1. Introduction
Nephron sparing surgery (NSS) has been advocated as the surgical treatment of choice for the management of small renal masses, secondarily improving renal function and long-term survival [
1]. Increasingly, robotic surgery has been utilized across many centers in the United States as the preferred NSS modality given the dexterity afforded by the robot and the ability of the surgeon to resect the mass and cover the renal defect. Particularly when tactile sensation is lost during robotic partial nephrectomy (RPN), the risk of incomplete tumor resection and positive margins can compromise cancer specific outcomes [
2]. Intraoperative renal ultrasonography has historically been utilized to identify complex or intraparenchymal lesions [
3], however the margin of masses may still be difficult to identify and may be cumbersome to use through a robotic assistant port.
The latest robotic surgery technology has attempted to circumvent these visual drawbacks, most commonly using near infrared fluorescence imaging, (
i.e., intravenous injection of indocyanine green (ICG) (
©Akorn, Incorporated, Lake Forest, IL, USA)) to delineate perfusion and uptake of normal renal parenchyma during RPN (
Figure 1) [
4]. ICG binds to plasma proteins, remaining in the vasculature and providing excellent delineation of the vascular system [
5]. Renal cortical tumors have reduced expression of bilitranslocase, a carrier protein for ICG in normal parenchyma proximal tubule cells, thus leading to a reduction in near infrared fluorescence imaging in these tumors and delineation from normal parenchyma [
6].
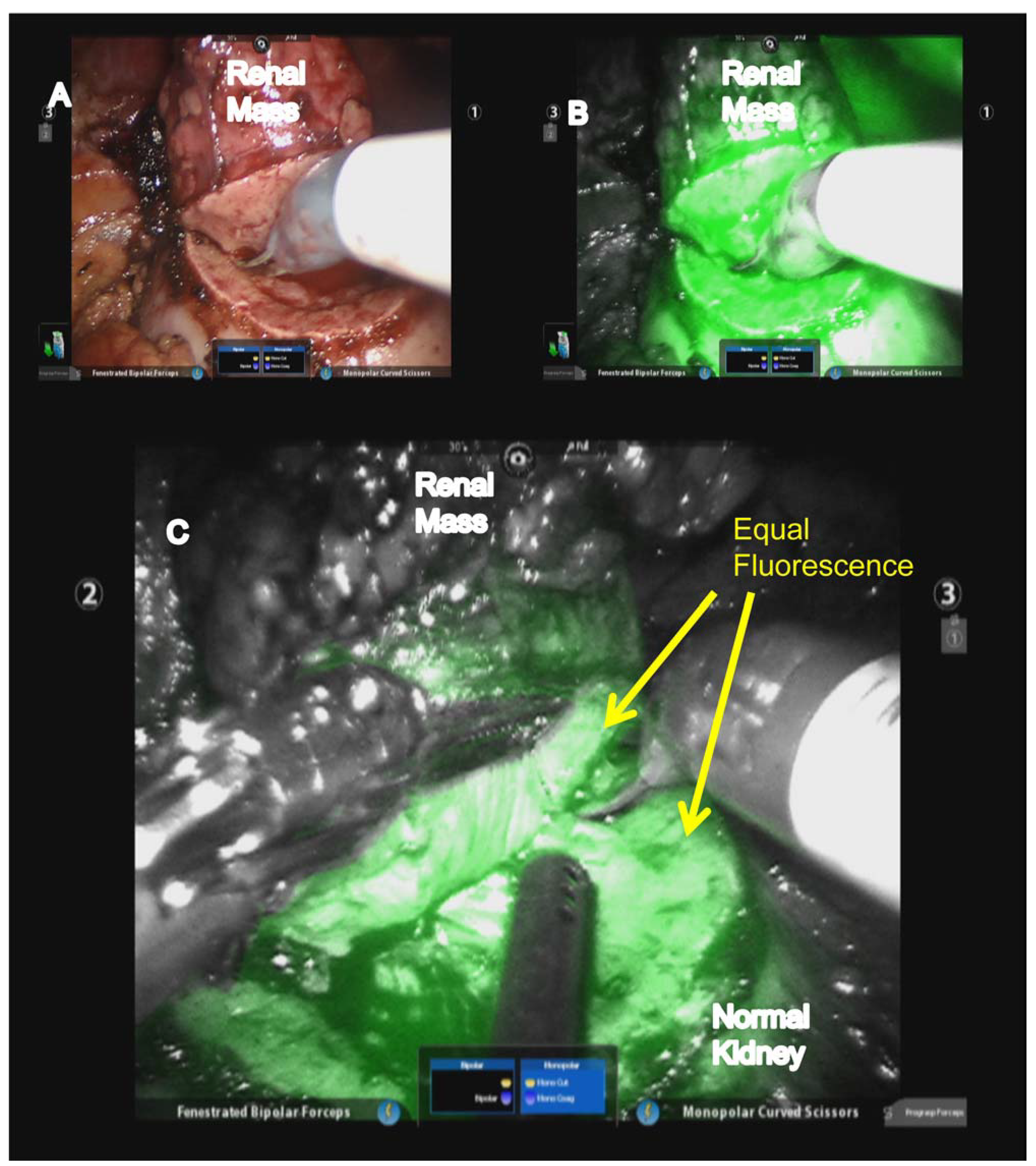
Figure 1.
Toggling between (A) white and (B) near infrared fluorescence (NIRF) to evaluate renal mass margins and (C) maintenance of equal fluorescence of normal renal parenchyma covering tumor and toward normal kidney. (Used with permission, Elsevier: Krane, L.S.; Manny, T.B.; Hemal, A.K. Urology 2012, 80, 110–118).
Figure 1.
Toggling between (A) white and (B) near infrared fluorescence (NIRF) to evaluate renal mass margins and (C) maintenance of equal fluorescence of normal renal parenchyma covering tumor and toward normal kidney. (Used with permission, Elsevier: Krane, L.S.; Manny, T.B.; Hemal, A.K. Urology 2012, 80, 110–118).
The purpose of this review is to analyze the current institutional experiences utilizing ICG during RPN, to address limitations and clinical situations when ICG may not be useful, and to highlight future directions of near infrared fluorescent imaging.
2. ICG RPN Institutional Studies
In 2011, Tobis
et al. [
4] were the first to publish their experience of ICG for RPN, having previously reported their success using ICG for open partial nephrectomy [
7]. In their series of 11 patients, nine patients successfully underwent RPN and two patients were converted to robotic radical nephrectomy secondary to an intraoperative identification of renal vein thrombus and dense perinephric inflammatory adhesions. Median warm ischemia time (WIT) was 19.3 min, estimated blood loss (EBL) was 100 cc, radiographic tumor size was 3.8 cm, nephrometry score was 7.5, and robotic surgical console time was 134 min. Their technique for injection of ICG included preparing 2.5 mg/mL at the beginning of the case and injecting as a bolus dose within six hours of preparation. Tobis
et al. used a total of 0.75 to 7.5 mg per injection based on the optimal tumor fluorescence, and injections were repeated as necessary to achieve adequate visualization taking care to remain below the recommended daily maximum dose of 2 mg/kg [
4]. Fluorescence was seen in the renal vasculature between 5 and 60 s following injection in all patients and renal parenchyma was seen to fluoresce in 1 min (maximal fluorescence lasting 10–15 min) from injection. The tumors demonstrated decreased or no fluorescence compared to the surrounding parenchyma in 8 patients and equivalent fluorescence in 3 patients. On final pathology, 10 of the 11 masses were malignant and there were no positive margins; median change in post-operative compared to preoperative creatinine was 0.1 mg/dL.
Following these initial positive results, Krane
et al. [
8] reported their experience in 47 consecutive patients undergoing ICG for RPN, who were compared to 47 consecutive previous patients undergoing RPN without ICG. Both groups had comparative demographic (age and comorbidities), preoperative (kidney function) and renal tumor anatomy (nephrometry score and tumor size). Intraoperatively, the ICG group had decreased WIT (15
vs. 17 min,
p = 0.03; only cases with hilar clamping included in calculating WIT) and more patients who underwent mass excision without hilar clamping (30%
vs. 10%,
p = 0.0002), however the ICG group had greater EBL (75
vs. 50 cc,
p = 0.023) although likely not clinically significant. Length of stay, incidence of malignancy, estimated glomerular filtration rate (eGFR) and positive margin rate were comparable between the two groups.
Recognizing that under dosing ICG causes inadequate fluorescence of peritumor parenchyma and overdosing causes inappropriate tumor fluorescence, Angell
et al. [
9] reported their experience of 79 patients utilizing a dosing strategy to determine the optimal ICG dose. Their dosing strategy consisted of giving a minimum of two ICG doses including a test dose prior to complete kidney exposure and a calibrated second dose prior to tumor resection. The test dose was based on patient weight and stature and was a median of 1.25 mg (range 0.625 to 2.5 mg) for the study. Based on tumor visualization of the test dose, the authors calibrated the second dose accordingly and reported a median second dose of 1.875 mg (range 0.625 to 5 mg). With this dosing regimen, differential fluorescence was achieved in 82% of tumors; after excluding five oncocytomas that fluoresced as expected, 88% of tumors exhibited the desired fluorescence.
Table 1 includes a complete summary of all institutional studies utilizing ICG for RPN.
Table 1.
Published institutional studies reporting outcomes of robotic partial nephrectomy (RPN) utilizing indocyanine green (ICG).
Table 1.
Published institutional studies reporting outcomes of robotic partial nephrectomy (RPN) utilizing indocyanine green (ICG).
| Study | Year | Institution | Patients (n) | Median Age (years) | Median Size (cm) | Median Operative Time (min) | Median WIT (min) | % Malignant | % Positive Margin |
|---|
| Tobis et al. [4] | 2011 | University of Rochester | 9 | 69 | 3.8 | 181 | 19 | 91 | 0 |
| Borofsky et al. [10] | 2012 | WFU, USC, NYU | 27 | 60 * | 2.8 * | 256 * | 0 | 81 | 0 |
| Krane et al. [8] | 2012 | WFU | 47 | 60 * | 2.7 | NR | 15 | 79 | 6.4 |
| Harke et al. [11] | 2013 | Missionsaerztliche, Klinik, Germany | 22 | 63 * | 3.8 * | 156 * | 12 | 50 | 0 |
| Bjurlin et al. [12] | 2013 | NYU | 48 | 54 | 2.6 | 155 | 17 | 75 | 3.8 |
| Angell et al. [9] | 2013 | Ohio State University | 79 | 55 * | 3.5 * | 187 * | 13 | 79 | 0 |
3. Limitations of ICG
Although ICG has improved the visualization of renal vasculature and exophytic cortical tumors, this has not resulted in improved positive margin rates [
8]. Perhaps this is secondary to an exophytic tumor being less likely to have a positive margin for experienced robotic surgeons. Furthermore, delineation of tumor margins for endophytic tumors has not improved with ICG [
8]. Tobis
et al. [
4] hypothesized that poor visualization with endophytic tumors may be secondary to the normal cap of parenchyma over the tumor. However, they reported that decreased fluorescence could be seen once resection commenced and suggested that tumor margin identification for endophytic tumors may be most useful once normal parenchyma has been incised.
In our practice, we have identified other limitations for the use of ICG in RPN. First, the lack of uptake in peripelvic/intrarenal fat and the collecting system itself may prevent the ICG delineation of the most medial/central extent of the tumor. Second, when toggling between white light and near infrared fluorescence imaging, the surrounding intracorporeal field is dark in relation to the ICG illuminated kidney. Presumably, this may increase the risk of iatrogenic injury to surrounding structures for the robotic surgeon. Third, we have found that the green color of ICG dye may “bleed” when excising the mass, making the margins less clear when cutting. Fourth, anecdotally in our experience, ICG is not helpful for reoperative surgery, particularly during recurrence after laparoscopic partial nephrectomy and cryoablation, secondary to the renal scar and associated post-inflammatory changes hypoperfusing similar to the tumor. Finally, the continued need for frozen sections to confirm negative margins in challenging cases has not been avoided by the introduction of ICG to RPN.
4. Future Directions
One of the most significant benefits of using ICG is to confirm that the region of potential excision is truly ischemic; there may be instances where a bulldog clamp is placed on the renal artery however ICG identifies an additional artery(ies). Furthermore, with the ability of ICG near infrared fluorescent imaging to delineate the vascular anatomy, attention has been focused on improving zero-ischemia and selective clamping using ICG. Borofsky
et al. [
10] reported their experience of super-selective arterial clamping during zero-ischemia RPN in 27 patients compared to 27 patients undergoing conventional clamping RPN. Between the two cohorts there were no differences in baseline patient or tumor characteristics. Operative outcomes were comparable between the two groups, however the conventional renal artery-clamping group had a shorter operative time (212
vs. 256 min,
p = 0.02). Post-operatively, the zero-ischemia group had superior kidney function compared to the conventional RPN group (reduction of estimated GFR −1.8%
vs. −14.9%,
p = 0.03). Both groups had comparable post-operative complication rates and all surgical margins were negative. Harke
et al. [
11] performed a single-surgeon matched-pair study of 22 patients who underwent selective clamping (tertiary vessels feeding the tumor) compared to 15 patients who underwent main renal artery clamping after administering ICG to both groups of patients. Between the groups there were no differences in demographic or perioperative data as well as post-operative complications. Short-term change in renal function was improved in the selective clamping group despite comparable baseline eGFR (6.2%
vs. 18.6%,
p = 0.045). These studies show that ICG-assisted vascular identification specific to the tumor may allow either off clamp or selective clamping of the arterial supply, demonstrating short-term post-operative improvement in renal function.
In an effort to assess whether ICG can predict malignancy in RPN patients, Manny
et al. [
13] reviewed the ICG fluorescence pattern in 100 patients undergoing RPN and correlated these findings to final tumor histology. The tumor fluorescent schema used included isofluorescent (the same amount as surrounding parenchyma), hypofluorescent (less than surrounding parenchyma, but with uptake), or afluorescent (no visible uptake of dye). Using a single intravenous dose of 5–7.5 mg of ICG before vascular clamping, 86 solid lesions were categorized as isofluorescent (
n = 3, two clear cell and one translocation tumor) and hypofluorescent (
n = 83, 65 malignant and 18 benign lesions). For determining malignant
vs. benign lesions, hypofluorescence had a positive predictive value of 87%, negative predictive value of 52%, sensitivity of 84% and specificity of 57%. Given these relatively poor predictive tools, the authors determined that the role of predicting malignancy based on ICG fluorescent patterns remains to be determined and should not supplant preoperative imaging. Perhaps standardization of the ICG dosing regimen, as suggested by Angell
et al. [
9], may improve intraoperative prediction of malignancy and possibly guide the surgeon’s aggressiveness during tumor resection.
Other compounds and dyes have been analyzed to assess differences in normal parenchyma and renal masses. For example, photodynamic diagnostic (PDD) has been used over the last decade to differentiate healthy from diseased tissue. Specifically, 5-aminolevulinic acid (5-ALA) accumulates in malignant cells and after endogenous metabolism to protoporphyrin IX can be irradiated at a wavelength of 390 to 440 nm and subsequently fluoresce red at 635 nm [
14,
15]. Hoda
et al. [
16] utilized an oral dose of 1.5 g of 5-ALA four hours prior to surgery in 77 patients undergoing laparoscopic partial nephrectomy and reported that 58 of 61 patients with renal cell carcinoma demonstrated a positive response to excitation light, however the remaining benign lesions also demonstrated some response to excitation light. Among the 61 malignant lesions, two patients had positive margins, however PDD was able to detect remaining tissue in the partial nephrectomy bed, allowing subsequent complete resection. To date, this technology applied to RPN has not been reported. Disciplines other than Urology have used additional fluorescent compounds to demonstrate combination nerve and tumor imaging for breast cancer surgery [
17]. Furthermore, animal models have demonstrated the feasibility of robotic-assisted sentinel lymph node mapping for pre-sacral nodes of the prostate using Ga-68-labeled tilmanocept [
18].
5. Conclusions
The initial institutional studies using near infrared fluorescent imaging of ICG dye demonstrate safety and feasibility when performing RPN. Identification of the renal vasculature and tumor margins is possible for mainly exophytic tumors; however, positive margin status for these tumors has not substantially improved. ICG may improve the ability of experienced surgeons to perform RPN with selective clamping or in some instances zero-ischemia, and early post-operative kidney function may improve using this technique. Although there are limitations to ICG for RPN, including visualization of endophytic tumors and difficultly demarcating tumor margins in reoperative cases, the field continues to advance as robotic surgeons become accustomed to ICG and additional compounds are developed. The precise combination of fluorescent compound, dose, and optimal tumor anatomy for ICG RPN has yet to be elucidated.
Author Contributions
Zachary Klaassen: Conceptual design, drafting of the manuscript, critical revision of the manuscript. Qiang Li: Critical revision of the manuscript. Rabii Madi: Critical revision of the manuscript. Martha K. Terris: Conceptual design, drafting of the manuscript, critical revision of the manuscript.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Huang, W.C.; Elkin, E.B.; Levey, A.S.; Jang, T.L.; Russo, P. Partial nephrectomy versus radical nephrectomy in patients with small renal tumors—Is there a difference in mortality and cardiovascular outcomes? J. Urol. 2009, 181, 55–61. [Google Scholar]
- Yossepowitch, O.; Thompson, R.H.; Leibovich, B.C.; Eggener, S.E.; Pettus, J.A.; Kwon, E.D.; Herr, H.W.; Blute, M.L.; Russo, P. Positive surgical margins at partial nephrectomy: Predictors and oncological outcomes. J. Urol. 2008, 179, 2158–2163. [Google Scholar] [CrossRef]
- Secil, M.; Elibol, C.; Aslan, G.; Kefi, A.; Obuz, F.; Tuna, B.; Yorukoglu, K. Role of intraoperative US in the decision for radical or partial nephrectomy. Radiology 2011, 258, 283–290. [Google Scholar] [CrossRef]
- Tobis, S.; Knopf, J.; Silvers, C.; Yao, J.; Rashid, H.; Wu, G.; Golijanin, D. Near Infrared Fluorescence Imaging with Robotic Assisted Laparoscopic Partial Nephrectomy: Initial Clinical Experience for Renal Cortical Tumors. J. Urol. 2011, 186, 47–52. [Google Scholar]
- Unno, N.; Suzuki, M.; Yamamoto, N.; Inuzuka, K.; Sagara, D.; Nishiyama, M.; Tanaka, H.; Konno, H. Indocyanine green fluorescence angiography for intraoperative assessment of blood flow: A feasibility study. Eur. J. Vasc. Endovasc. Surg. 2008, 35, 205–207. [Google Scholar] [CrossRef]
- Golijanin, D.J.; Marshall, J.; Cardin, A. Bilitranslocase (BTL) is immunolocalised in proximal and distal renal tubules and absent in renal cortical tumors accurately corresponding to intraoperative near infrared fluorescence (NIRF) expression of renal cortical tumors using intravenous indocyanine green (ICG). J. Urol. Suppl 2008, 179, 137. [Google Scholar] [CrossRef]
- Tobis, S.; Knopf, J.K.; Silvers, C.R.; Marshall, J.; Cardin, A.; Wood, R.W.; Reeder, J.E.; Erturk, E.; Madeb, R.; Yao, J.; et al. Near Infrared Fluorescence Imaging After Intravenous Indocyanine Green: Initial Clinical Experience with Open Partial Nephrectomy for Renal Cortical Tumors. Urology 2012, 79, 958–964. [Google Scholar] [CrossRef]
- Krane, L.S.; Manny, T.B.; Hemal, A.K. Is Near Infrared Fluorescence Imaging Using Indocyanine Green Dye Useful in Robotic Partial Nephrectomy: A Prospective Comparative Study of 94 Patients. Urology 2012, 80, 110–118. [Google Scholar] [CrossRef]
- Angell, J.E.; Khemees, T.A.; Abaza, R. Optimization of Near Infrared Fluorescence Tumor Localization during Robotic Partial Nephrectomy. J. Urol. 2013, 190, 1668–1673. [Google Scholar] [CrossRef]
- Borofsky, M.S.; Gill, I.S.; Hemal, A.K.; Marien, T.P.; Jayaratna, I.; Krane, L.S.; Stifelman, M.D. Near-infrared fluorescence imaging to facilitate super-selective arterial clamping during zero-ischemia robotic partial nephrectomy. BJU Int. 2012, 111, 604–610. [Google Scholar]
- Harke, N.; Schoen, G.; Schiefelbein, F.; Heinrich, E. Selective clamping under the usage of near-infrared fluorescence imaging with indocyanine green in robot-assisted partial nephrectomy: A single-surgeon matched-pair study. World J. Urol. 2013. [Google Scholar] [CrossRef]
- Bjurlin, M.A.; Gan, M.; McClintock, T.R.; Volpe, A.; Borofsky, M.S.; Mottrie, A.; Stifelman, M.D. Near-infrared Fluorescence Imaging: Emerging Applications in Robotic Upper Urinary Tract Surgery. Eur. Urol. 2014, 65, 793–801. [Google Scholar] [CrossRef]
- Manny, T.B.; Krane, L.S.; Hemal, A.K. Indocyanine Green Cannot Predict Malignancy in Partial Nephrectomy: Histopathologic Correlation with Fluorescence Pattern in 100 Patients. J. Endourol. 2013, 27, 918–921. [Google Scholar] [CrossRef]
- Uehlinger, P.; Zellweger, M.; Wagnieres, G.; Juillerat-Jeanneret, L.; van den Bergh, H.; Lange, N. 5-aminolevulinic acid and its derivatives: Physical chemical properties and proporphyrin IX formation in cultured cells. J. Photochem. Photobiol. 2000, 54, 72–80. [Google Scholar] [CrossRef]
- Steinbach, P.; Weingandt, H.; Baumgartner, R.; Kriegmair, M.; Hofstadter, F.; Knuchel, R. Cellular fluorescence of the endogenous photosensitizer protoporphyrin IX following exposure to 5-aminolevulinic acid. Photochem. Photobiol. 1995, 62, 887–895. [Google Scholar]
- Hoda, M.R.; Popken, G. Surgical Outcomes of Fluorescence-Guided Laparoscopic Partial Nephrectomy Using 5-Aminolevulinic Acid-Induced Protoporphyrin IX. J. Surg. Res. 2009, 154, 220–225. [Google Scholar] [CrossRef]
- Nguyen, Q.T.; Olson, E.S.; Aguilera, T.A.; Jiang, T.; Scadeng, M.; Ellies, L.G.; Tsien, R.Y. Surgery with molecular fluorescence imaging using activatable cell-penetrating peptides decreases residual cancer and improves survival. Proc. Natl. Acad. Sci. USA. 2010, 107, 4317–4322. [Google Scholar]
- Stroup, S.P.; Kane, C.J.; Farchshchi-Heydari, S.; James, C.M.; Davis, C.H.; Wallace, A.M.; Hoh, C.K.; Vera, D.R. Preoperative sentinel lymph node mapping of the prostate using PET/CT fusion imaging and Ga-68-labeled tilmanocept in an animal model. Clin. Exp. Metastasis 2012, 29, 673–680. [Google Scholar] [CrossRef]
© 2014 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/3.0/).



{kind=link}