
Pain Assessment of Elderly Patients with Cognitive Impairment in the Emergency Department: Implications for Pain Management—A Narrative Review of Current Practices


Abstract
:1. Introduction
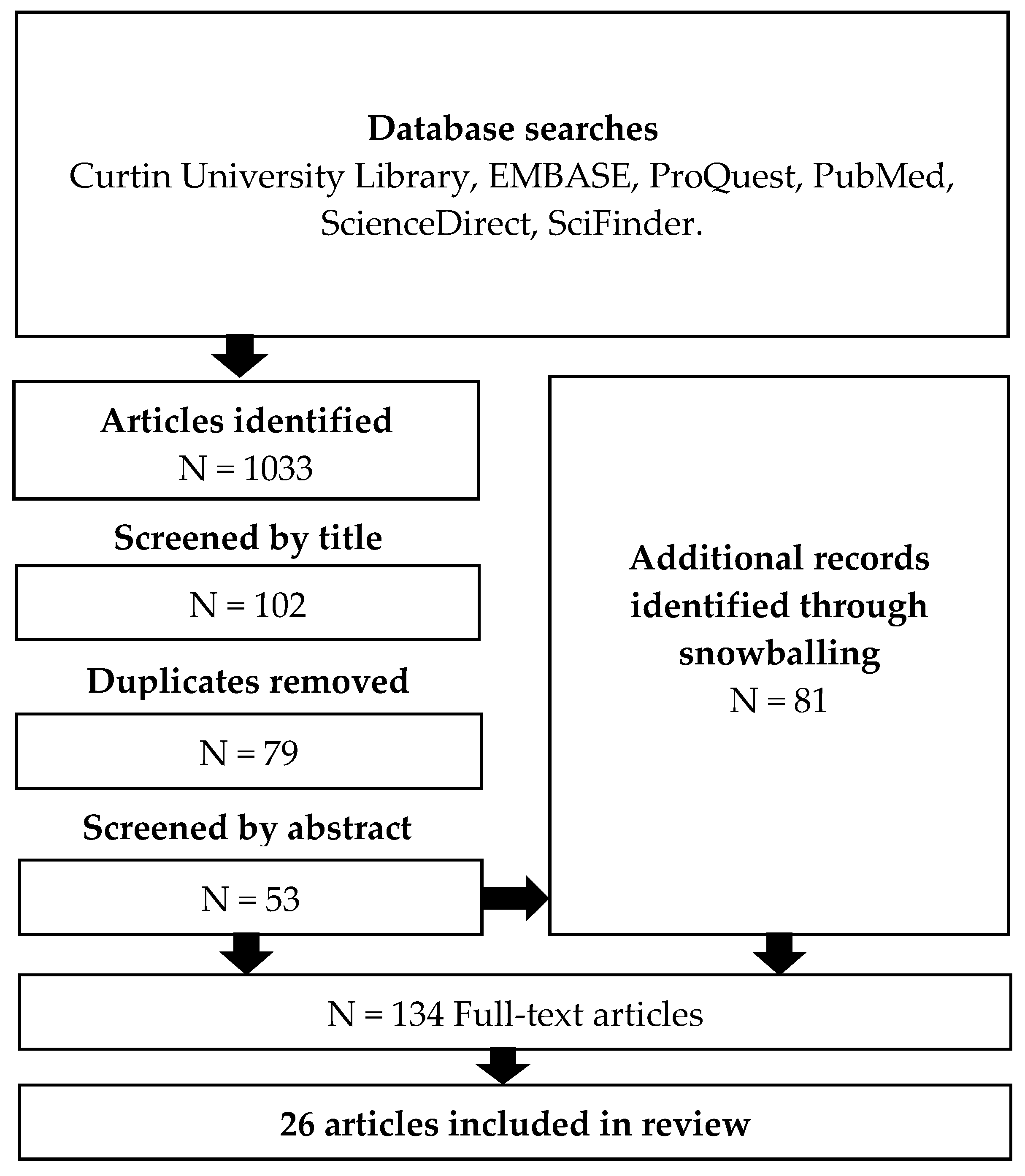
2. Methods
3. Findings
3.1. Methods of Pain Assessment
3.2. Frequency of Pain Assessment
3.3. Analgesia is Delayed for Elderly Patients with Cognitive Impairment
3.4. Pain Assessment Improves Pain Management
3.5. Consequences of Poor Pain Management
4. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Registered Nurses’ Association of Ontario. Assessment and Management of Pain, 3rd ed.; Registered Nurses’ Association of Ontario: Toronto, ON, Canada, 2013. [Google Scholar]
- Schofield, P.; O’mahony, S.; Collett, B.; Potter, J. Guidance for the assessment of pain in older adults: A literature review. Br. J. Nurs. 2008, 17, 914–918. [Google Scholar] [CrossRef] [PubMed]
- Brummel-Smith, K.; London, M.R.; Drew, N.; Krulewitch, H.; Singer, C.; Hanson, L. Outcomes of pain in frail older adults with dementia. J. Am. Geriatr. Soc. 2002, 50, 1847–1851. [Google Scholar] [CrossRef] [PubMed]
- Lukas, A.; Niederecker, T.; Günther, I.; Mayer, B.; Nikolaus, T. Self- and proxy report for the assessment of pain in patients with and without cognitive impairment. J. Gerontol. Geriatr. 2013, 3, 214–221. [Google Scholar] [CrossRef] [PubMed]
- Scherder, E.; Bouma, A. Visual analogue scales for pain assessment in Alzheimer’s disease. Gerontology 2000, 46, 47–53. [Google Scholar] [CrossRef] [PubMed]
- Wynne, C.F.; Ling, S.M.; Remsburg, R. Comparison of pain assessment instruments in cognitively intact and cognitively impaired nursing home residents. Geriatr. Nurs. 2000, 21, 20–23. [Google Scholar] [CrossRef] [PubMed]
- Kunz, M.; Mylius, V.; Scharmann, S.; Schepelman, K.; Lautenbacher, S. Influence of dementia on multiple components of pain. Eur. J. Pain 2009, 13, 317–325. [Google Scholar] [CrossRef] [PubMed]
- Vos, T.; Allen, C.; Arora, M.; Barber, R.M.; Bhutta, Z.A.; Brown, A.; Carter, A.; Casey, D.C.; Charlson, F.J.; Chen, A.Z.; et al. Global, regional, and national incidence, prevalence, and years lived with disability for 310 diseases and injuries, 1990–2015: A systematic analysis for the global burden of disease study 2015. Lancet 2016, 388, 1545–1602. [Google Scholar] [CrossRef]
- World Health Organization. WHO Global Report on Falls Prevention in Older Age; World Health Organization: Geneva, Switzerland, 2007; pp. 1–9. [Google Scholar]
- Burns, E.R.; Stevens, J.A.; Lee, R. The direct costs of fatal and non-fatal falls among older adults-united states. J. Saf. Res. 2016, 58, 99–103. [Google Scholar] [CrossRef] [PubMed]
- Stenhagen, M.; Ekström, H.; Nordell, E.; Elmståhl, S. Accidental falls, health-related quality of life and life satisfaction: A prospective study of the general elderly population. Arch. Gerontol. Geriatr. 2014, 58, 95–100. [Google Scholar] [CrossRef] [PubMed]
- Bradley, C. Trends in Hospitalisations due to Falls by Older People, Australia 1999-00 to 2010-11 (Injury Research and Statistics Series No. 84. Cat. No. INJCAT 160); Australian Institute of Health and Welfare: Canberra, Australia, 2013. Available online: Http://www.aihw.gov.au/publication-detail/?id=60129543594 (accessed on 5 May 2017).
- Tomlinson, E.J.; Phillips, N.M.; Mohebbi, M.; Hutchinson, A.M. Risk factors for incident delirium in an acute general medical setting: A retrospective case-control study. J. Clin. Nurs. 2017, 26, 658–667. [Google Scholar] [CrossRef] [PubMed]
- Fortini, A.; Morettini, A.; Tavernese, G.; Facchini, S.; Tofani, L.; Pazzi, M. Delirium in elderly patients hospitalized in internal medicine wards. Intern. Emerg. Med. 2014, 9, 435–441. [Google Scholar] [CrossRef] [PubMed]
- Morrison, R.; Magaziner, J.; Gilbert, M.; Koval, K.; McLaughlin, M.A.; Orosz, G.; Strauss, E.; Siu, A.L. Relationship between pain and opioid analgesics on the development of delirium following hip fracture. J. Gerontol. A Biol. Sci. Med. Sci. 2003, 58, 76–81. [Google Scholar] [CrossRef] [PubMed]
- Finkelstein, E.; Prabhu, M.; Chen, H. Increased prevalence of falls among elderly individuals with mental health and substance abuse conditions. Am. J. Geriatr. Psychiatry 2007, 15, 611–619. [Google Scholar] [CrossRef] [PubMed]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders: DSM-5, 5th ed.; American Psychiatric Association: Arlington, VA, USA, 2013. [Google Scholar]
- Bo, M.; Bonetto, M.; Bottignole, G.; Porrino, P.; Coppo, E.; Tibaldi, M.; Ceci, G.; Raspo, S.; Cappa, G.; Bellelli, G. Length of stay in the emergency department and occurrence of delirium in older medical patients. J. Am. Geriatr. Soc. 2016, 64, 1114–1119. [Google Scholar] [CrossRef] [PubMed]
- Gray, L.C.; Peel, N.M.; Costa, A.P.; Burkett, E.; Dey, A.B.; Jonsson, P.V.; Lakhan, P.; Ljunggren, G.; Sjostrand, F.; Swoboda, W.; et al. Profiles of older patients in the emergency department: Findings from the interRAI Multinational Emergency Department Study. Ann. Emerg. Med. 2013, 62, 467–474. [Google Scholar] [CrossRef] [PubMed]
- Shah, M.N.; Jones, C.M.C.; Richardson, T.M.; Conwell, Y.; Katz, P.; Schneider, S.M. Prevalence of depression and cognitive impairment in older adult emergency medical services patients. Prehosp. Emerg. Care 2011, 15, 4–11. [Google Scholar] [CrossRef] [PubMed]
- Schnitker, L.; Martin-Khan, M.; Burkett, E.; Beattie, E.; Jones, R.; Gray, L. Process quality indicators targeting cognitive impairment to support quality of care for older people with cognitive impairment in emergency departments. Acad. Emerg. Med. 2015, 22, 285–298. [Google Scholar] [CrossRef] [PubMed]
- White, C.; Katz, B. Position Statement 21: Pain in Older People. 2012. Available online: http://www.anzsgm.org/documents/PositionStatementNo21PaininOlderPeople_000.pdf (accessed on 5 May 2017).
- Fox, P.; Solomon, P.; Raina, P.; Jadad, A.R. Barriers and facilitators in pain management in long-term care institutions: A qualitative study. Can. J. Aging 2004, 23, 269–280. [Google Scholar] [CrossRef] [PubMed]
- Schnitker, L.M.; Beattie, E.R.A.; Martin-Khan, M.; Burkett, E.; Gray, L.C. Characteristics of older people with cognitive impairment attending emergency departments: A descriptive study. Australas. Emerg. Nurs. J. 2016, 19, 118–126. [Google Scholar] [CrossRef] [PubMed]
- Fry, M.; Chenoweth, L.; MacGregor, C.; Arendts, G. Emergency nurses perceptions of the role of family/carers in caring for cognitively impaired older persons in pain: A descriptive qualitative study. Int. J. Nurs. Stud. 2015, 52, 1323–1331. [Google Scholar] [CrossRef] [PubMed]
- Wells, N.; Pasero, C.; McCaffery, M. Improving the quality of care through pain assessment and management. In Patient Safety and Quality: An Evidence-Based Handbook for Nurses; Hughes, R., Ed.; Agency for Healthcare Research and Quality: Rockville, MD, USA, 2008. [Google Scholar]
- Pasero, C.; McCaffery, M. No self-report means no pain-intensity rating: Assessing pain in patients who cannot provide a report. Am. J. Nurs. 2005, 105, 50–53. [Google Scholar] [CrossRef] [PubMed]
- Pautex, S.; Michon, A.; Guedira, M.; Emond, H.; Lous, P.L.; Samaras, D.; Michel, J.P.; Herrmann, F.; Giannakopoulos, P.; Gold, G. Pain in severe dementia: Self-assessment or observational scales? J. Am. Geriatr. Soc. 2006, 54, 1040–1045. [Google Scholar] [CrossRef] [PubMed]
- Van Herk, R.; Van Dijk, M.; Biemold, N.; Tibboel, D.; Baar, F.P.M.; De Wit, R. Assessment of pain: Can caregivers or relatives rate pain in nursing home residents? J. Clin. Nurs. 2009, 18, 2478–2485. [Google Scholar] [CrossRef] [PubMed]
- Pierik, J.G.J.; Ijzerman, M.J.; Gaakeer, M.I.; Vollenbroek-Hutten, M.M.R.; Doggen, C.J.M. Painful discrimination in the emergency department: Risk factors for underassessment of patients’ pain by nurses. J. Emerg. Nurs. 2017, 43, 228–238. [Google Scholar] [CrossRef] [PubMed]
- Kamel, H.K.; Phlavan, M.; Malekgoudarzi, B.; Gogel, P.; Morley, J.E. Utilizing pain assessment scales increases the frequency of diagnosing pain among elderly nursing home residents. J. Pain Symptom Manag. 2001, 21, 450–455. [Google Scholar] [CrossRef]
- Jennings, P.A.; Cameron, P.; Bernard, S. Measuring acute pain in the prehospital setting. Emerg. Med. J. 2009, 26, 552–555. [Google Scholar] [CrossRef] [PubMed]
- Lichtner, V.; Dowding, D.; Esterhuizen, P.; Closs, S.J.; Long, A.F.; Corbett, A.; Briggs, M. Pain assessment for people with dementia: A systematic review of systematic reviews of pain assessment tools. BMC Geriatr. 2014, 14, 138. [Google Scholar] [CrossRef] [PubMed]
- Fry, M.; Arendts, G.; Chenoweth, L.; Macgregor, C. Cognitive impairment is a risk factor for delayed analgesia in older people with long bone fracture: A multicenter exploratory study. Int. Psychogeriatr. 2015, 27, 323–328. [Google Scholar] [CrossRef] [PubMed]
- Fry, M.; Chenoweth, L.; Arendts, G. Assessment and management of acute pain in the older person with cognitive impairment: A qualitative study. Int. Emerg. Nurs. 2016, 24, 54–60. [Google Scholar] [CrossRef] [PubMed]
- Holdgate, A.; Shepherd, S.A.; Huckson, S. Patterns of analgesia for fractured neck of femur in Australian emergency departments. Emerg. Med. Australas. 2010, 22, 3–8. [Google Scholar] [CrossRef] [PubMed]
- Herr, K. Pain in the older adult: An imperative across all health care settings. Pain Manag. Nurs. 2010, 11 (Suppl. 2), S1–S10. [Google Scholar] [CrossRef] [PubMed]
- Herr, K.; Coyne, P.J.; Key, T.; Manworren, R.; McCaffery, M.; Merkel, S.; Pelosi-Kelly, J.; Wild, L. Pain assessment in the nonverbal patient: Position statement with clinical practice recommendations. Pain Manag. Nurs. 2006, 7, 44–52. [Google Scholar] [CrossRef] [PubMed]
- Nelson, B.P.; Cohen, D.; Lander, O.; Crawford, N.; Viccellio, A.W.; Singer, A.J. Mandated pain scales improve frequency of ED analgesic administration. Am. J. Emerg. Med. 2004, 22, 582–585. [Google Scholar] [CrossRef] [PubMed]
- Herr, K.; Titler, M. Acute pain assessment and pharmacological management practices for the older adult with a hip fracture: Review of ED trends. J. Emerg. Nurs. 2009, 35, 312–320. [Google Scholar] [CrossRef] [PubMed]
- McDermott, J.H.; Nichols, D.R.; Lovell, M.E. A case-control study examining inconsistencies in pain management following fractured neck of femur: An inferior analgesia for the cognitively impaired. Emerg. Med. J. 2014, 31, e2–e8. [Google Scholar] [CrossRef] [PubMed]
- Boccio, E.; Wie, B.; Pasternak, S.; Salvador-Kelly, A.; Ward, M.F.; D’Amore, J. The relationship between patient age and pain management of acute long-bone fracture in the ED. Am. J. Emerg. Med. 2014, 32, 1516–1519. [Google Scholar] [CrossRef] [PubMed]
- Daoust, R.; Paquet, J.; Lavigne, G.; Sanogo, K.; Chauny, J.M. Senior patients with moderate to severe pain wait longer for analgesic medication in EDs. Am. J. Emerg. Med. 2014, 32, 315–319. [Google Scholar] [CrossRef] [PubMed]
- Quattromani, E.; Normansell, D.; Storkan, M.; Gerdelman, G.; Krits, S.; Pennix, C.; Sprowls, D.; Armbrecht, E.; Dalawari, P. Oligoanalgesia in blunt geriatric trauma. J. Emerg. Med. 2015, 48, 653–659. [Google Scholar] [CrossRef] [PubMed]
- Hwang, U.; Richardson, L.D.; Sonuyi, T.O.; Morrison, R.S. The effect of emergency department crowding on the management of pain in older adults with hip fracture. J. Am. Geriatr. Soc. 2006, 54, 270–275. [Google Scholar] [CrossRef] [PubMed]
- Chibnall, J.T.; Tait, R.C. Pain assessment in cognitively impaired and unimpaired older adults: A comparison of four scales. Pain 2001, 92, 173–186. [Google Scholar] [CrossRef]
- Feldt, K.S.; Ryden, M.B.; Miles, S. Treatment of pain in cognitively impaired compared with cognitively intact older patients with hip-fracture. J. Am. Geriatr. Soc. 1998, 46, 1079–1085. [Google Scholar] [CrossRef] [PubMed]
- Moschinski, K.; Kuske, S.; Andrich, S.; Stephan, A.; Gnass, I.; Sirsch, E.; Icks, A. Drug-based pain management for people with dementia after hip or pelvic fractures: A systematic review. BMC Geriatr. 2017, 17, 1–15. [Google Scholar] [CrossRef] [PubMed]
- Fuchs-Lacelle, S.; Hadjistavropoulos, T.; Lix, L. Pain assessment as intervention: A study of older adults with severe dementia. Clin. J. Pain 2008, 24, 697–707. [Google Scholar] [CrossRef] [PubMed]
- Iyer, R.G. Pain documentation and predictors of analgesic prescribing for elderly patients during emergency department visits. J. Pain Symptom Manag. 2011, 41, 367–373. [Google Scholar] [CrossRef] [PubMed]
- Provost, J.C. Adoption of a pain assessment tool in older homebound patients with dementia in a housecall practice: A dissemination study. Clin. Sch. Rev. 2012, 5, 124–131. [Google Scholar] [CrossRef]
- Dunwoody, C.J.; Krenzischek, D.A.; Pasero, C.; Rathmell, J.P.; Polomano, R.C. Assessment, physiological monitoring, and consequences of inadequately treated acute pain. J. Perianesth. Nurs. 2008, 9 (Suppl. 1), 11–27. [Google Scholar] [CrossRef]
- Erel, M.; Shapira, Z.; Volicer, L. Behavioral problems of seniors in an emergency department. J. Emerg. Med. 2013, 45, 13–18. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Authors | Design | Size | Setting | Findings |
|---|---|---|---|---|
| Fry, Chenoweth, and Arendts (2016) [35] | Focus group interviews, qualitative | 80 emergency nurses, 16 focus groups | Four Australian EDs | Nurses reported that visual or verbal analogue scales for pain assessment are often unsuitable in cognitively impaired patients. When these methods failed, nurses relied on clinical judgement and physiological measures (e.g., respiratory rate) rather than standardised observational pain assessment tools. |
| Fry, Arendts, Chenoweth, and MacGregor (2015) [34] | Retrospective cross-sectional study of patient ED records | 255 elderly patients with long bone fractures | Four Australian EDs | Only 68% of patients had a pain score during their ED admission. The verbal analogue scale was routinely used. There was no evidence that ED staff used tools designed specifically for cognitively impaired people. 204 of 255 patients received analgesia in the ED. A cognitively impaired patient was not more likely to receive no analgesia compared with a cognitively intact patient. Median wait time to analgesia was 72 min for cognitively intact patients compared with 149 min for cognitively impaired patients. |
| Holdgate, Shepherd, and Huckson (2010) [36] | Retrospective cross-sectional study of patient ED records | 646 patients with fractured neck of femur | 36 EDs across 5 Australian states | Confusion/dementia was reported as a barrier to analgesia in 42 out of the 99 patients who had a barrier recorded. 47% of patients had no documented pain score during their ED admission. Visual analogue scales, verbal numerical pain scores and Likert scales were used. |
| McDermott, Nichols, and Lovell (2014) [41] | Retrospective cross-sectional study of patient ED records | 224 patients with fractured neck of femur | Wythenshawe Hospital ED, Manchester, United Kingdom. | A pain score was documented for 45% of cognitively impaired patients compared with 75% of cognitively intact patients. 45% of cognitively impaired patients were not offered an analgesic while only eight percent of cognitively intact patients had no prescribed analgesia. |
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jones, J.; Sim, T.F.; Hughes, J. Pain Assessment of Elderly Patients with Cognitive Impairment in the Emergency Department: Implications for Pain Management—A Narrative Review of Current Practices. Pharmacy 2017, 5, 30. https://doi.org/10.3390/pharmacy5020030
Jones J, Sim TF, Hughes J. Pain Assessment of Elderly Patients with Cognitive Impairment in the Emergency Department: Implications for Pain Management—A Narrative Review of Current Practices. Pharmacy. 2017; 5(2):30. https://doi.org/10.3390/pharmacy5020030
Chicago/Turabian StyleJones, Joshua, Tin Fei Sim, and Jeff Hughes. 2017. "Pain Assessment of Elderly Patients with Cognitive Impairment in the Emergency Department: Implications for Pain Management—A Narrative Review of Current Practices" Pharmacy 5, no. 2: 30. https://doi.org/10.3390/pharmacy5020030