Assessing Spatial Accessibility of Public and Private Residential Aged Care Facilities: A Case Study in Wuhan, Central China



Abstract
:1. Introduction
2. Methods
2.1. Study Area and Data Preparation
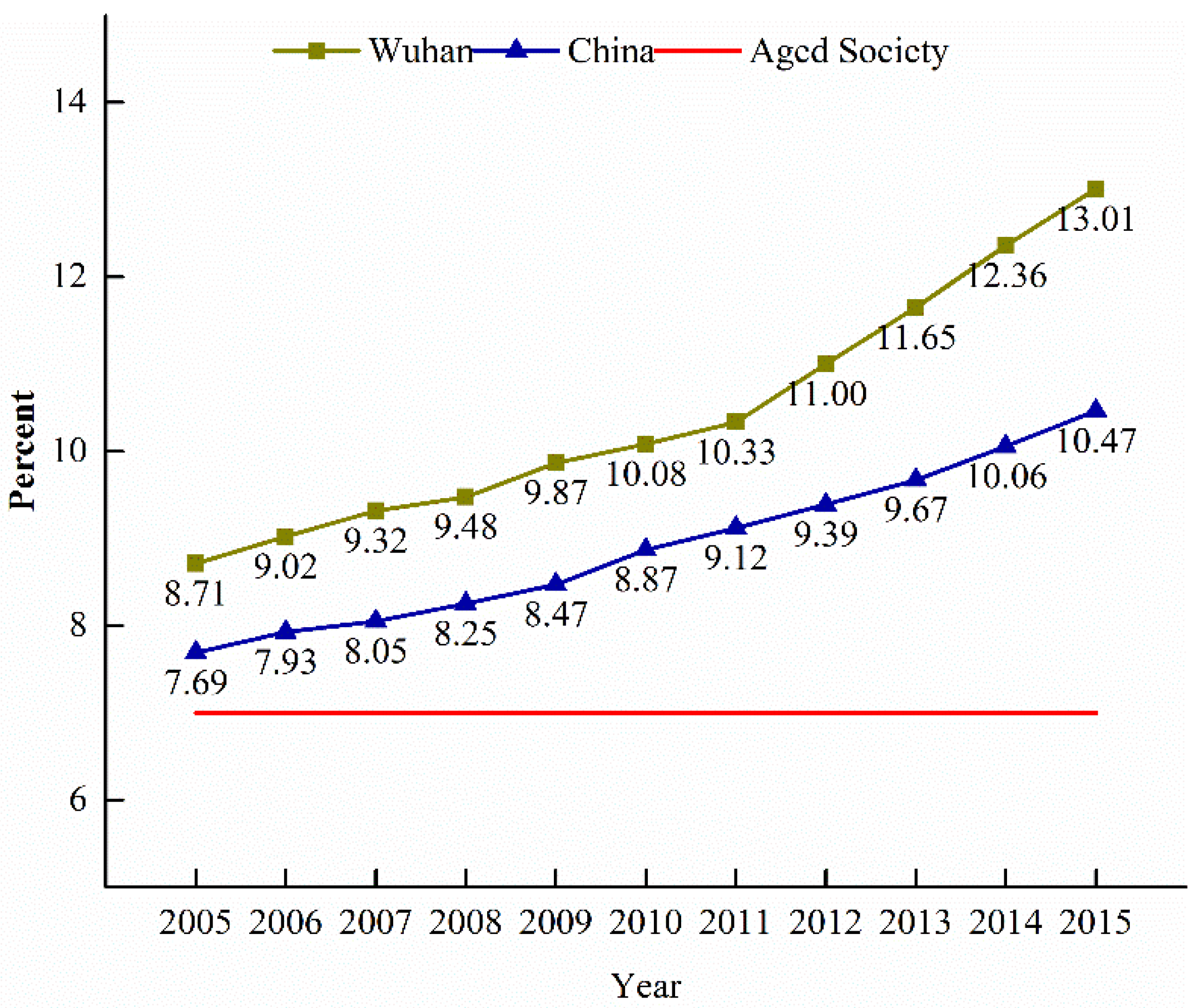
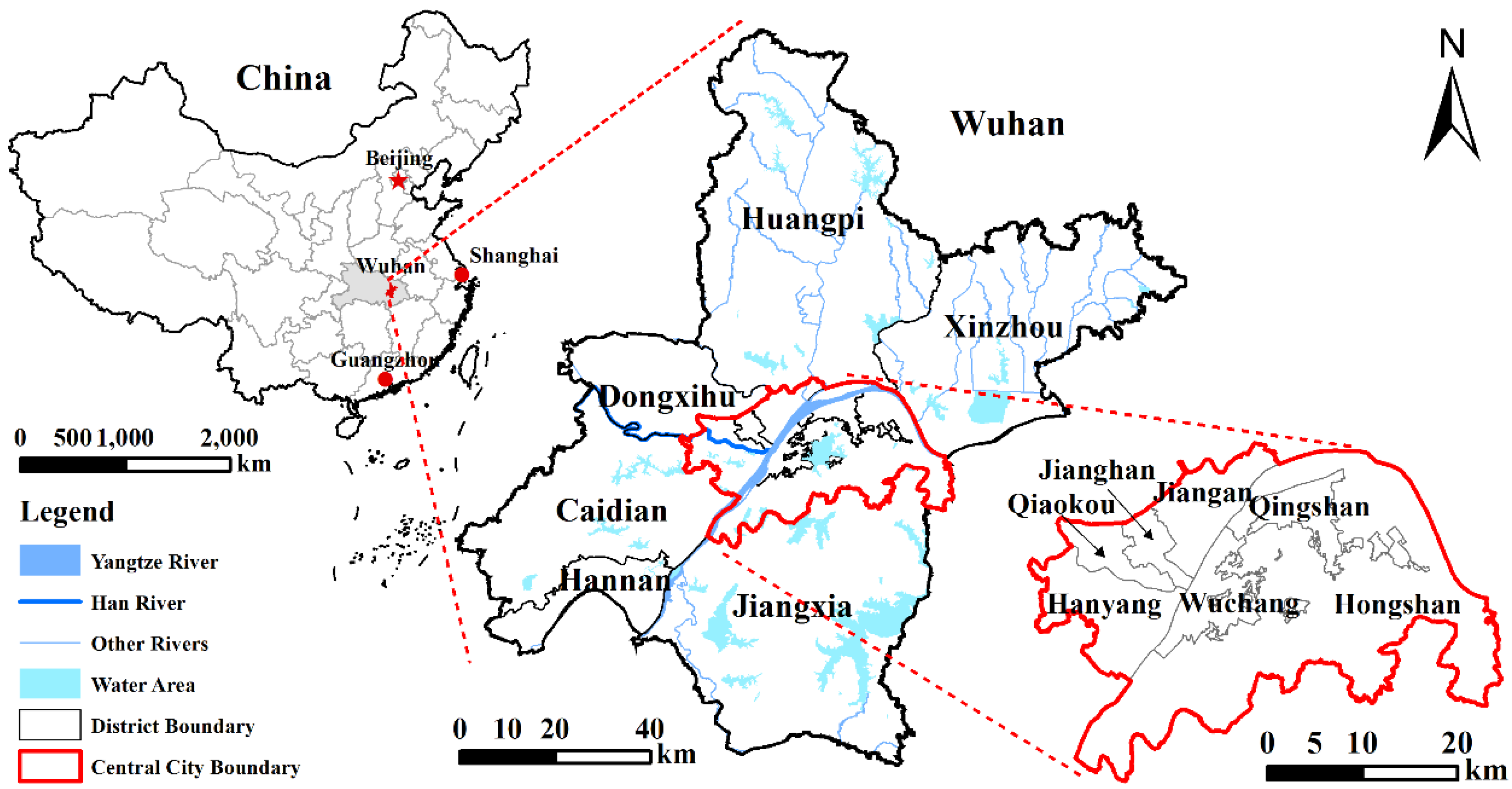
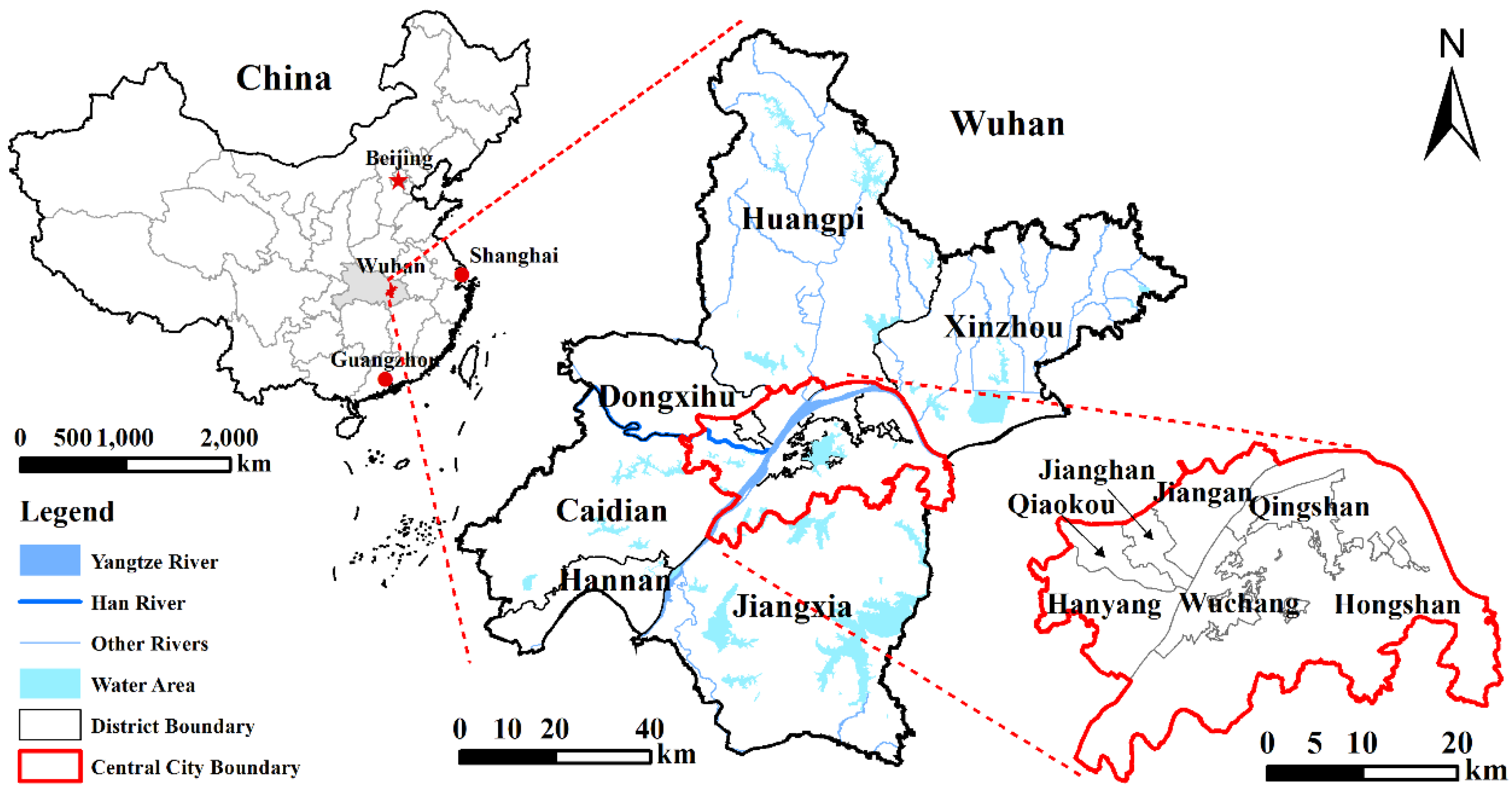
2.1.1. Study Area
2.1.2. Data Preparation
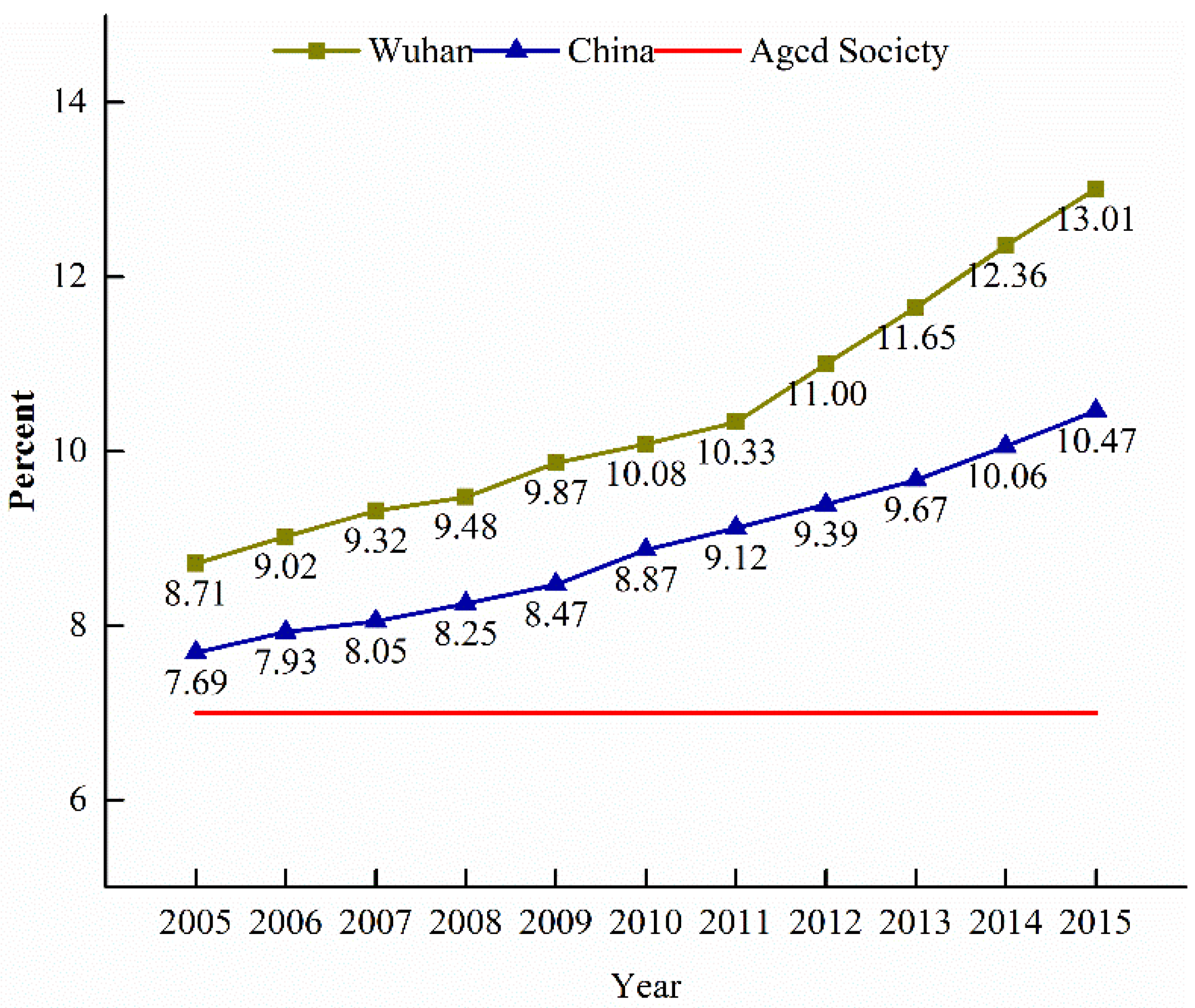
Aged Population
Residential Aged Care Facilities (RACFs)
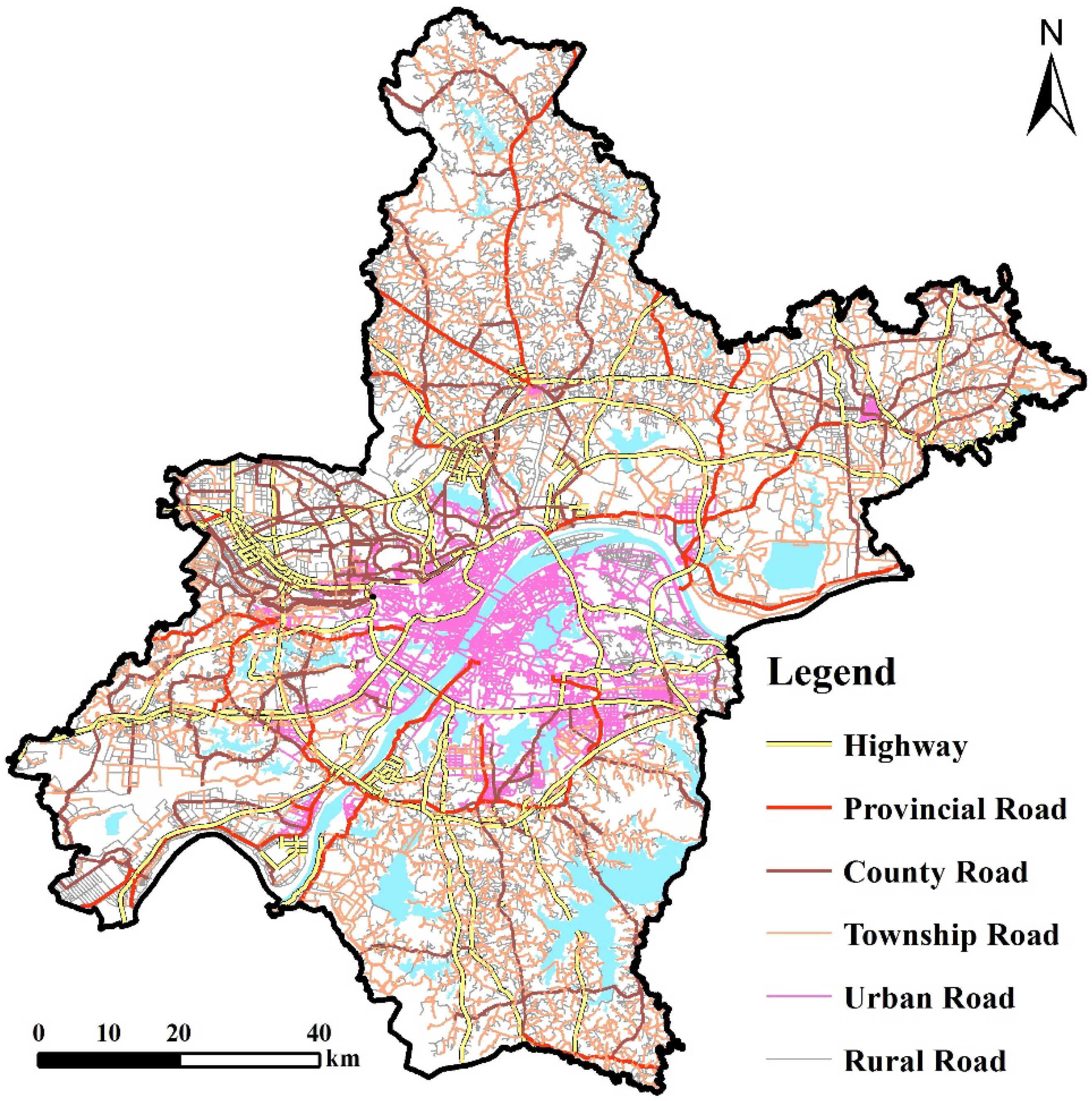
Traffic Network
2.2. Methods
2.2.1. MCSG2SFCA Method
2.2.2. Contribution of Public or Private RACFs
3. Results
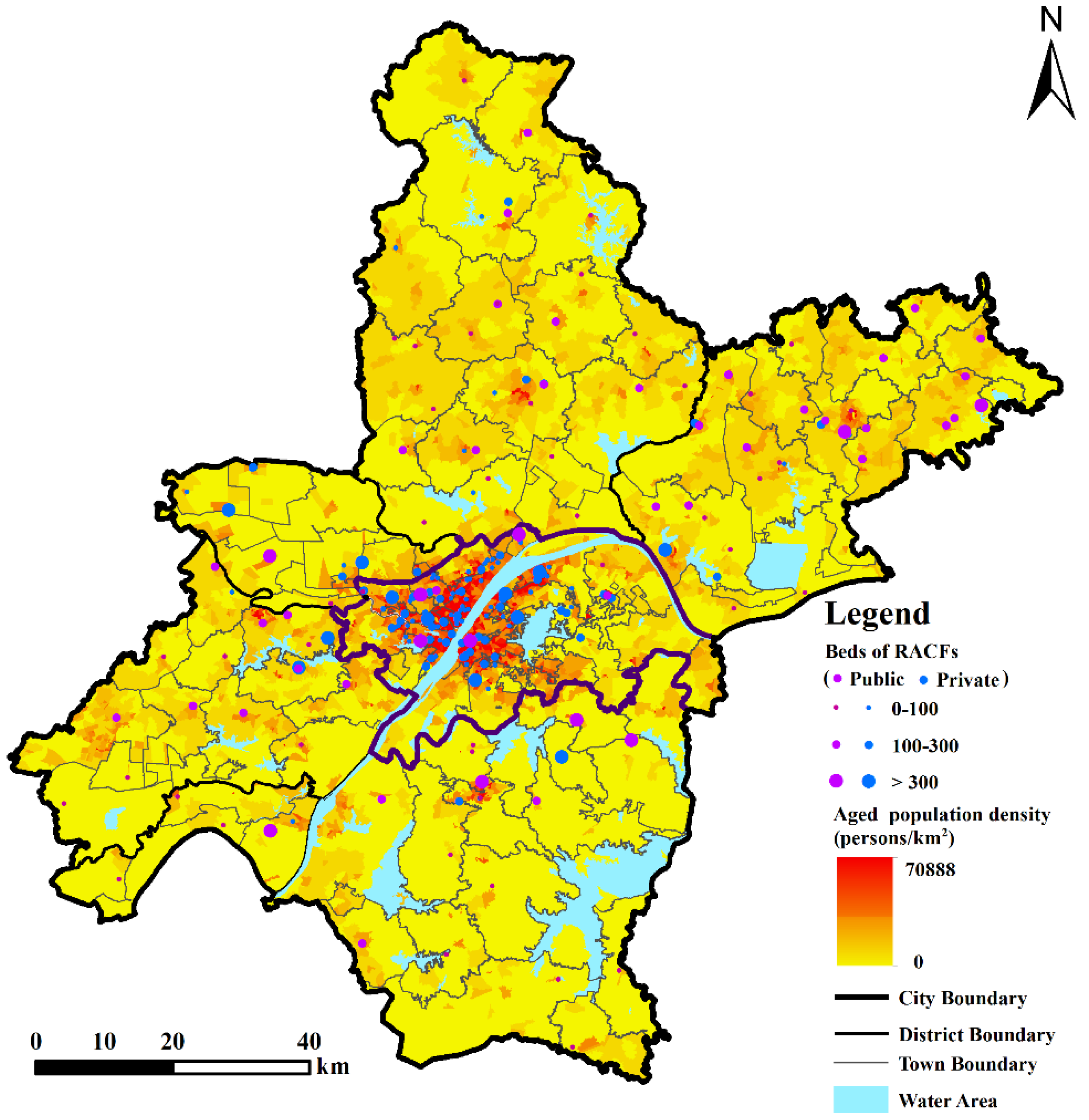
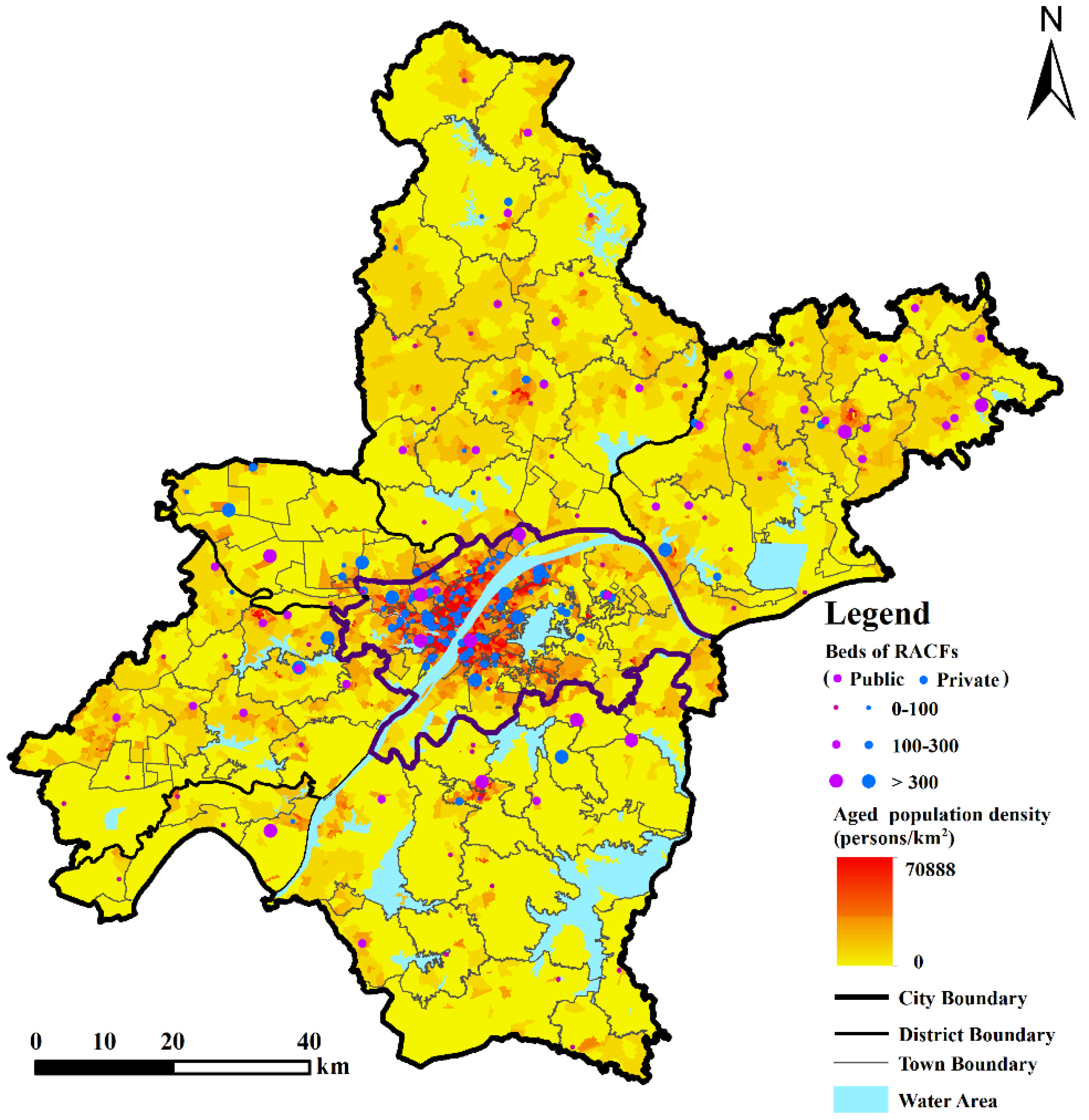
3.1. Distribution of Aged Population and Residential Aged Care Facilities
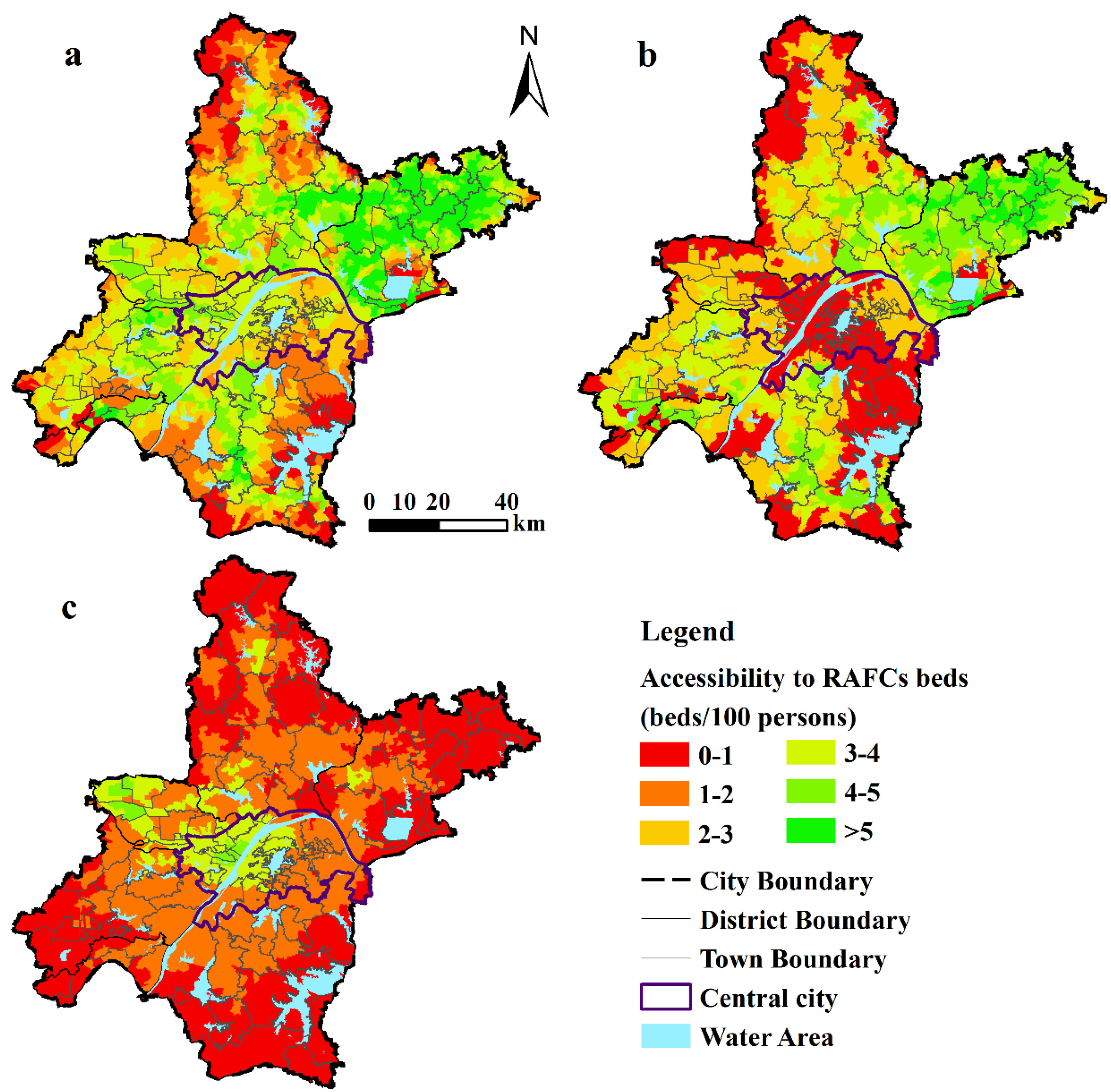
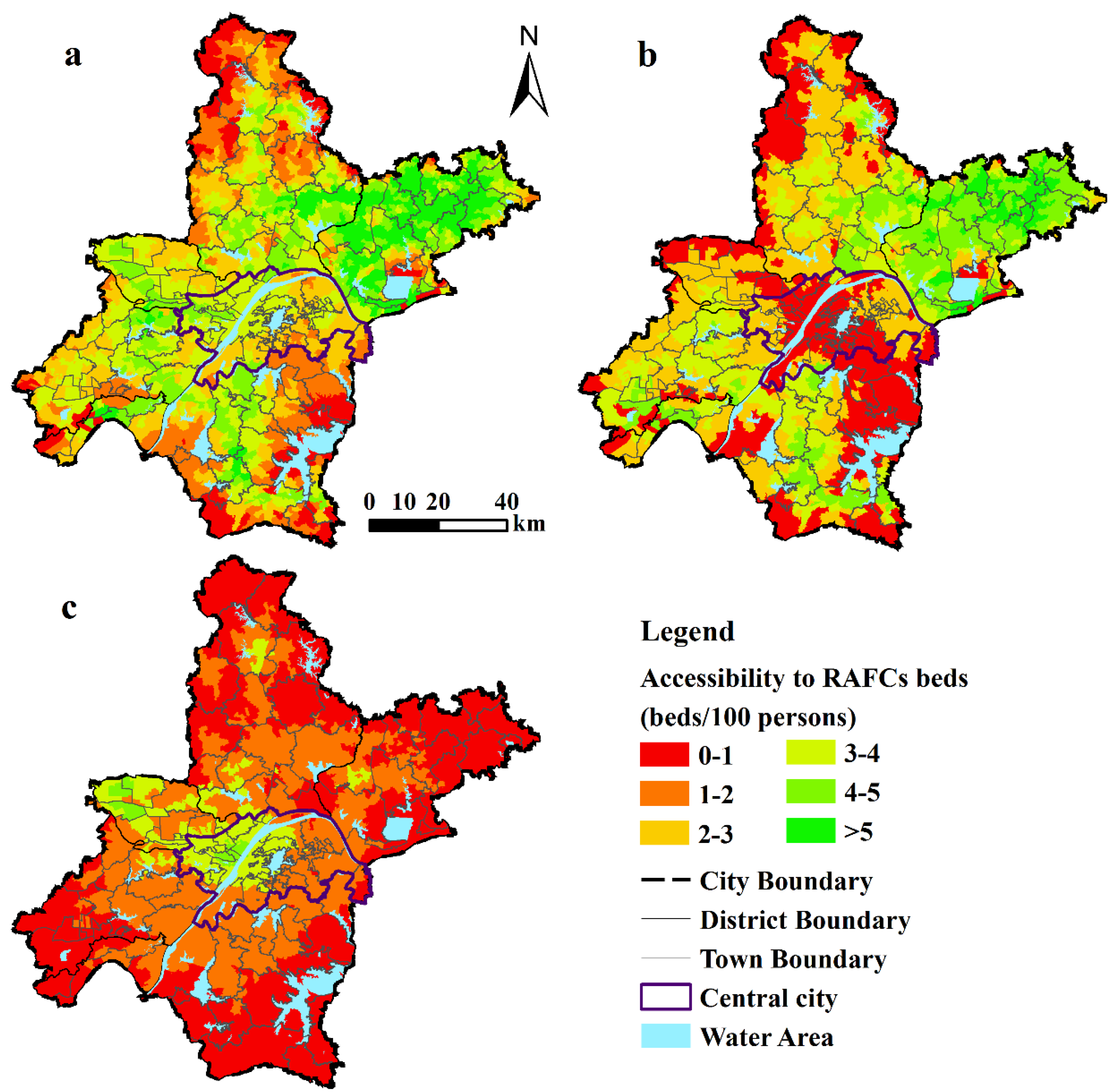
3.2. Spatial Pattern of Accessibility of RACFs
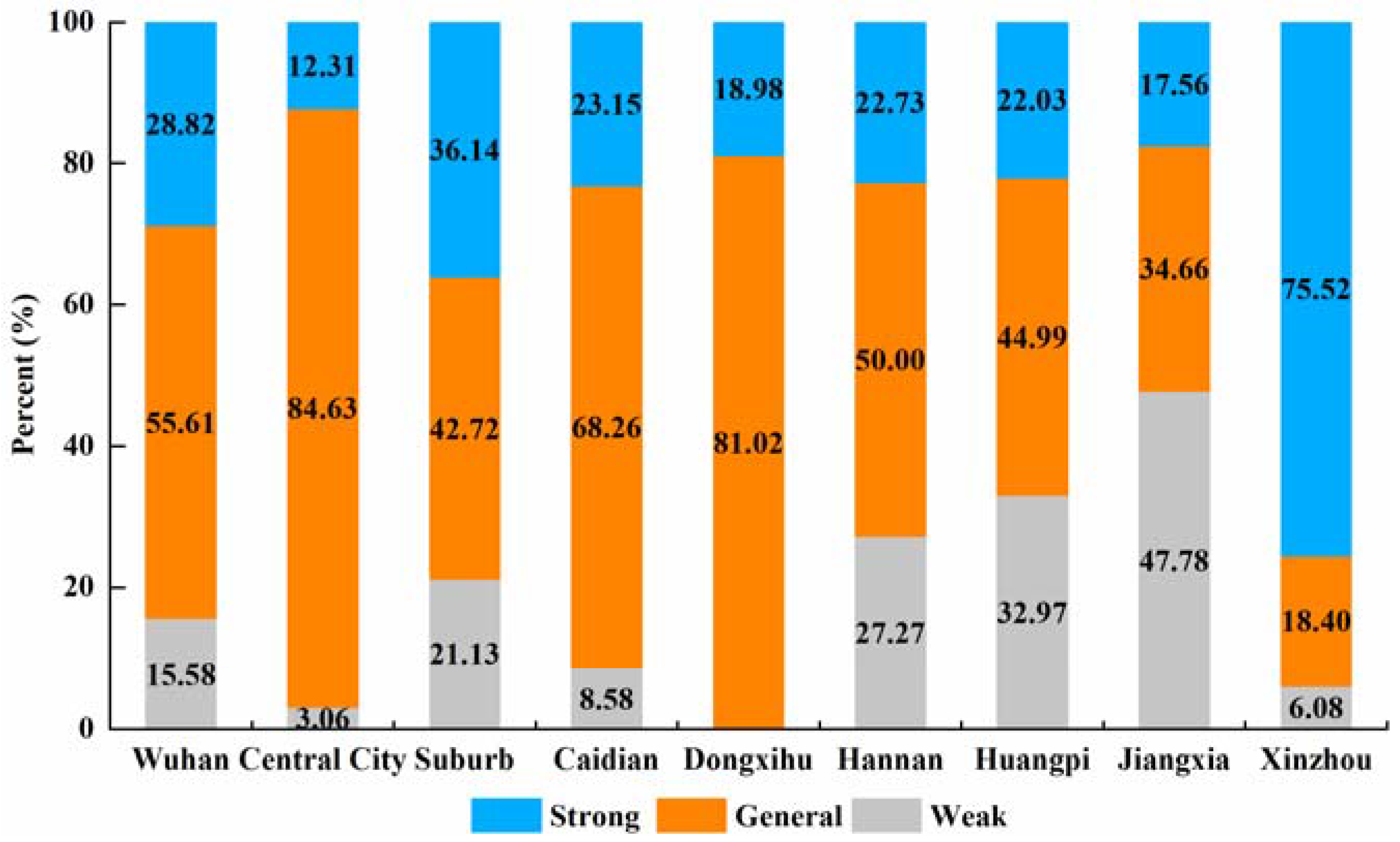
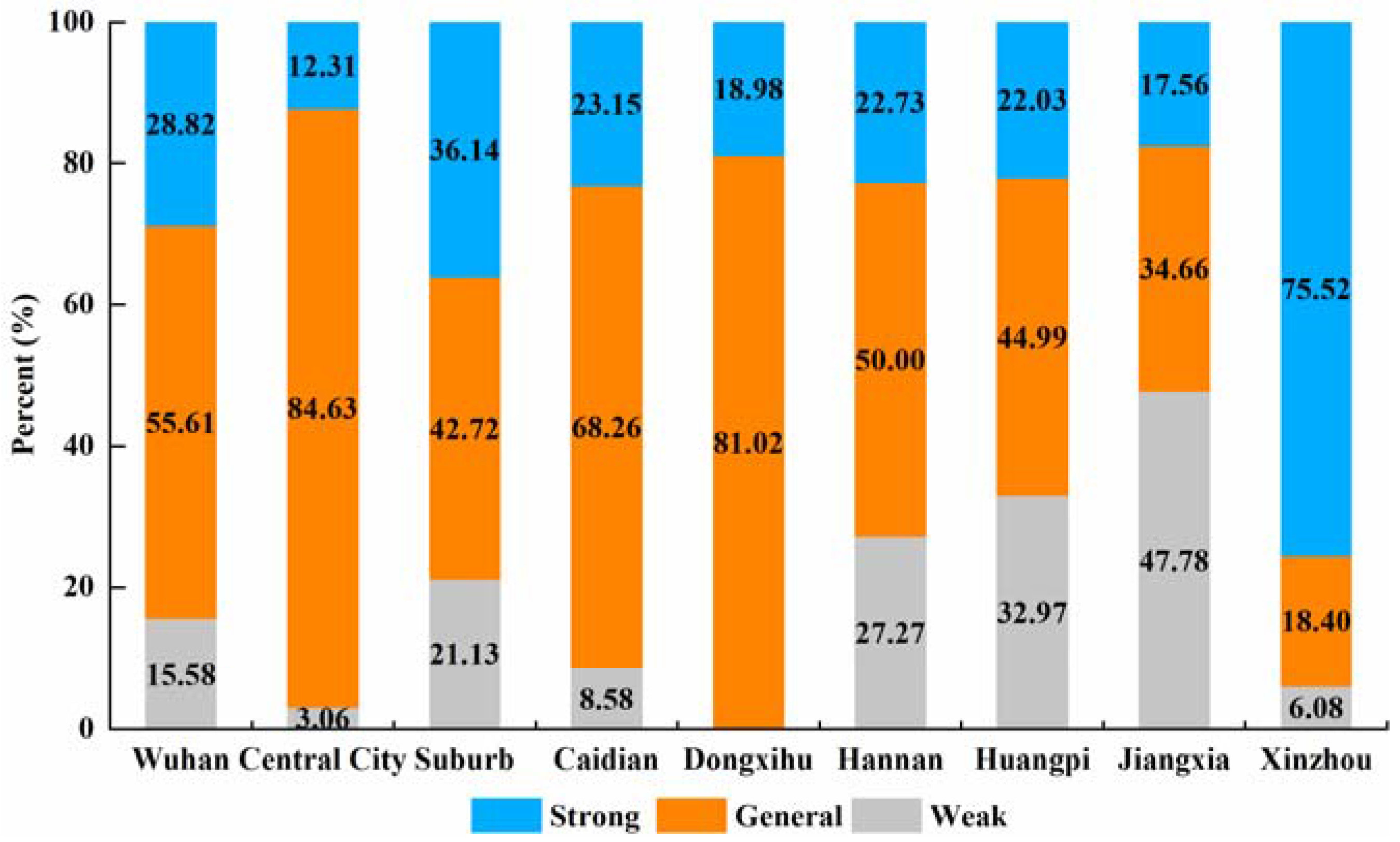
3.3. Aged Care Service Capability Analysis
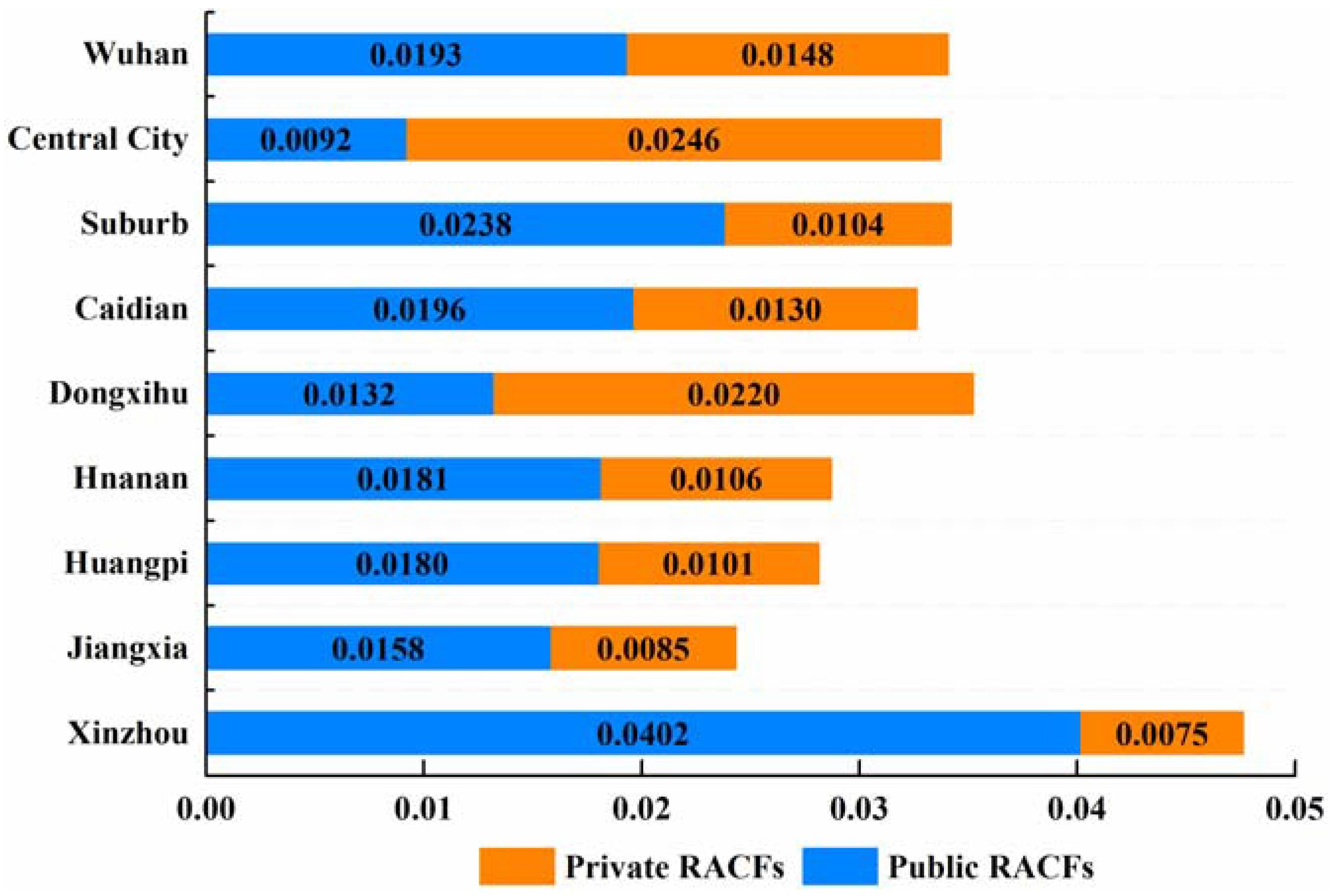
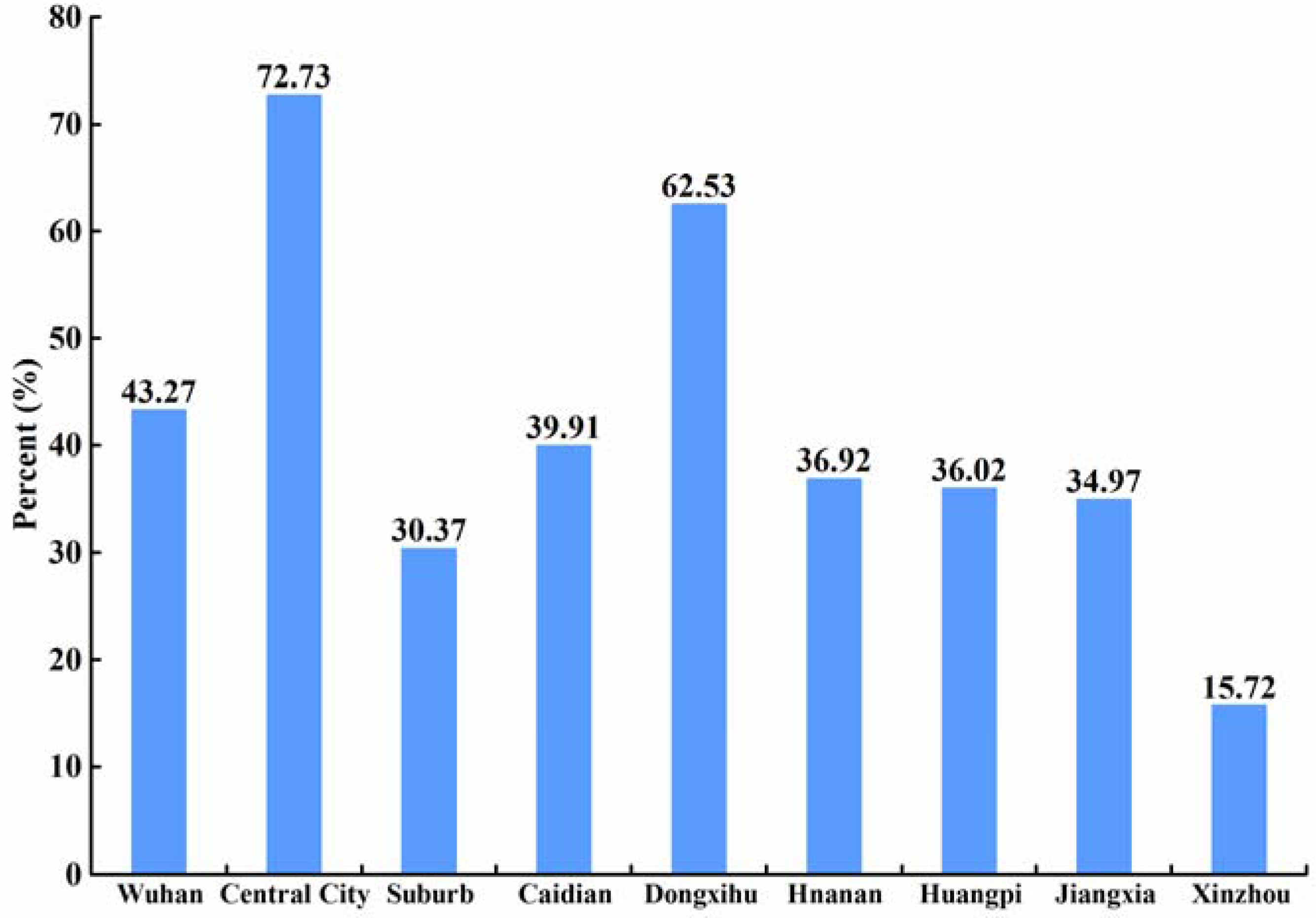
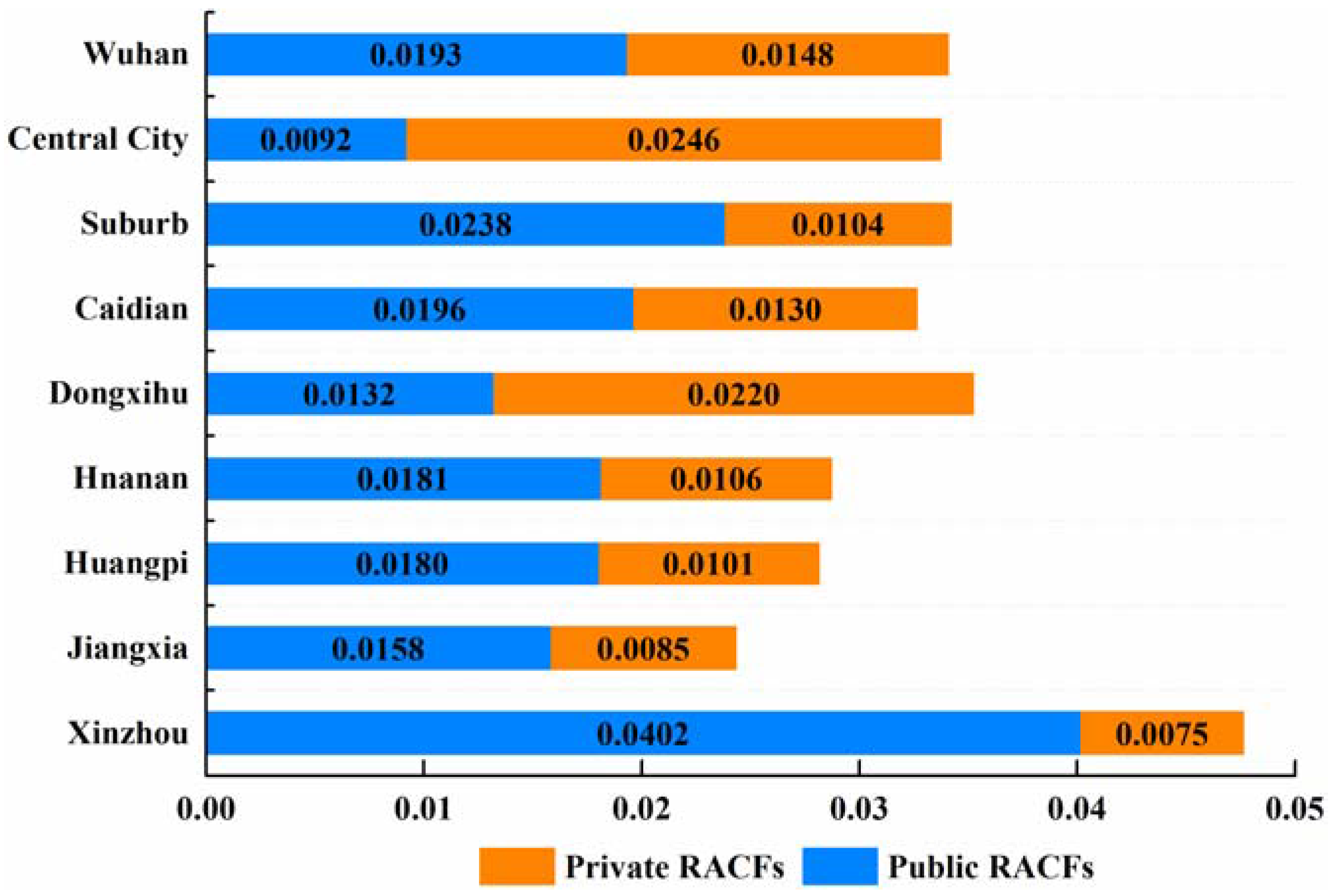
3.4. Difference Between Public and Private RACFs
4. Discussion
4.1. The Spatial Disparity in Accessibility of RACFs
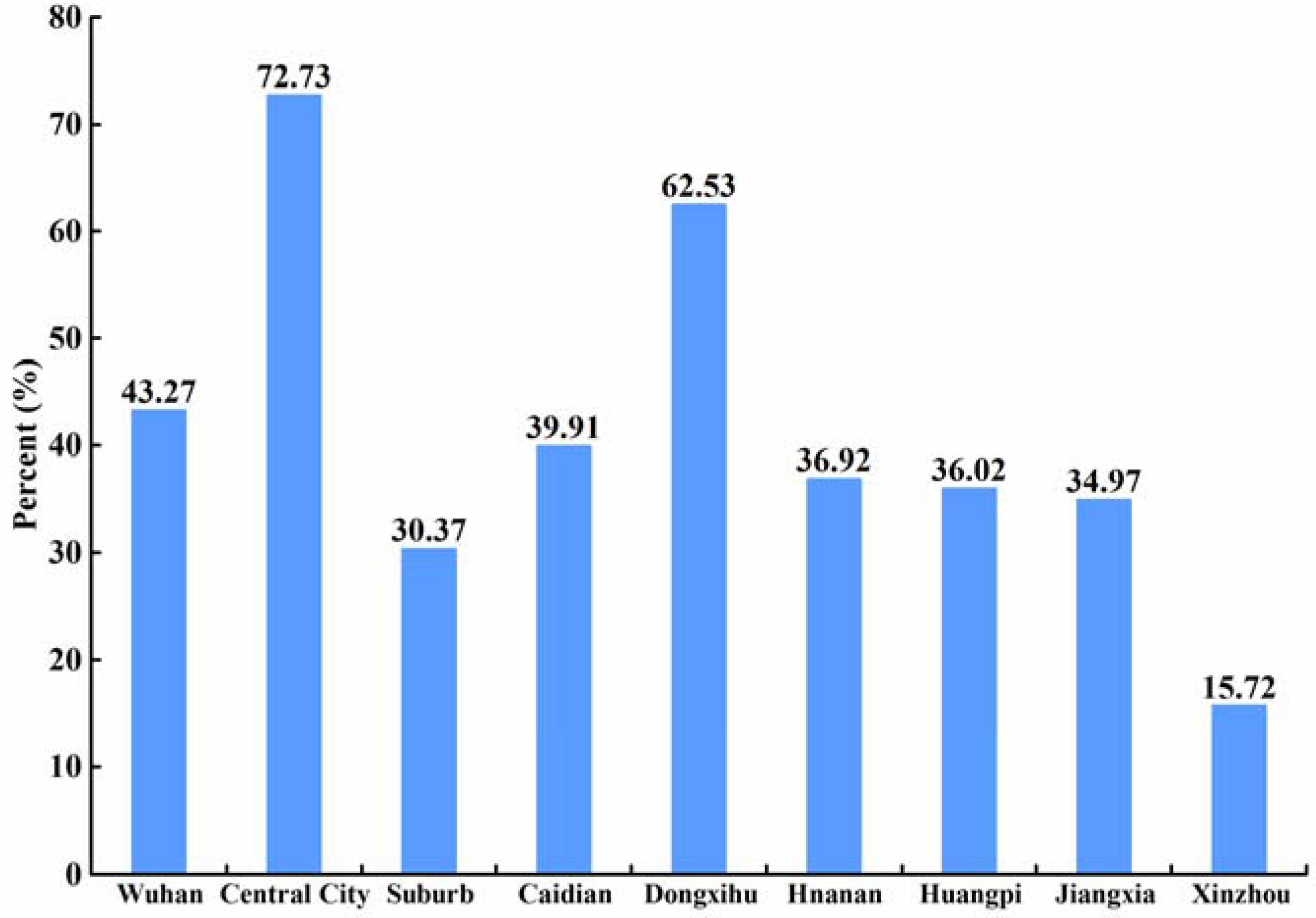
4.2. The Influence of Private RACFs
4.3. Implications for the Allocation of RACFs
4.4. Limitations
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of interests
References
- Zeng, Y. Toward deeper research and better policy for healthy aging—Using the unique data of Chinese longitudinal healthy longevity survey. China Econ. J. 2012, 5, 131. [Google Scholar] [CrossRef] [PubMed]
- The State Council the Construction Plan of Social Elderly Care System (2011–2015). Available online: http://www.gov.cn/zwgk/2011–12/27/content_2030503.htm (accessed on 3 December 2016).
- National Health and Family Planning Commission Implementation Opinions on Encouraging Private Capital to Participate in The Development of Elderly Care Service Industry. Available online: http://www.nhfpc.gov.cn/jtfzs/s3581c/201502/501ddc3de0e44b899e2cc53369225478.shtml (accessed on 4 December 2016).
- Hubei Province Working Committee on Aging Analysis on the situation of population aging in Wuhan city in 2013. Available online: http://www.hbllw.cn/html/2015/llyj_0709/17232.html (accessed on 9 July 2015).
- Wuhan Land Resources and Planning Bureau Spatial Layout Planning of Residential Care Facilities in Wuhan (2012–2020). Available online: http://www.mlr.gov.cn/zwgk/ghjh/201408/t20140813_1326862.htm (accessed on 15 March 2017).
- Wuhan Municipal Bureau of Civil Affairs Survey on the aged service in Wuhan. Available online: http://hb.qq.com/a/20130415/000786.htm (accessed on 10 October 2017).
- Zhou, S.; Xie, M.; Kwan, M. Ageing in place and ageing with migration in the transitional context of urban China: A case study of ageing communities in Guangzhou. Habitat Int. 2015, 49, 177–186. [Google Scholar] [CrossRef]
- Kim, K.; Gollamudi, S.S.; Steinhubl, S. Digital technology to enable aging in place. Exp. Gerontol. 2017, 88, 25–31. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization Global Age-Friendly Cities Project. Available online: www.who.int./ageing/age_friendly_cities_network (accessed on 10 October 2017).
- Wahl, H.W.; Iwarsson, S.; Oswald, F. Aging well and the environment: Toward an integrative model and research agenda for the future. Gerontologist 2012, 52, 306–316. [Google Scholar] [CrossRef] [PubMed]
- Wiles, J.L.; Leibing, A.; Guberman, N.; Reeve, J.; Allen, R.E.S. The Meaning of “Aging in Place” to Older People. Gerontologist 2012, 52, 357–366. [Google Scholar] [CrossRef] [PubMed]
- Lawton, M.P.; Simon, B. Ecology of social relationship in housing for elderly. Gerontologist 1968, 8, 108. [Google Scholar] [CrossRef] [PubMed]
- Sanchez Gonzalez, D. Environmental Gerontology: Making Meaningful Places in Old Age; Springer Publishing Company: New York, NY, USA, 2013. [Google Scholar]
- Iwarsson, S.; Wahl, H.; Nygren, C.; Oswald, F.; Sixsmith, A.; Sixsmith, J.; Szeman, Z.; Tomsone, S. Importance of the home environment for healthy aging: Conceptual and methodological background of the European ENABLE-AGE project. Gerontologist 2007, 47, 78–84. [Google Scholar] [CrossRef] [PubMed]
- Oswald, F.; Jopp, D.; Rott, C.; Wahl, H. Is aging in place a resource for or risk to life satisfaction? Gerontologist 2011, 51, 238–250. [Google Scholar] [CrossRef] [PubMed]
- Wu, Y.; Wang, L.; Kong, W.; Dong, P.; Yang, X. The Chinese Pension Institution Development Research. Sci. Res. Aging 2015, 3, 13–24. [Google Scholar]
- Cheng, Y. Residential Care for Elderly People in Beijing, China: A Study of the Relationship between Health and Place. Ph.D. Thesis, Queen’s University, Kingston, ON, Canada, 2010. [Google Scholar]
- Cheng, Y.; Wang, J.E.; Rosenberg, M.W. Spatial access to residential care resources in Beijing, China. Int. J. Health Geogr. 2012, 11, 32. [Google Scholar] [CrossRef] [PubMed]
- Yan, B.Q.; Gao, X.L.; Ji, J. Micro simulation and planning policies analysis for urban elderly care facilities: Take Beijing as an example. Prog. Geogr. 2015, 34, 1586–1597. [Google Scholar]
- Tao, Z.L.; Cheng, Y.; Dai, T.Q.; Li, X. Spatial optimization of residential care facility locations in 2020 in Beijing: Maximum equity in accessibility. Prog. Geogr. 2015, 34, 1609–1616. [Google Scholar]
- Dadashpoor, H.; Rostami, F.; Alizadeh, B. Is inequality in the distribution of urban facilities inequitable? Exploring a method for identifying spatial inequity in an Iranian city. Cities 2016, 52, 159–172. [Google Scholar] [CrossRef]
- Wang, F.; Tang, Q. Planning toward equal accessibility to services: A quadratic programming approach. Environ. Plan. B 2013, 40, 195–212. [Google Scholar] [CrossRef]
- Smoyer-Tomic, K.E.; Hewko, J.N.; Hodgson, M.J. Spatial accessibility and equity of playgrounds in Edmonton, Canada. Can. Geogr. 2004, 48, 287–302. [Google Scholar] [CrossRef]
- Lin, K.; Lu, Y.Q.; Liu, J.; Zhang, L.; Wang, T.N. Assessment of fair space of public product based on accessibility: A case of Yizheng city. Geogr. Res. 2009, 28, 215–224. [Google Scholar]
- Kaczynski, A.T.; Potwarka, L.R.; Saelens, B.E. Association of park size, distance, and features with physical activity in neighborhood parks. Am. J. Public Health 2008, 98, 1451–1456. [Google Scholar] [CrossRef] [PubMed]
- Connor, R.A.; Hillson, S.D.; Krawelski, J.E. Competition, professional synergism, and the geographic distribution of rural physicians. Med. Care 1995, 33, 1067–1078. [Google Scholar] [CrossRef] [PubMed]
- Schonfeld, H.K.; Heston, J.F.; Falk, I.S. Numbers of physicians required for primary medical care. N. Engl. J. Med. 1972, 286, 571–576. [Google Scholar] [CrossRef] [PubMed]
- Guagliardo, M.F. Spatial accessibility of primary care: Concepts, methods and challenges. Int. J. Health Geogr. 2004, 3, 3. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yang, D.; Goerge, R.; Mullner, R. Comparing GIS-based methods of measuring spatial accessibility to health services. J. Med. Syst. 2006, 30, 23–32. [Google Scholar] [CrossRef] [PubMed]
- Hilisdon, M.; Panter, J.; Foster, C.; Jones, A. The relationship between access and quality of urban green space with population physical activity. Public Health 2006, 120, 1127–1132. [Google Scholar] [CrossRef] [PubMed]
- Radke, J.; Mu, L. Spatial Decompositions, Modeling and Mapping Service Regions to Predict Access to Social Programs. Geogr. Inf. Sci. 2000, 2, 105–112. [Google Scholar] [CrossRef]
- Luo, W.; Wang, F.H. Measures of spatial accessibility to health care in a GIS environment: Synthesis and a case study in the Chicago region. Environ. Plan. B 2003, 30, 865–884. [Google Scholar] [CrossRef]
- McGrail, M.R. Spatial accessibility of primary health care utilising the two step floating catchment area method: An assessment of recent improvements. Int. J. Health Geogr. 2012, 11, 50. [Google Scholar] [CrossRef] [PubMed]
- Song, P.; Zhu, Y.J.; Mao, X.; Li, Q.; An, L. Assessing Spatial Accessibility to Maternity Units in Shenzhen, China. PLoS ONE 2013, 8. [Google Scholar] [CrossRef] [PubMed]
- Wang, F.H. Measurement, Optimization, and Impact of Health Care Accessibility: A Methodological Review. Ann. Assoc. Am. Geogr. 2012, 102, 1104–1112. [Google Scholar] [CrossRef] [PubMed]
- Luo, W.; Qi, Y. An enhanced two-step floating catchment area (E2SFCA) method for measuring spatial accessibility to primary care physicians. Health Place 2009, 15, 1100–1107. [Google Scholar] [CrossRef] [PubMed]
- Dai, D. Black residential segregation, disparities in spatial access to health care facilities, and late-stage breast cancer diagnosis in metropolitan Detroit. Health Place 2010, 16, 1038–1052. [Google Scholar] [CrossRef] [PubMed]
- Dai, D. Racial/ethnic and socioeconomic disparities in urban green space accessibility: Where to intervene? Landsc. Urban Plan 2011, 102, 234–244. [Google Scholar] [CrossRef]
- Wang, Q.; Xiu, C.; Wei, Y.; Zhang, L. Evaluation of job accessibility of Shengyang using Guassian based 2-step floating catchment area method. Hum. Geogr. 2015, 2, 78–82. [Google Scholar]
- Wuhan Municipal Government the Administrative Institutions of Wuhan City. Available online: http://www.wuhan.gov.cn/whszfwz/xwxx/whgl/201411/t20141109_13853.html (accessed on 10 December 2016).
- Gao, Y.; He, Q.S.; Liu, Y.L.; Zhang, L.Y.; Wang, H.F.; Cai, E.X. Imbalance in Spatial Accessibility to Primary and Secondary Schools in China: Guidance for Education Sustainability. Sustainability 2016, 8, 1236. [Google Scholar] [CrossRef]
- Wuhan Civil Affairs Bureau List of the Social Pension Institutions in Wuhan City. Available online: http://www.whmzj.gov.cn/mzdsj/index.aspx (accessed on 5 December 2016).
- Wuhan Land Resources and Planning Bureau Annual Report on Traffic Development in Wuhan. Available online: http://www.wpl.gov.cn/pc-0–51822.html (accessed on 5 December 2016).
- Ministry of Housing and Urban-Rural Development Design Code for Buildings of Elderly Facilities. Available online: http://www.mohurd.gov.cn/wjfb/201509/t20150910_224798.html (accessed on 12 December 2016).
- Dang, H.M. The Spatial Accessibility Research on Maternity Medical Resources: A Case of Six District Beijing. Master’s Thesis, Capital Normal University, Beijing, China, 2013. [Google Scholar]
- Ren, R.; Wang, Y.; He, Z.; Zhao, W. Research on Spatial Accessibility of Primary School Education Resources in Poverty Area Based On Modified Two-step Floating Catchment Area Method—A Case Study of Qian Jiang. Geomat. World 2014, 21, 22–28. [Google Scholar]
- The State Council the 12th Five-Year Plan for National Basic Public Service System. Available online: http://www.gov.cn/zwgk/2012-07/20/content_2187242.htm (accessed on 15 May 2017).
- Pan, J.; Zhao, H.Q.; Wang, X.L.; Shi, X. Assessing spatial access to public and private hospitals in Sichuan, China: The influence of the private sector on the healthcare geography in China. Soc. Sci. Med. 2016, 170, 35–45. [Google Scholar] [CrossRef] [PubMed]
- UNPF. State of World Population 2007; UNPF: New York, NY, USA, 2007. [Google Scholar]
- Ngui, A.N.; Apparicio, P. Optimizing the two-step floating catchment area method for measuring spatial accessibility to medical clinics in Montreal. BMC Health Serv. Res. 2011, 11, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Kang, C. Spatial access to pedestrians and retail sales in Seoul, Korea. Habitat Int. 2016, 57, 110–120. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Type | All RACFs | Public RACFs | Private RACFs | Distance Thresholds (d0) |
|---|---|---|---|---|
| T1 (Large) | 25 | 13 | 12 | 100 |
| T2 (Medium) | 97 | 41 | 56 | 50 |
| T3 (Small) | 114 | 40 | 74 | 25 |
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cai, E.; Liu, Y.; Jing, Y.; Zhang, L.; Li, J.; Yin, C. Assessing Spatial Accessibility of Public and Private Residential Aged Care Facilities: A Case Study in Wuhan, Central China. ISPRS Int. J. Geo-Inf. 2017, 6, 304. https://doi.org/10.3390/ijgi6100304
Cai E, Liu Y, Jing Y, Zhang L, Li J, Yin C. Assessing Spatial Accessibility of Public and Private Residential Aged Care Facilities: A Case Study in Wuhan, Central China. ISPRS International Journal of Geo-Information. 2017; 6(10):304. https://doi.org/10.3390/ijgi6100304
Chicago/Turabian StyleCai, Enxiang, Yaolin Liu, Ying Jing, Lei Zhang, Jiwei Li, and Chaohui Yin. 2017. "Assessing Spatial Accessibility of Public and Private Residential Aged Care Facilities: A Case Study in Wuhan, Central China" ISPRS International Journal of Geo-Information 6, no. 10: 304. https://doi.org/10.3390/ijgi6100304