A Novel Organo-Selenium Bandage that Inhibits Biofilm Development in a Wound by Gram-Positive and Gram-Negative Wound Pathogens

Abstract
:
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
1. Introduction
2. Results and Discussion
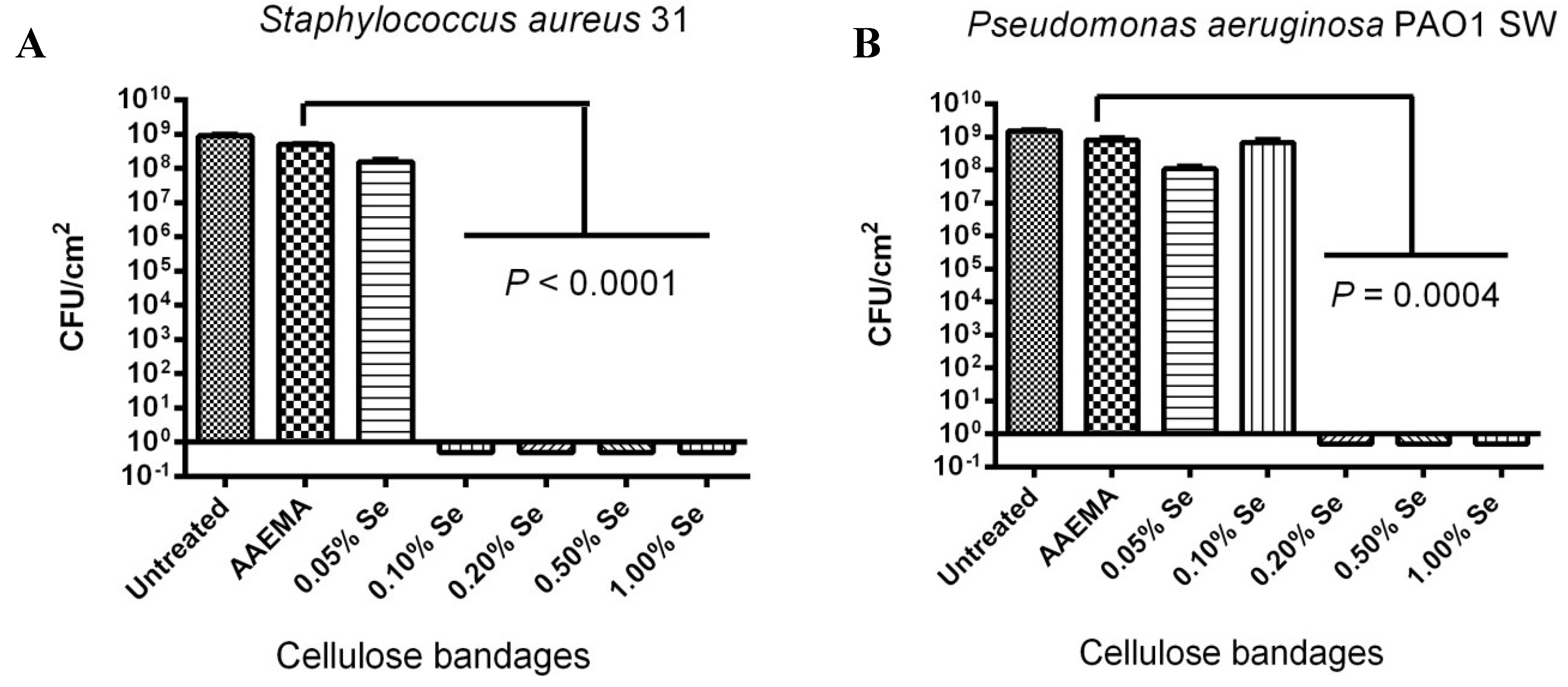
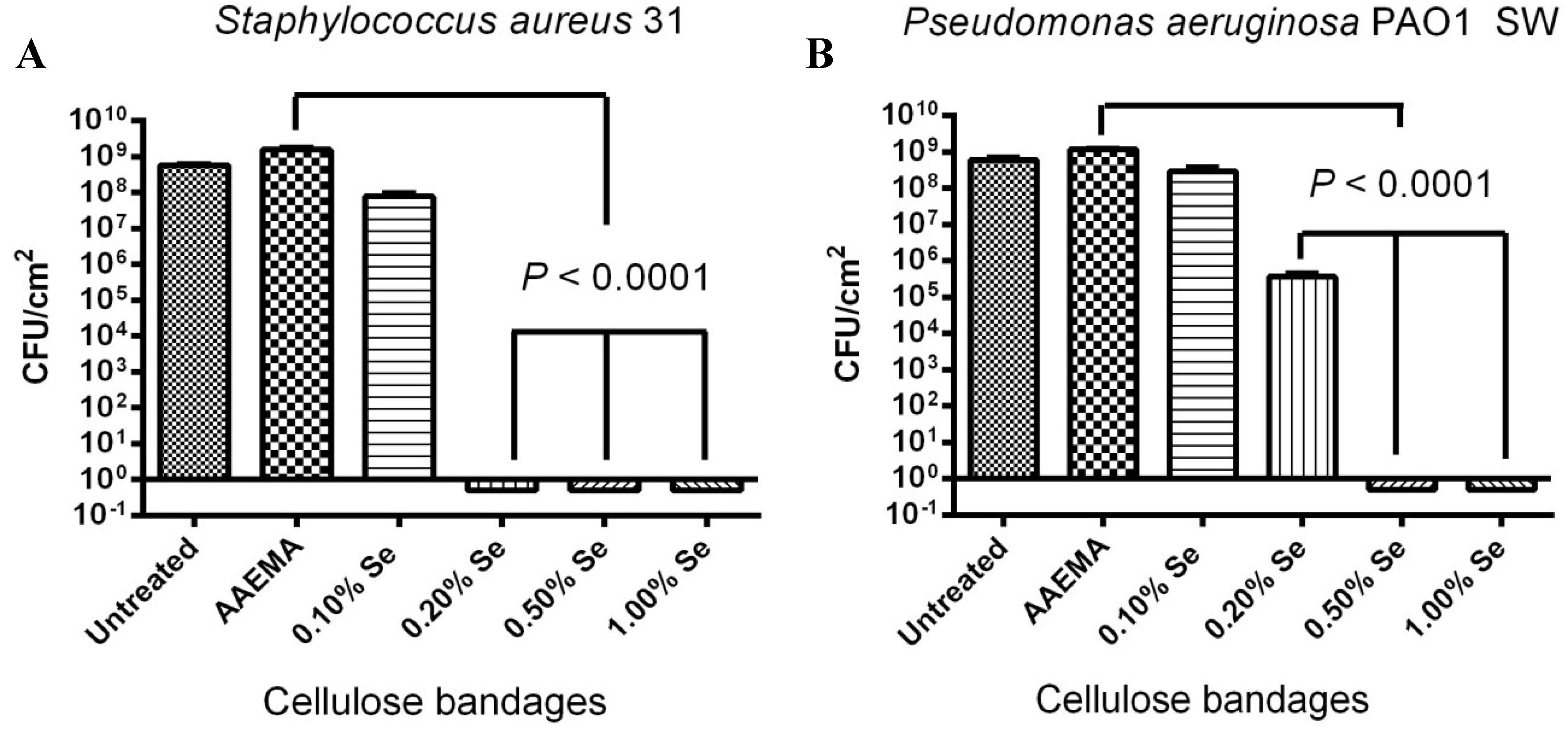
2.1. Organo-Selenium Bandage, Coated with Different Organo-Selenium Concentrations, was Tested for Its Ability to Block Biofilm Formation in Vitro for Laboratory Strains of Staphylococcus aureus and Pseudomonas aeruginosa

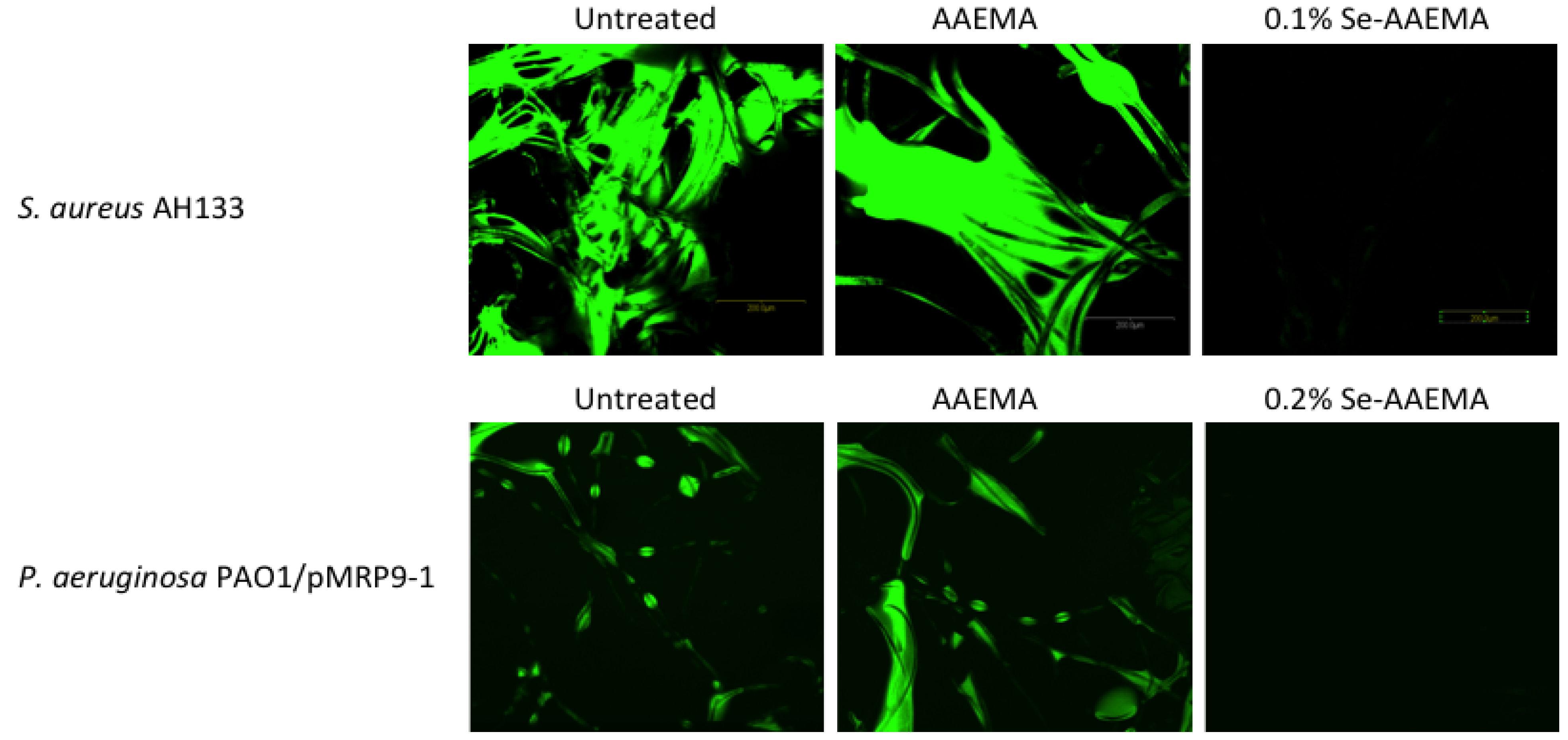
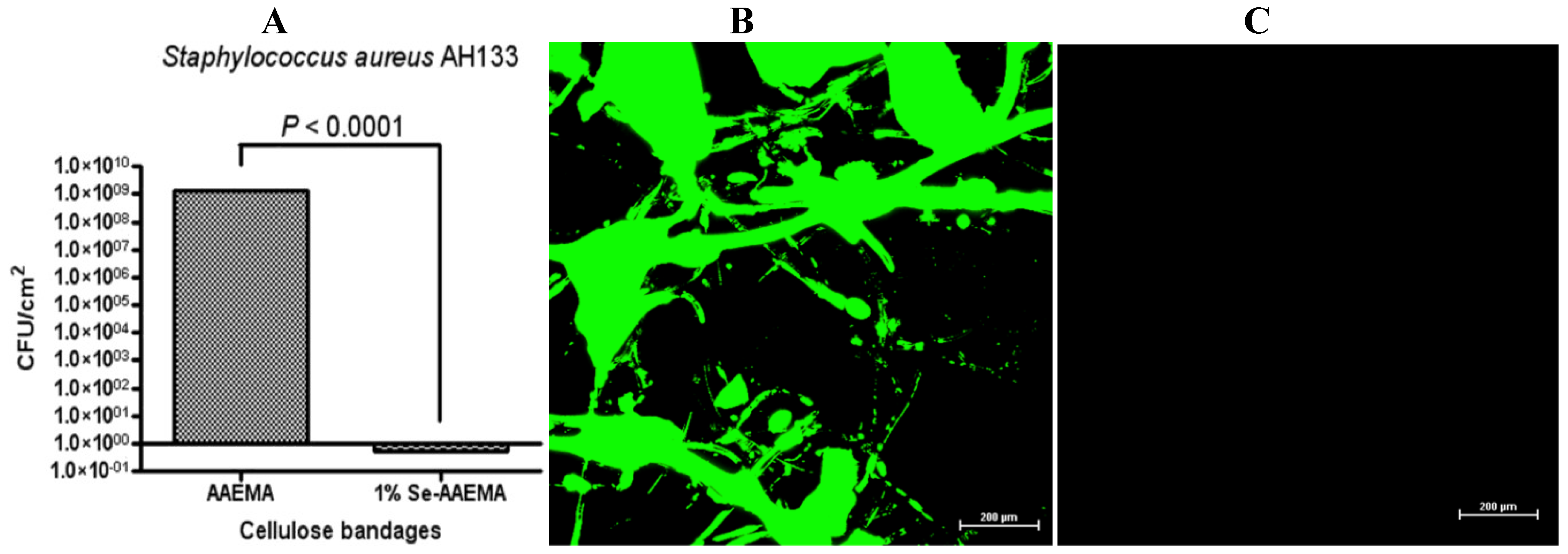
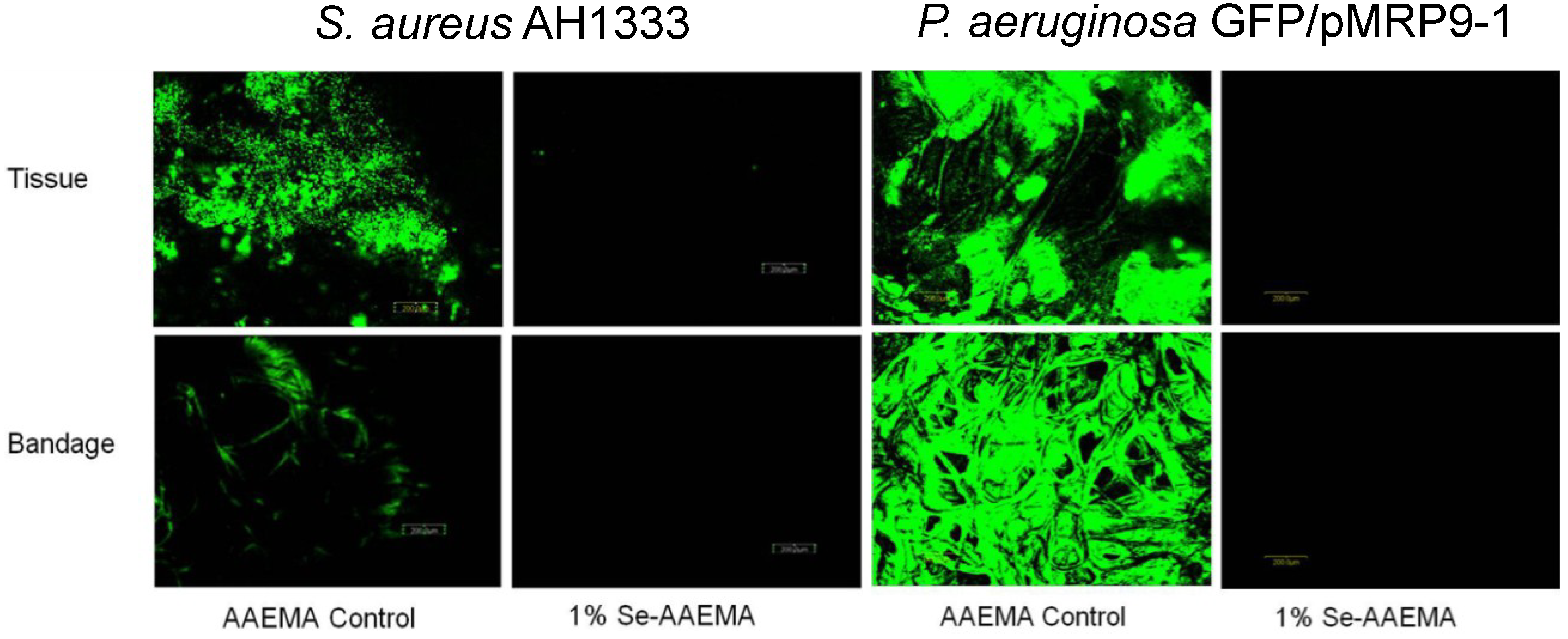
2.2. Confocal Visualization of the Biofilm Inhibition on a Bandage by Organo-Selenium in Vitro

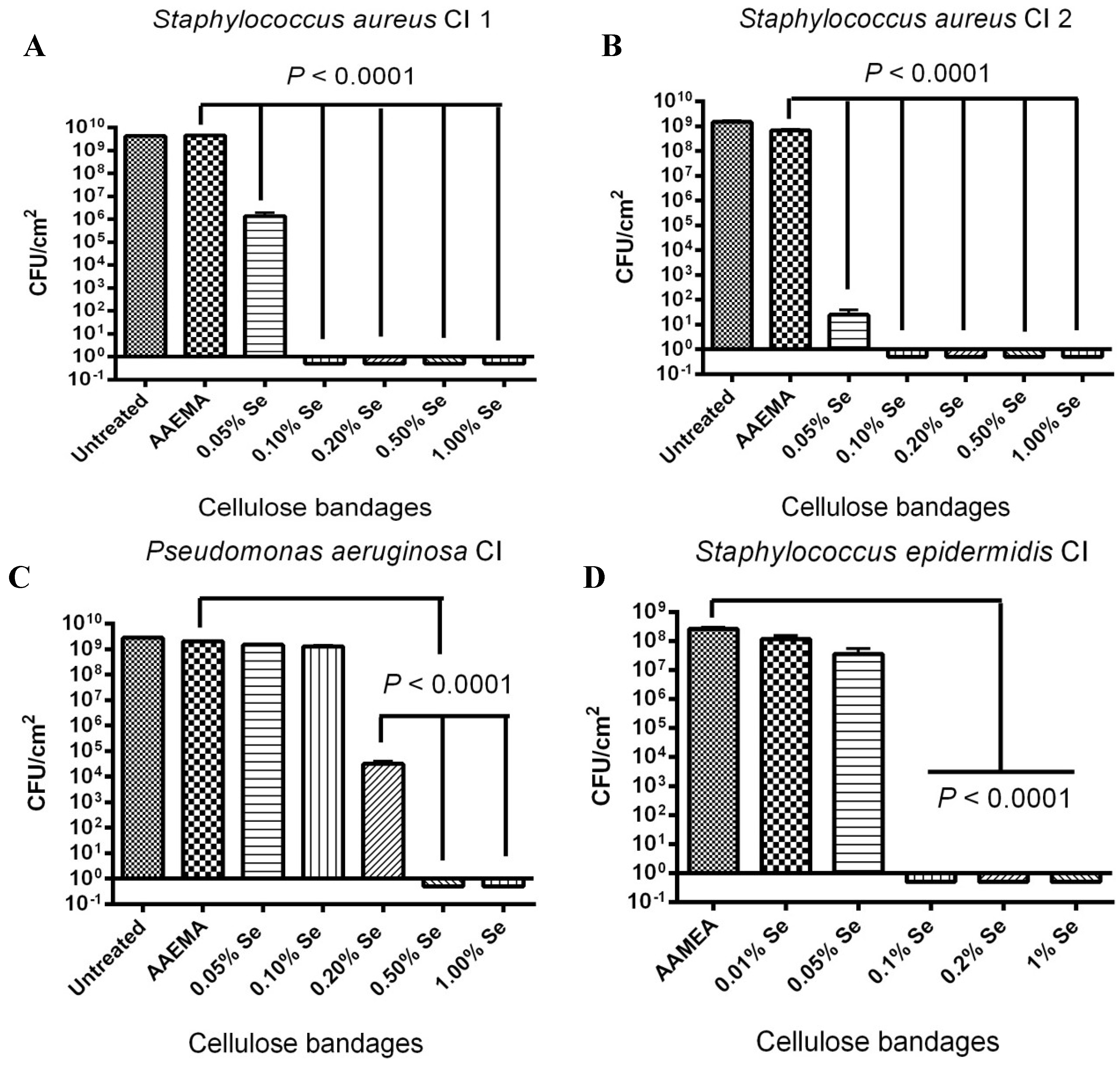
2.3. Selenium Bandage Inhibition of Clinical Isolates of S. aureus, P. aeruginosa and S. epidermidis

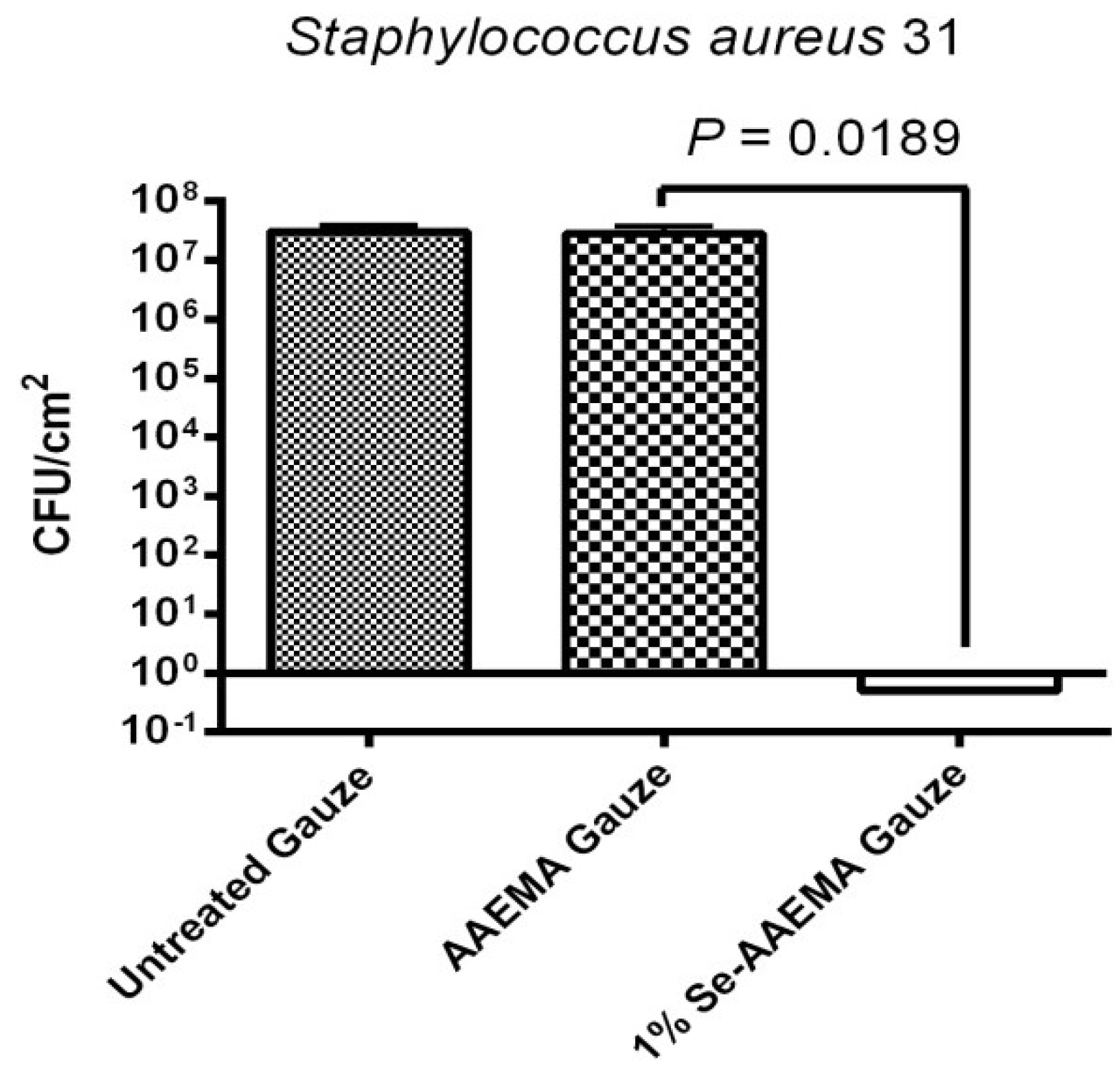
2.4. Stability of the Selenium Bandage in Preventing Biofilm Formation


2.5. Stability of the Organo-Selenium Bandage to Boiling Water

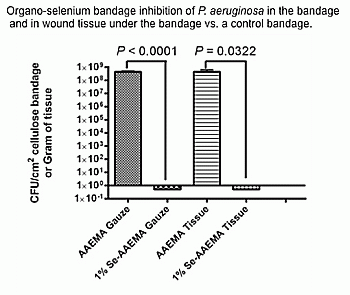
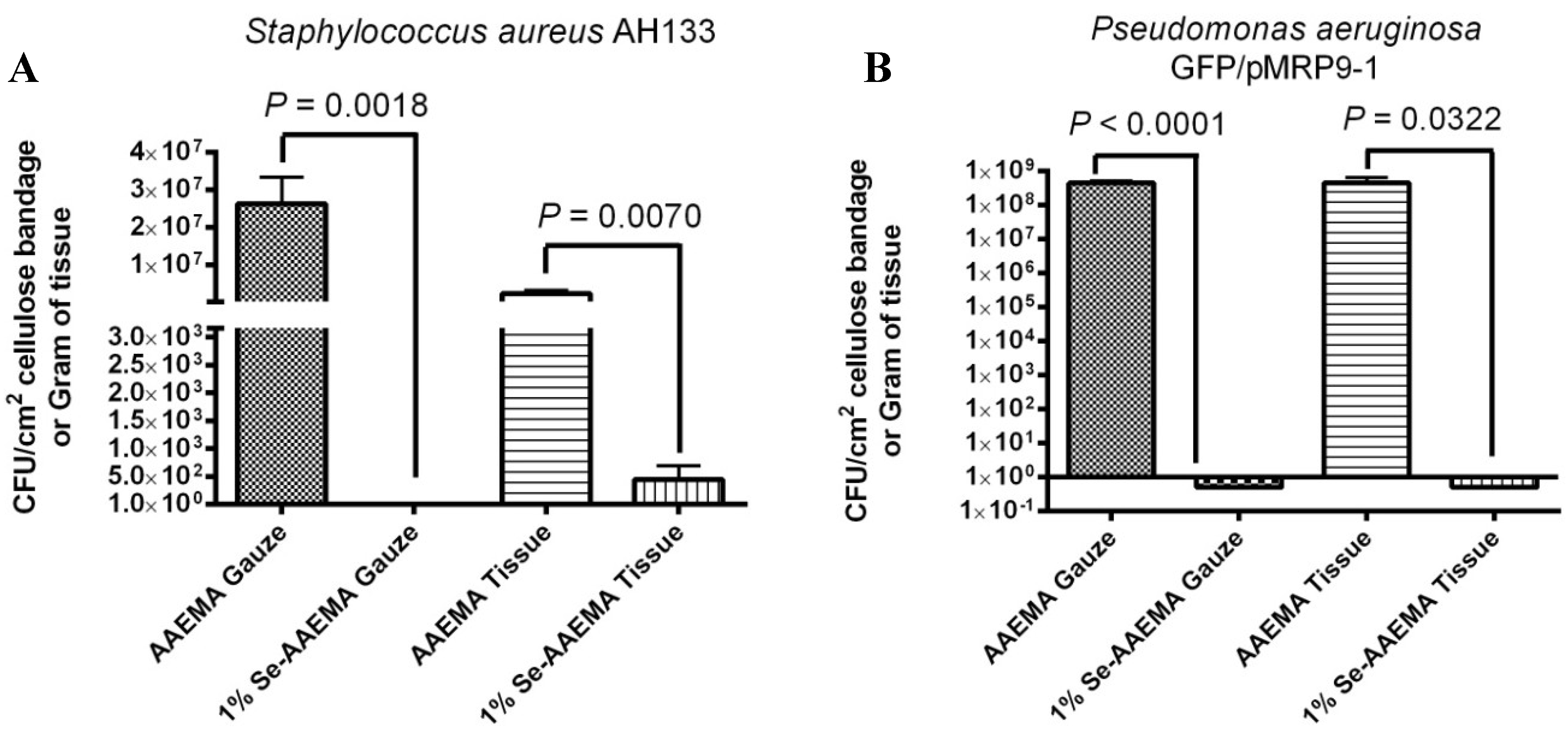
2.6. In Vivo Study of the Ability of a 1% Selenium Coated Bandage to Inhibit Biofilm in Both the Bandage and the Underlying Wound


2.7. Mammalian Cell Toxicity Assay
3. Experimental
3.1. Coating Cellulose Gauze with Polymerized Se-AAEMA
3.2. Bacterial Strains
3.3. Colony-Forming Unit Assays—in Vitro
3.4. Mouse Wound Infection Model
3.5. Biofilm Analysis by Fluorescence Microscopy
3.6. Analysis of the Long-term Stability of the Organo-Selenium-Containing Gauze Bandage
3.7. Accessing the Stability of the Organo-Selenium-Containing Gauze Bandage at Elevated Temperature
3.8. Analysis of Selenium Toxicity to Mammalian Cells
3.9. Statistical Analysis
4. Conclusions
Author Contributions
Conflicts of Interest
References
- Lipsky, B.A.; Berendt, A.R.; Deery, H.G.; Embil, J.M.; Joseph, W.S.; Karchmer, A.W.; Lefrock, J.L.; Lew, D.P.; Mader, J.T.; Norden, C.; et al. Diagnosis and treatment of diabetic foot infections. Clin. Infect. Dis. 2004, 39, 885–910. [Google Scholar] [CrossRef]
- Markogiannakis, H.; Pachylaki, N.; Samara, E.; Kalderi, M.; Minettou, M.; Toutouza, M.; Toutouzas, K.G.; Theodorou, D.; Katsaragakis, S. Infections in a surgical intensive care unit of a university hospital in Greece. Int. J. Infect. Dis. 2009, 13, 145–153. [Google Scholar] [CrossRef]
- McCaig, L.F.; McDonald, L.C.; Mandal, S.; Jernigan, D.B. Staphylococcus aureus-associated skin and soft tissue infections in ambulatory care. Emerg. Infect. Dis. 2006, 12, 1715–1723. [Google Scholar] [CrossRef]
- Murray, C.K. Infectious disease complications of combat-related injuries. Crit. Care Med. 2008, 36, S358–S364. [Google Scholar] [CrossRef]
- Church, D.; Elsayed, S.; Reid, O.; Winston, B.; Lindsay, R. Burn wound infections. Clin. Microbiol. Rev. 2006, 19, 403–434. [Google Scholar] [CrossRef]
- Schaber, J.A.; Triffo, W.J.; Suh, S.J.; Oliver, J.W.; Hastert, M.C.; Griswold, J.A.; Auer, M.; Hamood, A.N.; Rumbaugh, K.P. Pseudomonas aeruginosa forms biofilms in acute infection independent of cell-to-cell signaling. Infect. Immun. 2007, 75, 3715–3721. [Google Scholar] [CrossRef]
- Trafny, E.A. Susceptibility of adherent organisms from Pseudomonas aeruginosa and Staphylococcus aureus strains isolated from burn wounds to antimicrobial agents. Int. J. Antimicrob. Agents 1998, 10, 223–228. [Google Scholar] [CrossRef]
- Donlan, R.M.; Costerton, J.W. Biofilms: Survival mechanisms of clinically relevant microorganisms. Clin. Microbiol. Rev. 2002, 15, 167–193. [Google Scholar] [CrossRef]
- Sauer, K.; Camper, A.K.; Ehrlich, G.D.; Costerton, J.W.; Davies, D.G. Pseudomonas aeruginosa displays multiple phenotypes during development as a biofilm. J. Bacteriol. 2002, 184, 1140–1154. [Google Scholar] [CrossRef]
- Holder, I.A.; Durkee, P.; Supp, A.P.; Boyce, S.T. Assessment of a silver-coated barrier dressing for potential use with skin grafts on excised burns. Burns 2003, 29, 445–448. [Google Scholar] [CrossRef]
- Kuroyanagi, Y.; Shiraishi, A.; Shirasaki, Y.; Nakakita, N.; Yasutomi, Y.; Takano, Y.; Shioya, N. Development of a new wound dressing with antimicrobial delivery capability. Wound Repair Regen. 1994, 2, 122–129. [Google Scholar]
- Lin, S.S.; Ueng, S.W.; Lee, S.S.; Chan, E.C.; Chen, K.T.; Yang, C.Y.; Chen, C.Y.; Chan, Y.S. In vitro elution of antibiotic from antibiotic-impregnated biodegradable calcium alginate wound dressing. J. Trauma 1999, 47, 136–141. [Google Scholar] [CrossRef]
- Ong, S.Y.; Wu, J.; Moochhala, S.M.; Tan, M.-H.; Lu, J. Development of a chitosan-based wound dressing with improved hemostatic and antimicrobial properties. Biomaterials 2008, 29, 4323–4332. [Google Scholar] [CrossRef]
- Hidalgo, E.; Bartolomé, R.; Barroso, C.; Moreno, A.; Domínguez, C. Silver nitrate: Antimicrobial activity related to cytotoxicity in cultured human fibroblasts. Skin Pharmacol. Appl. Skin Physiol. 1998, 11, 140–151. [Google Scholar] [CrossRef]
- Lee, A.R.; Moon, H.K. Effect of topically applied silver sulfadiazine on fibroblast cell proliferation and biomechanical properties of the wound. Arch. Pharm. Res. 2003, 26, 855–860. [Google Scholar] [CrossRef]
- Ip, M.; Lui, S.L.; Poon, V.K.M.; Lung, I.; Burd, A. Antimicrobial activities of silver dressings: An in vitro comparison. J. Med. Microbiol. 2006, 55, 59–63. [Google Scholar] [CrossRef]
- Mathews, S.M.; Spallholz, J.E.; Grimson, M.J.; Dubielzig, R.R.; Gray, T.; Reid, T.W. Prevention of bacterial colonization of contact lenses with covalently attached selenium and effects on the rabbit cornea. Cornea 2006, 25, 806–814. [Google Scholar] [CrossRef]
- Tran, P.L.; Hammond, A.A.; Mosley, T.; Cortez, J.; Gray, T.; Colmer-Hamood, J.A.; Shashtri, M.; Spallholz, J.E.; Hamood, A.N.; Reid, T.W. Organoselenium coating on cellulose inhibits the formation of biofilms by Pseudomonas aeruginosa and Staphylococcus aureus. Appl. Environ. Microbiol. 2009, 75, 3586–3592. [Google Scholar] [CrossRef]
- Tran, P.L.; Lowry, N.; Campbell, T.; Reid, T.W.; Webster, D.R.; Tobin, E.; Aslani, A.; Mosley, T.; Dertien, J.; Colmer-Hamood, J.A.; et al. An organoselenium compound inhibits Staphylococcus aureus biofilms on hemodialysis catheters in vivo. Antimicrob. Agents Chemother. 2012, 56, 972–978. [Google Scholar] [CrossRef]
- Tran, P.; Hamood, A.; Mosley, T.; Gray, T.; Jarvis, C.; Webster, D.; Amaechi, B.; Enos, T.; Reid, T. Organo-selenium-containing dental sealant inhibits bacterial biofilm. J. Dent. Res. 2013, 92, 461–466. [Google Scholar] [CrossRef]
- Wang, J.C.; Tran, P.L.; Hanes, R.; Cordero, J.; Marchbanks, J.; Reid, T.W.; Colmer-Hamood, J.A.; Hamood, A.N. Inhibition of otopathogenic biofilms by organoselenium-coated tympanostomy tubes. JAMA Otolaryngol. Head Neck Surg. 2013, 139, 1009–1016. [Google Scholar] [CrossRef]
- Chaudiere, J.; Courtin, O.; Leclaire, J. Glutathione oxidase activity of selenocystamine: A mechanistic study. Arch. Biochem. Biophys. 1992, 296, 328–336. [Google Scholar] [CrossRef]
- Feigl, F.; West, P.W. Test for selenium based on catalytic effect. Anal. Chem. 1947, 19, 351–353. [Google Scholar] [CrossRef]
- Seko, Y.; Imura, N. Active oxygen generation as a possible mechanism of selenium toxicity. Biomed. Environ. Sci. 1997, 10, 333–339. [Google Scholar]
- Holloway, B.W.; Krishnapillai, V.; Morgan, A.F. Chromosomal genetics of Pseudomonas. Microbiol. Rev. 1979, 43, 73–102. [Google Scholar]
- Malone, C.L.; Boles, B.R.; Lauderdale, K.J.; Thoendel, M.; Kavanaugh, J.S.; Horswill, A.R. Fluorescent reporters for Staphylococcus aureus. J. Microbiol. Methods 2009, 77, 251–260. [Google Scholar] [CrossRef]
© 2014 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/3.0/).
Share and Cite
Tran, P.L.; Patel, S.; Hamood, A.N.; Enos, T.; Mosley, T.; Jarvis, C.; Desai, A.; Lin, P.; Reid, T.W. A Novel Organo-Selenium Bandage that Inhibits Biofilm Development in a Wound by Gram-Positive and Gram-Negative Wound Pathogens. Antibiotics 2014, 3, 435-449. https://doi.org/10.3390/antibiotics3030435
Tran PL, Patel S, Hamood AN, Enos T, Mosley T, Jarvis C, Desai A, Lin P, Reid TW. A Novel Organo-Selenium Bandage that Inhibits Biofilm Development in a Wound by Gram-Positive and Gram-Negative Wound Pathogens. Antibiotics. 2014; 3(3):435-449. https://doi.org/10.3390/antibiotics3030435
Chicago/Turabian StyleTran, Phat L., Saurabh Patel, Abdul N. Hamood, Tyler Enos, Thomas Mosley, Courtney Jarvis, Akash Desai, Pamela Lin, and Ted W. Reid. 2014. "A Novel Organo-Selenium Bandage that Inhibits Biofilm Development in a Wound by Gram-Positive and Gram-Negative Wound Pathogens" Antibiotics 3, no. 3: 435-449. https://doi.org/10.3390/antibiotics3030435