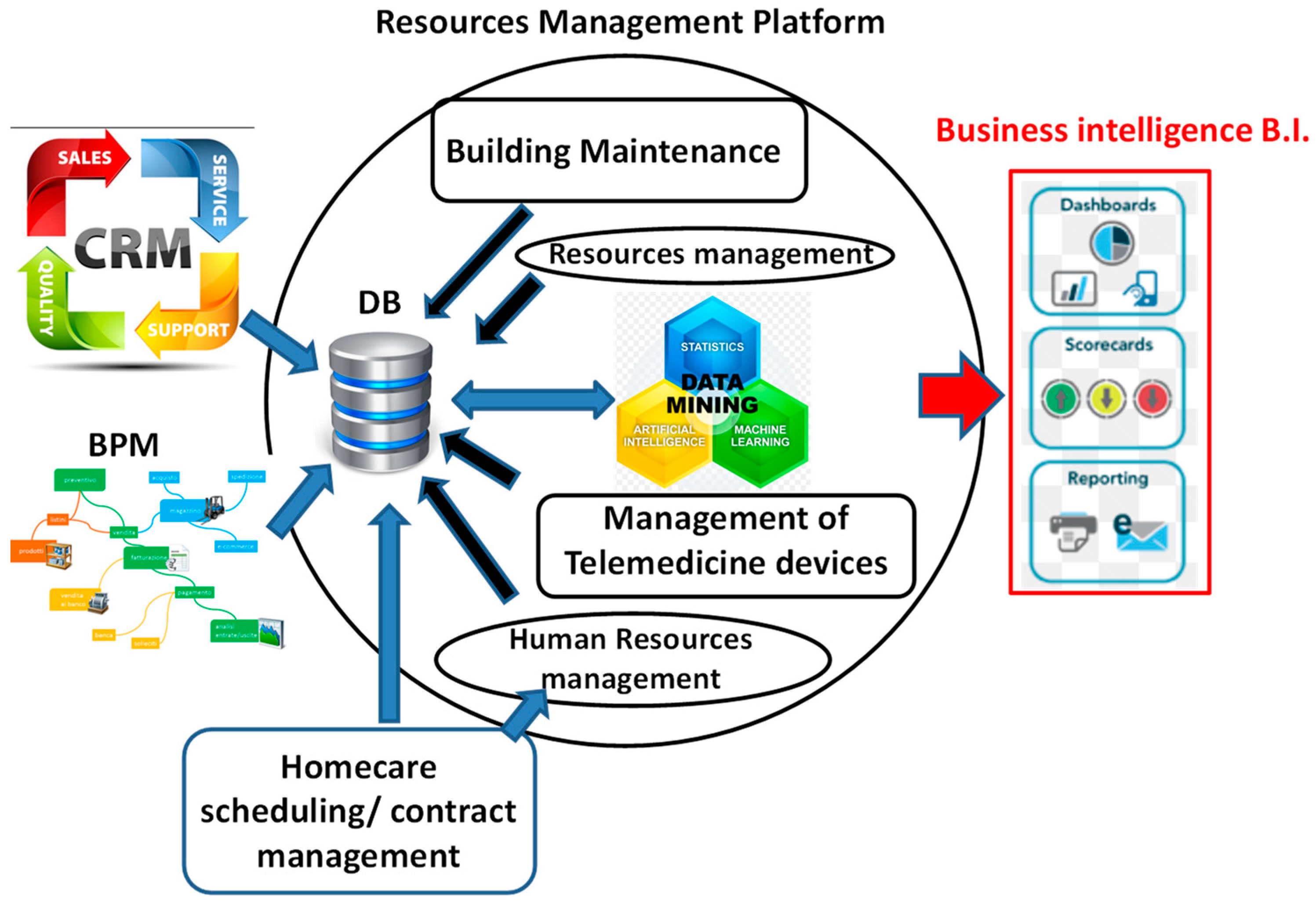
1.2. RMP-DSS Main Features
- CRM module: this module is useful for the optimization of business intelligence (BI) plans by profiling patients and following management activities.
- Homecare module: a digital sign system is implemented to speed up homecare activities and visit scheduling.
- Telemedicine module: some certified medical devices are tested on patients at home; the experimental devices are an ECG (electrocardiogram) device, a spirometer, an infrared thermometer, a pulse oximeter, a device for hematological analysis, a monitoring device of multiple parameters, and a sphygmomanometer device.
- Building maintenance management module: this module is integrated into the resource management platform and is suitable to plan the maintenance of the building structure thus reducing maintenance costs and increasing comfort of the clinic.
- Human resources management module: this module is able to allocate human resources by means of a dynamic scheduler indicating activities; the scheduler takes into account the patient profiling and the performance of the companies’ operators provided by scorecards; this module is also adopted for logistics of nurses and operators.
- Management module for other resources different from human resources (materials, energy, etc.).
- Database (DB) system: different MySQL database systems are implemented to collect data from multiple modules and from medical devices; this DB system is interfaced with the data-mining engine.
- Data-mining engine (ANN): this module is implemented and tested by reading the data of the DB system; neural networks are applied to predict patient status.
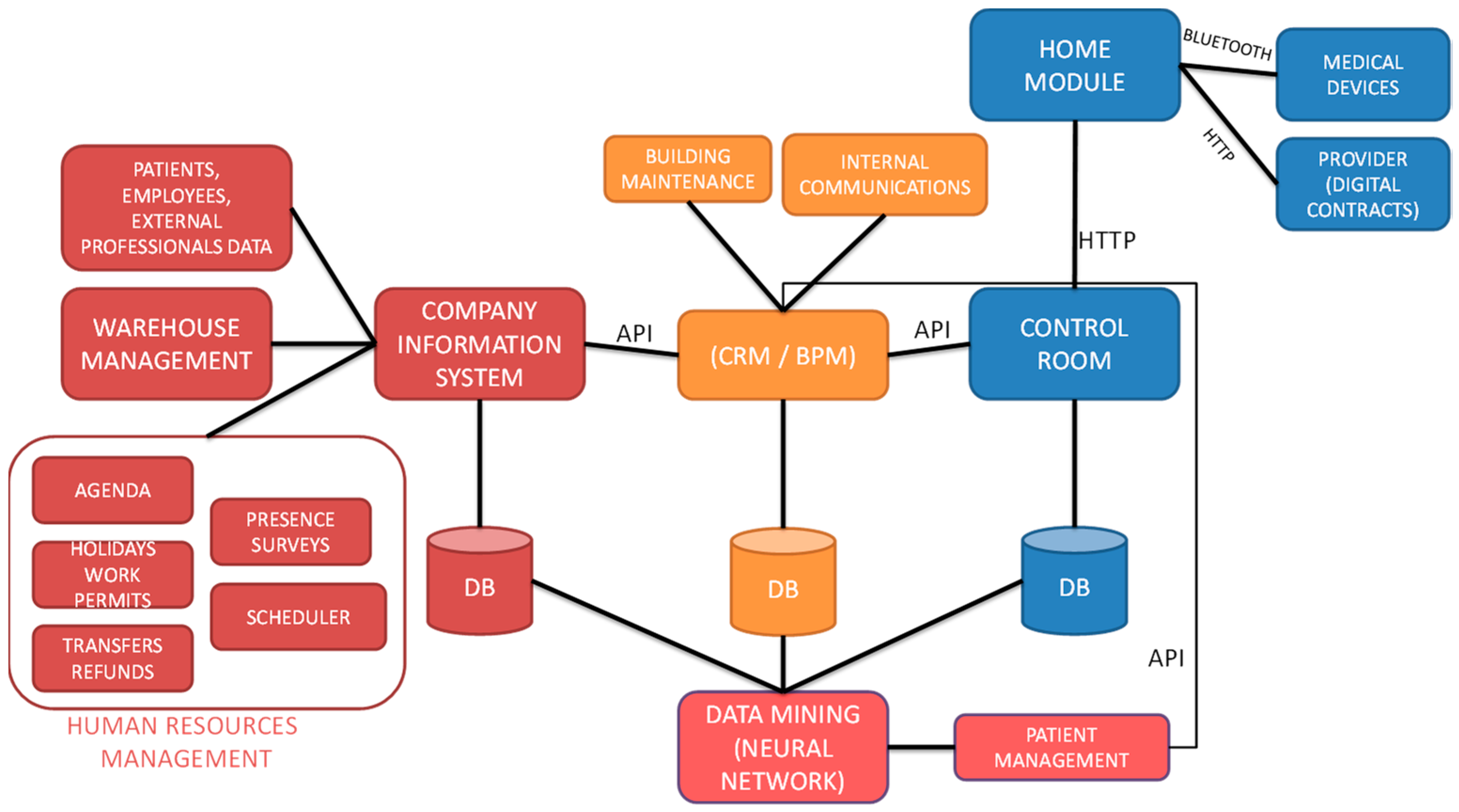
1.3. System Overview: Telemedicine Architecture Integrating RPM-DSS
2. Materials and Methods
3. RPM-DSS Prototype: Design and Implementation
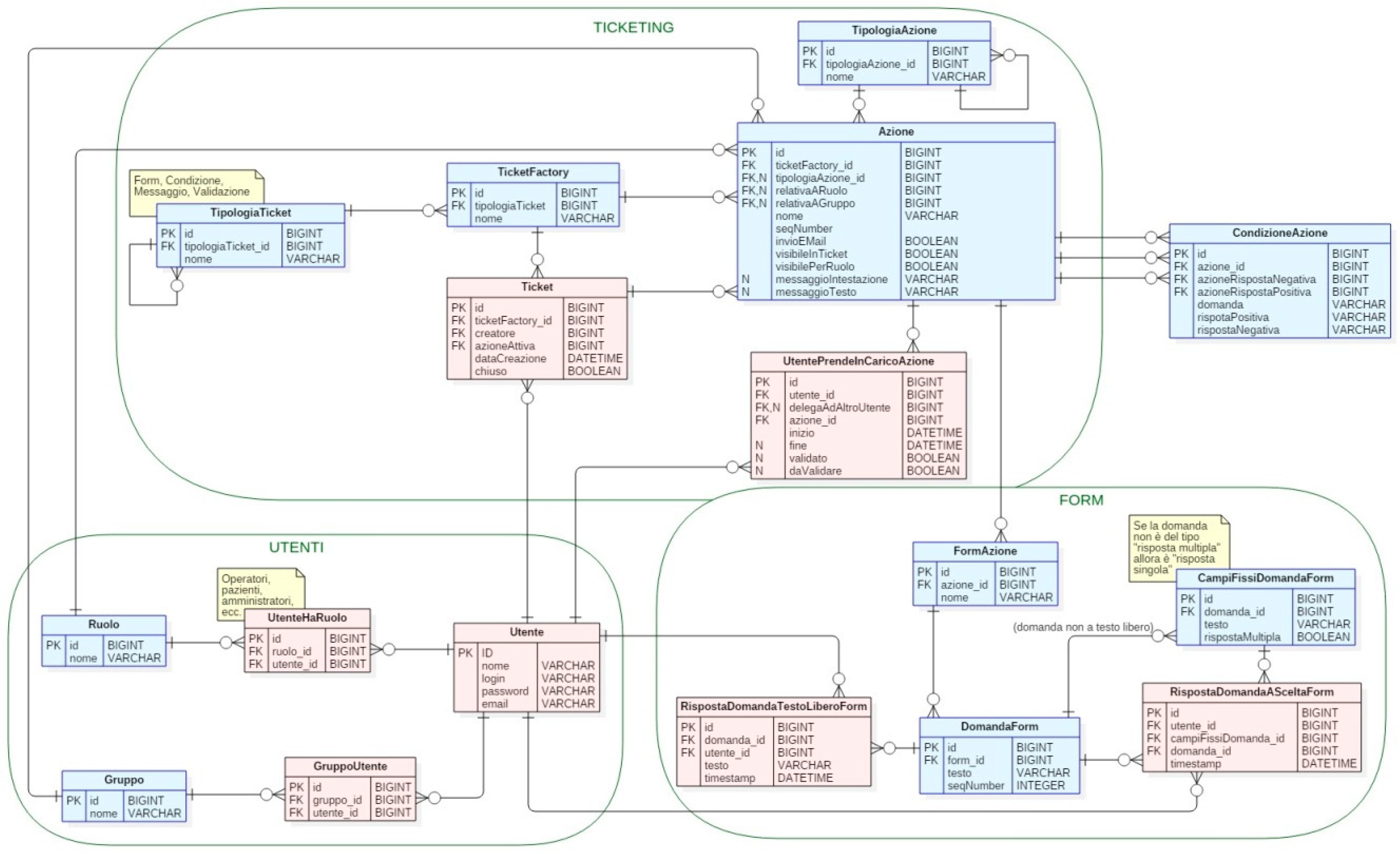
3.1. BPM and CRM Design: Basic Platform for Resources Management
- user ticket creator;
- operator who manages the ticket;
- ticket expiration date;
- list of operators/actors;
- ticket roles and access;
- traceability of the information taking into account historical communications of the ticket;
- traceability of the activities performed during the execution of the ticket.
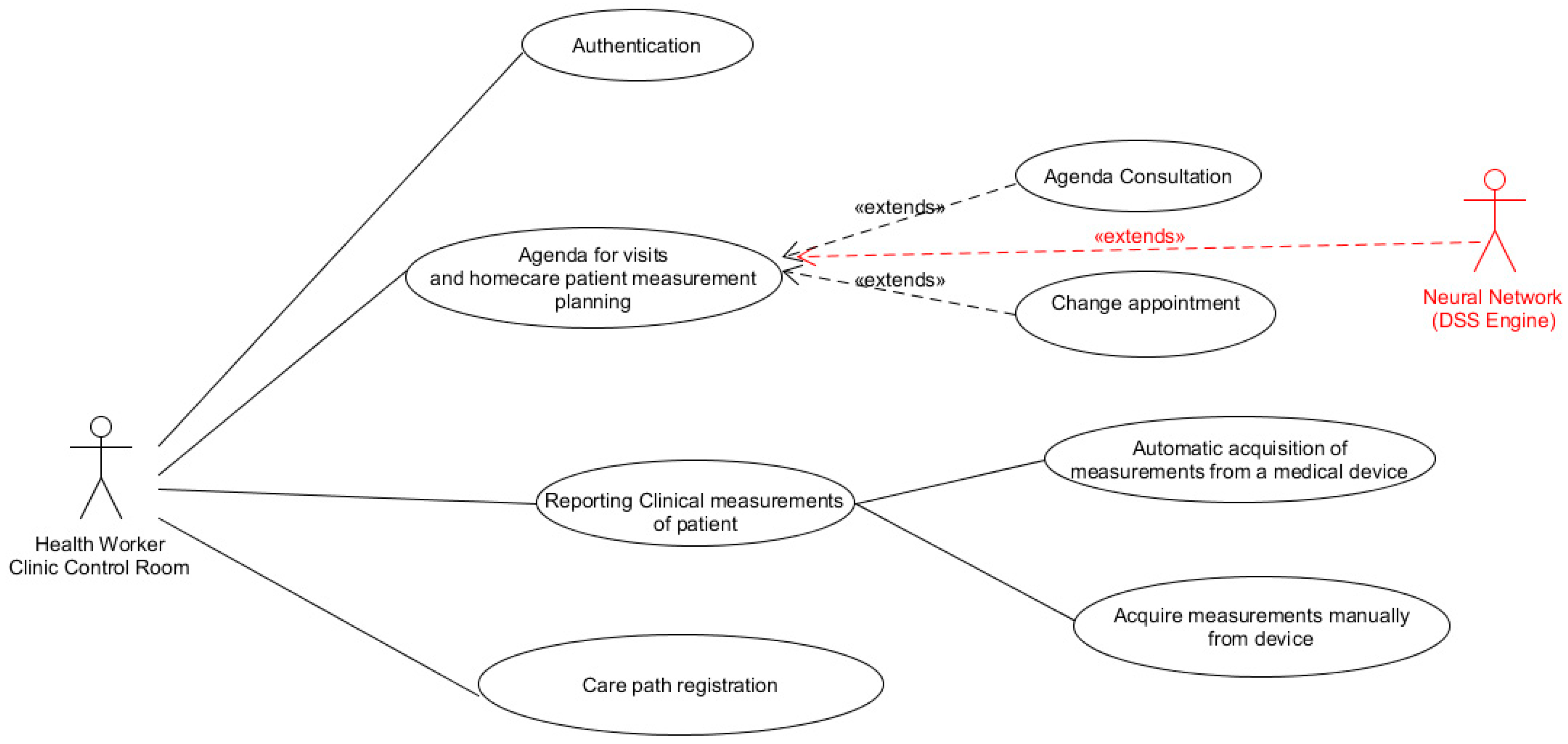
3.2. Artificial Intelligence Engine: Integration in the Homecare Assistance Platform and Health Patient Predictive Maintenance
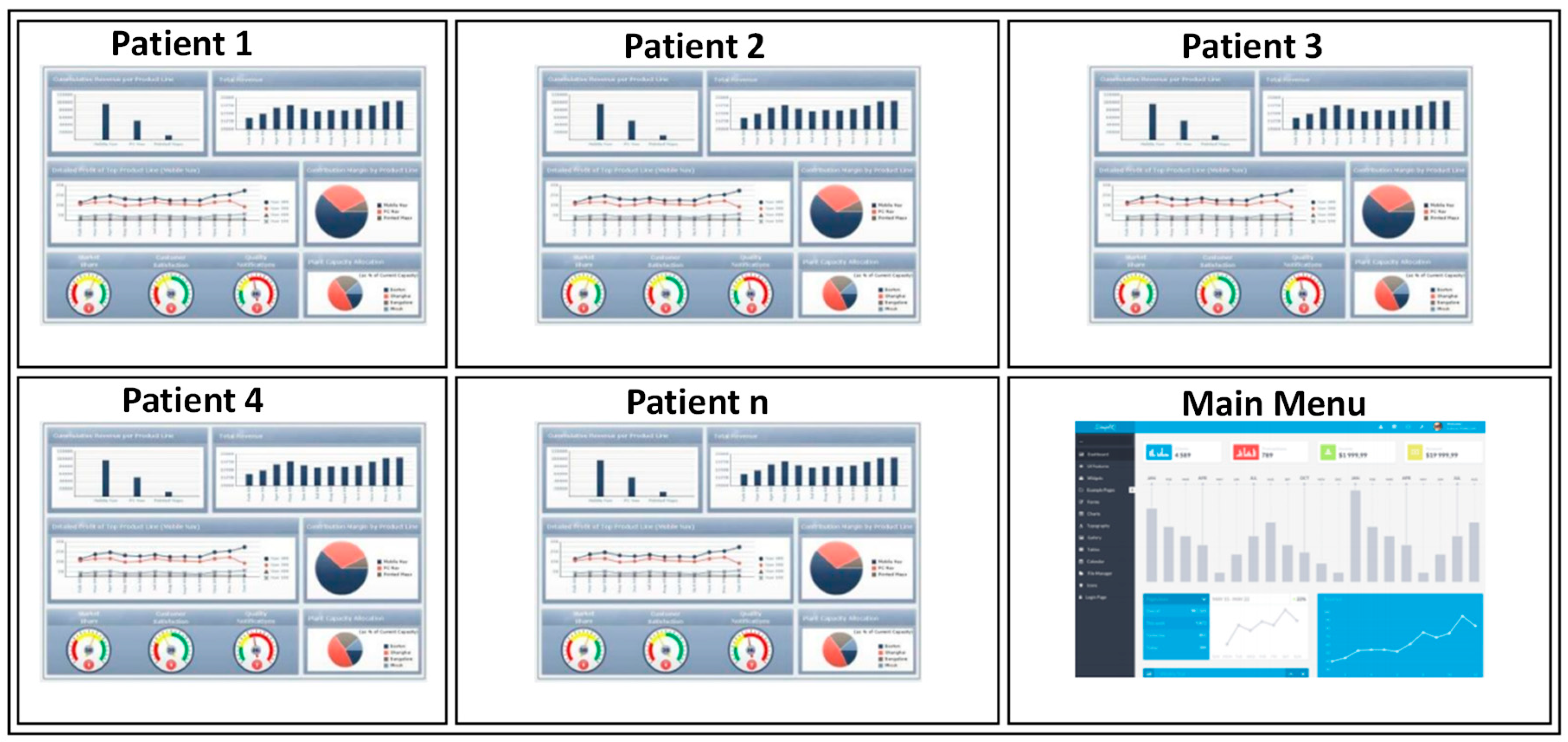
- Health Worker: the worker of the control room of the clinic which controls all patient data;
- Patient: patient at home;
- Health Operator: nurse or other homecare assistance operator;
- Neural Network: main actor of the DSS engine, which is an ANN engine able to predict patient status by processing historical and testing data.
3.3. Sensors Integration for Telemedicine Homecare Control Panel System and DSS System
- data related to the last 12 h;
- data related to the last 24 h;
- data relating to the whole period of monitoring or for periods defined by the doctor.
- add a new patient;
- associate to a patient an identification code (id number);
- manage the tablet connectivity.
3.4. Experimental Dataset and MLP ANN Predictive Results
- Input node (node 1): the input data are loaded in the local repository in order to be pre-processed by means of an Excel Reader (XLS) node by a MySQL DB connector, or by a Phyton Source Node connecting the Cassandra big data system.
- Normalizer (node 2): this node normalizes the values of the numeric columns of the systolic values; the normalization represents the data pre-processing necessary to equilibrate data on an unique scale, thus reducing data dispersion and errors during the followed data process.
- Partitioning (node 3): the input table is split into two partitions (i.e., row-wise), e.g., train and test data. The two partitions are available at the two output ports.
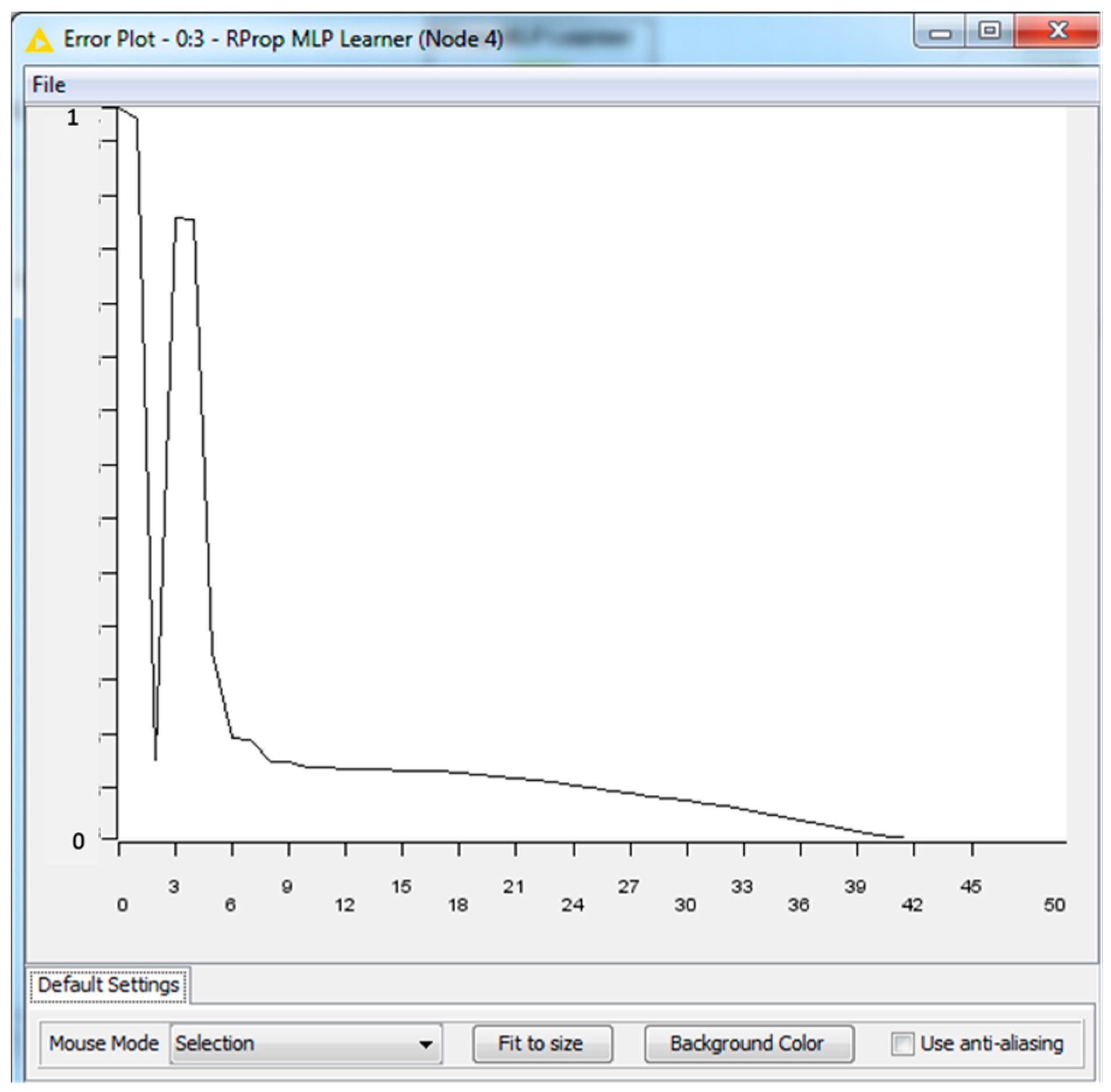
- RProp MLP Learner (node 4): RProp performs a local adaptation of the weight-updates according to the behavior of the error function.
- Multilayer Perceptron Predictor (node 5): this node processed by MLP algorithm the training and testing datasets provided by the first partition and the second partition of node 3, respectively.
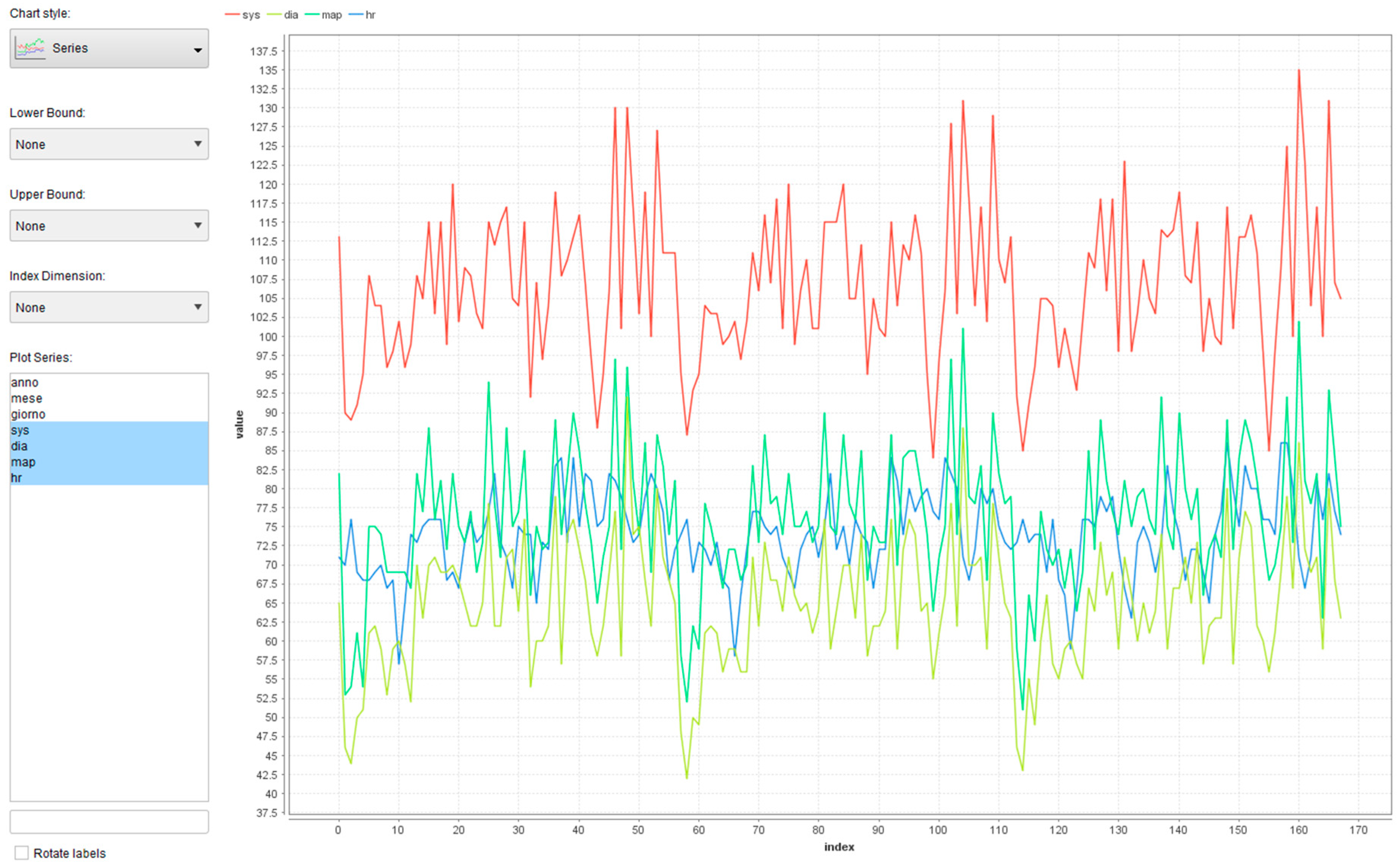
- Line Plot (JavaScript): this node allows to plot graphically output results, such as real values and predicted ones.
- Numeric Sorer (node 7): this node computes certain statistics between the a numeric column’s values (ri) and predicted (pi) values; it computes R² = 1 − SSres/SStot = 1 − Σ(pi − ri)²/Σ(ri − 1/n*Σri)², mean absolute error (1/n*Σ|pi − ri|), mean squared error (1/n*Σ(pi − ri)²), root mean squared error (sqrt(1/n*Σ(pi − ri)²)), and mean signed difference (1/n*Σ(pi − ri)).
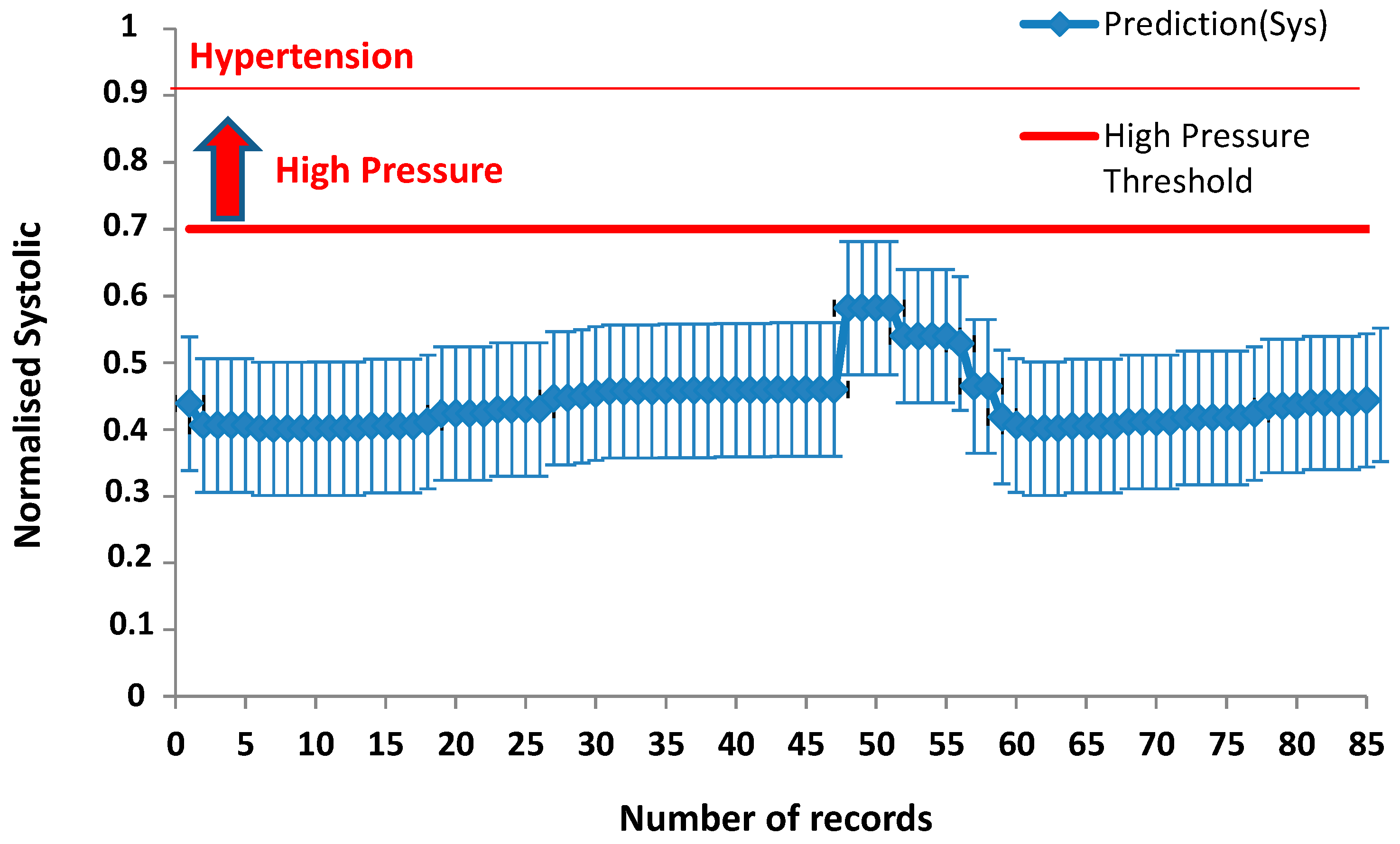
- Excel Writer (XLS): this node exports in an Excel file the output results allowing to further process data, for example by adding error bars (data post-processing).
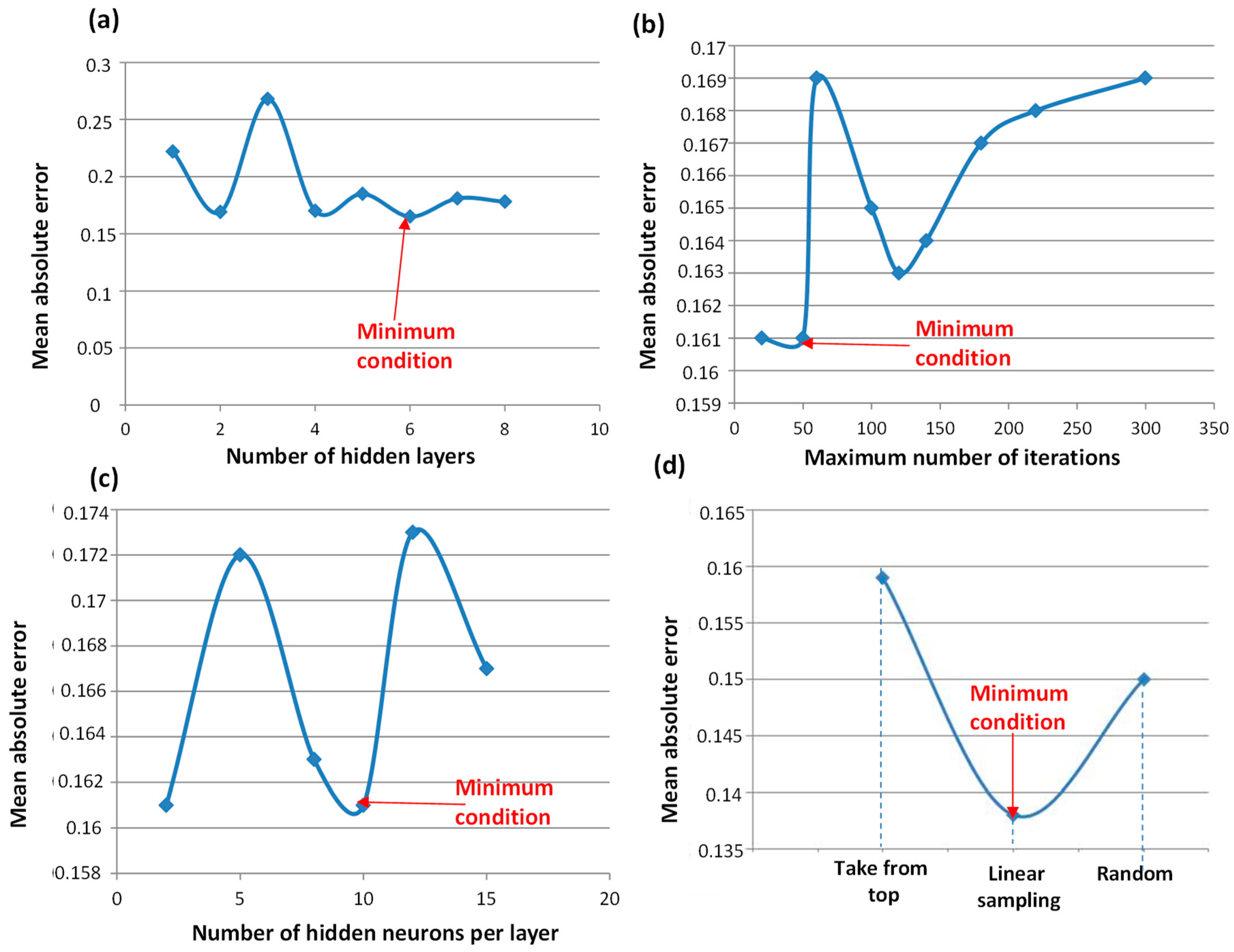
- Take from top (partitioning): this mode puts the top-most rows into the first output table and the remainder in the second table.
- Linear sampling (partitioning): this mode always includes the first and the last row and selects the remaining rows linearly over the whole table.
- Draw randomly (partitioning): random sampling of all rows.
- Number of hidden layers (RProp MLP Learner): number of hidden layers in the architecture of the neural network.
- Maximum number of iterations (RProp MLP Learner): number of learning iterations.
- Number of hidden neurons per layer (RProp MLP Learner): number of neurons contained in each hidden layer.
4. Discussion
- (a)
- Data input phase: by means of a cron activates the prediction by reading patient data from a database; the cron automatizes the prediction process;
- (b)
- Data pre-processing phase: input data are pre-processed and properly partitioned into training and testing branches;
- (c)
- Data processing: the system is learned and tested;
- (d)
- Output: the outputs results are plotted.
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
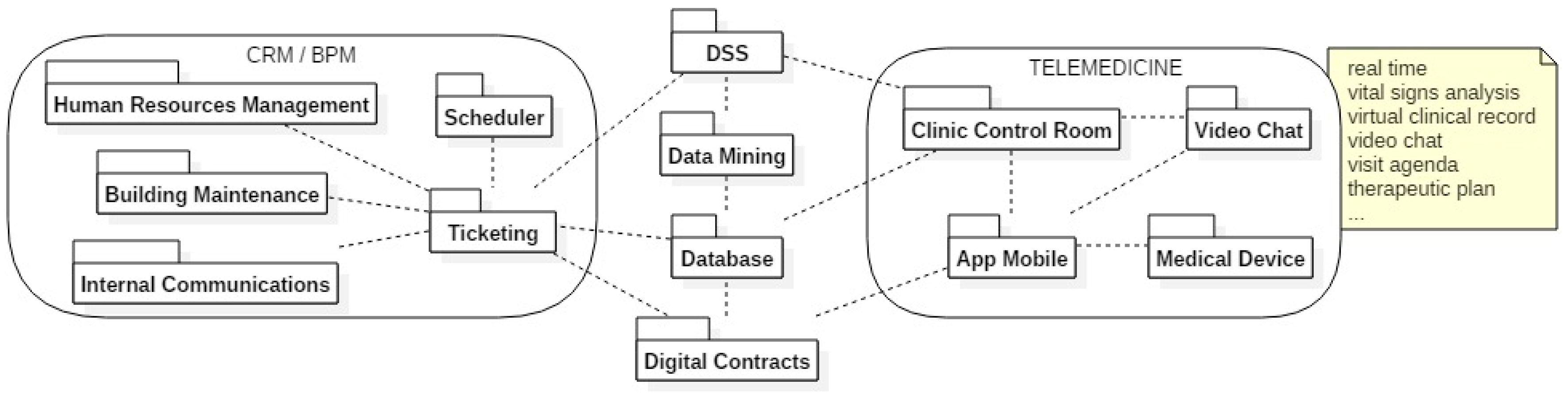
Appendix A. Diagram of the Implemented RPM-DSS Features

Appendix B. Error Plot of the ANN-MLP Approcah

Appendix C. HL7 Protocol

Appendix D. Example of Procedure Validating Sensor Measurements
References
- Naimah, A.; Habidin, N.F.; Jamaludin, N.H.; Khaidir, N.A.; Shazali, N.A. Customer relationship management and organizational performance in Malaysian healthcare industry. Int. J. Adv. Res. Technol. 2013, 2, 1–5. [Google Scholar]
- Chahal, H. Two component customer relationship management model for healthcare services. Manag. Serv. Qual. 2010, 20, 343–365. [Google Scholar] [CrossRef]
- Hsu, C.; Hsu, P.; Chiu, C. Customer relationship management in healthcare service—An integrated DSS framework for patient loyalty. In New Advances in Intelligent Decision Technologies. Studies in Computational Intelligence, 1st ed.; Nakamatsu, K., Phillips-Wren, G., Jain, L.C., Howlett, R.J., Eds.; Springer: Berlin/Heidelberg, Germany, 2009; Volume 199, pp. 509–517. ISBN 978-3-642-00908-2. [Google Scholar]
- Digital and Disrupted: All Change for Healthcare. ROLAND BERGER GMBH. 2016. Available online: https://www.rolandberger.com/de/Publications/pub_digital_and_disrupted_all_change_for_healthcare.html?country=null (accessed on 25 May 2018).
- Li, J.-S.; Yu, H.-Y.; Zhang, X.-G. Data mining in hospital information system. In New Fundamental Technologies in Data Mining, 1st ed.; Funatsu, K., Ed.; InTech: Rijeka, Croatia, 2011; Volume 1, pp. 143–172. ISBN 978-953-307-547-1. [Google Scholar]
- Goodwin, L.; VanDyne, M.; Lin, S. Data mining issues and opportunities for building nursing knowledge. J. Biomed. Inf. 2003, 36, 379–388. [Google Scholar] [CrossRef]
- Belacel, N.; Boulassel, M.R. Multicriteria fuzzy assignment method: A useful tool to assist medical diagnosis. Artif. Intell. Med. 2001, 21, 201–207. [Google Scholar] [CrossRef]
- Demšar, J.; Zupan, B.; Aoki, N.; Wall, M.J.; Granchi, T.H.; Beck, J.R. Feature mining and predictive model construction from severe trauma patient’s data. Int. J. Med. Inf. 2001, 63, 41–50. [Google Scholar] [CrossRef]
- Kusiak, A.; Dixon, B.; Shah, S. Predicting survival time for kidney dialysis patients: A data mining approach. Comp. Biol. Med. 2005, 35, 311–327. [Google Scholar] [CrossRef] [PubMed]
- Yu, H.; Li, J.; Han, X. Data mining analysis of inpatient fees in hospital information system. In Proceedings of the IEEE International Symposium on IT in Medicine & Education ITME2009, Jinan, China, 14–16 August 2009. [Google Scholar]
- Morando, M.; Ponte, S.; Ferrara, E.; Dellepiane, S. Definition of motion and biophysical indicators for home-based rehabilitation through serious games. Information 2018, 9, 105. [Google Scholar] [CrossRef]
- Chae, Y.M.; Kim, H.S.; Tark, K.C.; Park, H.J.; Ho, S.H. Analysis of healthcare quality indicator using data mining and decision support system. Exp. Sys. Appl. 2003, 24, 167–172. [Google Scholar] [CrossRef]
- Ozcan, Y.A. Quantitative Methods in Health Care Management, 2nd ed.; Josey-Bass: California, CA, USA, 2009; pp. 10–44. ISBN -13. [Google Scholar]
- Galiano, A.; Massaro, A.; Boussahel, B.; Barbuzzi, D.; Tarulli, F.; Pellicani, L.; Renna, L.; Guarini, A.; De Tullio, G.; Nardelli, G.; et al. Improvements in haematology for home health assistance and monitoring by a web based communication system. In Proceedings of the IEEE International Symposium on Medical Measurements and Applications, Benevento, Italy, 15–18 May 2016. [Google Scholar]
- Matlani, P.; Londhe, N.D. A cloud computing based telemedicine service. In Proceedings of the Point-of-Care Healthcare Technologies (PHT), Bangalore, India, 16–18 January 2013. [Google Scholar]
- Hsieh, J.; Hsu, M.W. A cloud computing based 12—Lead ECG telemedicine service. BMC Med. Inf. Dec. Mak. 2012, 12, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Ghavami, P.; Kapur, K. Artificial neural network-enabled prognostics for patient health management. In Proceedings of the Prognostics and Health Management (PHM), Denver, CO, USA, 18–21 June 2012. [Google Scholar]
- Grossi, E. Artificial Neural Networks and Predictive Medicine: A Revolutionary Paradigm Shift. In Artificial Neural Networks—Methodological Advances and Biomedical Applications, 1st ed.; Suzuki, K., Ed.; InTech: Rijeka, Croatia, 2011; Volume 1, pp. 130–150. ISBN 978-953-307-243-2. [Google Scholar]
- Adhikari, N.C.D. Prevention of heart problem using artificial intelligence. Int. J. Artif. Intell Appl. 2018, 9, 21–35. [Google Scholar] [CrossRef]
- Massaro, A.; Maritati, V.; Galiano, A. Data Mining model performance of sales predictive algorithms based on RapidMiner workflows. Int. J. Comp. Sci. Inf. Technol. 2018, 10, 39–56. [Google Scholar] [CrossRef]
- Massaro, A.; Galiano, A.; Meuli, G. Overview and application of enabling technologies oriented on energy routing monitoring, on network installation and on predictive maintenance. Int. J. Artif. Intell Appl. 2018, 9, 1–20. [Google Scholar] [CrossRef]
- Massaro, A.; Maritati, V.; Galiano, A.; Birardi, V.; Pellicani, L. ESB platform integrating KNIME data mining tool oriented on Industry 4.0 based on artificial neural network predictive maintenance. Int. J. Artif. Intell Appl. 2018, 9, 1–17. [Google Scholar] [CrossRef]
- Wimmer, H.; Powell, L.M. A comparison of open source tools for data science. J. Inf. Syst. Appl. Res. 2016, 9, 4–12. [Google Scholar]
- Al-Khoder, A.; Harmouch, H. Evaluating four of the most popular open source and free data mining tools. Int. J. Acad. Scient. Res. 2015, 3, 13–23. [Google Scholar]
- Gulli, A.; Pal, S. Deep Learning with KERAS—Implement Neural Networks with Keras on Theano and Tensor Flow; Packt Publishing: Birmingham, UK, 2017; ISBN 978-1-78712-842-2. [Google Scholar]
- Kovalev, V.; Kalinovsky, A.; Kovalev, S. Deep Learning with Theano, Torch, Caffe, TensorFlow, and deeplearning4j: Which one is the best in speed and accuracy? In Proceedings of the XIII International Conference on Pattern Recognition and Information Processing, Minsk, Belarus, 3–5 October 2016; pp. 99–103. [Google Scholar]
- Al-Shayea, Q.K. Artificial neural networks in medical diagnosis. Int. J. Comp. Sci. Issue 2011, 8, 150–154. [Google Scholar]
- Braun, H. A direct adaptive method for faster backpropagation learning: The RPROP algorithm. In Proceedings of the IEEE International Conference on Neural Networks, San Francisco, CA, USA, 28 March–1 April 1993. [Google Scholar]
- Igel, C.; Toussaint, M.; Weishui, W. RProp using the natural gradient. In Trends and Applications in Constructive Approximation; Mache, D.H., Szabados, J., de Bruin, M.G., Eds.; Birkhäuser: Basel, Switzerland, 2005; Volume 151, pp. 259–272. ISBN 978-3-7643-7124-1. [Google Scholar]
- Bastos, P.; Lopes, I.; Pires, L. Application of data mining in a maintenance system for failure prediction. In Safety, Reliability and Risk Analysis: Beyond the Horizon; Steenbergen, R., Van Gelder, P.H.A.J.M., Miraglia, S., Vrouwenvelder, T., Eds.; Taylor & Francis Group: London, UK, 2014; pp. 933–940. ISBN 978-1-138-00123-7. [Google Scholar]
- Communication from the Commission to the European Parliament, the Council, the European Economic and Social Committee and the Committee of the Regions on Telemedicine for the Benefit of Patients, Healthcare Systems and Society. Available online: https://ec.europa.eu/transparency/regdoc/rep/1/2008/EN/1-2008-689-EN-F1-1.pdf (accessed on 19 June 2018).
- Telemedicina—Linee di Indirizzo Nazionali (Approved by Italian Superior Council of Helath, 10 July 2012). Available online: http://www.salute.gov.it/imgs/C_17_pubblicazioni_2129_allegato.pdf (accessed on 19 June 2018).
- Cassandra: JDBC Driver Download. Available online: https://www.cdata.com/drivers/cassandra/download/jdbc/ (accessed on 25 May 2018).
- HL7 Health Level Seven International. Available online: http://www.hl7.org/implement/standards/product_section.cfm?section=1 (accessed on 19 June 2018).














{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Functionalities | Proposed RPM-DSS System | System Proposed in Reference [14] |
|---|---|---|
| Real-time monitoring (smart-sensor data) | √ | √ |
| Control panel room linked to patients at home (point to multi-point connection) | √ | √ |
| Wireless sensor (patient data) | √ | √ |
| Bidirectional communication system | √ | x |
| High number of supported sensors | √ | x |
| Video chat | √ | x |
| DSS multi-level | √ | x |
| Patient status prediction (MLP-ANN) | √ | x |
| DSS supporting BPM and visits scheduling | √ | x |
| BPM integration | √ | x |
| CRM integration | √ | x |
| Connection with a big data system | √ | x |
| Mobile device behaving as a router | √ | x |
| Predisposition for cross services | √ | x |
| Device | Functionality | Connectivity |
|---|---|---|
| Pulse oximeter | Blood oxygen saturation, pedometer, heartbeat | Bluetooth |
| ECG mobile | One channel ECG | Bluetooth |
| Spirometer | Respiratory function | Bluetooth |
| Sphygmomanometer | Blood pressure, heartbeat | Bluetooth |
| Infrared thermometer | Body temperature °C | Bluetooth |
| Device of multiple parameters | Heartbeat, external and internal body temperature, SpO2, NIBP, 5-channel ECG | Ethernet/WiFi |
| Hematological device | Hematological analysis | Ethernet |
| Category | Systolic (mmHg) | Diastolic (mmHg) |
|---|---|---|
| Hypotension | <90 | <60 |
| Normal | 90–119 | 60–79 |
| Stage 1 hypertension | 130–139 | 80–89 |
| Stage 2 hypertension | >140 | >90 |
| Hypertensive crisis | ≥180 | ≥120 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Massaro, A.; Maritati, V.; Savino, N.; Galiano, A.; Convertini, D.; De Fonte, E.; Di Muro, M. A Study of a Health Resources Management Platform Integrating Neural Networks and DSS Telemedicine for Homecare Assistance. Information 2018, 9, 176. https://doi.org/10.3390/info9070176
Massaro A, Maritati V, Savino N, Galiano A, Convertini D, De Fonte E, Di Muro M. A Study of a Health Resources Management Platform Integrating Neural Networks and DSS Telemedicine for Homecare Assistance. Information. 2018; 9(7):176. https://doi.org/10.3390/info9070176
Chicago/Turabian StyleMassaro, Alessandro, Vincenzo Maritati, Nicola Savino, Angelo Galiano, Daniele Convertini, Emanuele De Fonte, and Maurizio Di Muro. 2018. "A Study of a Health Resources Management Platform Integrating Neural Networks and DSS Telemedicine for Homecare Assistance" Information 9, no. 7: 176. https://doi.org/10.3390/info9070176