Elevated Circulating TNF-α in Fat-Free Mass Non-Responders Compared to Responders Following Exercise Training in Older Women

Abstract
:1. Introduction
2. Experimental Section
2.1. Subjects

{kind=link}
| Responders (n = 30) | Non-Responders (n = 20) | G | T | G*T | |||
|---|---|---|---|---|---|---|---|
| Pre | Post | Pre | Post | p | p | p | |
| Age (years) | 64.8 ± 3.6 | 65.2 ± 3.6 | 64.6 ± 3.2 | 65.1 ± 3.2 | 0.879 | 0.001 | 0.368 |
| Weight (kg) | 72.1 ± 9.7 | 71.8 ± 9.7 | 75.1 ± 14.1 | 73.5 ± 11.6 | 0.468 | 0.025 | 0.112 |
| BMI (kg/m2) | 26.8 ± 3.9 | 26.6 ± 4.1 | 27.9 ± 3.3 | 27.4 ± 3.7 | 0.398 | 0.011 | 0.154 |
| %fat | 43.1 ± 5.7 | 40.9 ± 5.9 | 41.5 ± 7 | 42.4 ± 5.9 | 0.974 | 0.013 | 0.001 |
| Fat Mass (kg) | 31.1 ± 7.9 | 29.7 ± 8.0 | 32.4 ± 12.2 | 32.0 ± 9.5 | 0.493 | 0.045 | 0.240 |
| Fat-Free Mass (kg) | 40.9 ± 3.6 | 42.2 ± 3.6 | 42.7 ± 3.5 | 41.5 ± 3.2 | 0.610 | 0.827 | 0.001 |
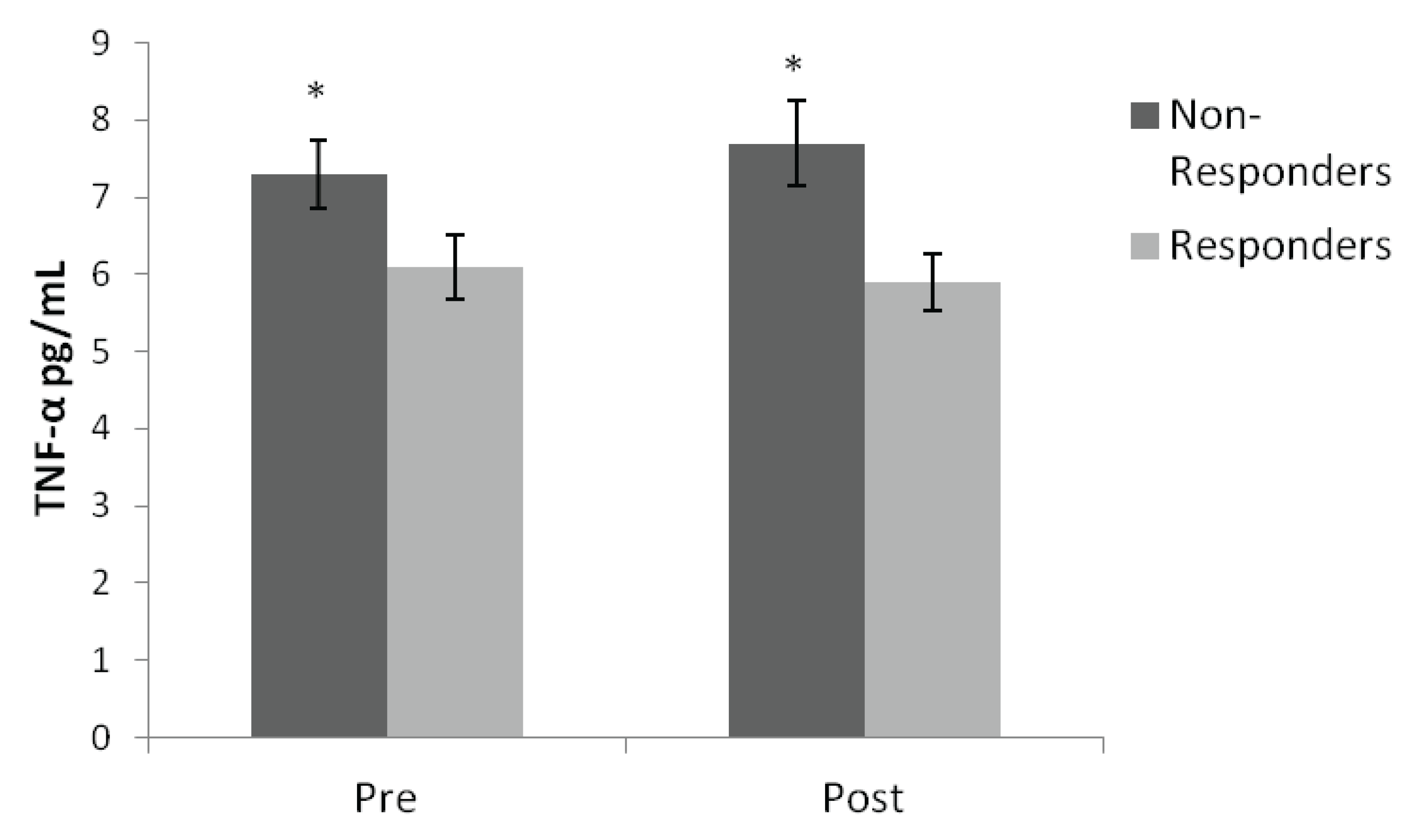
| TNF-α (pg/mL) | 6.1 ± 2.3 | 5.9 ± 2.1 | 7.3 ± 1.9 | 7.5 ± 2.3 | 0.022 | 0.718 | 0.239 |
| IL-6 (pg/mL) | 1.9 ± 0.91 | 1.6 ± 0.70 | 2.0 ± 2.3 | 2.2 ± 2.8 | 0.477 | 0.758 | 0.074 |
| CRP (mg/L) | 3.2 ± 3.7 | 2.8 ± 2.9 | 2.6 ± 2.1 | 2.8 ± 2.7 | 0.715 | 0.772 | 0.344 |
| Chest Press (kg) | 23.6 ± 6.4 | 27.1 ± 8.1 | 22 ± 3.9 | 27.4 ± 6.2 | 0.688 | 0.001 | 0.226 |
| Shoulder Press (kg) | 23.8 ± 4.9 | 26.2 ± 5.4 | 23.4 ± 3.9 | 26.9 ± 4.4 | 0.868 | 0.001 | 0.177 |
| Leg Press (kg) | 87.9 ± 26.1 | 110.7 ± 34.5 | 90.7 ± 16.3 | 111.8 ± 21.2 | 0.790 | 0.001 | 0.726 |
| Knee Extension (kg) | 30.6 ± 8.9 | 38.1 ± 10 | 30.9 ± 6.3 | 35.8 ± 6.4 | 0.670 | 0.001 | 0.114 |
| VO2max (mL/kg/min) | 23.4 ± 4.6 | 23.9 ± 4.9 | 21.8 ± 4.8 | 22.7 ± 4.6 | 0.379 | 0.172 | 0.665 |
2.2. Study Design
2.3. Strength Testing
2.4. Aerobic Capacity Testing
2.5. Resistance and Aerobic Training Program
2.6. Laboratory Analyses
2.7. Body Composition Measurements
2.8. Statistical Analysis
3. Results

4. Discussion and Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Hunter, G.R.; McCarthy, J.P.; Bamman, M.M. Effects of resistance training on older adults. Sports Med. 2004, 34, 329–348. [Google Scholar] [CrossRef]
- Häkkinen, K.; Kallinen, M.; Izquierdo, M.; Jokelainen, K.; Lassila, H.; Mälkiä, E.; Kraemer, W.J.; Newton, R.U.; Alen, M. Changes in agonist-antagonist emg, muscle csa, and force during strength training in middle-aged and older people. J. Appl. Physiol. 1998, 84, 1341–1349. [Google Scholar]
- Frontera, W.R.; Meredith, C.N.; O’Reilly, K.P.; Knuttgen, H.G.; Evans, W.J. Strength conditioning in older men: Skeletal muscle hypertrophy and improved function. J. Appl. Physiol. 1988, 64, 1038–1044. [Google Scholar]
- Dudley, G.; Djamil, R. Incompatibility of endurance- and strength-training modes of exercise. J. Appl. Physiol. 1985, 59, 1446–1451. [Google Scholar]
- Hickson, R.; Rosenkoetter, M.; Brown, M. Strength training effects on aerobic power and short-term endurance. Med. Sci. Sports Exerc. 1980, 12, 336–339. [Google Scholar]
- Hunter, G.; Demment, R.; Miller, D. Development of strength and maximum oxygen uptake during simultaneous training for strength and endurance. J. Sports Med. Phys. Fit. 1987, 27, 269–275. [Google Scholar]
- Wood, R.; Reyes, R.; Welsch, M.; Favaloro-Sabatier, J.; Sabatier, M.; Matthew Lee, C.; Johnson, L.; Hooper, P. Concurrent cardiovascular and resistance training in healthy older adults. Med. Sci. Sports Exerc. 2001, 33, 1751–1758. [Google Scholar] [CrossRef]
- Izquierdo, M.; Häkkinen, K.; Ibáñez, J.; Kraemer, W.; Gorostiaga, E. Effects of combined resistance and cardiovascular training on strength, power, muscle cross-sectional area, and endurance markers in middle-aged men. Eur. J. Appl. Physiol. 2005, 94, 70–75. [Google Scholar] [CrossRef]
- Holviala, J.; Häkkinen, A.; Karavirta, L.; Nyman, K.; Izquierdo, M.; Gorostiaga, E.; Avela, J.; Korhonen, J.; Knuutila, V.; Kraemer, W.; et al. Effects of combined strength and endurance training on treadmill load carrying walking performance in aging men. J. Strength Cond. Res. 2010, 24, 1584–1595. [Google Scholar] [CrossRef]
- Fisher, G.; McCarthy, J.P.; Zuckerman, P.A.; Bryan, D.R.; Bickel, C.S.; Hunter, G.R. Frequency of combined resistance and aerobic training in older women. J. Strength Cond. Res. 2012, 27, 1868–1876. [Google Scholar]
- Hubal, M.J.; Gordish-Dressman, H.; Thompson, P.D.; Price, T.B.; Hoffman, E.P.; Angelopoulos, T.J.; Gordon, P.M.; Moyna, N.M.; Pescatello, L.S.; Visich, P.S.; et al. Variability in muscle size and strength gain after unilateral resistance training. Med. Sci. Sports Exerc. 2005, 37, 964–972. [Google Scholar]
- Davidsen, P.K.; Gallagher, I.J.; Hartman, J.W.; Tarnopolsky, M.A.; Dela, F.; Helge, J.W.; Timmons, J.A.; Phillips, S.M. High responders to resistance exercise training demonstrate differential regulation of skeletal muscle microrna expression. J. Appl. Physiol. 2011, 110, 309–317. [Google Scholar]
- Karavirta, L.; Häkkinen, K.; Kauhanen, A.; Arija-Blázquez, A.; Sillanpää, E.; Rinkinen, N.; Häkkinen, A. Individual responses to combined endurance and strength training in older adults. Med. Sci. Sports Exerc. 2011, 43, 484–490. [Google Scholar]
- Izquierdo, M.; Ibañez, J.; HAkkinen, K.; Kraemer, W.J.; Larrión, J.L.; Gorostiaga, E.M. Once weekly combined resistance and cardiovascular training in healthy older men. Med. Sci. Sports Exerc. 2004, 36, 435–443. [Google Scholar]
- Bamman, M.M.; Petrella, J.K.; Kim, J.S.; Mayhew, D.L.; Cross, J.M. Cluster analysis tests the importance of myogenic gene expression during myofiber hypertrophy in humans. J. Appl. Physiol. 2007, 102, 2232–2239. [Google Scholar]
- Taaffe, D.R.; Harris, T.B.; Ferrucci, L.; Rowe, J.; Seeman, T.E. Cross-sectional and prospective relationships of interleukin-6 and c-reactive protein with physical performance in elderly persons: Macarthur studies of successful aging. J. Gerontol. A Biol. Sci. Med. Sci. 2000, 55, M709–M715. [Google Scholar]
- Visser, M.; Pahor, M.; Taaffe, D.R.; Goodpaster, B.H.; Simonsick, E.M.; Newman, A.B.; Nevitt, M.; Harris, T.B. Relationship of interleukin-6 and tumor necrosis factor-alpha with muscle mass and muscle strength in elderly men and women: The health abc study. J. Gerontol. A Biol. Sci. Med. Sci. 2002, 57, M326–M332. [Google Scholar] [CrossRef]
- Goodman, M.N. Tumor necrosis factor induces skeletal muscle protein breakdown in rats. Am. J. Physiol. 1991, 260, E727–E730. [Google Scholar]
- Bruunsgaard, H.; Bjerregaard, E.; Schroll, M.; Pedersen, B.K. Muscle strength after resistance training is inversely correlated with baseline levels of soluble tumor necrosis factor receptors in the oldest old. J. Am. Geriatr. Soc. 2004, 52, 237–241. [Google Scholar] [CrossRef]
- Kalb, J.S.; Hunter, G.R. Weight training economy as a function of intensity of the squat and overhead press exercise. J. Sports Med. Phys. Fit. 1991, 31, 154–160. [Google Scholar]
- Degens, H. Age-related skeletal muscle dysfunction: Causes and mechanisms. J. Musculoskelet. Neuronal Interact. 2007, 7, 246–252. [Google Scholar]
- Fisher, G.; Hyatt, T.C.; Hunter, G.R.; Oster, R.A.; Desmond, R.A.; Gower, B.A. Effect of diet with and without exercise training on markers of inflammation and fat distribution in overweight women. Obesity (Silver Spring) 2011, 19, 1131–1136. [Google Scholar]
- Nicklas, B.; Ambrosius, W.; Messier, S.; Miller, G.; Penninx, B.; Loeser, R.; Palla, S.; Bleecker, E.; Pahor, M. Diet-induced weight loss, exercise, and chronic inflammation in older, obese adults: A randomized controlled clinical trial. Am. J. Clin. Nutr. 2004, 79, 544–551. [Google Scholar]
- Mavros, Y.; Kay, S.; Simpson, K.A.; Baker, M.K.; Wang, Y.; Zhao, R.R.; Meiklejohn, J.; Climstein, M.; O’Sullivan, A.J.; de Vos, N.; et al. Reductions in c-reactive protein in older adults with type 2 diabetes are related to improvements in body composition following a randomized controlled trial of resistance training. J. Cachexia Sarcopenia Muscle 2014, 5, 111–120. [Google Scholar]
- Degens, H. The role of systemic inflammation in age-related muscle weakness and wasting. Scand. J. Med. Sci. Sports 2010, 20, 28–38. [Google Scholar] [CrossRef]
- Chen, S.E.; Jin, B.; Li, Y.P. Tnf-alpha regulates myogenesis and muscle regeneration by activating p38 mapk. Am. J. Physiol. Cell Physiol. 2007, 292, C1660–C1671. [Google Scholar] [CrossRef]
- Pedersen, B.K.; Febbraio, M.A. Muscles, exercise and obesity: Skeletal muscle as a secretory organ. Nat. Rev. Endocrinol. 2012, 8, 457–465. [Google Scholar] [CrossRef]
© 2014 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/3.0/).
Share and Cite
Fisher, G.; Bickel, C.S.; Hunter, G.R. Elevated Circulating TNF-α in Fat-Free Mass Non-Responders Compared to Responders Following Exercise Training in Older Women. Biology 2014, 3, 551-559. https://doi.org/10.3390/biology3030551
Fisher G, Bickel CS, Hunter GR. Elevated Circulating TNF-α in Fat-Free Mass Non-Responders Compared to Responders Following Exercise Training in Older Women. Biology. 2014; 3(3):551-559. https://doi.org/10.3390/biology3030551
Chicago/Turabian StyleFisher, Gordon, C. Scott Bickel, and Gary R. Hunter. 2014. "Elevated Circulating TNF-α in Fat-Free Mass Non-Responders Compared to Responders Following Exercise Training in Older Women" Biology 3, no. 3: 551-559. https://doi.org/10.3390/biology3030551