
Concerns about Breast Cancer, Pain, and Fatigue in Non-Metastatic Breast Cancer Patients Undergoing Primary Treatment

Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Procedures
2.3. Measures
2.3.1. Demographic and Medical Characteristics
2.3.2. Psychosocial Measures
2.4. Analytic Strategy
3. Results
3.1. Sample Characteristics
3.2. Post-Surgical Rejection Issues as a Predictor of Fatigue Interference at 12-Month Follow-Up
3.3. Testing the Mediating Role of Depressive Symptoms at 6-Month Follow-Up
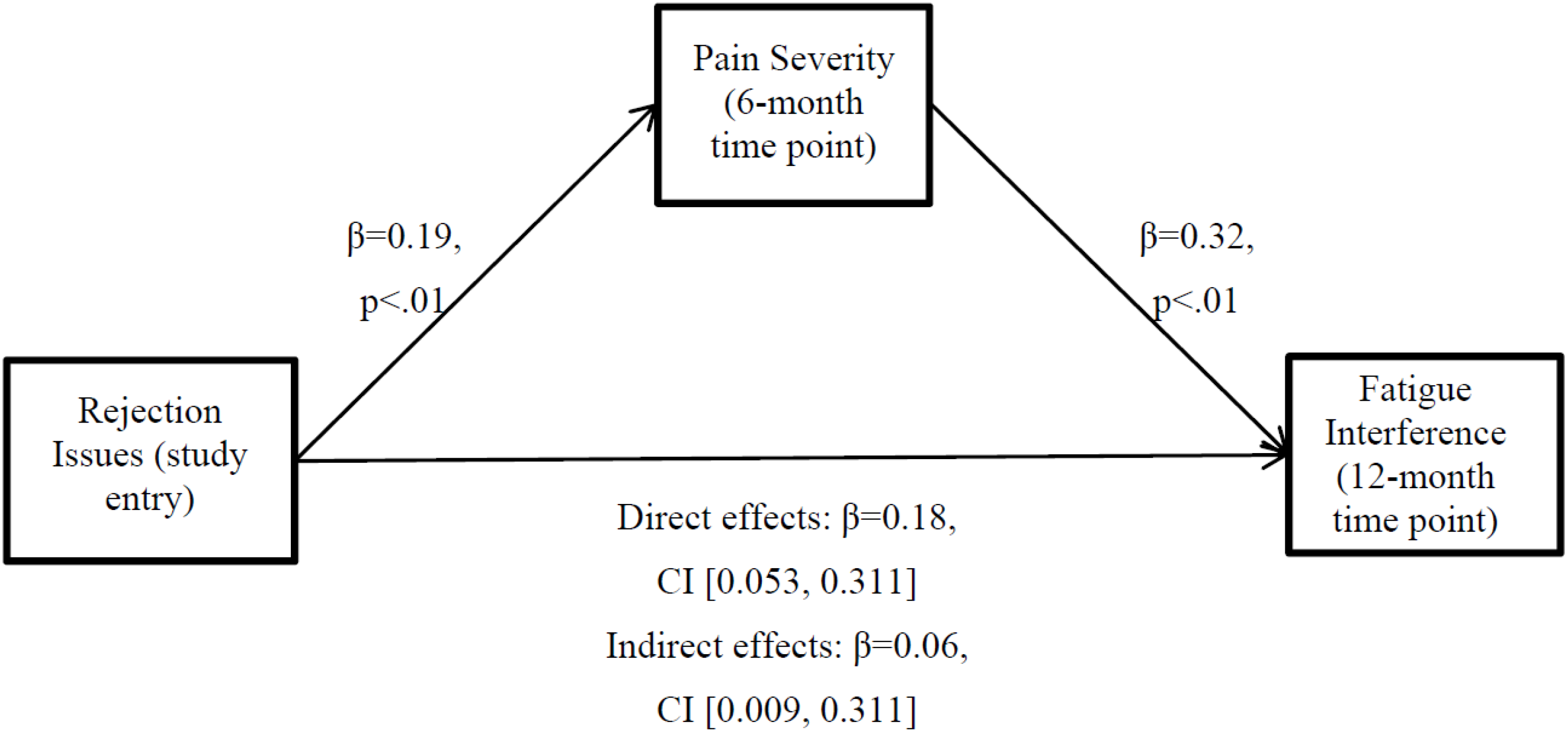
3.4. Testing the Mediating Role of Pain Severity at 6-Month Follow-Up
4. Discussion
4.1. Strengths and Limitations
4.2. Future Work and Clinical Implications
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Society, A.C. Breast Cancer Facts and Figures (2014–2015); American Cancer Society: Atlanta, GA, USA, 2014. [Google Scholar]
- Meyerowitz, B.E. Psychosocial correlates of breast cancer and its treatments. Psychol. Bull. 1980, 87, 108–131. [Google Scholar] [CrossRef] [PubMed]
- Burgess, C.; Cornelius, V.; Graham, J.; Richards, M.; Ramirez, A. Depression and anxiety in women with early breast cancer: Five year observational cohort study. BMJ 2005. [Google Scholar] [CrossRef] [PubMed]
- Dupont, A.; Bower, J.E.; Stanton, A.L.; Ganz, P.A. Cancer-related intrusive thoughts predict behavioral symptoms following breast cancer treatment. Health Psychol. 2014, 33, 155–163. [Google Scholar] [CrossRef] [PubMed]
- Spencer, S.M.; Lehman, J.M.; Wynings, C.; Arena, P.; Carver, C.S.; Antoni, M.H.; Derhagopian, R.P.; Ironson, G.; Love, N. Concerns about breast cancer and relations to psychosocial well-being in a multiethnic sample of early-stage patients. Health Psychol. 1999, 18, 159–168. [Google Scholar] [CrossRef] [PubMed]
- Pistrang, N.B.; Barker, C. Disclosure of Concerns in Breast Cancer. Psycho-Oncology 1992, 1, 183–192. [Google Scholar] [CrossRef]
- Bottrill, S.; Pistrang, N.; Barker, C.; Worrell, M. The use of therapist self-disclosure: Clinical psychology trainees’ experiences. Psychother. Res. 2010, 20, 165–180. [Google Scholar] [CrossRef] [PubMed]
- Peters-Golden, H. Breast cancer: Varied perceptions of social support in the illness experience. Soc. Sci. Med. 1982, 16, 483–491. [Google Scholar] [CrossRef]
- Boinon, D.; Sultan, S.; Charles, C.; Stulz, A.; Guillemeau, C.; Delaloge, S.; Dauchy, S. Changes in psychological adjustment over the course of treatment for breast cancer: The predictive role of social sharing and social support. Psychooncology 2014, 23, 291–298. [Google Scholar] [CrossRef] [PubMed]
- Bloom, J.R.; Stewart, S.L.; Johnston, M.; Banks, P.; Fobair, P. Sources of support and the physical and mental well-being of young women with breast cancer. Soc. Sci. Med. 2001, 53, 1513–1524. [Google Scholar] [CrossRef]
- Roberts, C.S.; Cox, C.E.; Shannon, V.J.; Wells, N.L. A closer look at social support as a moderator of stress in breast cancer. Health Soc. Work 1994, 19, 157–164. [Google Scholar] [PubMed]
- Northouse, L.L. Social support in patients’ and husbands’ adjustment to breast cancer. Nurs. Res. 1988, 37, 91–95. [Google Scholar] [CrossRef] [PubMed]
- Hack, T.F.; Pickles, T.; Bultz, B.D.; Ruether, J.D.; Weir, L.M.; Degner, L.F.; Mackey, J.R. Impact of providing audiotapes of primary adjuvant treatment consultations to women with breast cancer: A multisite, randomized, controlled trial. J. Clin. Oncol. 2003, 21, 4138–4144. [Google Scholar] [CrossRef] [PubMed]
- Fallowfield, L.J. Psychosocial adjustment after treatment for early breast cancer. Oncology 1990, 4, 89–97, discussion 97–98, 100. [Google Scholar] [PubMed]
- Golden-Kreutz, D.M.; Andersen, B.L. Depressive symptoms after breast cancer surgery: Relationships with global, cancer-related, and life event stress. Psychooncology 2004, 13, 211–220. [Google Scholar] [CrossRef] [PubMed]
- Fann, J.R.; Thomas-Rich, A.M.; Katon, W.J.; Cowley, D.; Pepping, M.; McGregor, B.A.; Gralow, J. Major depression after breast cancer: A review of epidemiology and treatment. Gen. Hosp. Psychiatry 2008, 30, 112–126. [Google Scholar] [CrossRef] [PubMed]
- Fecho, K.; Miller, N.R.; Merritt, S.A.; Klauber-Demore, N.; Hultman, C.S.; Blau, W.S. Acute and persistent postoperative pain after breast surgery. Pain Med. 2009, 10, 708–715. [Google Scholar] [CrossRef] [PubMed]
- Hickey, O.T.; Burke, S.M.; Hafeez, P.; Mudrakouski, A.L.; Hayes, I.D.; Shorten, G.D. Severity of acute pain after breast surgery is associated with the likelihood of subsequently developing persistent pain. Clin. J. Pain 2010, 26, 556–560. [Google Scholar] [CrossRef] [PubMed]
- Shelby, R.A.; Edmond, S.N.; Wren, A.A.; Keefe, F.J.; Peppercorn, J.M.; Marcom, P.K.; Blackwell, K.L.; Kimmick, G.G. Self-efficacy for coping with symptoms moderates the relationship between physical symptoms and well-being in breast cancer survivors taking adjuvant endocrine therapy. Support. Care Cancer 2014, 22, 2851–2859. [Google Scholar] [CrossRef] [PubMed]
- Vilholm, O.J.; Cold, S.; Rasmussen, L.; Sindrup, S.H. The postmastectomy pain syndrome: An epidemiological study on the prevalence of chronic pain after surgery for breast cancer. Br. J. Cancer 2008, 99, 604–610. [Google Scholar] [CrossRef] [PubMed]
- DeSantis, C.; Ma, J.; Bryan, L.; Jemal, A. Breast cancer statistics, 2013. CA Cancer J. Clin. 2014, 64, 52–62. [Google Scholar] [CrossRef] [PubMed]
- Kehlet, H.; Jensen, T.S.; Woolf, C.J. Persistent postsurgical pain: Risk factors and prevention. Lancet 2006, 367, 1618–1625. [Google Scholar] [CrossRef]
- Vargas, S.; Wohlgemuth, W.K.; Antoni, M.H.; Lechner, S.C.; Holley, H.A.; Carver, C.S. Sleep dysfunction and psychosocial adaptation among women undergoing treatment for non-metastatic breast cancer. Psychooncology 2010, 19, 669–673. [Google Scholar] [CrossRef] [PubMed]
- Hofman, M.; Ryan, J.L.; Figueroa-Moseley, C.D.; Jean-Pierre, P.; Morrow, G.R. Cancer-related fatigue: The scale of the problem. Oncologist 2007, 12 (Suppl. 1), 4–10. [Google Scholar] [CrossRef] [PubMed]
- Curt, G.A.; Breitbart, W.; Cella, D.; Groopman, J.E.; Horning, S.J.; Itri, L.M.; Johnson, D.H.; Miaskowski, C.; Scherr, S.L.; Portenoy, R.K.; et al. Impact of cancer-related fatigue on the lives of patients: New findings from the Fatigue Coalition. Oncologist 2000, 5, 353–360. [Google Scholar] [CrossRef] [PubMed]
- Bower, J.E.; Ganz, P.A.; Desmond, K.A.; Rowland, J.H.; Meyerowitz, B.E.; Belin, T.R. Fatigue in breast cancer survivors: Occurrence, correlates, and impact on quality of life. J. Clin. Oncol. 2000, 18, 743–753. [Google Scholar] [PubMed]
- Cella, D.; Davis, K.; Breitbart, W.; Curt, G.; Coalition, F. Cancer-related fatigue: Prevalence of proposed diagnostic criteria in a United States sample of cancer survivors. J. Clin. Oncol. 2001, 19, 3385–3391. [Google Scholar] [PubMed]
- Jaremka, L.M.; Fagundes, C.P.; Glaser, R.; Bennett, J.M.; Malarkey, W.B.; Kiecolt-Glaser, J.K. Loneliness predicts pain, depression, and fatigue: Understanding the role of immune dysregulation. Psychoneuroendocrinology 2013, 38, 1310–1317. [Google Scholar] [CrossRef] [PubMed]
- Eom, C.S.; Shin, D.W.; Kim, S.Y.; Yang, H.K.; Jo, H.S.; Kweon, S.S.; Kang, Y.S.; Kim, J.H.; Cho, B.L.; Park, J.H. Impact of perceived social support on the mental health and health-related quality of life in cancer patients: Results from a nationwide, multicenter survey in South Korea. Psychooncology 2013, 22, 1283–1290. [Google Scholar] [CrossRef] [PubMed]
- Hughes, S.; Jaremka, L.M.; Alfano, C.M.; Glaser, R.; Povoski, S.P.; Lipari, A.M.; Agnese, D.M.; Farrar, W.B.; Yee, L.D.; Carson, W.E., 3rd; et al. Social support predicts inflammation, pain, and depressive symptoms: Longitudinal relationships among breast cancer survivors. Psychoneuroendocrinology 2014, 42, 38–44. [Google Scholar] [PubMed]
- Jaremka, L.M.; Andridge, R.R.; Fagundes, C.P.; Alfano, C.M.; Povoski, S.P.; Lipari, A.M.; Agnese, D.M.; Arnold, M.W.; Farrar, W.B.; Yee, L.D.; et al. Pain, depression, and fatigue: Loneliness as a longitudinal risk factor. Health Psychol. 2014, 33, 948–957. [Google Scholar] [CrossRef] [PubMed]
- Bower, J.E. Management of cancer-related fatigue. Clin. Adv. Hematol. Oncol. 2006, 4, 828–829. [Google Scholar] [PubMed]
- Goedendorp, M.M.; Gielissen, M.F.; Verhagen, C.A.; Bleijenberg, G. Development of fatigue in cancer survivors: A prospective follow-up study from diagnosis into the year after treatment. J. Pain Symptom Manag. 2013, 45, 213–222. [Google Scholar] [CrossRef] [PubMed]
- Servaes, P.; Prins, J.; Verhagen, S.; Bleijenberg, G. Fatigue after breast cancer and in chronic fatigue syndrome: Similarities and differences. J. Psychosom. Res. 2002, 52, 453–459. [Google Scholar] [CrossRef]
- Geinitz, H.; Zimmermann, F.B.; Thamm, R.; Keller, M.; Busch, R.; Molls, M. Fatigue in patients with adjuvant radiation therapy for breast cancer: Long-term follow-up. J. Cancer Res. Clin. Oncol. 2004, 130, 327–333. [Google Scholar] [CrossRef] [PubMed]
- Blesch, K.S.; Paice, J.A.; Wickham, R.; Harte, N.; Schnoor, D.K.; Purl, S.; Rehwalt, M.; Kopp, P.L.; Manson, S.; Coveny, S.B.; et al. Correlates of fatigue in people with breast or lung cancer. Oncol. Nurs. Forum 1991, 18, 81–87. [Google Scholar] [PubMed]
- Nieboer, P.; Buijs, C.; Rodenhuis, S.; Seynaeve, C.; Beex, L.V.; van der Wall, E.; Richel, D.J.; Nooij, M.A.; Voest, E.E.; Hupperets, P.; et al. Fatigue and relating factors in high-risk breast cancer patients treated with adjuvant standard or high-dose chemotherapy: A longitudinal study. J. Clin. Oncol. 2005, 23, 8296–8304. [Google Scholar] [CrossRef] [PubMed]
- Antoni, M.H.; Lechner, S.C.; Kazi, A.; Wimberly, S.R.; Sifre, T.; Urcuyo, K.R.; Phillips, K.; Glück, S.; Carver, C.S. How stress management improves quality of life after treatment for breast cancer. J. Consult. Clin. Psychol. 2006, 74, 1143–1152. [Google Scholar] [CrossRef] [PubMed]
- Vargas, S.; Antoni, M.H.; Carver, C.S.; Lechner, S.C.; Wohlgemuth, W.; Llabre, M.; Blomberg, B.B.; Glück, S.; DerHagopian, R.P. Sleep quality and fatigue after a stress management intervention for women with early-stage breast cancer in southern Florida. Int. J. Behav. Med. 2014, 21, 971–981. [Google Scholar] [CrossRef] [PubMed]
- Cleeland, C.S.; Ryan, K.M. Pain assessment: Global use of the Brief Pain Inventory. Ann. Acad. Med. Singap. 1994, 23, 129–138. [Google Scholar] [PubMed]
- Kornguth, P.J.; Keefe, F.J.; Wright, K.R.; Delong, D.M. Mammography pain in women treated conservatively for breast cancer. J. Pain. 2000, 1, 268–274. [Google Scholar] [CrossRef] [PubMed]
- Daut, R.L.; Cleeland, C.S.; Flanery, R.C. Development of the Wisconsin Brief Pain Questionnaire to assess pain in cancer and other diseases. Pain 1983, 17, 197–210. [Google Scholar] [CrossRef]
- Miller, I.W.; Bishop, S.; Norman, W.H.; Maddever, H. The Modified Hamilton Rating Scale for Depression: Reliability and validity. Psychiatry Res. 1985, 14, 131–142. [Google Scholar] [CrossRef]
- Williams, J.B. A structured interview guide for the Hamilton Depression Rating Scale. Arch. Gen. Psychiatry 1988, 45, 742–747. [Google Scholar] [CrossRef] [PubMed]
- Soygur, H.; Palaoglu, O.; Akarsu, E.S.; Cankurtaran, E.S.; Ozalp, E.; Turhan, L.; Ayhan, I.H. Interleukin-6 levels and HPA axis activation in breast cancer patients with major depressive disorder. Prog. Neuropsychopharmacol. Biol. Psychiatry 2007, 31, 1242–1247. [Google Scholar] [CrossRef] [PubMed]
- Poleshuck, E.L.; Giles, D.E.; Tu, X. Pain and depressive symptoms among financially disadvantaged women’s health patients. J. Womens Health (Larchmt.) 2006, 15, 182–193. [Google Scholar] [CrossRef] [PubMed]
- Hann, D.M.; Jacobsen, P.B.; Azzarello, L.M.; Martin, S.C.; Curran, S.L.; Fields, K.K.; Greenberg, H.; Lyman, G. Measurement of fatigue in cancer patients: Development and validation of the Fatigue Symptom Inventory. Qual. Life Res. 1998, 7, 301–310. [Google Scholar] [CrossRef] [PubMed]
- Hann, D.M.; Denniston, M.M.; Baker, F. Measurement of fatigue in cancer patients: Further validation of the Fatigue Symptom Inventory. Qual. Life Res. 2000, 9, 847–854. [Google Scholar] [CrossRef] [PubMed]
- Baron, R.M.; Kenny, D.A. The moderator-mediator variable distinction in social psychological research: Conceptual, strategic, and statistical considerations. J. Personal. Soc. Psychol. 1986, 51, 1173–1182. [Google Scholar] [CrossRef]
- Preacher, K.J.; Hayes, A.F. SPSS and SAS procedures for estimating indirect effects in simple mediation models. Behav. Res. Methods Instrum. Comput. 2004, 36, 717–731. [Google Scholar] [CrossRef] [PubMed]
- Serlin, R.C.; Mendoza, T.R.; Nakamura, Y.; Edwards, K.R.; Cleeland, C.S. When is cancer pain mild, moderate or severe? Grading pain severity by its interference with function. Pain 1995, 61, 277–284. [Google Scholar] [PubMed]
- Zimmerman, M.; Martinez, J.H.; Young, D.; Chelminski, I.; Dalrymple, K. Severity classification on the Hamilton Depression Rating Scale. J. Affect. Disord. 2013, 150, 384–388. [Google Scholar] [CrossRef] [PubMed]
- Jacobsen, P.B. Assessment of fatigue in cancer patients. J. Natl. Cancer Inst. Monogr. 2004, 32, 93–97. [Google Scholar] [CrossRef] [PubMed]
- Hsu, M.C.; Tu, C.H. Improving quality-of-life outcomes for patients with cancer through mediating effects of depressive symptoms and functional status: A three-path mediation model. J. Clin. Nurs. 2014, 23, 2461–2472. [Google Scholar] [CrossRef] [PubMed]
- Servaes, P.; Verhagen, C.; Bleijenberg, G. Fatigue in cancer patients during and after treatment: Prevalence, correlates and interventions. Eur. J. Cancer 2002, 38, 27–43. [Google Scholar] [CrossRef]
- Beck, S.L.; Dudley, W.N.; Barsevick, A. Pain, sleep disturbance, and fatigue in patients with cancer: Using a mediation model to test a symptom cluster. Oncol. Nurs. Forum 2005, 32. [Google Scholar] [CrossRef]
- Dodd, M.J.; Miaskowski, C.; Paul, S.M. Symptom clusters and their effect on the functional status of patients with cancer. Oncol. Nurs. Forum 2001, 28, 465–470. [Google Scholar] [PubMed]
- Liu, L.; Fiorentino, L.; Natarajan, L.; Parker, B.A.; Mills, P.J.; Sadler, G.R.; Dimsdale, J.E.; Rissling, M.; He, F.; Ancoli-Israel, S. Pre-treatment symptom cluster in breast cancer patients is associated with worse sleep, fatigue and depression during chemotherapy. Psychooncology 2009, 18, 187–194. [Google Scholar] [CrossRef] [PubMed]
- Kreps, G.L.; Sivaram, R. Strategic health communication across the continuum of breast cancer care in limited-resource countries. Cancer 2008, 113 (Suppl. 8), 2331–2337. [Google Scholar] [CrossRef] [PubMed]
- Antoni, M.H.; Wimberly, S.R.; Lechner, S.C.; Kazi, A.; Sifre, T.; Urcuyo, K.R.; Phillips, K.; Smith, R.G.; Petronis, V.M.; Guellati, S.; et al. Reduction of cancer-specific thought intrusions and anxiety symptoms with a stress management intervention among women undergoing treatment for breast cancer. Am. J. Psychiatry 2006, 163, 1791–1797. [Google Scholar] [CrossRef] [PubMed]
- Costanzo, E.S.; Lutgendorf, S.K.; Mattes, M.L.; Trehan, S.; Robinson, C.B.; Tewfik, F.; Roman, S.L. Adjusting to life after treatment: Distress and quality of life following treatment for breast cancer. Br. J. Cancer 2007, 97, 1625–1631. [Google Scholar] [CrossRef] [PubMed]
- Ganz, P.A.; Kwan, L.; Stanton, A.L.; Krupnick, J.L.; Rowland, J.H.; Meyerowitz, B.E.; Bower, J.E.; Belin, T.R. Quality of life at the end of primary treatment of breast cancer: First results from the moving beyond cancer randomized trial. J. Natl. Cancer Inst. 2004, 96, 376–387. [Google Scholar] [CrossRef] [PubMed]
- So, W.K.; Marsh, G.; Ling, W.M.; Leung, F.Y.; Lo, J.C.; Yeung, M.; Li, G.K. The symptom cluster of fatigue, pain, anxiety, and depression and the effect on the quality of life of women receiving treatment for breast cancer: A multicenter study. Oncol. Nurs. Forum 2009, 36, E205–E214. [Google Scholar] [CrossRef] [PubMed]
- Reuter, K.; Classen, C.C.; Roscoe, J.A.; Morrow, G.R.; Kirshner, J.J.; Rosenbluth, R.; Flynn, P.J.; Shedlock, K.; Spiegel, D. Association of coping style, pain, age and depression with fatigue in women with primary breast cancer. Psychooncology 2006, 15, 772–779. [Google Scholar] [CrossRef] [PubMed]
- Reddick, B.K.; Nanda, J.P.; Campbell, L.; Ryman, D.G.; Gaston-Johansson, F. Examining the influence of coping with pain on depression, anxiety, and fatigue among women with breast cancer. J. Psychosoc. Oncol. 2005, 23, 137–157. [Google Scholar] [CrossRef] [PubMed]
- Broeckel, J.A.; Jacobsen, P.B.; Horton, J.; Balducci, L.; Lyman, G.H. Characteristics and correlates of fatigue after adjuvant chemotherapy for breast cancer. J. Clin. Oncol. 1998, 16, 1689–1696. [Google Scholar] [PubMed]
- Bower, J.E. Prevalence and causes of fatigue after cancer treatment: The next generation of research. J. Clin. Oncol. 2005, 23, 8280–8282. [Google Scholar] [CrossRef] [PubMed]
- Edwards, R.R.; Bingham, C.O., 3rd; Bathon, J.; Haythornthwaite, J.A. Catastrophizing and pain in arthritis, fibromyalgia, and other rheumatic diseases. Arthritis Rheum. 2006, 55, 325–332. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Participant Characteristic | Mean | SD |
| Age at diagnosis | 50.34 | 9.03 |
| Positive Lymph Nodes (N = 239) | 1.56 | 3.32 |
| Days since surgery | 40.64 | 23.03 |
| Income, in thousands (N = 213) | 79.62 | 67.08 |
| Years of education | 15.58 | 2.38 |
| Stage of disease | N | Percentage |
| Stage * | ||
| 0 | 38 | 15.8 |
| I | 90 | 37.5 |
| II | 91 | 37.9 |
| III | 19 | 7.9 |
| Type of surgery * | ||
| Lumpectomy | 122 | 50.8 |
| Mastectomy | 118 | 49.2 |
| Menopausal Status | ||
| Pre | 107 | 44.6 |
| Peri/Post | 133 | 55.4 |
| Radiation * | 134 | 55.8 |
| Chemotherapy * | 127 | 52.9 |
| Hormonal Therapy * | 161 | 67.1 |
| Ethnicity | ||
| Non-Hispanic White | 152 | 63.3 |
| Hispanic | 61 | 25.4 |
| African American | 21 | 8.8 |
| Asian | 5 | 2.1 |
| Partnered | 150 | 62.5 |
| Employed | 178 | 74.2 |
| Study Variable | T1 | T2 | T3 |
|---|---|---|---|
| Fatigue Interference | |||
| N | 226 † | 189 | 190 |
| M | 3.63 | 2.88 | 2.53 |
| SD | 1.97 | 1.77 | 1.63 |
| α | 0.9 | 0.9 | 0.9 |
| Pain Severity | |||
| N | 226 † | 189 | 190 |
| M | 2.28 | 1.90 | 1.81 |
| SD | 1.62 | 1.58 | 1.54 |
| α | 0.9 | 0.9 | 0.9 |
| Rejection Issues | |||
| N | 229 † | 184 | 184 |
| M | 3.70 | 3.46 | 3.40 |
| SD | 1.73 | 1.23 | 0.99 |
| α | 0.8 | 0.6 | 0.4 |
| Depressive Symptoms | |||
| N | 231 † | 195 | 180 |
| M | 7.52 | 6.03 | 5.96 |
| SD | 5.46 | 5.10 | 5.02 |
| α | 0.8 | 0.8 | 0.8 |
| Pain Medication | |||
| % (N) Yes | 25.0 (60) | 10.0 (24) | 10.0 (24) |
| % (N) No | 75.0 (180) | 70.4 (169) | 69.2 (166) |
| Anti-Depressants | |||
| % (N) Yes * | 10.8 (26) | 9.6 (23) | 12.1 (29) |
| % (N) No | 89.2 (214) | 70.8 (170) | 67.1 (161) |
| Sleep Medication | |||
| % (N) Yes | 17.9 (43) | 9.2 (22) | 11.7 (28) |
| % (N) No | 82.1 (197) | 70.8 (170) | 67.9 (163) |
| Anti-Anxiety Medication | |||
| % (N) Yes | 17.5 (42) | 12.1 (29) | 14.2 (34) |
| % (N) No | 82.5 (198) | 68.3 (164) | 65.0 (156) |
© 2016 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Amiel, C.R.; Fisher, H.M.; Antoni, M.H. Concerns about Breast Cancer, Pain, and Fatigue in Non-Metastatic Breast Cancer Patients Undergoing Primary Treatment. Healthcare 2016, 4, 62. https://doi.org/10.3390/healthcare4030062
Amiel CR, Fisher HM, Antoni MH. Concerns about Breast Cancer, Pain, and Fatigue in Non-Metastatic Breast Cancer Patients Undergoing Primary Treatment. Healthcare. 2016; 4(3):62. https://doi.org/10.3390/healthcare4030062
Chicago/Turabian StyleAmiel, Chelsea R., Hannah M. Fisher, and Michael H. Antoni. 2016. "Concerns about Breast Cancer, Pain, and Fatigue in Non-Metastatic Breast Cancer Patients Undergoing Primary Treatment" Healthcare 4, no. 3: 62. https://doi.org/10.3390/healthcare4030062