Hemocompatibility of Inorganic Physical Vapor Deposition (PVD) Coatings on Thermoplastic Polyurethane Polymers

Abstract
:1. Introduction
2. Results and Discussion


3. Experimental Section
3.1. Substrate Materials, Surface Modification and Deposited Films

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Material | Deposition technique | Target material | Target manufacturer | Process gases |
|---|---|---|---|---|
| Ti | Sputter (DC) | Ti (grade 2) | Eurotitan GmbH, Solingen, Germany | Ar |
| TiN | PLD | Ti (grade 2) | N2, Ar | |
| TiOx | Sputter (HF) | Ti (grade 2) | O2, Ar | |
| a-C:H | Sputter (HF) | Electrocarbon graphite (99.7% carbon) | Hoffmann & Co., Steeg, Austria | C2H2, Ar |
| Si:a-C:H | Sputter (RF) | Ti (grade 2) | Eurotitan GmbH, Solingen, Germany | C2H2, Ar |
| Ti:a-C:H | Sputter (HF) | Ti (grade 2) | C2H2, Ar | |
| Ti:a-C:H:N | PLD | Ti (grade 2) | C2H2, N2, Ar |

3.2. Platelet Function Testing
3.2.1. Materials
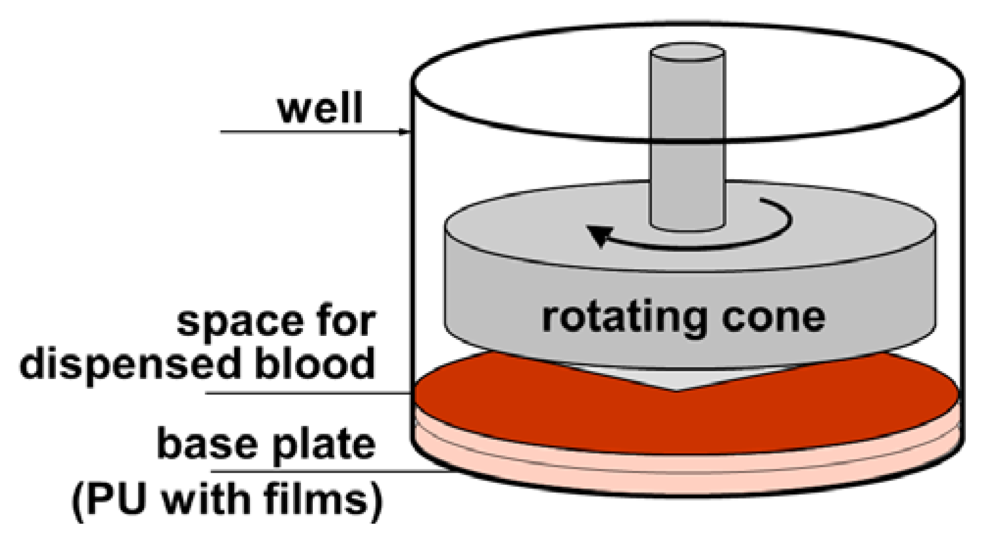
3.2.2. Cone-and-Plate(let) Analyzer Testing

3.2.3. Flow Cytometry for Platelet Analysis in Blood
3.2.4. Thromogenic Microparticle Activity Analysis
3.3. Statistics
4. Conclusions
Acknowledgments
References
- Hasebe, T.; Shimada, A.; Suzuki, T.; Matsuoka, Y.; Saito, T.; Yohena, Y. Fluorinated diamond-like carbon as antithrombogenic coating for blood-contacting devices. J. Biomed. Mater. Res. A 2006, 76, 86–94. [Google Scholar]
- Hussain, M.; Siedlecki, C. The platelet integrin alpha(IIb) beta(3) imaged by atomic force microscopy on model surfaces. Micron 2004, 35, 565–573. [Google Scholar] [CrossRef]
- Massa, T.; Yang, M.; Ho, J. Fibrinogen surface distribution correlates to platelet adhesion pattern on fluorinated surface-modified polyetherurethane. Biomaterials 2005, 26, 7367–7376. [Google Scholar] [CrossRef]
- Yang, P.; Huang, N.; Lenge, Y. Activation of platelets adhered on amorphous hydrogenated carbon films synthesized by plasma immersion ion implantation-deposition (PIII-D). Biomaterials 2003, 24, 2821–2829. [Google Scholar] [CrossRef]
- Plant, S.; Grant, D.; Leach, L. Surface modification of NiTi alloy and human platelet activation under static and flow conditions. Mater. Lett. 2007, 61, 2864–2867. [Google Scholar] [CrossRef]
- Cui, F.; Li, D. A review of investigations on biocompatibility of diamond-like carbon and carbon nitride films. Surf. Coat. Technol. 2000, 131, 481–487. [Google Scholar] [CrossRef]
- Hauert, R.; Müller, U. An overview on tailored tribological and biological behavior of diamond-like carbon. Diam. Relat. Mater. 2003, 12, 171–177. [Google Scholar] [CrossRef]
- Vinnichenko, M.; Gago, R.; Huang, N. Spectroscopic ellipsometry investigation of amorphous carbon films with different sp3 content: Relation with protein adsorption. Thin Solid Films 2004, 455–456, 530–534. [Google Scholar] [CrossRef]
- Maguire, P.; McLaughlin, J.; Okpalugo, T. Mechanical stability, corrosion performance and bioresponse of amorphous diamond-like carbon for medical stents and guidewires. Diam. Relat. Mater. 2005, 14, 1277–1288. [Google Scholar] [CrossRef]
- Lackner, J.M.; Waldhauser, W. Inorganic PVD and CVD coatings in medicine—A review of protein and cell adhesion on coated surfaces. J. Adhes. Sci. Technol. 2010, 24, 925–961. [Google Scholar] [CrossRef]
- Charitidis, C.; Logothetidis, S.; Gioti, M. A comparative study of the nanoscratching behavior of amorphous carbon films grown under various deposition conditions. Surf. Coat. Technol. 2000, 125, 201–206. [Google Scholar] [CrossRef]
- Robertson, J. Diamond-like amorphous carbon. Mater. Sci. Eng. 2002, 37, 129–281. [Google Scholar] [CrossRef]
- Kubova, O.; Svorcik, V.; Heitz, J. Characterization and cytocompatibility of carbon layers prepared by photo-induced chemical vapor deposition. Thin Solid Films 2007, 515, 6765–6772. [Google Scholar] [CrossRef]
- Saito, T.; Hasebe, T.; Yohena, S.; Matsuoka, Y.; Kamijo, A.; Takahashi, K. Antithrombogenicity of fluorinated diamond-like carbon films. Diam. Relat. Mater. 2005, 14, 1116–1119. [Google Scholar] [CrossRef]
- Hasebe, T.; Matsuoka, Y.; Kodama, H.; Saito, T.; Yohena, S.; Kamijo, A. Lubrication performanceof diamond-like carbon and fluorinated diamond-like carbon coatings for intravascular guidewires. Diam. Relat. Mater. 2006, 15, 129–132. [Google Scholar] [CrossRef]
- Okpalugo, T.I.; Ogwu, A.A.; Maguire, P.D.; McLaughlin, J.A. Platelet adhesion on silicon modified hydrogenated amorphous carbon films. Biomaterials 2004, 25, 239–245. [Google Scholar] [CrossRef]
- Kwok, S.C.H.; Wang, J.; Chu, P.K. Surface energy, wettability, and blood compatibility phosphorus doped diamond-like carbon films. Diam. Relat. Mater. 2005, 14, 78–85. [Google Scholar] [CrossRef]
- Maitz, M.F.; Gago, R.; Abendroth, B.; Camero, M.; Caretti, I.; Kreissig, L. Hemocompatibility of low-friction boron-carbon-nitrogen containing coatings. J. Biomed. Mater. Res. B 2006, 77, 179–187. [Google Scholar]
- Hong, J.; Andersson, J.; Nilsson Ekdahl, K.; Elgue, G.; Axen, N; Larsson, R.; Nilsson, B. Titanium is a highly thrombogenic biomaterial. Possible implications for osteogenesis. Thromb. Haemost. 1999, 82, 58–64. [Google Scholar]
- Hauert, R. A review of modified DLC coatings for biological applications. Diam. Relat. Mater. 2003, 12, 583–589. [Google Scholar] [CrossRef]
- Roy, R.K.; Lee, K.-R. Biomedical applications of diamond-like carbon coatings: A review. J. Biomed. Mater. Res. B 2007, 38B, 72–84. [Google Scholar]
- Jones, M.I.; McColl, I.R.; Grant, D.M.; Parker, K.G.; Parker, T.L. Protein adsorption and platelet attachment and activation, on TiN, TiC, and DLC coatings on titanium for cardiovascular applications. J. Biomed. Mater. Res. 2000, 52, 413–421. [Google Scholar] [CrossRef]
- Cui, F.Z.; Li, D.J. A review of investigations on biomcompatibility of diamond-like carbon and carbon nitride films. Surf. Coat. Technol. 2000, 131, 481–487. [Google Scholar] [CrossRef]
- Gorbet, M.B.; Sefton, M.V. Biomaterial-associated thrombosis: Roles of coagulation factors, complement, platelets and leukocyte. Biomaterials 2004, 25, 5681–5703. [Google Scholar] [CrossRef]
- Andrews, R.K.; Lopez, J.A.; Berndt, MC. Molecular mechanisms of platelet adhesion and activation. Int. J. Biochem. Cell Biol. 1997, 29, 91–105. [Google Scholar] [CrossRef]
- Bithell, T.C. The physiology of primary hemostasis. In Wintrobe’s Clinical Hematology, 9th; Lee, G.R., Bithell, T.C., Foerster, J., Athens, J.W., Lukens, J., Eds.; Lea and Febinger: Philadelphia, PA, USA, 1993. [Google Scholar]
- O’Brien, J.R. Shear-induced platelet aggregation. Lancet 1990, 335, 711–713. [Google Scholar] [CrossRef]
- Marcus, A.J. Platelet activation. In Atherosclerosis and Coronary Artery Disease; Fuster, V., Ross, R., Topol, E.J., Eds.; Lippincott-Raven Publishers: Philadelphia, PA, USA, 1996; pp. 607–637. [Google Scholar]
- Calvette, J.J. Clues for understanding the structure and function of a prototypic human integrin: The platelet glycoprotein IIb/IIIa complex. Thromb. Haemost. 1994, 72, 1–15. [Google Scholar]
- Sixma, J.J. teraction of blood platelets with the vessel wall. In Haemostasis and Thrombosis, 3rd; Bloom, A., Forbes, C.D., Eds.; Churchill Livingston: New York, NY, USA, 1994; pp. 259–285. [Google Scholar]
- Charo, I.F.; Nannizzi, I.; Phillips, D.R.; Hsu, M.A.; Scarborough, R.M. Inhibition of fibrinogen binding to GPIIb-IIIa by a GPIIIa peptide. J. Biol. Chem. 1991, 266, 1415–1421. [Google Scholar]
- Gawaz, M.P. Blood Platelets; Thieme: Stuttgart, Germany, 2001; pp. 12–24. [Google Scholar]
- Nieuwland, R.; Bercmans, R.J.; Rotteveel-Eijkman, R.C. Cell-derived microparticle gnerated in patients during cardiopulmonary bypass are highly procoagulant. Circulation 1997, 96, 3534–3541. [Google Scholar] [CrossRef]
- Rinder, H.M.; Tracey, J.L.; Rinder, C.S.; Leitenberg, D.; Smith, B.R. Neutrophil but not monocyte activation inhibits P-selectin-mediated platelet adhesion. Throm. Haemost. 1994, 72, 750–756. [Google Scholar]
- Rinder, H.M.; Bonan, J.L.; Rinder, C.S.; Ault, K.A.; Smith, B.R. Dynamics of leukocyte-platelet adhesion in whole blood. Blood 1991, 87, 1730–1737. [Google Scholar]
- Cholokis, C.H.; Zingg, W.; Sefton, M.V. Effect of heparin-PVA hydrogel on platelets in a chronic canine AV shunt. J. Biomed. Mater. Res. 1989, 23, 417–441. [Google Scholar] [CrossRef]
- Hanson, S.R.; Harker, L.A.; Ratner, B.D.; Hoffman, A.S. In vivo evaluation of artificial surfaces with a nonhuman primate model of arterial thrombosis. J. Lab. Clin. Med. 1980, 95, 289–304. [Google Scholar]
- Ip, W.F.; Sefton, M.V. Platelet consumption by NHLBI reference materials and silastic. J. Biomed. Mater. Res. 1991, 25, 1321–1324. [Google Scholar] [CrossRef]
- Sanak, M.; Jakiela, B.; Wegrzyn, W. Assessment of hemocompatibility of materials with arterial blood flow by platelet functional test. Bull. Pol. Acad. Sci. Tech. Sci. 2010, 58, 317–321. [Google Scholar]
- Tans, G.; Rosing, J.; Christella, M. Comparison of anticoagulant and procoagulant activities of stimulated platelets and platelet-derived microparticles. Blood 1991, 88, 2641–2648. [Google Scholar]
- Gemmell, C.H. Assessment of material-induced procoagulant activity by a modified Russell viper venom coagulation time test. J. Biomed. Mater. Res. 1998, 42, 611–616. [Google Scholar] [CrossRef]
- Sbrana, S.; Della Pina, F.; Rizza, A.; Buffa, M.; De Filipis, R.; Gianetti, J.; Clerico, A. relationship between optical aggregometry (type born) and flow cytometry in evaluation ADP-induced platelet activation. Cytom. B Clin. Cytom. 2008, 74, 30–39. [Google Scholar]
- Sims, P.J.; Wiedmer, T. Induction of cellular procoagulant activity by the membrane attack complex of complement. Semin. Cell Biol. 1995, 6, 275–282. [Google Scholar]
- Jy, W.; Mao, W.-W.; Horstman, L.L.; Tao, J.; Ahn, Y.S. Platelet microparticles bind, activate and aggregate neutrohils in vitro. Blood Cells Mol. Dis. 1992, 21, 217–231. [Google Scholar]
- Nomura, S.; Ozaki, Y.; Ikeda, Y. Function and role of microparticles in various clinical settings. Thromb. Res. 2008, 123, 8–23. [Google Scholar] [CrossRef]
- Blann, A.; Shantsila, E.; Shantsila, A. Microparticles and arterial disease. Semin. Thromb. Hemost. 2009, 35, 488–496. [Google Scholar] [CrossRef]
- Siljander, P.; Carpen, O.; Lassila, R. Platelet derived microparticles associate with fibrin during thrombosis. Blood 1996, 87, 4651–4653. [Google Scholar]
- Holme, P.A.; Solum, N.O.; Brosstad, F.; Pedersen, T.; Kveine, M. Microvesicles bind soluble fibrinogen, adhere to immmobilized fibrinogen and coaggregates with platelets. Thromb. Haemost. 1998, 79, 389–394. [Google Scholar]
- Cozens-Roberts, C.; Quinn, A.; Lauffenburger, D.A. Receptor-mediated adhesion phenomena. I. Model studies with the radial-flow detachment assay. Biophys. J. 1990, 58, 107–125. [Google Scholar] [CrossRef]
- Cozens-Roberts, C.; Quinn, A.; Lauffenburger, D.A. Receptor-mediated cell attachment and detachment kinetics. II. Experimental model studies with the radial-flow detachment assay. Biophys. J. 1990, 58, 857–872. [Google Scholar] [CrossRef]
- Decave, E.; Garrivier, D.; Brechet, Y.; Fourcade, B.; Bruckert, F. Shear flow-induced detachment kinetics of Dictyostelium discoideum cells from solid substrate. Biophys. J. 2002, 82, 2383–2395. [Google Scholar] [CrossRef]
- Di Milla, P.A.; Stone, J.A.; Quinn, A.; Albelda, S.M.; Lauffenburger, D.A. Maximal migration of human smooth muscle cells on fibronectin and type IV collagen occurs at an intermediate attachment strength. J. Cell Biol. 1993, 122, 729–737. [Google Scholar] [CrossRef]
- Lackner, J.M.; Waldhauser, W.; Major, R.; Major, B.; Bruckert, F. Hemocompatible pulsed laser deposited coatings on polymers. Biomed. Tech. 2010, 55, 57–64. [Google Scholar] [CrossRef]
- Spijker, H.T.; Graaff, R.; Boonstra, P.W.; Busscher, J.H.; van Oeveren, W. On the influence of flow conditions and wettability on blood material interactions. Biomaterials 2003, 24, 4717–4727. [Google Scholar] [CrossRef]
- Bonnefoy, A.; Liu, Q.; Legrand, C.; Frojmovic, M.M. Efficiency of platelet adhesion to fibrinogen depends on both cell activation and flow. Biophys.J. 2000, 78, 2834–2843. [Google Scholar] [CrossRef]
- Tandon, P.; Diamond, S.L. Hydrodynamic effects and interactions of platelets and their aggregates in linear shear flow. Biophys. J. 1997, 73, 2819–2835. [Google Scholar] [CrossRef]
- Lackner, J.M. Industrially-scaled Pulsed Laser Deposition at Room Temperature; Orekop: Krakow, Poland, 2005. [Google Scholar]
- Lackner, J.M. Innovatives Schichtdesign Mittels Pulsed Laser Deposition. Ph.D. Dissertation, University of Leoben: Leoben, Austria. 2003. [Google Scholar]
- Lackner, J.M.; Waldhauser, W.; Schwarz, M.; Mahoney, L.; Major, L.; Major, B. Polymer pre-treatment by linear anode layer source plasma for adhesion improvement of sputtered TiN coatings. Vacuum 2008, 83, 302–307. [Google Scholar] [CrossRef]
- Kahn, M. Room-Temperature Deposition of DLC Films by an Ion Beam Method, Reactive Magnetron Sputtering and Pulsed Laser Deposition: Process Design, Film Structure and Film Properties. Ph.D. Dissertation, University of Leoben: Leoben, Austria. 2009. [Google Scholar]
- Lackner, J.M.; Waldhauser, W.; Alamanou, A.; Teichert, C.; Schmied, F.; Major, L. Mechanisms for self-assembling topography formation in low-temperature vacuum deposition of inorganic coatings on polymer surface. Bull. Pol. Acad. Sci. Tech. Sci. 2010, 58, 281–294. [Google Scholar]
- Seyfert, U.T.; Biehl, V.; Schenk, J. In vitro hemocompatibility testing of biomaterials according to the ISO 10993-4. Biomol. Eng. 2002, 19, 91–96. [Google Scholar] [CrossRef]
- Otto, M.; Klein, C.L.; Köhler, H.; Wagner, M.; Röhrig, O.; Kirkpatrick, C.J. Dynamic blood cell contact with biomaterials: Validation of a flow chamber system according to international standards. J. Mater. Sci. Mater. Med. 1997, 8, 119–129. [Google Scholar] [CrossRef]
- Streller, U.; Sperling, C.; Hübner, J.; Ranke, R.; Werner, C. Design and evaluation of novel blood incubation systems for in vitro hemocompatibility assessment of planar solid surface. J. Biomed. Mater. Res. B 2003, 66, 379–390. [Google Scholar]
- Nomura, S.; Shouzu, A.; Tamoto, K.; Togane, Y.; Goto, S.; Uchiyama, S.; Ikeda, Y. Assessment of an ELISA kit for platelet-derived microparticles by joint research at many institutes in Japan. J. Atheroscer. Thromb. 2009, 16, 878–887. [Google Scholar]
© 2012 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/3.0/).
Share and Cite
Lackner, J.M.; Waldhauser, W.; Hartmann, P.; Bruckert, F.; Weidenhaupt, M.; Major, R.; Sanak, M.; Wiesinger, M.; Heim, D. Hemocompatibility of Inorganic Physical Vapor Deposition (PVD) Coatings on Thermoplastic Polyurethane Polymers. J. Funct. Biomater. 2012, 3, 283-297. https://doi.org/10.3390/jfb3020283
Lackner JM, Waldhauser W, Hartmann P, Bruckert F, Weidenhaupt M, Major R, Sanak M, Wiesinger M, Heim D. Hemocompatibility of Inorganic Physical Vapor Deposition (PVD) Coatings on Thermoplastic Polyurethane Polymers. Journal of Functional Biomaterials. 2012; 3(2):283-297. https://doi.org/10.3390/jfb3020283
Chicago/Turabian StyleLackner, Juergen M., Wolfgang Waldhauser, Paul Hartmann, Franz Bruckert, Marianne Weidenhaupt, Roman Major, Marek Sanak, Martin Wiesinger, and Daniel Heim. 2012. "Hemocompatibility of Inorganic Physical Vapor Deposition (PVD) Coatings on Thermoplastic Polyurethane Polymers" Journal of Functional Biomaterials 3, no. 2: 283-297. https://doi.org/10.3390/jfb3020283