
A Holistic Model of Care to Support Those Living with and beyond Cancer


{kind=link}
Abstract
:1. Introduction
1.1. Holistic Cancer Care
- Integrated care models emphasize a patient centered approach;
- Services are provided in a consistent approach across a range of providers, not just one organization or provider;
- Patients should have access to high quality care as close to home as possible assuming the availability of equipment and resources exist;
- Shared protocols, guidelines, and care pathways ensure consistency of care;
- Comprehensive screening for supportive care needs is critical to ensuring holistic care for cancer patients [17]
1.2. Survivorship Care in Australia
2. Methods
2.1. Design
2.2. Model of Care
2.3. BCC Philosophy
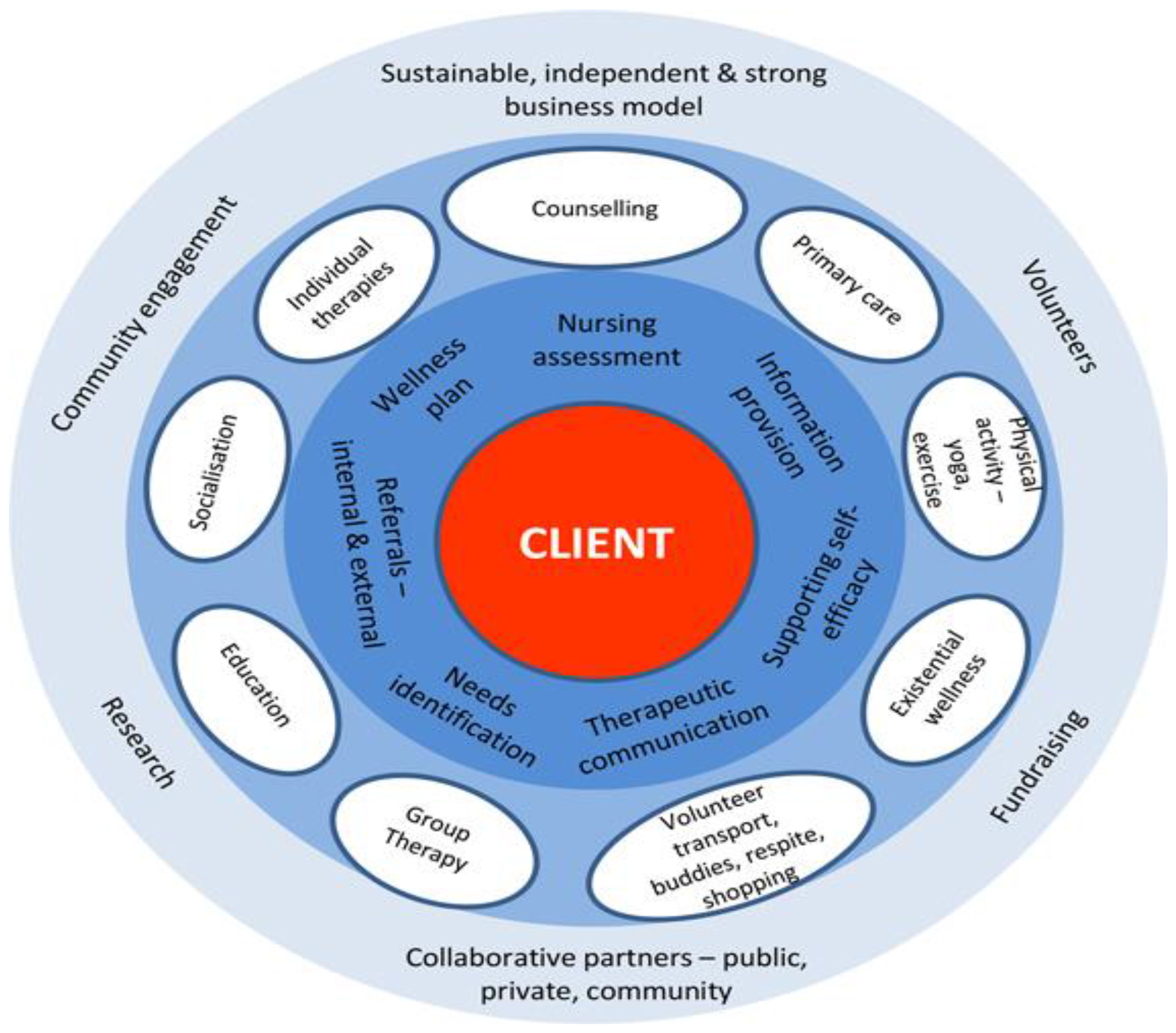
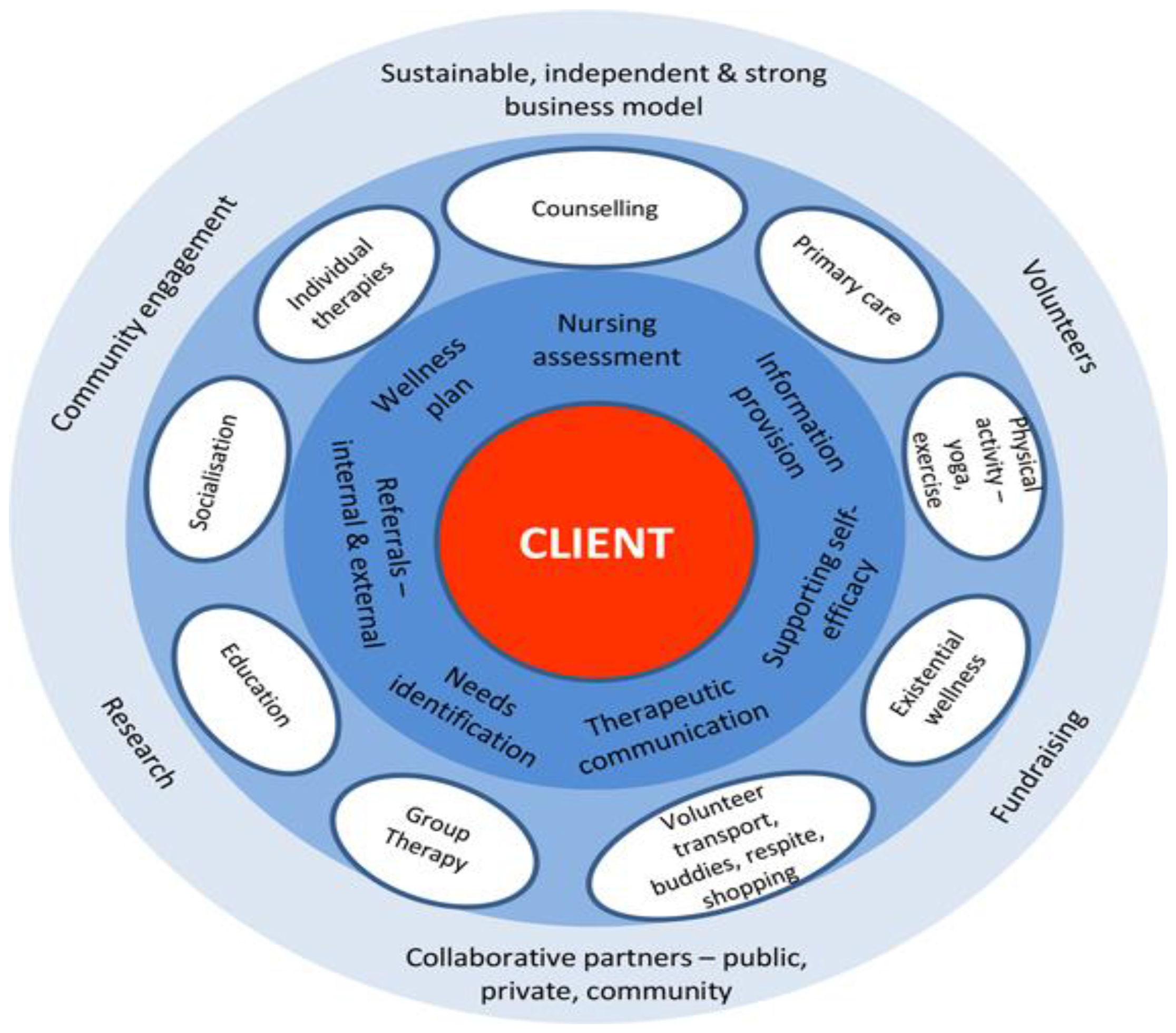
2.4. Description of the Model
- Ongoing support from experienced oncology registered nurses;
- Access to support and information from cancer clinical nurse specialists;
- Support groups for the patient and carer (e.g., Living with Cancer treatment, Chemo Brain support group);
- Qualified Allied Health Care, including clinical psychology, counsellors, dietician, and exercise physiology services;
- Free counselling services;
- Lymphoedema management; and Complementary services (e.g., Touch therapies, Meditation, Mindfulness, Yoga).
2.5. Child and Adolescent and Young Adult Services
3. Results
Results of Client Survey of Needs
4. Discussion and Conclusions
Author Contributions
Conflicts of Interest
References
- Centers for Disease Control. Available online: http://www.cdc.gov/cancer/international/statistics.htm (accessed on 6 June 2016).
- Jemal, A.; Bray, F.; Center, M.M.; Ferlay, J.; Ward, E.; Forman, D. Global cancer statistics. CA Cancer J. Clin. 2011, 61, 69–90. [Google Scholar] [CrossRef] [PubMed]
- American Cancer Society. Available online: http://www.cancer.org/acs/groups/content/@research/documents/document/acspc-047079.pdf (accessed on 6 June 2016).
- American Cancer Society. Available online: http://www.cancer.org/acs/groups/content/@research/documents/document/acspc-044738.pdf (accessed on 6 June 2016).
- Australian Institute of Health and Welfare. Cancer Survival and Prevalence in Australia: Period Estimates from 1982 to 2010. Cancer Series No. 69. Cat. No. CAN 65; 2012. Available online: http://www.aihw.gov.au/WorkArea/DownloadAsset.aspx?id=10737422721 (accessed on 6 June 2016). [Google Scholar]
- Hewitt, M.; Greenfield, S.; Stovall, E. From Cancer Patient to Cancer Survivor: Lost in Transition. Committee on Cancer Survivorship: Improving Care and Quality of Life, Institute of Medicine and National Research Council. 2006. Available online: http://www.nationalacademies.org/hmd/Reports/2005/From-Cancer-Patient-to-Cancer-Survivor-Lost-in-Transition.aspx (accessed on 10 October 2016).
- Jefford, M.; Karahalios, E.; Pollard, A.; Baravelli, C.; Carey, M.; Franklin, J.; Aranda, S.; Schofield, P. Survivorship issues following treatment completion—Results from focus groups with Australian cancer survivors and health professionals. J. Cancer Surviv. 2008, 2, 20–32. [Google Scholar] [CrossRef] [PubMed]
- McCabe, M.S.; Bhatia, S.; Oeffinger, K.C.; Reaman, G.H.; Tyne, C.; Wollins, D.S.; Hudson, M.M. American Society of Clinical Oncology statement: Achieving high-quality cancer survivorship care. J. Clin. Oncol. 2013, 31, 631–640. [Google Scholar] [CrossRef] [PubMed]
- Borras, J.M.; Albreht, T.; Audisio, R.; Briers, E.; Casali, P.; Esperou, H.; Grube, B.; Hamoir, M.; Henning, G.; Kelly, J.; et al. Policy statement on multidisciplinary cancer care. Eur. J. Cancer 2014, 50, 475–480. [Google Scholar] [CrossRef] [PubMed]
- Hanan, T.; Mullen, L.; Laffoy, M.; O’Toole, E.; Richmond, J.; Wynne, M. Delivering care to oncology patients in the community: An innovative integrated approach. Br. J. Commun. Nurs. 2014, 19, 382–387. [Google Scholar] [CrossRef] [PubMed]
- Jefford, M. Improving outcomes for cancer survivors in Australia. In Cancer Forum; The Cancer Council Australia: Sydney, Australia, 2009; Volume 33, p. 159. [Google Scholar]
- Berman, B. Integrative approaches to pain management: How to get the best of both worlds. Br. Med. J. 2003, 326, 1320–1321. [Google Scholar] [CrossRef] [PubMed]
- Cramer, H.; Cohen, L.; Dobos, G.; Witt, C.M. Integrative oncology: Best of both worlds—Theoretical, practical, and research issues. Evid.-Based Complement. Altern. Med. 2013. [Google Scholar] [CrossRef] [PubMed]
- Deng, G.; Weber, W.; Sood, A.; Kemper, K. Integrative Medicine Research: Context and Priorities. Available online: https://www.nationalacademies.org/hmd/~/media/Files/Activity%20Files/Quality/IntegrativeMed/Integrative%20Medicine%20Research%20--%20Context%20and%20Priorities.pdf (accessed on 7 June 2016).
- Romeyke, T.; Stummer, H. Economic aspects of nursing in inpatient naturopathy: Evidence from Germany. Nurs. Econ. 2013, 31, 137–143. [Google Scholar] [PubMed]
- Weil, A. Why integrative oncology? In Integrative Oncology; Abrams, D., Weil, A., Eds.; Oxford University Press: Oxford, UK, 2014; pp. 1–12. [Google Scholar]
- Rushton, M.; Morash, R.; Larocque, G.; Liska, C.; Stoica, L.; DeGrasse, C.; Segal, R. Wellness Beyond Cancer Program: building an effective survivorship program. Curr. Oncol. 2015, 22, e419–e434. [Google Scholar] [CrossRef] [PubMed]
- Bower, W.F.; Vlantis, A.C.; Chung, T.M.; van Hasselt, C.A. Mode of treatment affects quality of life in head and neck cancer survivors: Implications for holistic care. Acta Otolaryngol. 2010, 130, 1185–1192. [Google Scholar] [CrossRef] [PubMed]
- Hanahan, D. Rethinking the war on cancer. Lancet 2014, 383, 558–563. [Google Scholar] [CrossRef]
- Schloss, J.; Steel, A. Thriving after cancer: The role of integrative medicine (IM) in cancer survivorship and wellbeing programs. Adv. Integr. Med. 2015, 2, 123–124. [Google Scholar] [CrossRef]
- American Cancer Society. Available online: http://www.cancer.org/acs/groups/content/@research/documents/document/acspc-042801.pdf (accessed on 6 June 2016).
- Simard, S.; Thewes, B.; Humphris, G.; Dixon, M.; Hayden, C.; Mireskandari, S.; Ozakinci, G. Fear of cancer recurrence in adult cancer survivors: A systematic review of quantitative studies. J. Cancer Surviv. 2013, 7, 300–322. [Google Scholar] [CrossRef] [PubMed]
- Davies, N.J.; Batehup, L. Towards a personalised approach to aftercare: A review of cancer follow-up in the UK. J. Cancer Surviv. 2011, 5, 142–151. [Google Scholar] [CrossRef] [PubMed]
- Keesing, S.; McNamara, B.; Rosenwax, L. Cancer survivors’ experiences of using survivorship care plans: A systematic review of qualitative studies. J. Cancer Surviv. 2015, 9, 260–268. [Google Scholar] [CrossRef] [PubMed]
- Briggs, J. Building the evidence base for integrative approaches to care of cancer survivors. J. Natl. Cancer Inst. Monogr. 2014, 2014, 288. [Google Scholar] [CrossRef] [PubMed]
- Adler, N.E.; Page, A.E.K. (Eds.) Cancer Care for the Whole Patient: Meeting Psychosocial Health Needs; National Academies Press: Washington, DC, USA, 2008.
- Beaver, K.; Luker, K.A. Follow-up in breast cancer clinics: Reassuring for patients rather than detecting recurrence. Psychooncology 2005, 14, 94–101. [Google Scholar] [CrossRef] [PubMed]
- Salz, T.; Oeffinger, K.C.; McCabe, M.S.; Layne, T.M.; Bach, P.B. Survivorship care plans in research and practice. CA Cancer J. Clin. 2012, 62, 101–117. [Google Scholar] [CrossRef] [PubMed]
- Jefford, M.; Rowland, J.; Grunfeld, E.; Richards, M.; Maher, J.; Glaser, A. Implementing improved post-treatment care for cancer survivors in England, with reflections from Australia, Canada and the USA. Br. J. Cancer 2013, 108, 14–20. [Google Scholar] [CrossRef] [PubMed]
- Coory, M.D.; Ho, T.; Jordan, S.J. Australia is continuing to make progress against cancer, but the regional and remote disadvantage remains. Med. J. Aust. 2013, 199, 605–608. [Google Scholar] [CrossRef] [PubMed]
- Australia Institute of Health and Welfare. Remoteness Classifications. Available online: http://www.aihw.gov.au/rural-health-remoteness-classifications (accessed on 7 June 2016).
- Adams, P.; Hardwick, J.; Embree, V.; Sinclair, S.; Conn, B.; Bishop, J. Literature Review: Models of Cancer Services for Rural and Remote Communities. Available online: http://www.cancerinstitute.org.au/media/70218/web09-83-02_literature_review_models_cancer_services_rural_and_remote_communities.pdf (accessed on 7 June 2016).
- Beckmann, K.R.; Bennett, A.; Young, G.P.; Cole, S.R.; Joshi, R.; Adams, J.; Singhal, N.; Karapetis, C.; Wattchow, D.; Roder, D. Sociodemographic disparities in survival from colorectal cancer in South Australia: A population-wide data linkage study. BMC Health Serv. Res. 2016, 16, 24. [Google Scholar] [CrossRef] [PubMed]
- Queensland Cancer Registry. Cancer in Queensland, Incidence, Mortality, Survival and Prevalence 1982–2012. 2014. Available online: https://cancerqld.org.au/wp-content/uploads/2015/11/fact-sheet-cancer-in-queensland.pdf (accessed on 7 June 2016).
- Oliver-Baxter, J.; Brown, L.; O’Connor, J.; Lunnay, B.; Bywood, P. Integrated Care: What Can Be Done at the Micro Level to Influence Integration in Primary Health Care; PHCRIS Policy Issue Review; Primary Health Care Research & Information Service: Adelaide, Australia, 2013; Available online: http://www.phcris.org.au/phplib/filedownload.php?file=/elib/lib/downloaded_files/publications/pdfs/phcris_pub_8417.pdf (accessed on 7 June 2016).
- Cancer Council Queensland. Queensland Cancer Statistics On-Line. 2014. Available online: www.cancerqld.org.au/research/qcsol (accessed on 7 June 2016).
- Cancer Council Queensland. 2014 Sunshine Coast Region Impact Statement. Available online: https://cancerqld.org.au/wp-content/uploads/2015/12/regional-impact-statement_sunshinecoastregion2014.pdf (accessed on 7 June 2016).
- Debono, D.; Travaglia, J. Complaints and Patient Satisfaction: A Comprehensive Review of the Literature. Available online: https://www2.health.vic.gov.au/about/publications/researchandreports/toolkit-lit-review (accessed on 15 June 2016).
- NSW Government Health. Integrated Care Strategy 2014–2017. Available online: http://www.health.nsw.gov.au/integratedcare/Documents/integrated-care-info-summary.pdf (accessed on 7 June 2016).
- Bloomhill Cancer Center. Welcome Booklet. Available online: http://www.bloomhill.com.au/about-bloomhill/index.html (accessed on 9 June 2016).
- National Wellness Institute. Six Dimensions of Wellness Model. Available online: http://c.ymcdn.com/sites/www.nationalwellness.org/resource/resmgr/docs/sixdimensionsfactsheet.pdf (accessed on 10 June 2016).
- Kazak, A.E.; Rourke, M.T.; Alderfer, M.A.; Pai, A.; Reilly, A.F.; Meadows, A.T. Evidence-based assessment, intervention and psychosocial care in pediatric oncology: A blueprint for comprehensive services across treatment. J. Pediatr. Psychol. 2007, 32, 1099–1110. [Google Scholar] [CrossRef] [PubMed]
- Paediatric Integrated Cancer Service. Addressing psychosocial concerns in children affected by cancer. Available online: http://www.pics.org.au/Psychologicalimpactofdiagnosisandtreatment (accessed on 10 June 2016).
- Clinical Oncology Society of Australia. Psychosocial Management of AYAs Diagnosed with Cancer: Guidance for Health Professionals. Available online: http://wiki.cancer.org.au/australia/COSA:Psychosocial_management_of_AYA_cancer_patients (accessed on 10 June 2016).
- Siegrist, R.B., Jr. Patient satisfaction: history, myths, and misperceptions. Virtual Mentor 2013, 15, 982–987. [Google Scholar] [PubMed]
- Cancer Council Queensland. Breast cancer. Available online: https://cancerqld.org.au/wp-content/uploads/2015/11/fact-sheet-breast-cancer.pdf (accessed on 13 June 2016).
© 2016 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cadet, T.; Davis, C.; Elks, J.; Wilson, P. A Holistic Model of Care to Support Those Living with and beyond Cancer. Healthcare 2016, 4, 88. https://doi.org/10.3390/healthcare4040088
Cadet T, Davis C, Elks J, Wilson P. A Holistic Model of Care to Support Those Living with and beyond Cancer. Healthcare. 2016; 4(4):88. https://doi.org/10.3390/healthcare4040088
Chicago/Turabian StyleCadet, Tamara, Cindy Davis, Jacinta Elks, and Patricia Wilson. 2016. "A Holistic Model of Care to Support Those Living with and beyond Cancer" Healthcare 4, no. 4: 88. https://doi.org/10.3390/healthcare4040088