
Association between Vitamin D Status and Coronary Heart Disease among Adults in Saudi Arabia: A Case-Control Study


Abstract
:1. Introduction
2. Materials and Methods
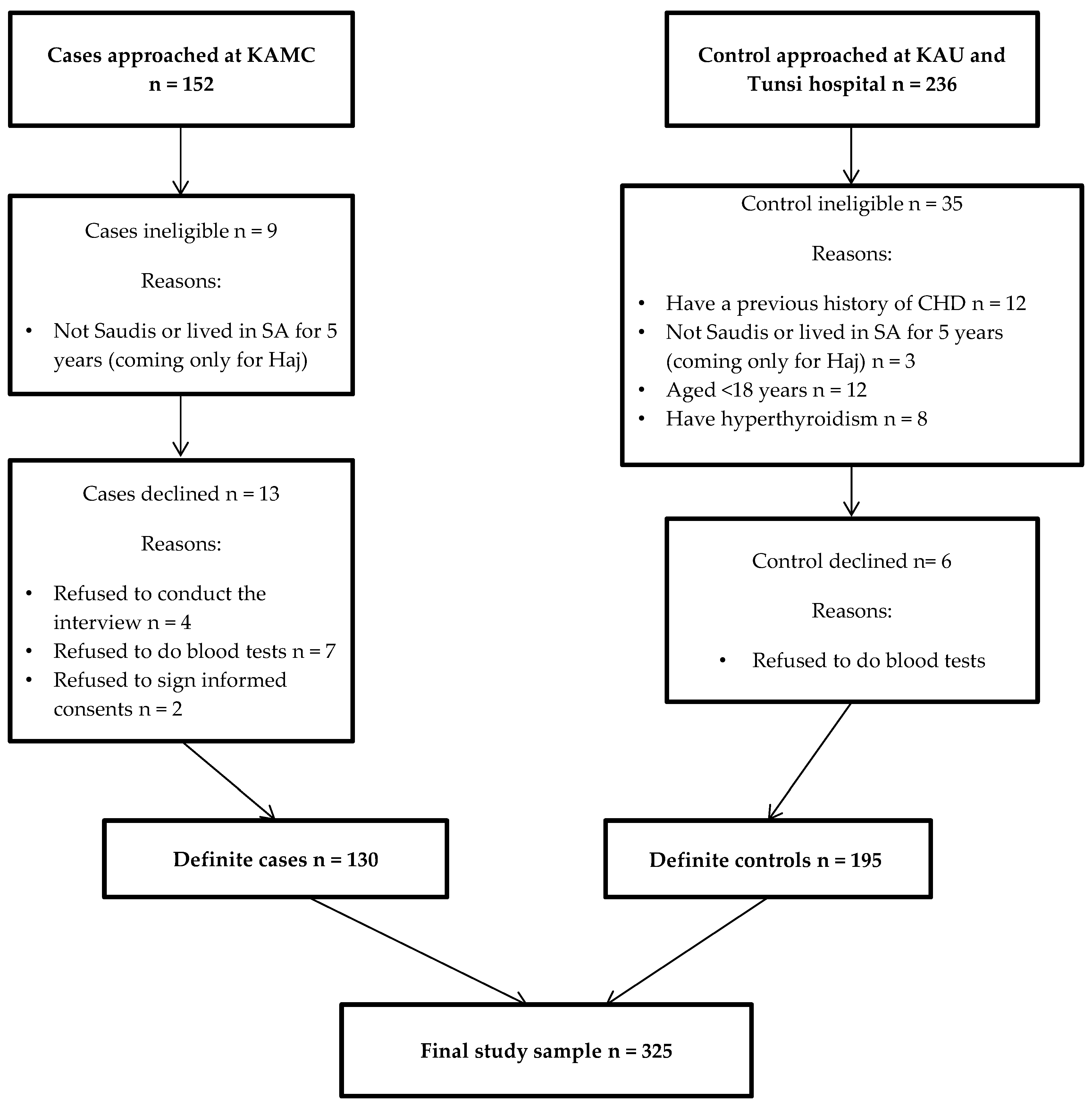
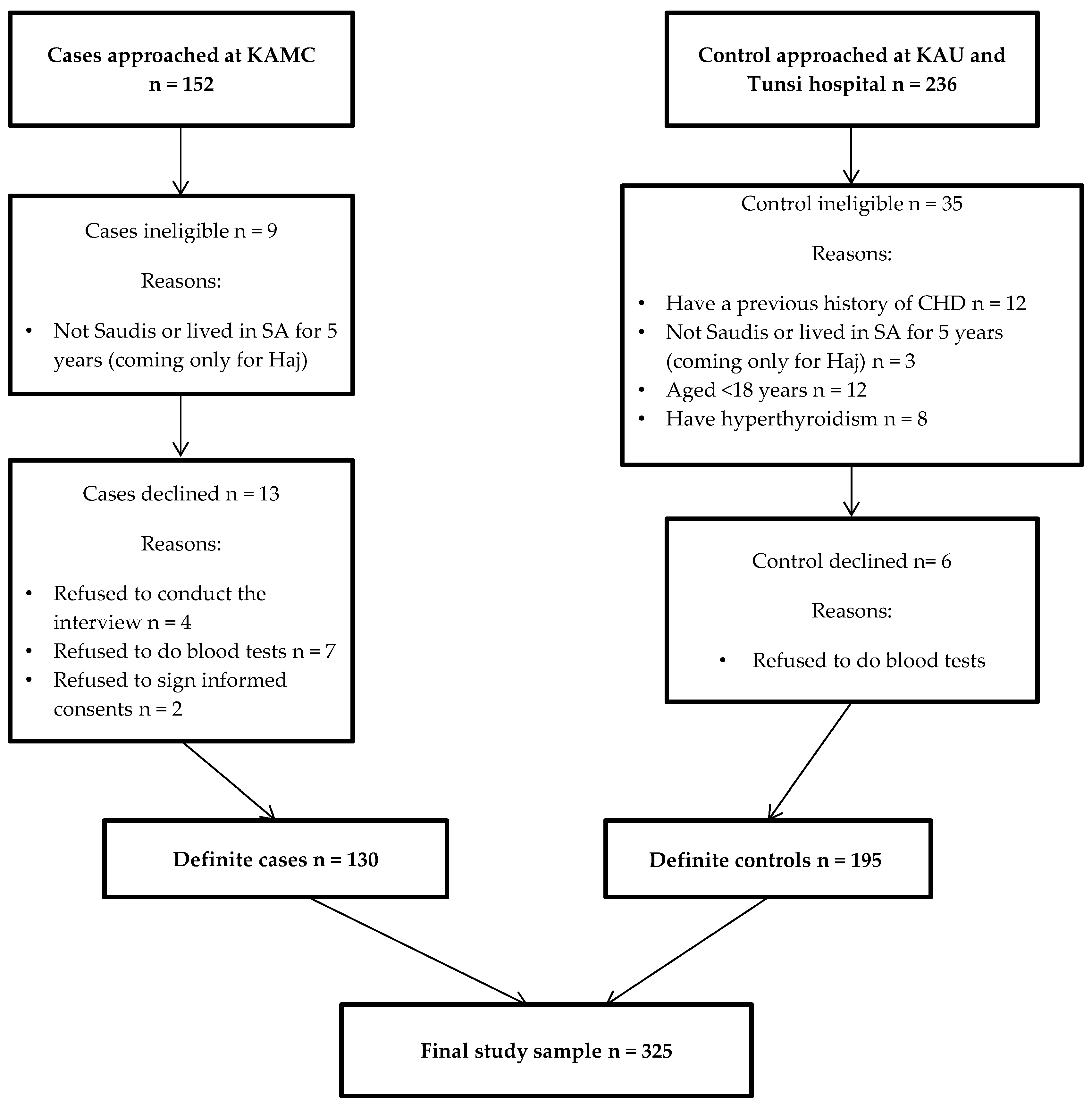
2.1. Study Design and Population
2.2. Inclusion and Exclusion Criteria
2.3. Data Collection
2.4. Biochemical Measurements
2.5. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Aljefree, N.; Ahmed, F. Prevalence of cardiovascular disease and associated risk factors among adult population in the Gulf region: A systematic review. Adv. Public Health 2015. [Google Scholar] [CrossRef]
- Kumosani, T.A.; Alama, M.N.; Iyer, A. Cardiovascular disease in Saudi Arabia. Prime. Res. Med. 2007, 1, 1–6. [Google Scholar]
- Al-Nozha, M.M.; Arafah, M.R.; Al-Mazrou, Y.Y.; Al-Maatouq, M.A.; Khan, N.B.; Khalil, M.Z.; Al-Khadra, A.H.; Al-Marzouki, K.; Abdullah, M.A.; Al-Harthi, S.S. Coronary artery disease in Saudia Arabia. Saudi Med. J. 2004, 25, 1165–1171. [Google Scholar] [PubMed]
- Al-Nozha, M.M.; Arafah, M.R.; Al-Maatouq, M.A.; Khalil, M.Z.; Khan, N.B.; Al-Marzouki, K.; Al-Mazrou, Y.Y.; Abdullah, M.; Al-Khadra, A.; Al-Harthi, S.S. Hyperlipidemia in Saudi Arabia. Saudi Med. J. 2008, 29, 282–287. [Google Scholar]
- Al-Nozha, M.M.; Al-Mazrou, Y.Y.; Al-Maatouq, M.A.; Arafah, M.R.; Khalil, M.Z.; Khan, N.B.; Al-Marzouki, K.; Abdullah, M.A.; Al-Khadra, A.H.; Al-Harthi, S.S. Obesity in Saudi Arabia. Saudi Med. J. 2005, 26, 824–829. [Google Scholar] [PubMed]
- Al-Nozha, M.M.; Al-Maatouq, M.A.; Al-Mazrou, Y.Y.; Al-Harthi, S.S.; Arafah, M.R.; Khalil, M.Z.; Khan, N.B.; Al-Khadra, A.; Al-Marzouki, K.; Nouh, M.S. Diabetes mellitus in Saudi Arabia. Saudi Med. J. 2004, 25, 1603–1610. [Google Scholar] [PubMed]
- Al-Nozha, M.M.; Abdullah, M.; Arafah, M.R.; Al-Maatouq, M.A.; Al-Marzouki, K.; Al-Khadra, A.; Nouh, M.S.; Al-Harthi, S.S.; Al-Shahid, M.S.; Al-Mobeireek, A. Hypertension in Saudi Arabia. Saudi Med. J. 2007, 28, 77–84. [Google Scholar] [PubMed]
- Aljefree, N.; Ahmed, F. Association between dietary pattern and risk of cardiovascular disease among adults in the Middle East and North Africa region: A systematic review. Food Nutr. Res. 2015, 59. [Google Scholar] [CrossRef] [PubMed]
- Nitta, K. Impact of vitamin D metabolism on cardiovascular disease. Int. J. Clin. Med. 2011, 2. [Google Scholar] [CrossRef]
- Judd, S.E.; Tangpricha, V. Vitamin D deficiency and risk for cardiovascular disease. Am. J. Med. Sci. 2009, 338, 40. [Google Scholar] [CrossRef] [PubMed]
- Wang, T.J.; Pencina, M.J.; Booth, S.L.; Jacques, P.F.; Ingelsson, E.; Lanier, K.; Benjamin, E.J.; D’Agostino, R.B.; Wolf, M.; Vasan, R.S. Vitamin D deficiency and risk of cardiovascular disease. Circulation 2008, 117, 503–511. [Google Scholar] [CrossRef] [PubMed]
- Kim, D.H.; Sabour, S.; Sagar, U.N.; Adams, S.; Whellan, D.J. Prevalence of hypovitaminosis D in cardiovascular diseases (from the national health and nutrition examination survey 2001 to 2004). Am. J. Cardiol. 2008, 102, 1540–1544. [Google Scholar] [CrossRef] [PubMed]
- Wang, L.; Song, Y.; Manson, J.E.; Pilz, S.; März, W.; Michaëlsson, K.; Lundqvist, A.; Jassal, S.K.; Barrett-Connor, E.; Zhang, C. Circulating 25-hydroxy-vitamin D and risk of cardiovascular disease a meta-analysis of prospective studies. Circulation 2012, 5, 819–829. [Google Scholar] [CrossRef] [PubMed]
- Schöttker, B.; Jorde, R.; Peasey, A.; Thorand, B.; Jansen, E.H.; de Groot, L.; Streppel, M.; Gardiner, J.; Ordóñez-Mena, J.M.; Perna, L. Vitamin D and mortality: meta-analysis of individual participant data from a large consortium of cohort studies from Europe and the United States. Br. Med. J. 2014, 348, g3656. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hosseinpanah, F.; Yarjanli, M.; Sheikholeslami, F.; Heibatollahi, M.; Eskandary, P.S.; Azizi, F. Associations between vitamin D and cardiovascular outcomes; Tehran lipid and glucose study. Atherosclerosis 2011, 218, 238–242. [Google Scholar] [CrossRef] [PubMed]
- El-Menyar, A.; Rahil, A.; Dousa, K.; Ibrahim, W.; Ibrahim, T.; Khalifa, R.; Rahman, M.O.A. Low vitamin D and cardiovascular risk factors in males and females from a sunny, rich country. Open Cardiovasc. Med. J. 2012, 6, 76–80. [Google Scholar] [CrossRef] [PubMed]
- Elsammak, M.; Al-Wossaibi, A.; Al-Howeish, A.; Alsaeed, J. High prevalence of vitamin D deficiency in the sunny Eastern region of Saudi Arabia: A hospital-based study. East. Mediterr. Health J. 2011, 17, 317–322. [Google Scholar] [PubMed]
- Ghannam, N.; Hammami, M.; Bakheet, S.; Khan, B. Bone mineral density of the spine and femur in healthy Saudi females: Relation to vitamin D status, pregnancy, and lactation. Calcif. Tissue Int. 1999, 65, 23–28. [Google Scholar] [CrossRef] [PubMed]
- Sadat-Ali, M.; AlElq, A.; Al-Turki, H.; Al-Mulhim, F.; Al-Ali, A. Vitamin D levels in healthy men in eastern Saudi Arabia. Ann. Saudi Med. 2009, 29, 378–382. [Google Scholar] [CrossRef] [PubMed]
- Naeem, Z.; AlMohaimeed, A.; Sharaf, F.K.; Ismail, H.; Shaukat, F.; Inam, S.B. Vitamin D status among population of Qassim Region, Saudi Arabia. Int. J. Health Sci. 2011, 5, 116–117. [Google Scholar]
- Alfawaz, H.; Tamim, H.; Alharbi, S.; Aljaser, S.; Tamimi, W. Vitamin D status among patients visiting a tertiary care center in Riyadh, Saudi Arabia: A retrospective review of 3475 cases. BMC Public Health 2014, 14, 159–160. [Google Scholar] [CrossRef] [PubMed]
- Sedrani, S.H.; Elidrissy, A.; El Arabi, K.M. Sunlight and vitamin D status in normal Saudi subjects. Am. J. Clin. Nutr. 1983, 38, 129–132. [Google Scholar] [PubMed]
- Ardawi, M.-S.; Sibiany, A.; Bakhsh, T.; Qari, M.; Maimani, A. High prevalence of vitamin D deficiency among healthy Saudi Arabian men: Relationship to bone mineral density, parathyroid hormone, bone turnover markers, and lifestyle factors. Osteoporos. Int. 2012, 23, 675–686. [Google Scholar] [CrossRef] [PubMed]
- Ardawi, M.-S.; Qari, M.; Rouzi, A.; Maimani, A.; Raddadi, R. Vitamin D status in relation to obesity, bone mineral density, bone turnover markers and vitamin D receptor genotypes in healthy Saudi pre-and postmenopausal women. Osteoporos. Int. 2011, 22, 463–475. [Google Scholar] [CrossRef] [PubMed]
- Holick, M.F. Vitamin D deficiency. N. Engl. J. Med. 2007, 357, 266–281. [Google Scholar] [CrossRef] [PubMed]
- Wells, S.; Broad, J.; Jackson, R. Alcohol consumption and its contribution to the burden of coronary heart disease in middle-aged and older New Zealanders: A population-based case-control study. Available online: https://researchspace.auckland.ac.nz/handle/2292/4707 (accessed on 1 July 2016).
- Shaikh, R.; Vijayaraghavan, N.; Sulaiman, A.; Kazi, S.; Shafi, M. The acute effects of waterpipe smoking on the cardiovascular and respiratory systems. J. Prev. Med. Hyg. 2008, 49. [Google Scholar] [CrossRef]
- Shils, M.E.; Shike, M. Modern Nutrition in Health and Disease, 1st ed.; Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2006. [Google Scholar]
- Gallagher, J.C.; Sai, A.J. Vitamin D insufficiency, deficiency, and bone health. J. Clini. Endocrinol. Metab. 2010, 95, 2630–2633. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.H.; Gadi, R.; Spertus, J.A.; Tang, F.; O’Keefe, J.H. Prevalence of vitamin D deficiency in patients with acute myocardial infarction. Am. J. Cardiol. 2011, 107, 1636–1638. [Google Scholar] [CrossRef] [PubMed]
- Giovannucci, E.; Liu, Y.; Hollis, B.W.; Rimm, E.B. 25-Hydroxyvitamin D and risk of myocardial infarction in men: A prospective study. Arch. Int. Med. 2008, 168, 1174–1180. [Google Scholar] [CrossRef] [PubMed]
- Scragg, R.; Jackson, R.; Holdaway, I.M.; Lim, T.; Beaglehole, R. Myocardial infarction is inversely associated with plasma 25-hydroxyvitamin D3 levels: A community-based study. Int. J. Epidemiol. 1990, 19, 559–563. [Google Scholar] [CrossRef] [PubMed]
- Kendrick, J.; Targher, G.; Smits, G.; Chonchol, M. 25-Hydroxyvitamin D deficiency is independently associated with cardiovascular disease in the third national health and nutrition examination survey. Atherosclerosis 2009, 205, 255–260. [Google Scholar] [CrossRef] [PubMed]
- Roy, A.; Lakshmy, R.; Tarik, M.; Tandon, N.; Reddy, K.S.; Prabhakaran, D. Independent association of severe vitamin D deficiency as a risk of acute myocardial infarction in Indians. Indian Heart J. 2015, 67, 27–32. [Google Scholar] [CrossRef] [PubMed]
- Ross, A.C.; Taylor, C.L.; Yaktine, A.L.; Del Valle, H.B. Dietary Reference Intakes for Calcium and Vitamin D, 1st ed.; National Academies Press: Washington, WA, USA, 2011. [Google Scholar]
- Nemerovski, C.W.; Dorsch, M.P.; Simpson, R.U.; Bone, H.G.; Aaronson, K.D.; Bleske, B.E. Vitamin D and cardiovascular disease. J. Hum. Pharmacol. Drug Ther. 2009, 29, 691–708. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Manson, J.E. Vitamin D and the heart: Why we need large-scale clinical trials. Clevel. Clin. J. Med. 2010, 77, 903–910. [Google Scholar] [CrossRef] [PubMed]
- Alsuwaida, A.O.; Farag, Y.M.; Al Sayyari, A.A.; Mousa, D.H.; Alhejaili, F.F.; Al-Harib, A.S.; Housawi, A.A.; Mittal, B.V.; Singh, A.K. Prevalence of vitamin D deficiency in Saudi adults. Saudi Med. J. 2013, 34, 814–818. [Google Scholar]
- Tuffaha, M.; El Bcheraoui, C.; Daoud, F.; Al Hussaini, H.A.; Alamri, F.; Al Saeedi, M.; Basulaiman, M.; Memish, Z.A.; AlMazroa, M.A.; Al Rabeeah, A.A. Deficiencies under plenty of sun: Vitamin D status among adults in the kingdom of Saudi Arabia, 2013. N. Am. J. Med. Sci. 2015, 7, 467–475. [Google Scholar]

{kind=link}
| Variable | Cases (n = 130)% | Control (n = 195)% | p-Value |
|---|---|---|---|
| Age (years) | |||
| <49 | 25 | 30 | |
| ≥49 | 75 | 70 | 0.340 |
| Gender | |||
| Male | 63 | 63 | |
| Female | 37 | 37 | >0.05 |
| Marital status | |||
| Single | 5 | 17 | |
| Married | 70 | 72 | <0.001 |
| Divorced | 25 | 11 | |
| Citizenship | |||
| Saudis | 81 | 63 | |
| Non-Saudis | 19 | 37 | <0.001 |
| Place of residence | |||
| Rural | 12 | 1 | |
| Urban | 86 | 98 | |
| Semi-rural | 2 | 1 | <0.001 |
| Education | |||
| Up to primary levels | 51 | 14 | |
| High School and bachelor or diploma degree | 25 | 35 | <0.001 |
| Master or PhD degree | 24 | 51 | |
| Employment | |||
| Employed (Full time, Part time, self-employed) | 32 | 82 | |
| Unemployed (Student, Retired, Housewife) | 68 | 18 | <0.001 |
| Family income (SR */monthly) | |||
| <5000 | 72 | 69 | |
| 5000–15000 | 10 | 19 | |
| 15000 ≥ 25000 | 18 | 12 | 0.036 |
| Smoke cigarettes | |||
| Current <20 cigarettes/day | 15 | 10 | |
| Previous smoker | 26 | 5 | |
| Non-smoker | 59 | 85 | <0.001 |
| Water pipe smoker | |||
| Yes | 3 | 10 | |
| No | 97 | 90 | 0.022 |
| Moderate exercise | |||
| Never and rarely | 34 | 44 | |
| 1–2 times/week | 17 | 24 | |
| More than 3–4 times/week | 49 | 32 | 0.007 |
| Vigorous exercise | |||
| Never and rarely | 98 | 96 | |
| 1–2 times/week | 1 | 0 | |
| More than 3–4 times/week | 1 | 4 | 0.259 |
| Family history of CVD | |||
| Yes | 41 | 42 | |
| No | 59 | 58 | 0.890 |
| Variable | Cases (n = 130)% | Control (n = 195)% | p-Value |
|---|---|---|---|
| BMI | |||
| Normal weight < 25 kg/m² | 31 | 33 | |
| Overweight 25–29.9 kg/m² | 25 | 45 | <0.001 |
| Obese ≥ 30 kg/m² | 44 | 22 | |
| SBP | |||
| <112.58 mmHg | 35 | 31 | |
| 112.59–128.42 mmHg | 29 | 38 | 0.031 |
| ≥128.43 mmHg | 36 | 31 | |
| DBP | |||
| <69.58 mmHg | 56 | 17 | |
| 69.59–79 mmHg | 23 | 43 | <0.001 |
| ≥79.1 mmHg | 21 | 40 | |
| Fasting glucose (FPG) | |||
| <93 mg/dL | 21 | 42 | |
| 93.1–112.42 mg/dL | 28 | 37 | <0.001 |
| ≥112.43 mg/dL | 51 | 21 | |
| Total Cholesterol | |||
| <154 mg/dL | 56 | 20 | |
| 154.1–193 mg/dL | 28 | 37 | <0.001 |
| ≥193.1 mg/dL | 16 | 43 | |
| Vitamin D | |||
| Adequate ≥ 20 ng/mL | 24 | 61 | |
| Insufficient 10 to < 19.9 ng/mL | 30 | 36 | <0.001 |
| Deficiency < 10 ng/mL | 46 | 3 |
| Vitamin D status | Crude OR 1 (95% CI) | Adjusted OR 2 (95% CI) | Adjusted OR 3 (95% CI) |
|---|---|---|---|
| Adequate (≥20 ng/mL) | 1.00 (referent) | 1.00 (referent) | 1.00 (referent) |
| Deficient (<20 ng/mL) * | 5 (3.04–8.20) <0.001 | 7.8 (3.79–16.3) <0.001 | 6.5 (2.7–15) <0.001 |
© 2016 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Aljefree, N.M.; Lee, P.; Alsaqqaf, J.M.; Ahmed, F. Association between Vitamin D Status and Coronary Heart Disease among Adults in Saudi Arabia: A Case-Control Study. Healthcare 2016, 4, 77. https://doi.org/10.3390/healthcare4040077
Aljefree NM, Lee P, Alsaqqaf JM, Ahmed F. Association between Vitamin D Status and Coronary Heart Disease among Adults in Saudi Arabia: A Case-Control Study. Healthcare. 2016; 4(4):77. https://doi.org/10.3390/healthcare4040077
Chicago/Turabian StyleAljefree, Najlaa M., Patricia Lee, Jamal M. Alsaqqaf, and Faruk Ahmed. 2016. "Association between Vitamin D Status and Coronary Heart Disease among Adults in Saudi Arabia: A Case-Control Study" Healthcare 4, no. 4: 77. https://doi.org/10.3390/healthcare4040077