Provision of Integrated Early Childhood Development in Namibia: Are We on the Right Track?


1
Social Science Division, Multi-disciplinary Research Center, University of Namibia, Windhoek 12007, Namibia
2
Department of Mathematics, Science and Sport Education, Faculty of Education, Windhoek Campus, University of Namibia, Windhoek 12007, Namibia
*
Author to whom correspondence should be addressed.
Educ. Sci. 2018, 8(3), 117; https://doi.org/10.3390/educsci8030117
Submission received: 20 June 2018
/
Revised: 31 July 2018
/
Accepted: 1 August 2018
/
Published: 7 August 2018
Abstract
:The provision of Integrated Early Childhood Development (IECD) positively impacts children’s futures physically, cognitively, emotionally and socially. The assessment sought to inform intervention programs to improve the status of children’s physical, social-emotional, cognitive and educational needs, as well as their health and nutritional needs. A mixed method approach was used to collect data: a survey and multiple case studies through interviews with 32 caregivers were conducted and focus group discussions were held with community members. The findings show that the Early Childhood Development (ECD) centers lacked the essential prerequisites for the provision of quality IECD education as per the requirements stipulated in the Adapted Theory of Change (ATC). The study recommends formation of smart partnerships in providing integrated childhood development services at ECD centers to meet their health, sanitation, nutritional, physical, socio-emotional and cognitive needs.
1. Introduction
Access to Integrated Early Childhood Development (IECD) is a very important building block toward productive and responsible citizenry, a notion supported by the Namibian constitution [1]. Namibia has adopted IECD as a prerequisite to successfully provide quality primary school education. Therefore, the proliferation of Early Childhood Development (ECD) centers should be encouraged, within the guidelines developed by the Ministry of Gender, Equality and Child Welfare (MGECW), to ensure a quality ECD environment and subsequently contribute to the general education system in the country [2].
To date, Namibia experiences highly skewed income distribution and resource allocation along not only racial lines, but also biased against rural communities, who make up most of the population (54%) [3]. The majority of ECD centers are community-based and informal or not registered with the MGECW. An ECD center is a facility that provides education and care to children in the temporary absence of their parents in a holistic manner by tending to their health, nutrition, education, psychological development and other needs [4]. According to [5], the centers are supposed to serve as a safe area for children to play; provide adequate space and ventilation; safe drinking water; hygienic and adequate toilet facilities; a hygienic area for the preparation of food for the children; and appropriate first aid supplies. In addition, the center should provide a secure environment. Provision of ECD to children in a holistic manner and incorporating health, nutrition, water and sanitation, education and interventions that support their full development is crucial. MGECW ([6], p. 5) notes that ECD is “… foundational to the overall development of children and their success in education”. This view is in line with the global perspective on the importance of ECD as a building block for further education and for nations to achieve equitable socio-economic progress and sustainable development [7]. In the same vein, significant investment and numerous efforts to strengthen education and skills have been made [3] although the Namibian education system is still perceived as performing below its potential and quality ECD provision is viewed as the solution to low learner performance in schools [6]. Ironically, the ECD centers are funded and maintained by the communities within which they are located, with little assistance from the MGECW provided they meet certain standards before the caregiver is provided with an allowance of N$ 1500.00 to N$ 3000.00, depending on their qualification and training [8]. Children in Africa are said to be vulnerable and mostly affected by various factors such as: environmental, geographic, political, economic and cultural [9,10]. The provision of ECD services to rural communities may lead to higher achievement scores, completion rate in subsequent years of schooling, and reduce criminal activities. Therefore, investments in ECD must begin from birth and should include health, nutrition and attention to cognitive and social development to take children up to the transition into primary school [9]. Without adequate understanding of ECD services to rural areas, as a baseline, the Namibian government will continue to disadvantage these communities to develop a quality IECD program. Evaluating ECD provision is necessary to obtain comparatively the extent to which the country is providing quality IECD and related services, especially to the vulnerable communities. Therefore, this study sought answers to the following research question: Is the Namibian government providing an adequate ECD services to rural communities?
2. Literature Review
According to the Child Care Protection Act [5], the first 1000 days of life are very important for the child’s growth. These days are important because they form the foundation for health, skills development and affectionate human relationships in the child’s later life. Therefore, the first two years of a child’s life are important, and the child should be exposed to a rich social environment that enhances his/her development intellectually and physically. To achieve a rich social environment, an integrated “multi-sectoral life-cycle approach is essential in giving children the best start in life” ([5], p. 5). In line with the social environment, ECD is therefore defined by developmental theorists as the gradual emergence and development of sensory-motor, cognitive, language, and social-emotional capacities in young children of 0–8 years [11,12]. In this study, ECD refers to more than mere schooling and the cognitive development of children. It focuses on the potential of ECD centers to enhance multiple interdependent dimensions of a child’s life; including health and safety, nutrition, emotional well-being, and social competence [13]. These domains affect the development of any child differently depending on the environment surrounding the child e.g., the home, family, community and early secondary socialization such as the ECD center, school or other community social arenas. It refers to what is happening within the child, and to the care that children require to thrive. For a child to develop and learn in a healthy and normal way, it is important to meet the basic needs of food, health, protection, interaction and stimulation, affection, and learning through exploration and discovery [11,12].
Since growth and development take place at a very fast rate, unfavorable experiences such as lack of nutrition, health care, nurturance, stimulation, and unhealthy living conditions may hinder development to a considerable extent [7,14]. Inadequate nutrition at birth and in the first years of life can seriously interfere with brain development and lead to neurological and behavioral disorders which may result in learning disabilities. In the same way, favorable conditions foster development. The effect of enrichment or deprivation is long-lasting since the foundation of development for later years is laid at this age [14]. In line with this, several studies have found that positive early experiences and interactions are vital in the development of the child in achieving quality learning [15,16,17]. It is, therefore, important that in the provision of a quality ECD program, all stakeholders need to be actively involved in the day-to-day activities of ECD centers in their communities.
The Department of Social Development [4] in South Africa found that ECD was dominated by females aged below 30 years. Caregivers at the ECD center joined the profession due to lack of suitable qualifications and unemployment. Hence, qualifications of the caregivers are generally low, and some have no formal qualifications. Further, the report highlights the general lack of support with respect to hiring assistant caregivers and reluctance to increase subsidies to the ECD centers. Researchers [8] found that in Namibia, there is a lack of quality ECD education and services. Many centers operate in the open with: no structures, no qualified caregivers, and a few safe playgrounds, lack of appropriate materials and supplies, and food insecurity at the ECD centers [8]. Further, very few of the ECD centers provide food in the form of grains and milk to the children [8]. This has resulted in many children being malnourished, and the situation is perpetual, since even if the child receives medical attention, he/she is returned to the same environment. The survey conducted by the Ministry of Health and Social Services (MoHSS) and International Classification of Functional Disabilities and Health (ICF) found that twenty-four percent of children under the age of 5 from poor households had stunted growth and 8% are severely stunted [18]. To address the factors that hinder provision of IECD in Namibia, this study adopted the School Readiness Theory of Change Outcomes Framework for Some Cities of Pennsylvania [19]. The School Readiness Theory is gaining currency as a strategy in closing the learning gap between children from well-to-do families and those from poor homes. This in turn brings about educational equity in achieving full developmental potential of all children regardless of their home background. The theory supports and promotes policies and programs that enhance early learning and the creation of opportunities for inclusiveness. Further, the theory assumes that the acquisition of positive social and behavioral competences enhances primary school readiness and subsequent secondary school learners’ performance [20].
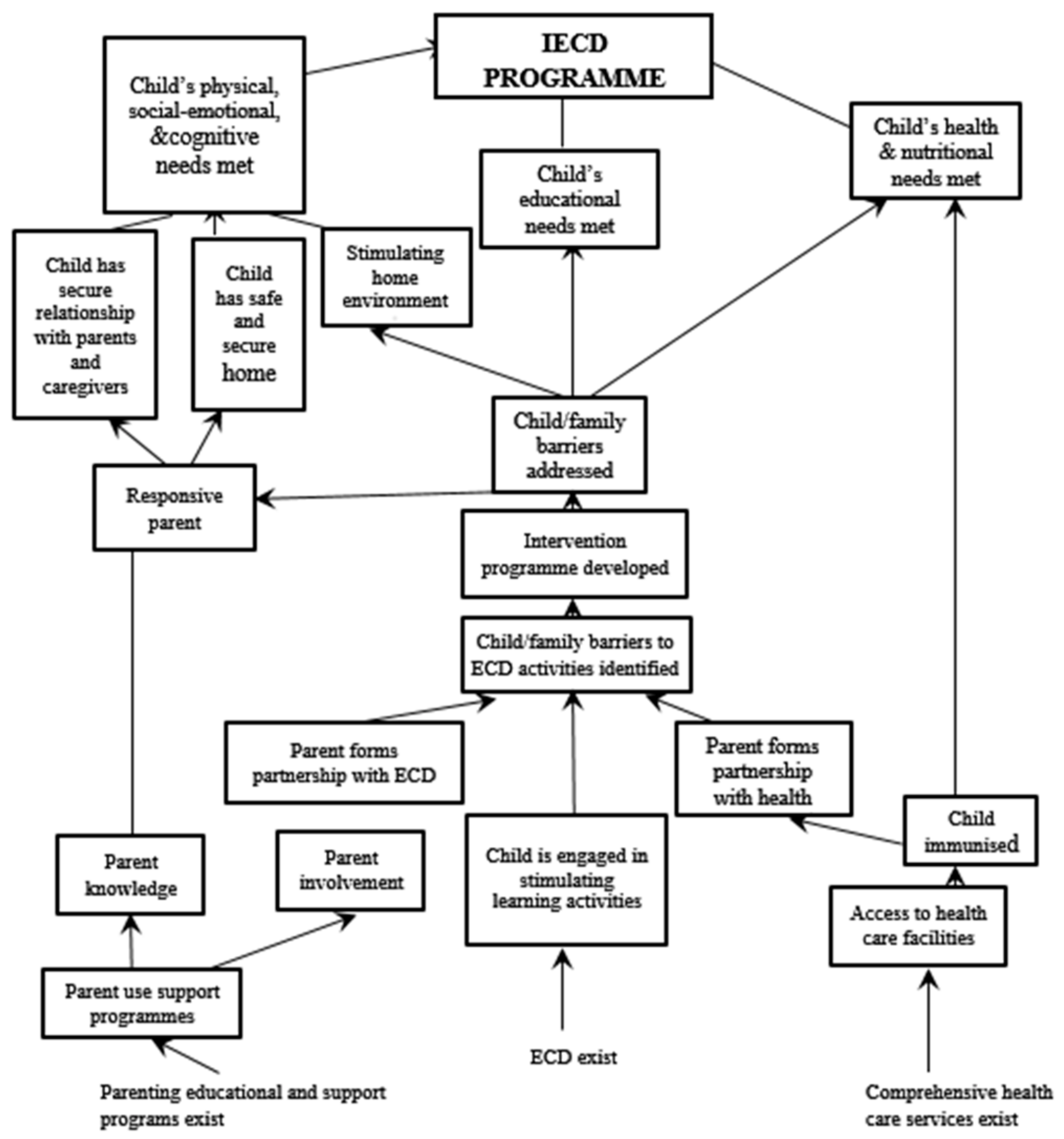
Furthermore, the theory recognizes that change is required at community, system and program levels to achieve its goal of achieving full developmental potential of all children and therefore require innovative programs and more effective approaches to fill the gaps of identified needs and system improvements. This theory was embraced for this needs assessment to try and identify the needs of the selected thirty-two ECD centers with respect to community engagement and to achieve an effective IECD program for children in Namibia. Also, the location of the identified centers is remote without basic services and depends on the community involvement for their operations. The adapted version of the theory is depicted in Figure 1.
Figure 1 [21] depicts the logical connections between the identified needs of the 32 ECD centers and communities and strategies to be employed to achieve the IECD Program. Figure 1 shows factors that may have effects on children’s growth and development, which should be taken into consideration when implementing interventions that are necessary to achieve an effective IECD Program. The adapted Theory of Change is important to this needs assessment because it emphasizes the importance of a child’s needs in terms of physical, social-emotional and cognitive needs, educational as well as nutritional needs necessary to get the child ready for school and subsequently succeed in life. Specifically, the theory emphasizes the following skills acquisition, namely: age appropriate self-regulatory skills, positive relationship with peers and adults, emergent literary and numeracy competencies, confident and excitement about learning, familiarity with school culture and health. Therefore, the research question: To what extent is the provision of IECD on track, especially among rural communities in Namibia?
3. Methodological Approach
This study followed a mixed method using quantitative and qualitative approaches, employing a multiple case studies design [22]. The use of quantitative and qualitative research was required to complement each other to obtain a comprehensive or holistic picture of the ECD centers [20].
3.1. Instruments
The quantitative component used a questionnaire that comprised both open and close-ended questions on the background information, teaching aids and skills development; health, safety and nutritional measures; and positioning of basic amenities. The qualitative component used the observation Check List, Interview Guide and Focus Group Discussions. Specifically, the observation checklist focused on: physical structure, facilities and classroom environment and physical infrastructure, including physical status of playrooms, child-sized furniture, play learning materials, curriculum and learning strategies to guide the teaching activities, feeding programs, safety and protection precautions, caregiver-child ratio, and availability of water and sanitation. The observation checklist also included statements on caregiver and learner behavior, and classroom climate for learning. An interview guide for the ECD caregivers dealt with the understanding of ECD concept, services provided to children with disabilities, teaching and challenges faced. Focus Group Discussions (FGDs) focused on issues related to nutrition, health, hygiene, environment and any other issues that affected the ECD center, including; the physical appearance of the ECD centers which was used later in this study to classify the ECD centers, level of participation and care at the centers.
3.2. Population and Sample
There are two thousand nine hundred and thirty-four (2934) ECD centers registered with the MGECW across Namibia offering ECD services [23].
The study employed the typical case sampling technique. The sample is illustrative of typical rural-based ECD centers which are remote and; located in a classified poor rural constituency; and poorly resourced and registered with MGECW. Based on the criteria described, a sample of thirty-two communities within which the ECD centers are located was identified. For purposes of analysis, the sample was divided into three communities as follows: Community A was located within the school premises and closer to urban areas; Community B was located within the informal settlements and the ECD centers are made of corrugated iron sheets; and Community C was located within the poor rural constituencies and had mud structures. A total of 32 caregivers and 10 community members including educational stakeholders participated at every site.
3.3. Methods
This study was conducted during 2016–2017. Data was collected by researchers. Thirty-two caregivers were asked to fill in the questionnaire with guidance from the researchers. Further, the researchers directly observed the caregivers undertaking lessons and or any other activities for at least three hours. The direct observations were recorded using an observational form. The Regional Liaison Officer at the MGECW was also requested to invite at least 10 members of the community which included parents, caregivers, ECD Committee members, community health workers, Village Councilor, Town Council representative, and chiefs or village headmen to attend the focus group discussions. The focus group discussions lasted for at least an hour at ECD centers. These discussions were recorded, and the researchers also took notes during the FGDs. Face-to-face interviews were carried out with the caregivers and ECD Committee members as well as other stakeholders at the selected ECD centers. The participants were encouraged to respond in the language they felt more comfortable with. In some cases, the researchers and the Community Liaison Officers from the MGECW acted as translators when the need arose. Interviews and focus group discussions were recorded and later transcribed verbatim. Ethical clearance was granted by the MGECW which is the custodian of the ECD Program in Namibia.
3.4. Data Analysis
The quantitative data was analyzed using the Statistical Package for Social Sciences (SPSS) in generating descriptive statistics such as frequency counts and percentages to provide the number of caregivers, types and levels of their qualifications, and number of children at ECD centers. Further, the qualitative data was analyzed case by case using Atlas.ti to generate content that would illuminate key issues to be considered in the improved IECD Program. The responses were then collated under three themes identified as per the School Readiness Theory, namely: child’s physical, social-emotional and cognitive needs, educational needs, and health and nutritional needs. Further, the results are described under the constructs per the three categories of communities.
4. Results
The biographical information of the caregivers and children is presented below:
All the ECD centers were community owned and 25 of the 32 centers were established before 2010, while 4 were established before 2013 and the remaining 3 were established between 2014 and 2015. Twenty-eight out of the 32 caregivers were female while the rest were male. Information about the total number of children attending the ECD centers is presented in Table 1.
Table 1 presents the number of children per community as well as the qualifications of ECD caregivers. The total number of children is highest in Community C (531) than it is in Community B (453) and A (51). On average, a class had a maximum of 32 children aged between 0 and 5 and above, depending on the location. All caregivers had some form of qualification; either formal qualification and/or an additional qualification. Of those who indicated their qualifications, only one caregiver had a tertiary education qualification. All caregivers except for two did not indicate a qualification or training, had at least a Grade 10 education (higher than the minimum Grade 6 required), but 8 of them did not indicate having participated in the MGECW’s 7-week ECD course. It is worth noting that the 7 weeks basic training comprises 14 themes, including: foundation of ECD; Nutrition and health, hygiene and sanitation, children’s rights, child development stages, behavior and discipline, children with special needs and community engagement (MGECW, 2009). Caregivers in Communities A and B had undergone at least a seven- week training on the concept of ECD and understood it to mean a developmental phase of a child in terms of social, physical and moral development, while their counterparts in Community C understood it as to teach the child. Accordingly, caregivers rendered their services based on their understanding of the concept.
4.1. Physical, Social-Emotional and Cognitive Needs
The observation results indicated that children were eager to learn and participated actively in all activities. Children at all the ECD centers had attained physical competence of running, climbing, jumping, and swinging among others. The provision of playgrounds and child friendly equipment were observed only in Community A ECD centers. In other communities, the physical competence was limited to running and jumping due to lack of playground and the necessary equipment. Four children in Community C were found to have some form of disability but the support offered to those children was limited to identifying them and making appropriate referrals for expert assessment and treatment. None of the centers were equipped with the necessary materials for these children. In addition, the caregivers advised the affected community members to register vulnerable children with the MGECW in order for them to obtain the necessary support services. Also, different languages other than home languages were being used as media for communication at the centers. Caregivers in Communities A and B used mostly English and another local language that was dominant while Community C used their local languages to teach the children. It was observed that caregivers were not fluent in English and taught narrowly what they knew. In addition, caregivers were observed to be establishing an orderly learning environment; and communicating in a fair, firm and consistent manner at the level of the children; giving clear instructions; and moving around the room to monitor children. The observed interactions enabled the children to establish a good relationship with their peers.
4.2. Educational Needs
Children showed familiarity with the school environment and culture in the sense that they knew and followed the curriculum as presented by the caregivers. For example, they followed the classroom routine of reading, counting, in-between activity breaks and playtime. Children were observed putting up their hands and standing up when responding to the caregiver. This shows that children had attained self-regulatory skills. These behaviors and patterns were observed in all ECD centers.
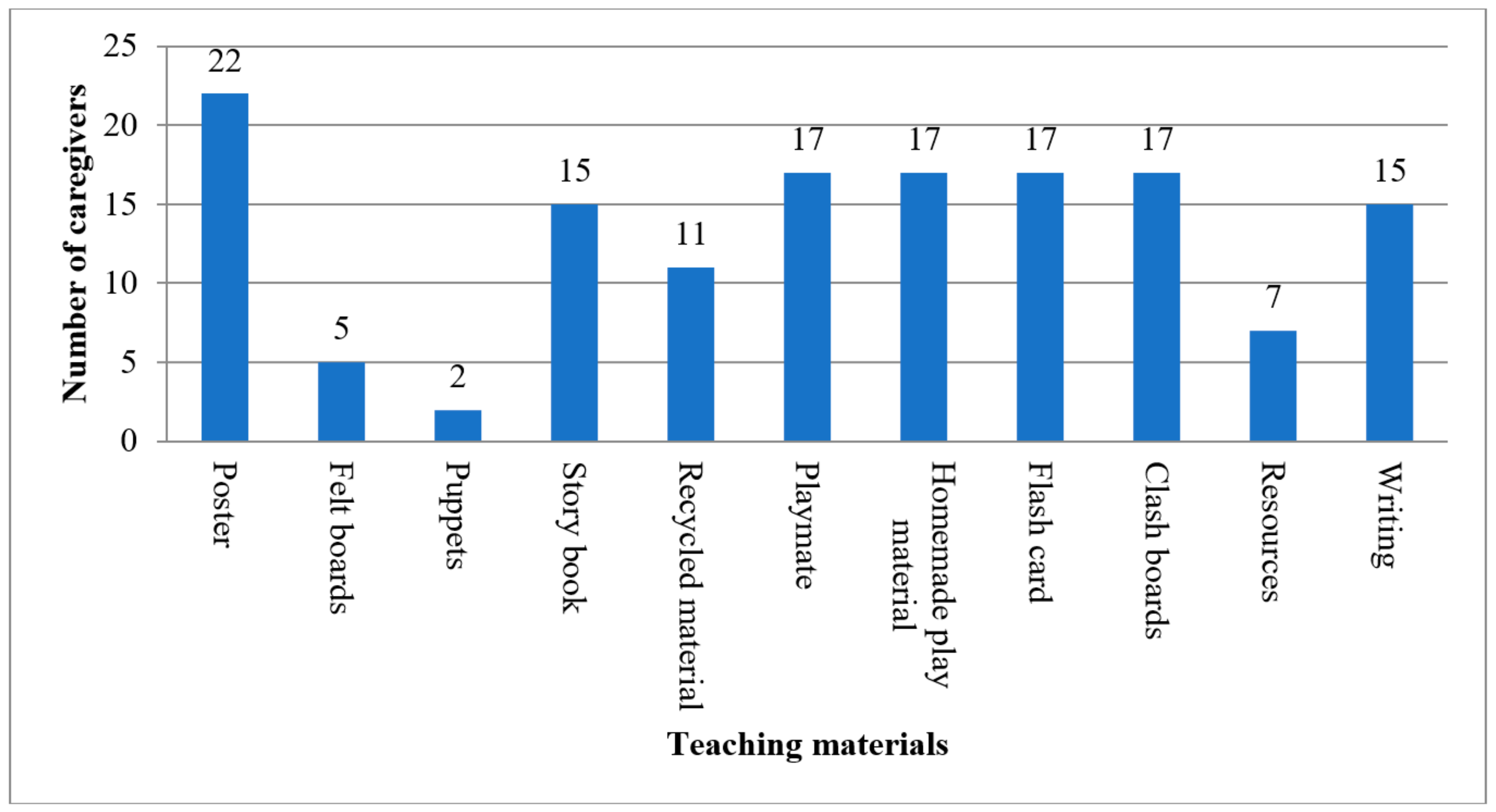
Caregivers from category B and C communities indicated that they did not have a curriculum to teach from and had less teaching resources, unlike centers in Community A which are better resourced as indicated earlier. Thus, Community A centers had at least copies of the 7-week training curriculum the caregivers were teaching from. Some caregivers in Communities B and C used their intuition to teach the children in the absence of the curriculum and used the following teaching resources as presented in Figure 2.
Figure 2 shows that commonly available teaching resources were posters; playmate, homemade materials, flash cards, clash boards; story books and writing, drawing or painting equipment; and recycled materials in that order. In addition, children sang more and had story telling as learning activities, portraying low capabilities.
A small group of community members from Communities B and C expressed ignorance of what children learn at the centers. This impression came from parents and grandparents who were not educated and could not read and write. However, they trusted that whatever their children learnt was the right content. On the other hand, some community members from Community A were skeptical with content taught to the children, indicating that there was no chronological order. The latter group also cited the lack of the ECD Policy and ECD Curriculum documents at these centers as a concern, as children might not be taught key concepts and skills. Further, the results show that caregivers at all communities were enthusiastic and interested in children’ activities (68.75%); and knew and used children’s names (75%); acknowledged children for contributions that deserved commendation (59.38%) and treated children equally (62.5%). Also, the caregivers used authority in creating an environment safe and conducive for learning (56.25%); recognized when children did not understand (59.38%); spoke warmly to the children (65.63%); listened attentively when children spoke to her/him (65.63%); enjoyed being with the children (71.88%); showed enthusiasm about the children’s activities and efforts (62.5%). In addition, the caregivers talked to children on a level they understood (75%); exercised firmness when necessary (62.5%).); supervised children very closely (65.63%); when talking to children, knelt, bent, or sat at their level to establish better eye contact (65.63%). On the contrary, some caregiver seemed unnecessarily harsh (65.63%); and spoke with irritation or hostility to the children (62.5%). Caregivers also tried to exercise a lot of control over children (62.5%); and spoke with irritation or hostility to the children (56.25%). A few caregivers threatened children in trying to control them (50%).
It should be pointed out also that during the reading activity the ECD caregivers tended to read to the children and then asked the children questions that reflected what they had read. This was done to find out whether the children had grasped what had been read to them. It was found that the responses given by the children showed that they had followed the story as read to them. In one center, the children were awarded certificates to show that they had all performed at the expected level according to the caregiver. In addition, caregivers used stone and bottle tops to teach basic numeracy, specifically counting.
4.3. Health and Nutritional Needs
It was noted that when a child became ill at the ECD center, the caregiver would notify the parents, who would then come to collect the child. Likewise, if a child became ill at home, the parents would notify the caregiver about the absence of the child. However, parents were responsible for illnesses or vaccinations. For Communities A and B, a mobile clinic visited the communities monthly but not specifically at the ECD centers. However, parents could take their children for treatment and vaccination. For Community C, hospitals were approximately 30 km away, as a result these centers depended on bi-monthly visit from health workers for observations and minor treatments. None of the centers were equipped with first aid kits. Children from Community C would come to the center hungry and appeared sick because of lack of food. Nevertheless, at most centers hand washing was promoted before meals and after the use of the toilet, and children dried their hands with towels. In general, none of the centers exhibited negative personal care routines and practices, which might critically impact the children’s health and hygiene.
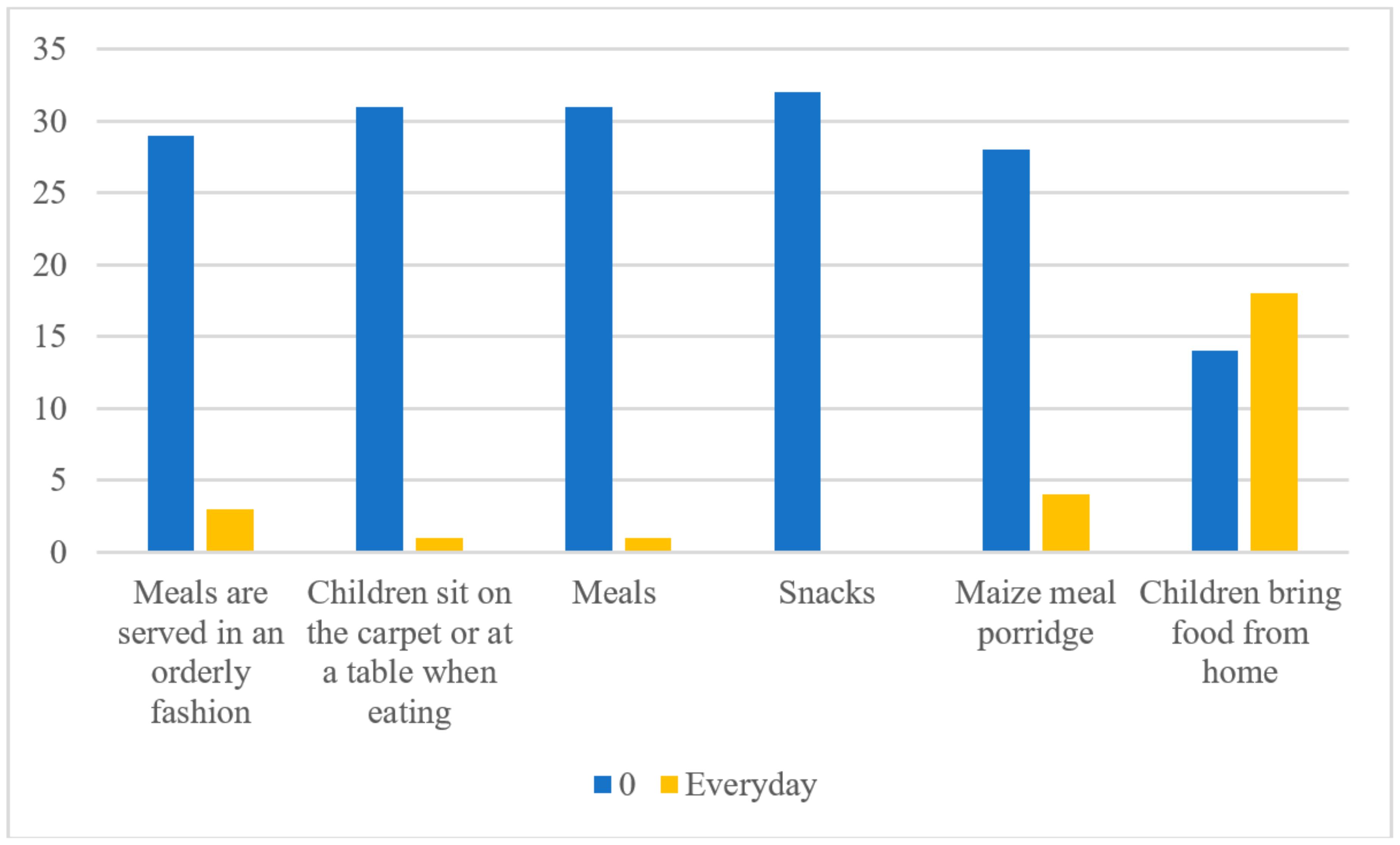
Regarding food provision, most centers did not serve any meals to the children. They had their meals at home after day care (Figure 3).
Figure 3 shows that at 18 ECD centers, children brought food from home and less than 5 centers served food. However, at 3 centers in Community A, children received food every day in a form of maize meal porridge, which was served in an orderly fashion and one center had a carpet for children to sit on as they ate their meals. Some ECD centers in Communities A and B, depended on the School Principal’s discretion to provide them with food under the School Feeding Program (SFP). In essence, parents were responsible for providing food to their children. Parents in Community C depended on the Drought Relief Program (DRP) for provision of food for their children. None of the centers had proper storage for food and shelves to keep utensils (cups, spoons, pots, etc.). Further, the community members at the specific centers that served food observed that the maize from the SFP was infested with weevils and needed to be sieved before use, but they had no means to do so. The caregivers explained that the supply of food at the ECD centers increased attendance. Thus, children who do not eat before coming to the ECD center might show signs of malnutrition and may risk failure of cognitive and physical development.
5. Discussion
The physical structures of most ECD centers were in a poor and dilapidated state and this might impact the quality of the ECD delivery service. These centers were owned by poor communities who could not develop them. To worsen the situation, these communities lacked basic infrastructure and services such as running water, access to electricity or suitable sanitation which might impact negatively on children’s health and subsequently their education. According to the Guidelines, ECD centers should comply with sanitation and health requirements [2]. The World Health Organization has established that ECD services have positively impacted children’s lives through the provision of health services such as Prevention of Mother to Child Transmissions (PMTCT), treatment services, child protection and health screening [8]. However, given the fact that the centers were owned and run by poor rural communities, standards were not met. This finding is similar to that of [8,20,21] who concluded that since most ECD centers were community owned they did not have the necessary means to build and support proper structures to enhance children’s readiness for primary school.
Further, it was found that most ECD centers in the rural areas did not have ‘formal’ structures and ECD activities were being conducted in the open, sometimes next to Cuca shops affecting children’s concentration abilities [7]. This seems to indicate that ECD centers are being ‘constructed’ and/or conducted without applying the general standard guidelines [1], disadvantaging children from the rural areas. Nevertheless, evidence shows these ECD centers continue to grow, for example in Malawi, ECD improved access grew from 2% in 1999 to 32% in 2009 [8] and if not supported, this might have a detrimental effect on the children’s education later in life even though communities show positive attitudes toward the existing ECD services under conditions of hardship. Such a situation is contrary to the school readiness notion that an effective school readiness program is important for the provision of basic foundations for children’s later development and success in school [24]. Notably, there is general lack of monitoring and evaluation of the ECD centers, as some of them would not be authorized to operate given their current state. This situation is contrary to the plight of providing equal educational opportunities to the Namibian children [22]. Further, these researchers stress the need for inclusive societies, where every child should be provided with equitable access to schooling and quality education [22]. Nevertheless, the caregivers could only offer services within their knowledge and means given the fact that the said communities lacked most of the basic services and therefore efficiency in terms of service delivery is non-existent.
The academic qualifications of ECD caregivers are below standard and hence their various interpretation of the ECD concepts. This indicates that the caregivers do not follow a common curriculum, nor do they possess the necessary skills to teach children. According to the guidelines [2], the caregivers were supposed to be trained on how to develop a child holistically, including physical, social-emotional and cognitive development, health and nutrition, safe and curricular which might help them to manage and teach the children perfectly. This condition was however not met as expected for caregivers to lead and demonstrate good values, attitudes and principles and assess progress made by children and maintain the standards and practices of ECD services [4,5]. According to [25] other researchers stress the importance of physical competence in running, climbing and cognitive competence to enable the children to control their impulse and to listen to the caregivers. The apparent inadequate training of the caregivers in this study did not to allow them to carry out the indicated requirements successfully nor to identify the needy children and support them effectively. It is emphasized that children with special needs should be assessed through diverse methodologies [26]. However, the enthusiastic and interest shown in children’s activities might be an indication of the caregivers’ willingness to improve on their skills acquisition and given a chance to advance their studies. It is possible that the caregivers might excel in the IECD program.
Existence of child appropriate learning materials was found to be lacking, affecting the children’s gross motor, socio-emotional, cognitive and language development. These developmental needs are necessary to create a conducive environment [15]. Caregivers with appropriate training would have realized the need and importance of creating various learning materials which would enhance the growth and development of the whole child. Further, homemade and recycled teaching materials would have proved useful in these poor resourced centers. This argument is supported by researchers [24] who argue that children from poor communities are generally unable to access high quality services and resources and that they remain poor. Thus, provision of inadequate learning opportunities and facilities may hinder a child’s ability to learn, create self-doubt and delay learning. These deficiencies perpetuate the poverty cycle which is against the norms of the School Readiness Theory. It is further argued, that children who have attended ECD are less likely to repeat classes at primary school and less likely to undergo special needs classes [9]. Furthermore, researchers have established that children who have attended ECD programs and have mastered skills in three core areas of regulation of emotion, behavior, and attention; language, reasoning, and problem solving; and relating well to others and forming friendships are better prepared to experience educational success than those who fail to develop such skills [27].
Not having enough nutritious food or no food at all, may result in stunted physical growth and delayed cognitive development of the child. These health risks may cause physical, cognitive, neurological, or sensory problems that in turn are likely to cause disabilities and learning difficulties [25]. It is argued that the introduction of school feeding programs to poor communities has contributed to enabling environments for optimal learning in primary school [22]. Thus, for the IECD program to be successful, children must be healthy and ready cognitively, emotionally and physically for them to be school ready. This effort in turn requires the support of parents, especially, in typical rural areas where the basic services are lacking [6].
6. Conclusions and Recommendations
The 32 centers in the eight regions lacked the essential requisites necessary for the provision of quality ECD education [1]. The many deficiencies in the ECD center structures, the general poverty in the area, the lack of early learning material, the far away health facilities, did not work to bring about quality ECD services to the children served in these centers. All ECD centers lacked: proper physical infrastructure and facilities, basic amenities, hygienic conditions, nutritious food and teaching resources. The study recommends the following to improve the quality of ECD provision in the 32 ECD centers in this needs assessment:
- The building of informal ECD center structures should be discouraged. When a need for an ECD center is identified, the community members should be encouraged to contact local MGECW’s officials to help with the building specifications of 1.5 m2 of indoor floor space and 2.0 m2 of outdoor space per child enrolled, toilets for boys and girls [23] and should be provided with the necessary child-sized furniture and other essentials. A clearer system of keeping ECD centers accountable to their clientele and aware of their registration status needs to be developed and implemented by the MGECW.
- Children with disabilities should be assisted by the MGECW to acquire the necessary aid and equipment.
- The 7 weeks course offered by the MGECW needs review to determine the quality of the content and determine the skills of the trainers. In addition, workshops should be held by MoHSS to train caregivers in basic health practices to ensure that ECD centers are ready to tackle minor health risks that may occur at the center, hence limiting the health risks. Caregivers should be required to register through distance education via ECD training to upgrade their skills in health.
- All centers should be supplied with teaching and learning resources such as story books, posters, puzzles, technology equipment, and clay.
- Where Community Health workers exist, they should visit the ECD center regularly for health check-ups of children thereby enhancing the well-being of the children and should be supplied with First Aid Kits that could be used for treating minor injuries.
7. Limitations of the Needs Assessment
The needs assessment was affected by the following limitations:
- The time was not enough for exhaustive consultations with all ECD stakeholders involved.
- Lack of adequate finances for researchers to stay longer at the ECD centers to comprehensively observe the activities.
- The questionnaire was in English and the researchers and research assistants had to translate it into local languages, sometimes losing the essence of the content.
- A pilot study was not carried out due to time constraints. This could have eliminated some irrelevant questions.
Author Contributions
E.N.K. has helped with the conceptualization and; formulation of the idea that culminated into the said research goals and aims. She has also developed the research methodology and administered the activity planning and execution. In addition, she has also produced the initial draft for publication and reviewed it a number of times. C.K. was also involved in the conceptualization of the paper. Draft the initial outline of the paper. Contribute to the writing of the methodology, the analysis, and was overall responsible for the quality control of the paper in all aspects of the writing of the paper. G.V.R. was responsible for developing the research methodology and research tools for collecting the data. Conceptualise the data to be used for the article and was involved in drafting the initial concept article. Comment on the final article for submission. All three authors equality contribute to the paper.
Funding
The data collection for this article was funded by the Office of the First Lady, Republic of Namibia.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Republic of Namibia, The Constitution of the Republic of Namibia. First Amendment Act 34, 1998. Available online: http://www.gov.na/documents/10181/14134/Namibia_Constitution.pdf/37b70b76-c15c-45d4-9095-b25d8b8aa0fb (accessed on 2 August 2018).
- Ministry of Gender Equality and Child Welfare. Guidelines for Establishing Early Childhood Centres in Namibia; Ministry of Gender Equality and Child Welfare: Windhoek, Namibia, 2005. [Google Scholar]
- Republic of Namibia. National Development Plan (NDP4) 2012/13 to 2016/17; Office of the President, National Planning Commission: Windhoek, Namibia, 2017. [Google Scholar]
- Department of Social Development. Audit of Early Childhood Development (ECD) Centres National Report. Department of Social Development, Pretoria, Republic of South Africa. Available online: http://ilifalabantwana.co.za/wp-content/uploads/2015/08/ECDAuditNationalReport20140731ReviewedFINALVersionES11.pdf (accessed on 2 August 2018).
- Child Care and Protection Act. No. 3, 2015. Available online: https://laws.parliament.na/annotated-laws-regulations/law-regulation.php?id=473 (accessed on 2 August 2018).
- Ministry of Gender Equality and Child Welfare. National Integrated Early Childhood Development Policy; Ministry of Gender Equality and Child Welfare: Windhoek, Namibia, 2007. [Google Scholar]
- UNESCO-UNICEF. Early Childhood Care and Education. 2012. Available online: http://www.uis.unesco.org/Library/Documents/asia-pacific-end-decade-notes-efa-goal-1-early-childhood-care-education-2012-en.pdf (accessed on 2 August 2018).
- Rangasami, J.; Naeser, G. Mapping of Integrated Early Childhood Development (IECD) in Namibia 2015; UNICEF: Windhoek, Namibia, 2015. [Google Scholar]
- World Bank. Newsletter of the Africa Early Childhood Care and Development Initiative. Issue IV. Available online: http://siteresources.worldbank.org/EXTAFRREGTOPEDUCATION/Resources/ECCD-Newsletter-NL2.pdf (accessed on 2 August 2018).
- Mwamwenda, T.S. Early Childhood Education in Africa. Mediterr. J. Soc. Sci. 2014, 20, 1403–1412. [Google Scholar] [CrossRef]
- Engle, P.L.; Fernald, L.C.; Alderman, H.; Behrman, J.; O’Gara, C.; Yousafzai, A.; de Mello, M.C.; Hidrobo, M.; Ulkuer, N.; Ertem, I.; et al. Strategies for reducing inequalities and improving developmental outcomes for young children in low-income and middle-income countries. Lancet 2011, 378, 1339–1353. [Google Scholar] [CrossRef]
- Walker, S.P.; Wachs, T.D.; Grantham-McGregor, S.; Black, M.M.; Nelson, C.A.; Huffman, S.L.; Baker-Henningham, H.; Chang, S.M.; Hamadani, J.D.; Lozoff, B.; et al. Inequality in early childhood: Risk and protective factors for early child development. Lancet 2011, 378, 1325–1338. [Google Scholar] [CrossRef]
- Donald, D.; Lazarus, S.; Lolwana, P. Educational Psychology in Social Context; Oxford University Press: Cape Town, UK, 2014. [Google Scholar]
- De Witt, M.W. The Young Child in Context. A Psycho-Social Perspectives; Van Schaik Publication: Pretoria, South Africa, 2016. [Google Scholar]
- Coury, D.; Opper, S.; Nahayo, J. Early Child Development in Burundi: Community Delivery System (or Community-Driven Response?) to Improve the Well-Being of Young Children. Available online: http://siteresources.worldbank.org/INTPH/Resources/376086-1256847692707/6526326-1287681563483/RachelMentalHealth.pdf (accessed on 2 August 2018).
- Pence, A.; Evans, J.L. Africa’s Future, Africa’s Challenge: Early Childhood Care and Development in Sub-Saharan Africa. 2008. Available online: https://openknowledge.worldbank.org/handle/10986/6365 (accessed on 2 August 2018).
- Rimm-Kaufman, S.; Sandilos, L. School Transition and School Readiness: An Outcome of Early Childhood Development. In Encyclopedia on Early Childhood Development; Tremblay, R.E., Boivin, M., Peters, R., Eds.; 2017; Available online: http://www.child-encyclopedia.com/school-readiness/according-experts/school-transition-and-school-readiness-outcome-early-childhood (accessed on 31 July 2018).
- Rvachew, S. Technology in Early Childhood Education: Overall Commentary. In Encyclopedia on Early Childhood Development; Tremblay, R.E., Boivin, M., Peters, R., Eds.; 2016; Available online: http://www.child-encyclopedia.com/school-readiness/according-experts/school-transition-and-school-readiness-outcome-early-childhood (accessed on 31 July 2018).
- The Namibia Ministry of Health and Social Services (MoHSS) and ICF International. The Namibia Demographic and Health Survey 2013; MoHSS and ICF International: Windhoek, Namibia; Rockville, MD, USA, 2014. [Google Scholar]
- Department of Public Welfare, Office of Youth and Families. Pennsylvania’s Outcomes Framework: Improving Outcomes for Children and Families through a Shared Community Agenda. 2000. Available online: https://www.center-school.org/fssr/downloads/documents/PACoutcomesFramework.pdf (accessed on 2 August 2018).
- UNICEF. School Readiness: A Conceptual Framework; United Nations Children’s Fund: New York, NY, USA, 2012. [Google Scholar]
- The Centre for Theory of Change, Inc. Theory of Change for School Readiness. 2016. Available online: http://www.theoryofchange.org/wp-content/uploads/toco_library/pdf/2006 (accessed on 2 August 2018).
- Gay, L.; Mills, G.; Airasian, P. Educational Research: Competencies for Analysis and Application, 8th ed.; Prentice Hall: New York, NY, USA, 2006. [Google Scholar]
- Ministry of Gender Equality and Child Welfare. Namibian Standards for Early Childhood Development Centres; Ministry of Gender Equality and Child Welfare: Windhoek, Namibia, 2012. [Google Scholar]
- Hu, H.; Pattugalan, M. Factors that Impact Children’s School Readiness: Comparing the Perspectives of Charles Wright Mills and bell hooks. Ryerson J. Policy Stud. 2017, 1, 1–13. [Google Scholar]
- Donald, D.; Lazarus, S.; Moolla, N. Educational Psychology in Social Context: Ecosystemic Applications in Southern Africa; ABC Press: Cape Town, South Africa, 2015. [Google Scholar]
- Brown, A.; Haihambo, C.K. Inclusive Education as a Democratic Imperative (in) Democracy and Education in Namibia and Beyond; Amukugo, E.M., Ed.; UNAM Press, University of Namibia: Wenhaoke, Namibia, 2016. [Google Scholar]
Figure 1.
Adapted Theory of Change for School Readiness [21].
Figure 1.
Adapted Theory of Change for School Readiness [21].

Figure 2.
Commonly available teaching resources.

Figure 3.
Nutritious food provided by the ECD Centers.


{kind=link}
{kind=link}
{kind=link}
Table 1.
Number of children and qualification of ECD caregivers per community.
| Community | ||||
|---|---|---|---|---|
| A | B | C | Grand Total | |
| Number of children | 51 | 453 | 531 | 1035 |
| Education of caregivers | ||||
| Basic Education Teacher Diploma | 1 | 1 | ||
| Certificate of Attendance: 7 weeks ECD Basic Course Curriculum | 10 | 4 | 14 | |
| Diploma in Lower Primary | 1 | 1 | ||
| Grade 10 | 2 | 2 | 3 | 7 |
| Grade 11 | 1 | 1 | ||
| Grade 12 | 1 | 4 | 5 | |
| Lower primary certificate | 1 | 1 | ||
| Not indicated | 2 | 2 | ||
| Grand Total | 2 | 15 | 15 | 32 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Ngololo Kamara, E.; Kasanda, C.; Van Rooy, G. Provision of Integrated Early Childhood Development in Namibia: Are We on the Right Track? Educ. Sci. 2018, 8, 117. https://doi.org/10.3390/educsci8030117
AMA Style
Ngololo Kamara E, Kasanda C, Van Rooy G. Provision of Integrated Early Childhood Development in Namibia: Are We on the Right Track? Education Sciences. 2018; 8(3):117. https://doi.org/10.3390/educsci8030117
Chicago/Turabian StyleNgololo Kamara, Elizabeth, Choshi Kasanda, and Gert Van Rooy. 2018. "Provision of Integrated Early Childhood Development in Namibia: Are We on the Right Track?" Education Sciences 8, no. 3: 117. https://doi.org/10.3390/educsci8030117
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.