Exploring Resilience When Living with a Wound — An Integrative Literature Review

Abstract
:1. Introduction
2. Experimental Section
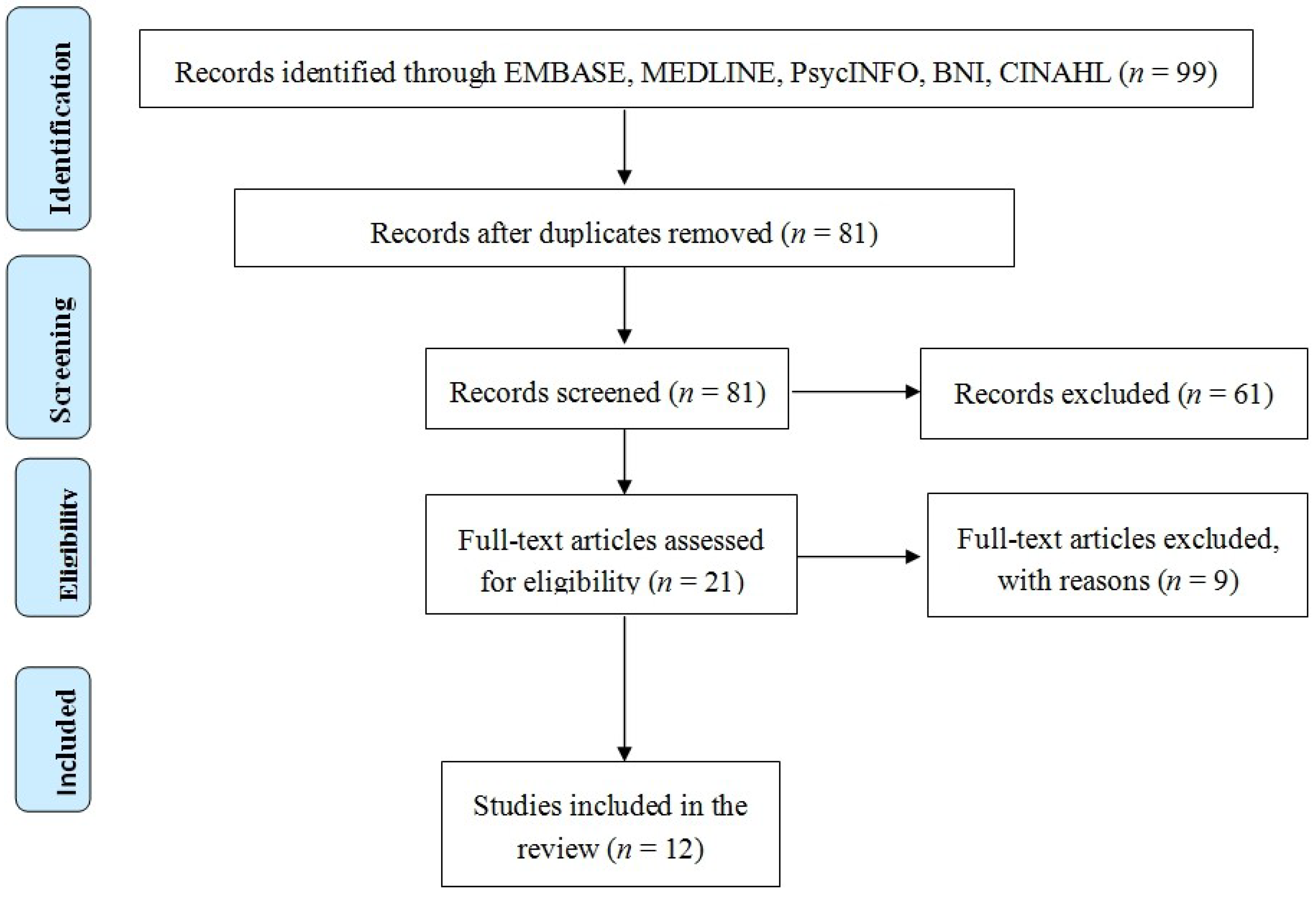
Search Strategy
3. Results and Discussion


{kind=link}
| Papers | Included/Excluded |
|---|---|
| 1. Beitz et al. [23] | Included-A phenomenological design to investigate the experiences of people living with a chronic wound using interviews and field notes |
| 2. Carlsson et al. [24] | Included-The aim of this study was to assess concerns and health-related quality of life pre operatively and during the first 6 months following ostomy surgery in the presence of rectal cancer. Paper focused on quality of life and the effect of rectal cancer |
| 3. de Meneses et al. [25] | Included-the paper examined differences in health-related quality of life and self-esteem of patients with Diabetes Mellitus with and without foot ulcers. |
| 4. Douglas et al. [26] | Excluded-one patient case study |
| 5. Douglas [26] | Included-Grounded theory related to patient experience of living with a wound. The relationship with healthcare workers is important and may contribute to bolstering a sense of control and having a vision for the future. |
| 6. Dougherty [27] | Included-the aim of the paper was exploring the effect on quality of life outcomes following a major injury |
| 7. Gonzalez et al. [28] | Excluded as was a letter to the editor. |
| 8. Gonzalez et al. [29] | Included-the paper examined the relationship between symptoms of depression and the development of diabetic foot ulcers |
| 9. Goldberg [30] | Included-the paper described the phenomenon of living with a chronic non healing wound in elders of colour and in financially fragile circumstances |
| 10. Hollinworth et al. [31] | Included-reported nurses approach to psychological aspects of wound care |
| 11. Hopkins [32] | Excluded-review paper |
| 12. Jones [33] | Excluded-one patient evaluation |
| 13. Lund-Nielsen [34] | Included-The study described experiences of health care avoidance in women with advanced breast cancer who had developed malignant wounds. |
| 14. Probst et al. [35] | Included-the study focussed on understanding the lived experiences of patients with a malignant fungating breast wound and their informal carers. |
| 15. Pragnell et al. [36] | Excluded as a one patient case study focussing on the use of a dressing product |
| 16. Probst et al. [37] | Included-the aim of the paper was to explore experiences of carers who cared for a loved one with a fungating breast wound. |
| 17. Vileikyte [38] | Excluded-review paper |
| 18. Vileikyte et al. [39] | Excluded-conference abstract only |
| 19. Woo [40] | Excluded as was a continuing education paper |
| 20. Woo [41] | Excluded-review paper |
| 21. Winkley et al. [42] | Included-the paper examined the association between depressive disorder and increased mortality in people with their first foot ulcer at 5 years. |
Discussion
4. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Antoni, M.H.; Goodkin, K. Host moderator variables in the promotion of cervical neoplasia—I. Personal facets. J. Psychosomatic Res. 1988, 32, 327–338. [Google Scholar] [CrossRef]
- Rabkin, J.G.; Remien, R.; Williams, J.B.W.; Katoff, L. Resilience in adversity among long-term survivors of AIDS. Psychiatric Serv. 1993, 44, 162–167. [Google Scholar]
- Edward, K. Resilience: A protector from depression. J. Am. Psychiatric Nurses Assoc. 2005, 11, 241–243. [Google Scholar] [CrossRef]
- Edward, K.; Welch, A.; Chater, K. The phenomenon of resilience as described by adults who have experienced mental illness. J. Adv. Nursing 2009, 65, 587–595. [Google Scholar] [CrossRef]
- Edward, K. Chronic illness and wellbeing: Using nursing practice to foster resilience as resistance. Br. J. Nursing 2013, 22, 741. [Google Scholar] [CrossRef]
- Ebrecht, M.; Hextall, J.; Kirtley, L.-G.; Taylor, A.; Dyson, M.; Weinman, J. Perceived stress and cortisol levels predict speed of wound healing in healthy male adults. Psychoneuroendocrinology 2004, 29, 798–809. [Google Scholar] [CrossRef] [PubMed]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences; Routledge Academic: New York, NY, USA, 2013. [Google Scholar]
- Goldberg, D.P.; Hillier, V.F. A scaled version of the general health questionnaire. Psychol. Med. 1979, 9, 139–145. [Google Scholar] [PubMed]
- Gouin, J.-P.; Kiecolt-Glaser, J.K.; Malarkey, W.B.; Glaser, R. The influence of anger expression on wound healing. Brain Behav. Immunity 2008, 22, 699–708. [Google Scholar] [CrossRef]
- Solowiej, K.; Mason, V.; Upton, D. Psychological stress and pain in wound care, part 3: Management. J. Wound Care 2010, 19, 153. [Google Scholar] [CrossRef] [PubMed]
- Adams, N.; Poole, H.; Richardson, C. Psychological approaches to chronic pain management: Part 1. J. Clin. Nursing 2006, 15, 290–300. [Google Scholar] [CrossRef]
- Cole-King, A.; Harding, K.G. Psychological factors and delayed healing in chronic wounds. Psychosom. Med. 2001, 63, 216–220. [Google Scholar]
- Jones, J.; Barr, W.; Robinson, J.; Carlisle, C. Depression in patients with chronic venous ulceration. Br. J. Nursing 2006, 15, S17. [Google Scholar] [CrossRef]
- Guarnera, G.; Tinelli, G.; Abeni, D.; di Pietro, C.; Sampogna, F.; Tabolli, S. Pain and quality of life in patients with vascular leg ulcers: An Italian multicentre study. J. Wound Care 2007, 16, 347–351. [Google Scholar]
- Finlayson, K.; Edwards, H.; Courtney, M. The impact of psychosocial factors on adherence to compression therapy to prevent recurrence of venous leg ulcers. J. Clin. Nursing 2010, 19, 1289–1297. [Google Scholar]
- Mapplebeck, L. Case study: Psychosocial aspects of chronic bilateral venous leg ulcers. Br. J. Community Nursing 2008, 13, S33–S38. [Google Scholar] [CrossRef]
- Pieper, B.; Vallerand, A.H.; Nordstrom, C.K.; DiNardo, E. Comparison of bodily pain: Persons with and without venous ulcers in an indigent care clinic. J. Wound Ostomy Continence Nursing 2009, 36, 493–502. [Google Scholar] [CrossRef]
- Upton, D.; Solowiej, K.; Woo, K.Y. A multinational health professional perspective of the prevalence of mood disorders in patients with acute and chronic wounds. Int. Wound J. 2013. [Google Scholar] [CrossRef]
- Edward, K. Being resilient as described by people who experience mental illness. Int. J. Mental Health Nursing 2008, 17, A6. [Google Scholar]
- Edward, K.; Warelow, P. Resilience: When coping is emotionally intelligent. J. Am. Psychiatric Nurses Assoc. 2005, 11, 101–102. [Google Scholar] [CrossRef]
- Taylor, R.; Reeves, B.; Ewings, P.; Binns, S.; Keast, J.; Mears, R. A systematic review of the effectiveness of critical appraisal skills training for clinicians. Med. Educ. 2000, 34, 120–125. [Google Scholar] [CrossRef] [PubMed]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gøtzsche, P.C.; Ioannidis, J.P.A.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: Explanation and elaboration. Ann. Int. Med. 2009, 151, W-65-W-94. [Google Scholar]
- Beitz, J.M.; Goldberg, E.; Yoder, L.H. The lived experience of having a chronic wound: A phenomenologic study. Medsurg Nursing 2005, 14, 51–82. [Google Scholar] [PubMed]
- Carlsson, E.; Berndtsson, I.; Hallén, A.-M.; Lindholm, E.; Persson, E. Concerns and quality of life before surgery and during the recovery period in patients with rectal cancer and an ostomy. J. Wound Ostomy Continence Nursing 2010, 37, 654–661. [Google Scholar] [CrossRef]
- De Meneses, L.C.; Blanes, L.; Francescato Veiga, D.; Carvalho Gomes, H.; Masako Ferreira, L. Health-related quality of life and self-esteem in patients with diabetic foot ulcers: Results of a cross-sectional comparative study. Ostomy-Wound Manage. 2011, 57, 36. [Google Scholar]
- Douglas, V. Living with a chronic leg ulcer: An insight into patients’ experiences and feelings. J. Wound Care 2001, 10, 355–362. [Google Scholar] [CrossRef] [PubMed]
- Dougherty, P.J. Transtibial amputees from the Vietnam war twenty-eight-year follow-up. J. Bone Joint Surg. 2001, 83, 383–383. [Google Scholar] [PubMed]
- Gonzalez, J.; Hardman, M.; Boulton, A.J.; Vileikyte, L. Coping and depression in diabetic foot ulcer healing: Causal influence, mechanistic evidence or none of the above? Diabetologia 2011, 54, 205–206. [Google Scholar] [CrossRef] [PubMed]
- Gonzalez, J.; Vileikyte, L.; Ulbrecht, J.; Rubin, R.; Garrow, A.; Delgado, C.; Cavanagh, P.; Boulton, A.; Peyrot, M. Depression predicts first but not recurrent diabetic foot ulcers. Diabetologia 2010, 53, 2241–2248. [Google Scholar] [CrossRef] [PubMed]
- Goldberg, E.; Beitz, J.M. The lived experience of diverse elders with chronic wounds. Ostomy/Wound Manage. 2010, 56, 36–46. [Google Scholar]
- Hollinworth, H.; Hawkins, J. Teaching nurses psychological support of patients with wounds. Br. J. Nursing 2002, 11, 8–19. [Google Scholar] [CrossRef]
- Hopkins, S. Psychological aspects of wound healing. Nursing Times 2001, 97, 57. [Google Scholar] [PubMed]
- Jones, J. Stress responses, pressure ulcer development and adaptation. Br. J. Nursing 2003, 12, S17–S24. [Google Scholar] [CrossRef]
- Lund-Nielsen, B.; Midtgaard, J.; Rørth, M.; Gottrup, F.; Adamsen, L. An avalanche of ignoring-a qualitative study of health care avoidance in women with malignant breast cancer wounds. Cancer Nursing 2011, 34, 277–285. [Google Scholar]
- Probst, S.; Arber, A.; Faithfull, S. Malignant fungating wounds—the meaning of living in an unbounded body. Eur. J. Oncol. Nursing 2013, 17, 38–45. [Google Scholar] [CrossRef] [Green Version]
- Pragnell, J; Neilson, J. The social and psychological impact of hard-to-heal wounds. Br. J. Nursing 2009, 19, 1248–1252. [Google Scholar]
- Probst, S.; Arber, A.; Trojan, A.; Faithfull, S. Caring for a loved one with a malignant fungating wound. Supportive Care in Cancer 2012, 20, 3065–3070. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vileikyte, L. Psychosocial and behavioral aspects of diabetic foot lesions. Curr. Diabetes Rep. 2008, 8, 119–125. [Google Scholar] [CrossRef]
- Vileikyte, L.; Shen, B.-J.; Hardman, M.; Kirsner, R.; Boulton, A.; Schneiderman, N. Emotional distress may impede diabetic foot ulcer healing through elevated levels of interleukin-6: Preliminary findings. In Diabetologia; Springer: New York, NY, USA, 2010. [Google Scholar]
- Woo, K.Y. Exploring the effects of pain and stress on wound healing. Adv. Skin Wound Care 2012, 25, 38–44. [Google Scholar] [CrossRef] [PubMed]
- Woo, K. Chronic wound-associated pain, psychological stress, and wound healing. Surgical Technol. Int. 2012, 22, 57–65. [Google Scholar]
- Winkley, K.; Sallis, H.; Kariyawasam, D.; Leelarathna, L.; Chalder, T.; Edmonds, M.; Stahl, D.; Ismail, K. Five-year follow-up of a cohort of people with their first diabetic foot ulcer: The persistent effect of depression on mortality. Diabetologia 2012, 55, 303–310. [Google Scholar] [CrossRef] [PubMed]
- Williams, L.H.; Miller, D.R.; Fincke, G.; Lafrance, J.-P.; Etzioni, R.; Maynard, C.; Raugi, G.J.; Reiber, G.E. Depression and incident lower limb amputations in veterans with diabetes. J. Diabetes Complicat. 2011, 25, 175–182. [Google Scholar] [CrossRef] [PubMed]
- Van der Feltz-Cornelis, C.M.; Nuyen, J.; Stoop, C.; Chan, J.; Jacobson, A.M.; Katon, W.; Snoek, F.; Sartorius, N. Effect of interventions for major depressive disorder and significant depressive symptoms in patients with diabetes mellitus: A systematic review and meta-analysis. Gen. Hosp. Psychiatry 2010, 32, 380–395. [Google Scholar]
- Edwards, H.; Courtney, M.; Finlayson, K.; Lewis, C.; Lindsay, E.; Dumble, J. Improved healing rates for chronic venous leg ulcers: Pilot study results from a randomized controlled trial of a community nursing intervention. Int. J. Nursing Pract. 2005, 11, 169–176. [Google Scholar] [CrossRef] [Green Version]
© 2014 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/3.0/).
Share and Cite
Ousey, K.; Edward, K.-l. Exploring Resilience When Living with a Wound — An Integrative Literature Review. Healthcare 2014, 2, 346-355. https://doi.org/10.3390/healthcare2030346
Ousey K, Edward K-l. Exploring Resilience When Living with a Wound — An Integrative Literature Review. Healthcare. 2014; 2(3):346-355. https://doi.org/10.3390/healthcare2030346
Chicago/Turabian StyleOusey, Karen, and Karen-leigh Edward. 2014. "Exploring Resilience When Living with a Wound — An Integrative Literature Review" Healthcare 2, no. 3: 346-355. https://doi.org/10.3390/healthcare2030346