Assessing Clinical Outcomes in Colorectal Cancer with Assays for Invasive Circulating Tumor Cells

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patient and Clinical Samples
2.2. Clinical Data Collection
2.3. Cell Culture, Identification of CTCs and iCTCs, and Functional Proliferation/Invasion Assays
2.4. Microarray Data Analysis
2.5. Statistical Analysis
3. Results
3.1. Patient Characteristics
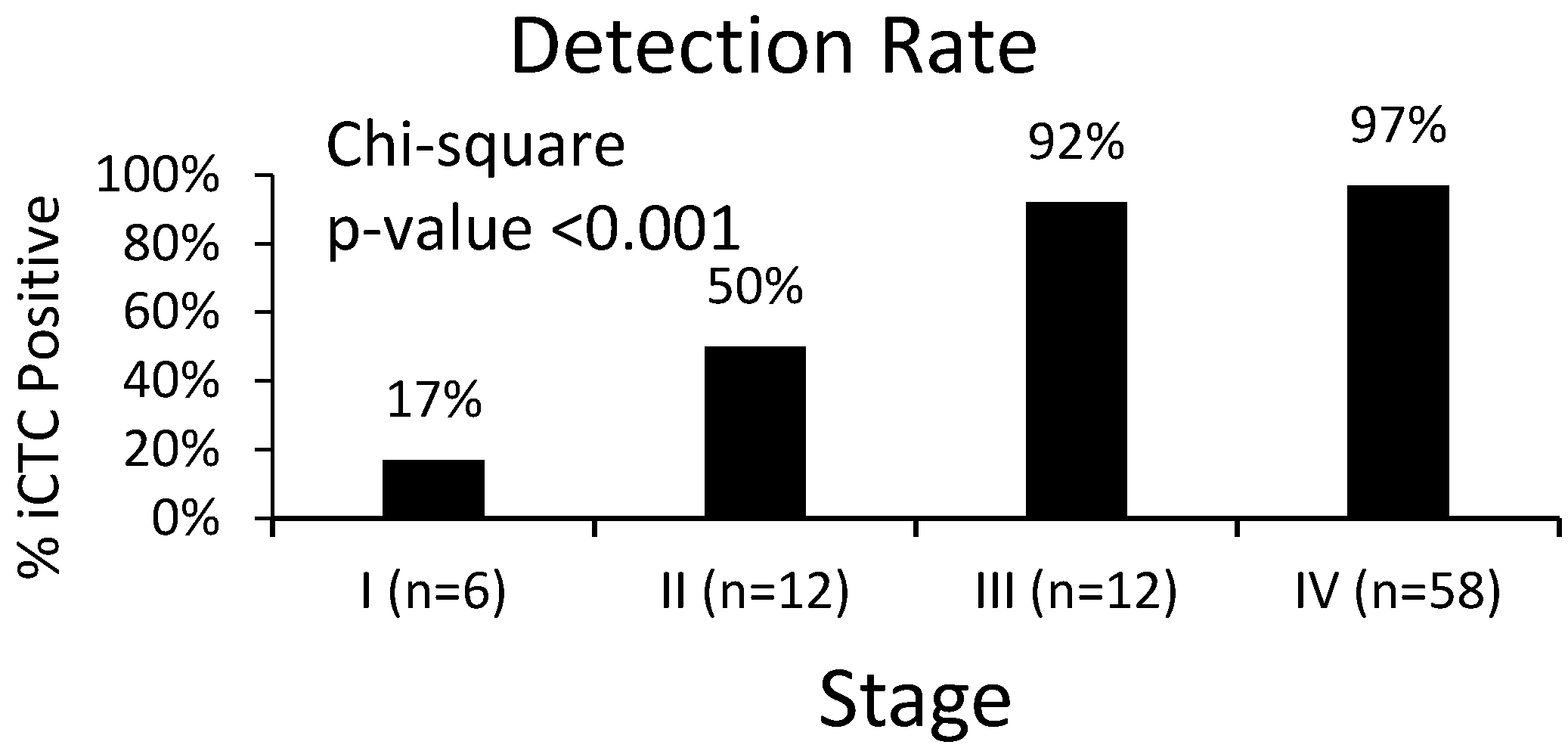
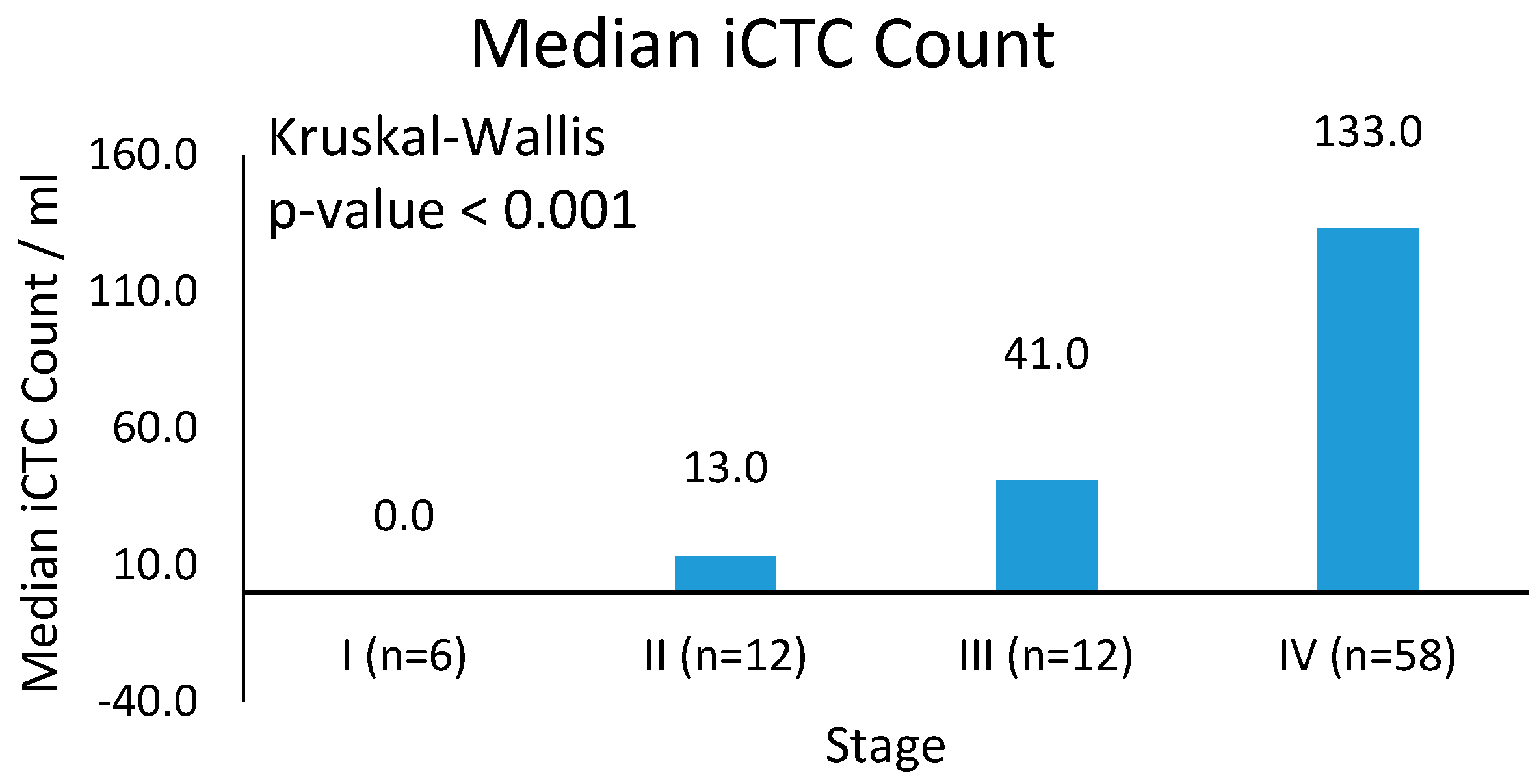
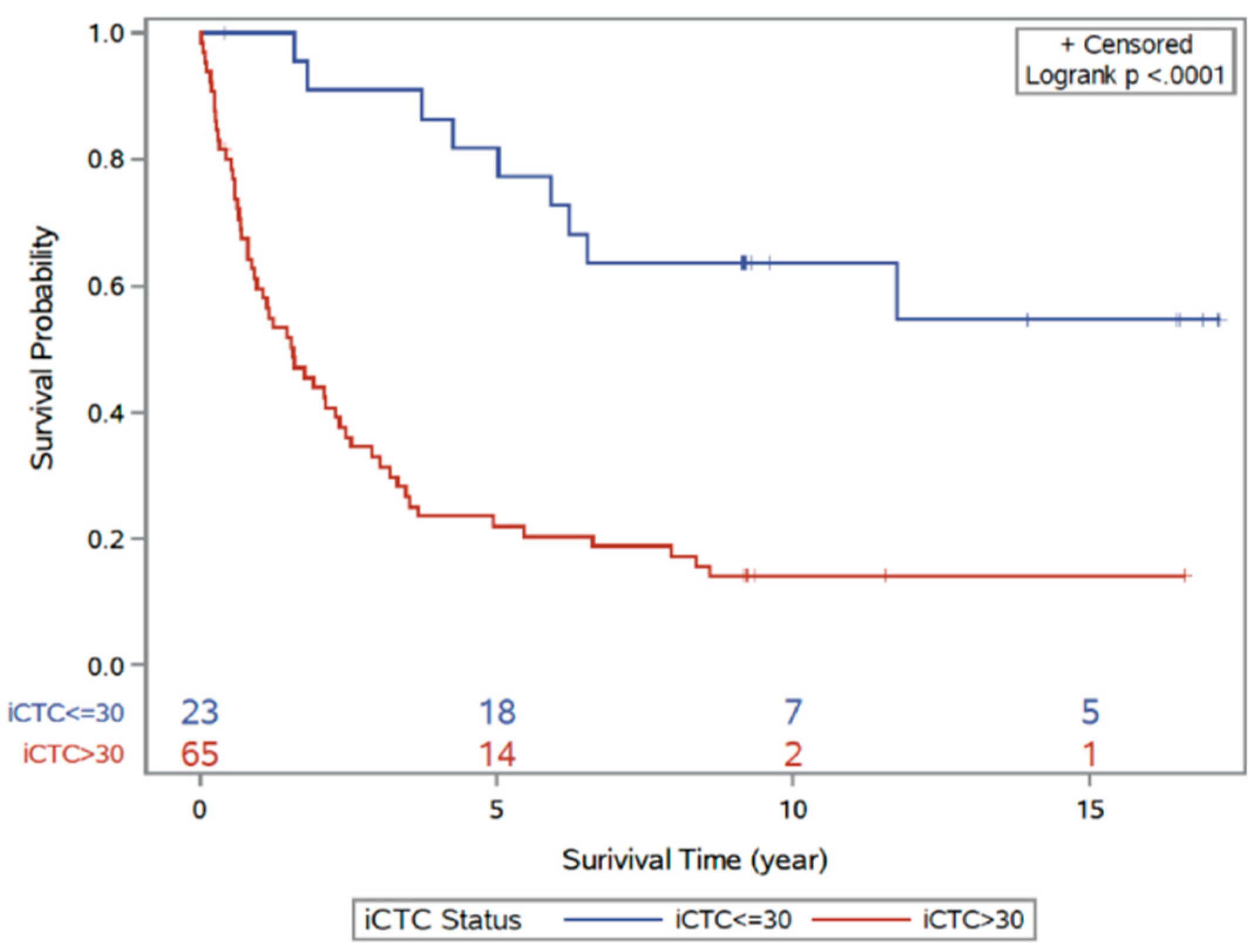
3.2. Clinical Characteristics of iCTCs: Stage and Survival
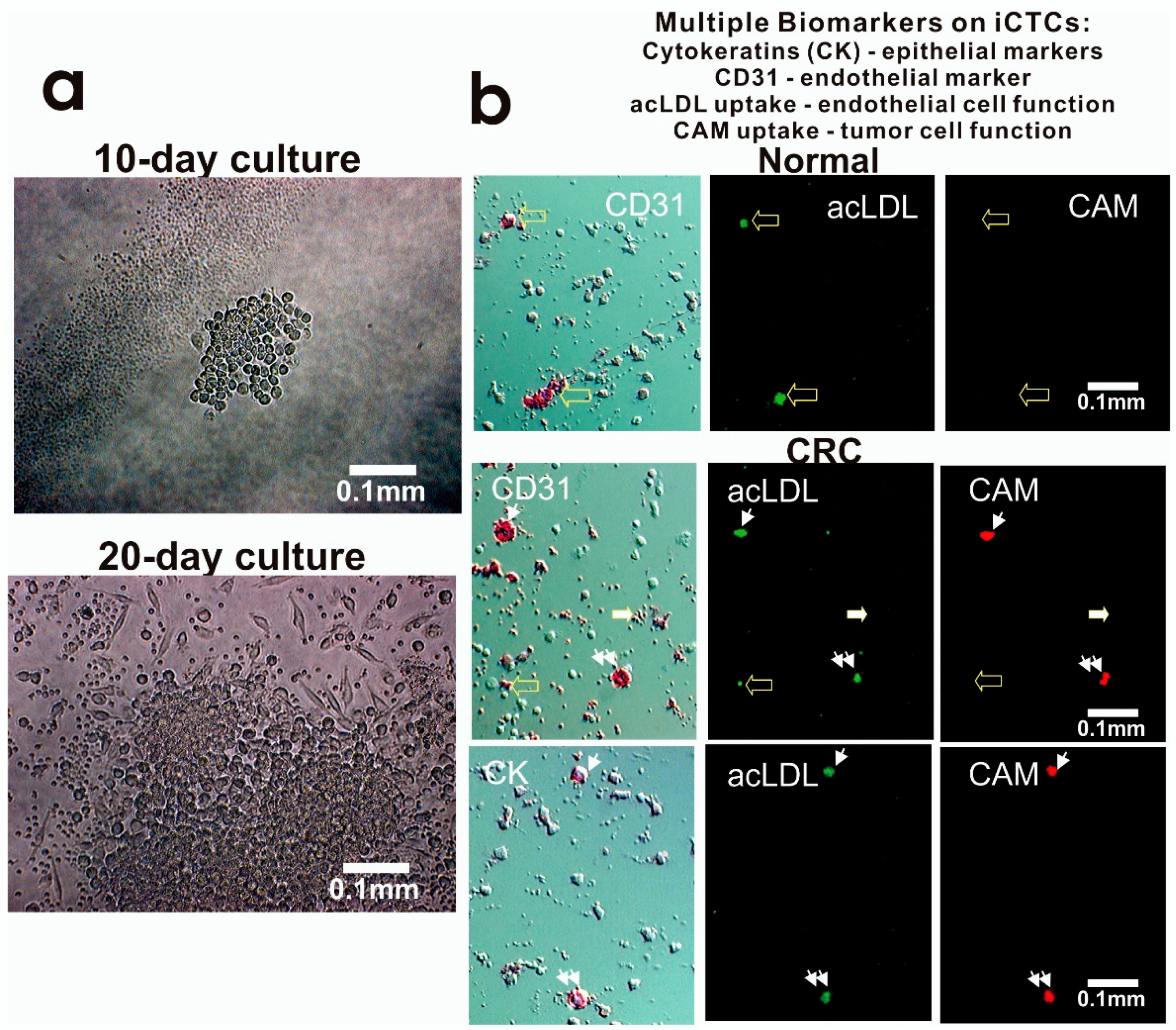
3.3. Molecular and Functional Phenotyping of iCTCs in CRC Patients
4. Discussion
Author Contributions
Acknowledgments
Conflicts of Interest
Abbreviations
| Progression-free survival | PFS |
| Overall survival | OS |
| Colorectal carcinoma | CRC |
| Circulating tumor cells | CTCs |
| Epithelial cell adhesion molecule | EpCAM |
| Collagen adhesion matrix | CAM |
| Epithelial markers | Epi+ |
| Hazard ratio | HR |
| Confidence interval | CI |
| Akaike information criterion | AIC |
| Invasive CTCs | iCTCs |
| Carcinoembryonic antigen | CEA |
References
- American Cancer Society. Cancer Facts & Figures; The Society: Atlanta, GA, USA, 2017. [Google Scholar]
- Brenner, H.; Kloor, M.; Pox, C.P. Colorectal cancer. Lancet 2014, 383, 1490–1502. [Google Scholar] [CrossRef]
- Torino, F.; Bonmassar, E.; Bonmassar, L.; De Vecchis, L.; Barnabei, A.; Zuppi, C.; Capoluongo, E.; Aquino, A. Circulating tumor cells in colorectal cancer patients. Cancer Treat Rev. 2013, 39, 759–772. [Google Scholar] [CrossRef] [PubMed]
- Hayashi, M.; Inoue, Y.; Komeda, K.; Shimizu, T.; Asakuma, M.; Hirokawa, F.; Miyamoto, Y.; Okuda, J.; Takeshita, A.; Shibayama, Y.; et al. Clinicopathological analysis of recurrence patterns and prognostic factors for survival after hepatectomy for colorectal liver metastasis. BMC Surg. 2010, 10, 27. [Google Scholar] [CrossRef] [PubMed]
- Fakih, M.G. Metastatic colorectal cancer: Current state and future directions. J. Clin. Oncol. 2015, 33, 1809–1824. [Google Scholar] [CrossRef] [PubMed]
- Hou, J.M.; Krebs, M.; Ward, T.; Sloane, R.; Priest, L.; Hughes, A.; Clack, G.; Ranson, M.; Blackhall, F.; Dive, C. Circulating tumor cells as a window on metastasis biology in lung cancer. Am. J. Pathol. 2011, 178, 989–996. [Google Scholar] [CrossRef] [PubMed]
- Huang, M.Y.; Tsai, H.L.; Huang, J.J.; Wang, J.Y. Clinical Implications and Future Perspectives of Circulating Tumor Cells and Biomarkers in Clinical Outcomes of Colorectal Cancer. Transl. Oncol. 2016, 9, 340–347. [Google Scholar] [CrossRef] [PubMed]
- Sequist, L.V.; Nagrath, S.; Toner, M.; Haber, D.A.; Lynch, T.J. The CTC-chip: An exciting new tool to detect circulating tumor cells in lung cancer patients. J. Thorac. Oncol. 2009, 4, 281–283. [Google Scholar] [CrossRef] [PubMed]
- Lu, J.; Fan, T.; Zhao, Q.; Zeng, W.; Zaslavsky, E.; Chen, J.J.; Frohman, M.A.; Golightly, M.G.; Madajewicz, S.; Chen, W.T. Isolation of circulating epithelial and tumor progenitor cells with an invasive phenotype from breast cancer patients. Int. J. Cancer 2010, 126, 669–683. [Google Scholar] [CrossRef] [PubMed]
- Pearl, M.L.; Zhao, Q.; Yang, J.; Dong, H.; Tulley, S.; Zhang, Q.; Golightly, M.; Zucker, S.; Chen, W.T. Prognostic analysis of invasive circulating tumor cells (iCTCs) in epithelial ovarian cancer. Gynecol. Oncol. 2014, 134, 581–590. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fan, T.; Zhao, Q.; Chen, J.J.; Chen, W.T.; Pearl, M.L. Clinical significance of circulating tumor cells detected by an invasion assay in peripheral blood of patients with ovarian cancer. Gynecol. Oncol. 2009, 112, 185–191. [Google Scholar] [CrossRef] [Green Version]
- Pearl, M.L.; Dong, H.; Tulley, S.; Zhao, Q.; Golightly, M.; Zucker, S.; Chen, W.T. Treatment monitoring of patients with epithelial ovarian cancer using invasive circulating tumor cells (iCTCs). Gynecol. Oncol. 2015, 137, 229–238. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Paris, P.L.; Kobayashi, Y.; Zhao, Q.; Zeng, W.; Sridharan, S.; Fan, T.; Adler, H.L.; Yera, E.R.; Zarrabi, M.H.; Zucker, S.; et al. Functional phenotyping and genotyping of circulating tumor cells from patients with castration resistant prostate cancer. Cancer Lett. 2009, 277, 164–173. [Google Scholar] [CrossRef] [PubMed]
- Tulley, S.; Zhao, Q.; Dong, H.; Pearl, M.L.; Chen, W.T. Vita-Assay (TM) Method of Enrichment and Identification of Circulating Cancer Cells/Circulating Tumor Cells (CTCs). Methods Mol. Biol. 2016, 1406, 107–119. [Google Scholar] [PubMed]
- Friedlander, T.W.; Ngo, V.T.; Dong, H.; Premasekharan, G.; Weinberg, V.; Doty, S.; Zhao, Q.; Gilbert, E.G.; Ryan, C.J.; Chen, W.T.; et al. Detection and characterization of invasive circulating tumor cells derived from men with metastatic castration-resistant prostate cancer. Int. J. Cancer 2014, 134, 2284–2293. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tsai, W.S.; Chen, J.S.; Shao, H.J.; Wu, J.C.; Lai, J.M.; Lu, S.H.; Hung, T.F.; Chiu, Y.C.; You, J.F.; Hsieh, P.S.; et al. Circulating Tumor Cell Count Correlates with Colorectal Neoplasm Progression and Is a Prognostic Marker for Distant Metastasis in Non-Metastatic Patients. Sci. Rep. 2016, 6, 24517. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alix-Panabieres, C.; Bartkowiak, K.; Pantel, K. Functional studies on circulating and disseminated tumor cells in carcinoma patients. Mol. Oncol. 2016, 10, 443–449. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Asahara, T.; Murohara, T.; Sullivan, A.; Silver, M.; van der Zee, R.; Li, T.; Witzenbichler, B.; Schatteman, G.; Isner, J.M. Isolation of putative progenitor endothelial cells for angiogenesis. Science 1997, 275, 964–967. [Google Scholar] [CrossRef] [PubMed]
- Micalizzi, D.S.; Haber, D.A.; Maheswaran, S. Cancer metastasis through the prism of epithelial to mesenchymal transition in circulating tumor cells. Mol. Oncol. 2017, 11, 770–780. [Google Scholar] [CrossRef] [PubMed]
- Cohen, S.J.; Punt, C.J.; Iannotti, N.; Saidman, B.H.; Sabbath, K.D.; Gabrail, N.Y.; Picus, J.; Morse, M.; Mitchell, E.; Miller, M.C.; et al. Relationship of circulating tumor cells to tumor response, progression-free survival, and overall survival in patients with metastatic colorectal cancer. J. Clin. Oncol. 2008, 26, 3213–3221. [Google Scholar] [CrossRef] [PubMed]
- Tol, J.; Koopman, M.; Miller, M.C.; Tibbe, A.; Cats, A.; Creemers, G.J.; Vos, A.H.; Nagtegaal, I.D.; Terstappen, L.W.; Punt, C.J. Circulating tumour cells early predict progression-free and overall survival in advanced colorectal cancer patients treated with chemotherapy and targeted agents. Ann. Oncol. 2010, 21, 1006–1012. [Google Scholar] [CrossRef] [PubMed]
- Wu, W.; Zhang, Z.; Gao, X.H.; Shen, Z.; Jing, Y.; Lu, H.; Li, H.; Yang, X.; Cui, X.; Li, Y.; et al. Clinical significance of detecting circulating tumor cells in colorectal cancer using subtraction enrichment and immunostaining-fluorescence in situ hybridization (SE-iFISH). Oncotarget 2017, 8, 21639–21649. [Google Scholar] [CrossRef] [PubMed]
- Cabel, L.; Proudhon, C.; Gortais, H.; Loirat, D.; Coussy, F.; Pierga, J.Y.; Bidard, F.C. Circulating tumor cells: Clinical validity and utility. Int. J. Clin. Oncol. 2017. 22, 421–430. [CrossRef]
- León-Mateos, L.; Casas, H.; Abalo, A.; Vieito, M.; Abreu, M.; Anido, U.; Gómez-Tato, A.; López, R.; Abal, M.; Muinelo-Romay, L. Improving circulating tumor cells enumeration and characterization to predict outcome in first line chemotherapy mCRPC patients. Oncotarget 2017, 8, 54708–54721. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.Y.; Yeh, C.S.; Tzou, W.S.; Hsieh, J.S.; Chen, F.M.; Lu, C.Y.; Yu, F.J.; Cheng, T.L.; Huang, T.J.; Lin, S.R. Analysis of progressively overexpressed genes in tumorigenesis of colorectal cancers using cDNA microarray. Oncol. Rep. 2005, 14, 65–72. [Google Scholar] [PubMed]
- Wang, J.Y.; Lin, S.R.; Wu, D.C.; Lu, C.Y.; Yu, F.J.; Hsieh, J.S.; Cheng, T.L.; Koay, L.B.; Uen, Y.H. Multiple molecular markers as predictors of colorectal cancer in patients with normal perioperative serum carcinoembryonic antigen levels. Clin. Cancer Res. 2007, 13, 2406–2413. [Google Scholar] [CrossRef] [PubMed]
- Paterlini-Brechot, P.; Benali, N.L. Circulating tumor cells (CTC) detection: Clinical impact and future directions. Cancer Lett. 2007, 253, 180–204. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Total (n = 88 *) | ||
|---|---|---|
| Male | 63 (72%) | |
| Race | Caucasian | 70 (80%) |
| African American | 5 (6%) | |
| Asian | 2 (2%) | |
| Hispanic | 3 (3%) | |
| Unknown | 8 (9%) | |
| Stage | 1 | 6 (7%) |
| 2 | 12 (14%) | |
| 3 | 12 (14%) | |
| 4 | 58 (65%) | |
| Chemotherapy | 71 (81%) | |
| Surgery | 74 (84%) | |
| Radiation | 30 (34%) |
| Stage | CTC < 5 | CTC ≥ 5 | CTC ≥ 5% |
|---|---|---|---|
| I (n = 6) | 5 | 1 | 17% |
| II (n = 12) | 6 | 6 | 50% |
| III (n = 12) | 1 | 11 | 92% |
| IV (n = 58) | 2 | 56 | 97% |
| Stage | iCTC Median | iCTC Mean | iCTC Standard Error |
|---|---|---|---|
| I (n = 6) | 0.0 | 8.3 | 8.3 |
| II (n = 12) | 13.0 | 35.8 | 13.5 |
| III (n = 12) | 41.0 | 65.9 | 23.1 |
| IV (n = 58) | 133.0 | 144.8 | 13.8 |
| Factor | Univariable Model | Multivariable Model | ||
|---|---|---|---|---|
| Hazard Ratio (95% CI) | p Value | Hazard Ratio (95% CI) | p Value | |
| iCTCs | 1.05 (1.03–1.07) | <0.0001 | 1.04 (1.01–1.06) | 0.009 |
| Stage | 1.89 (1.37–2.61) | 0.0001 | 1.66 (1.12–2.47) | 0.01 |
| Surgery | 0.17 (0.08–0.36) | <0.0001 | 0.37 (0.15–0.92) | 0.03 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zhang, Y.; Zarrabi, K.; Hou, W.; Madajewicz, S.; Choi, M.; Zucker, S.; Chen, W.-T. Assessing Clinical Outcomes in Colorectal Cancer with Assays for Invasive Circulating Tumor Cells. Biomedicines 2018, 6, 69. https://doi.org/10.3390/biomedicines6020069
Zhang Y, Zarrabi K, Hou W, Madajewicz S, Choi M, Zucker S, Chen W-T. Assessing Clinical Outcomes in Colorectal Cancer with Assays for Invasive Circulating Tumor Cells. Biomedicines. 2018; 6(2):69. https://doi.org/10.3390/biomedicines6020069
Chicago/Turabian StyleZhang, Yue, Kevin Zarrabi, Wei Hou, Stefan Madajewicz, Minsig Choi, Stanley Zucker, and Wen-Tien Chen. 2018. "Assessing Clinical Outcomes in Colorectal Cancer with Assays for Invasive Circulating Tumor Cells" Biomedicines 6, no. 2: 69. https://doi.org/10.3390/biomedicines6020069