1. Introduction
In cataract surgery, the lens of the eye is replaced by artificial intra ocular lens (IOL) while the implanted lens is usually a mono focal lens with a fixed focal length, which does not allow focusing on objects at different distances. This effect is equivalent to what happens in the case of presbyopia. Various solutions to this problem are based on fabricating diffractive IOLs [
1,
2,
3] (e.g., IOLs as Restor of Alcon and Acrilisa of Zeiss) which suffer from high chromatic aberrations (these lenses lose some of their multi focal capability and function as almost mono focal lenses when non-green illumination is used [
4]) as well as loss of resolution (due to defocusing) in the intermediate ranges. Note that the intermediate ranges are very important for working in front of a computer, watching a television,
etc. In the market, there are also various types of refractive solutions [
2,
5] such as the ReZoom of AMO. However, these lenses also, in the case of diffraction solution, produce a discrete number of focal lengths, and thus, they provide no solution for focusing on intermediate ranges.
There is another type of available solution which is called accommodative lenses [
6]. In these lenses, the subject can achieve some accommodation after the implantation. There are two types of technological solutions for this category. In the first, a mono focal lens is positioned on an axial pivot such that when this lens is pressed with the muscles of the eye it is axially shifted [
7,
8]. As an example, one may have the Crystalens of Bausch and Lomb. Based on the same technology another lens was created. A doublet composed of two mono focal lenses that, when pressed by the muscles of the eye, adjust their distance from each other, and thus, also their overall focal length [
9]. The second technology includes construction of a lens built out of flexible material that when pressed by the muscles of the eye its curvature is changed, and thus, also its focal length [
10]. The problem with these lenses is that they are not able to provide sufficiently large accommodation ability and this ability even decreases with time. The subjects also have long adaptation time. In addition, these lenses function differently for every subject since each subject applies a different force on the lens.
The solution presented in this paper produces continuously focused vision over the full required range that in regular eye is covered by accommodation of 3.00 Diopters (from near range of 33 cm and up to infinity) [
11,
12,
13]. All this is obtained with static element with high energetic efficiency and without any need of applying force by the muscles of the eye. The solution is based upon addition of special annular like engraved profile on the surface of the lens. The engraving has depth of less than 1 micron. This profile generates extended depth of focus (EDOF) by fulfilling proper interference conditions within a focus channel starting before and ending after the original focal plane of the lens. Therefore, we coin this type of EDOF solution as an interference-based EDOF approach. The engraved profile does not contain any high spatial frequencies and therefore it is relatively easy and cheap for fabrication and its diffraction effects and chromatic dispersion are small. Nonetheless, the energetic efficiency is high, as no energy is diverted into diffraction orders away from the central order of interest as in the case of diffractive optical elements. Due to the continuous focal extension, the proposed solution can ensure IOL are effective for near, intermediate as well as distance working ranges.
2. Method and Materials
In this paper, we present clinical results of an IOL designed lens denoted in the figures as design #426. This design has continuous addition ranging from 1.5 D–2.25 D (D denotes diopters). This EDOF design is fabricated by Xceed Imaging.
An example image presenting how interference based EDOF IOL look like can be seen in
Figure 1. It includes circular scratches having etching depth of less than one micron. The diameter of the external circle is about 3 mm.
Figure 1.
Image of an interference based EDOF design. The diameter of the external circle is about 3 mm.
Figure 1.
Image of an interference based EDOF design. The diameter of the external circle is about 3 mm.
The clinical trials have been performed using phase plates (PP) technique. This method includes conversion of the IOL design to a spectacle plate design—which can be located exterior to the eye, yet produces parallel response to an interiorly placed lens. Optical bench testing has previously proven that IOL testing and PP testing both produce parallel responses. This allows clinical examination of the multifocal design prior to surgery, allowing patients to experience the high visual acuity (VA) and visual quality of the proposed element prior to its implantation and to provide feedback before the implantation of the lens.
In addition to the interference based EDOF design of Xceed #426, a PP analogue of the Restor 3 lens, based on the public patent of Alcon, has been produced. This PP was clinically tested along with Xceed #426 lens. All subjects were tested monocularly.
The clinical VA tests were done in an ophthalmology properly equipped lab and included patients wearing spectacles frames into which the relevant PP (either of lens #426 or of the Restor lens) were placed after correcting the vision of all subjects to far range (by placing proper mono focal lenses into the spectacles frame). The subjects attempted to read the smallest possible letters appearing in ETDRS charts. The patients were asked to look at the ETDRS charts suitable for a 3 m distance (0.33 Diopter) and for a 40 cm distance (2.5 Diopter). Those ETDRS charts were placed at distances of 3 m (0.33 Diopter), 65 cm (1.539 Diopter), 40 cm (2.5 Diopter) and 25 cm (4 Diopter). For distances of 65 cm and 25 cm, appropriate conversions of the VA were performed (as the ETDRS charts that were used for this were for 40 cm).
In the clinical trials, we had between 17−20 participants at an average age of 66 years old with a standard deviation of 5 years. Most of the patients (about 60%) were men and the remainder were women. All patients were emmetropes (after completing for them the best distance correction as we did in our clinical trial procedure).
3. Results Explanation
As previously stated, for the VA testing, the ETDRS charts were placed at distances of 3 m, 65 cm, 40 cm and 25 cm (with the appropriate conversions of VA at the 65 cm and 25 cm distances). Each of these distances were tested three times; firstly, with the subjects best distance correction (which was used as the reference), secondly with the best distance correction and the Xceed #426 PP placed in the trial frame, and thirdly with the Restor 3 PP placed in the trial frame instead of the Xceed #426 PP (the best distance correction lens was left in). The last two were performed in a randomized manner.
The results display the actual VA which was recorded at the clinical examination (the lower the numerical value, the better the result is) in LogMar units.
The X- axis in all figures represents the testing distance, and the Y axis represents the obtained VA. Each VA (Y-axis) result is composed of four numbers/bars, corresponding to the test distance: the blue column represents the distance VA, the red column represents the VA at 65 cm, the green column represents the VA at 40 cm and the purple column represents the VA at 25 cm. Each difference of 0.1 in the Y axis represents one line in the ETDRS chart.
Additionally, individual subject results are also graphed. This helps to highlight the fact that the IOL design of Xceed allows not only superior performance to its competitors when looking at the average results, but rather shows better performance for each tested individual subject.
To be more specific, during the clinical trial we used ETDRS charts for 3 m and 40 cm. In each test, the VA for four distances has been measured: for 3 m, 65 cm, 40 cm and 25 cm (appearing as four bars for each patient). The ETDRS chart has five letters in each line. Each line represents 0.1 in LogMar units while the 6/6 line (20/20) is the 0 (zero) line, the line above is 0.1 (bigger letters) and the line below is −0.1 (smaller letters). Each letter represents a 0.02 change in the LogMar units.
4. Clinical Results
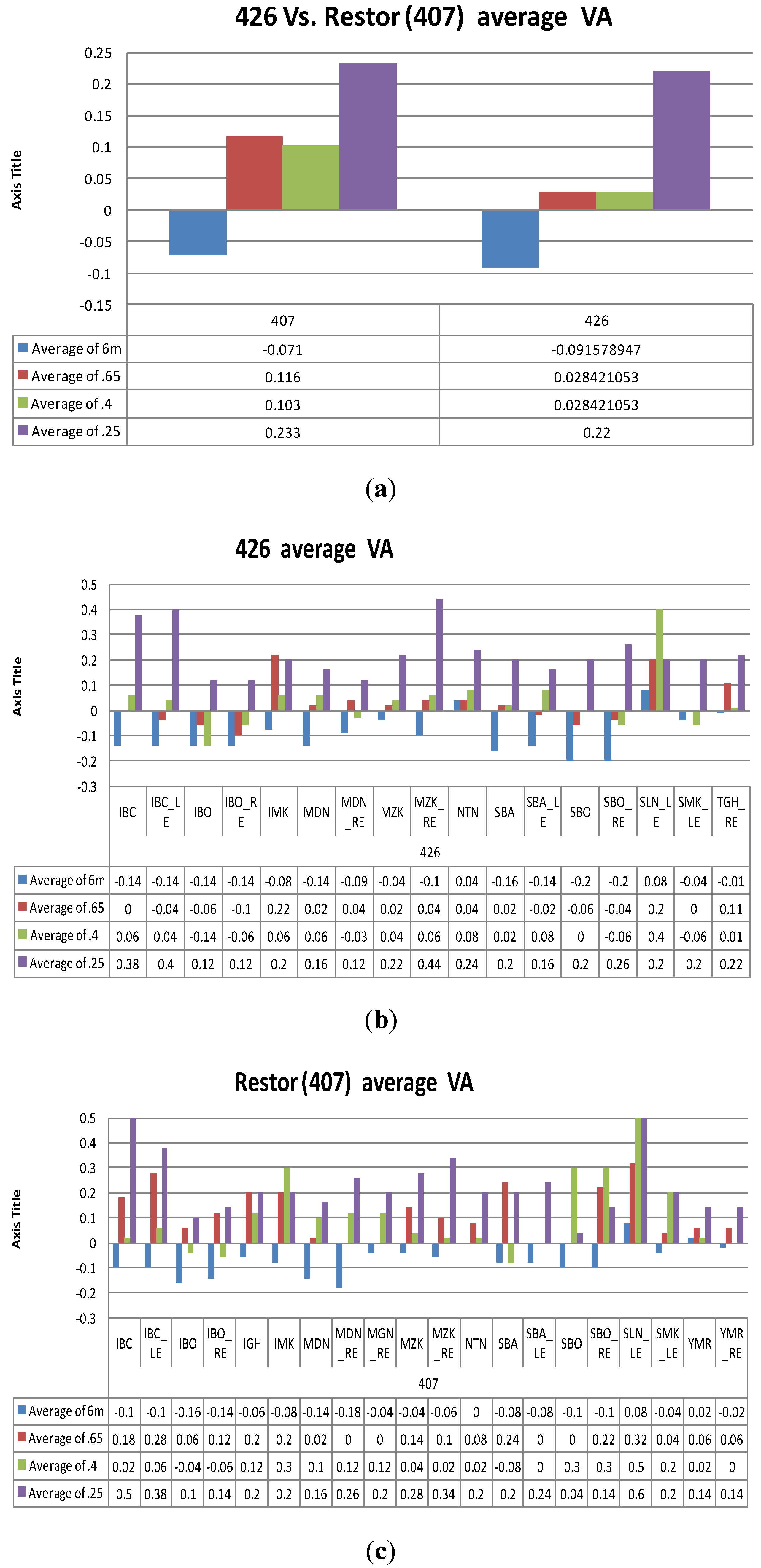
The average VA results are shown in
Figure 2a in which in the left side one may see the performance of the Restor IOL design and in the right side the performance of Xceed #426 design. One may clearly see that the performance of Xceed IOL is indeed better for intermediate distances.
Figure 2.
(a). Average visual acuity (VA) for design #426 (Number of patients was N = 17) and Restor (PP number 407) (Number of patients was N = 20). Lower value represents a better result. (b). and (c). Individual VA results. The X axis contains the initials of all the subjects tested with this design. (b). Results for Xceed design #426. Number of patients was N = 17. (c). Results for Restor (PP design #407). Number of patients is N = 20.
Figure 2.
(a). Average visual acuity (VA) for design #426 (Number of patients was N = 17) and Restor (PP number 407) (Number of patients was N = 20). Lower value represents a better result. (b). and (c). Individual VA results. The X axis contains the initials of all the subjects tested with this design. (b). Results for Xceed design #426. Number of patients was N = 17. (c). Results for Restor (PP design #407). Number of patients is N = 20.
In
Figure 2b and 2c we show the individual results obtained for Xceed design (in
Figure 2b) and for Restor design (
Figure 2c) while by individual we mean the results obtained per each one of the patients participating in the clinical trials. One may see that the improvement in the average chart of
Figure 2a is basically obtained per each one of the patients individually as well.
5. Discussion
The clinical results of Xceed IOL #426 were better for all distances in respect to the Restor design, especially at the 65 cm tested distance, where the IOL #426 excelled the Restor 3 PP by about one line on average. The loss of vision in the case of Xceed element at distances of 65 cm and 40 cm was only 0.028 which is about one letter only in the ETDRS chart.
The results that we have presented in
Figure 2 include the absolute measurement performed on the patients taking part in our clinical trials (after being corrected to distance vision,
i.e., becoming emmotropes) and adding in the effect of either Xceed’s EDOF IOL design or the Restor IOL design (both realized on a PP). However, in order to better quantify our results, we also compared the obtained improvement of both PP elements in each one of our patients in respect to their VA when the tested PP element is taken out,
i.e., how many lines of absolute improvement the addition of either one of the PPs (the one of Xceed or the one of Restor) gives to the tested patient. In this experiment, we have ascertained that, in the case of the IOL of Restor when the PP was taken out, the patient’s loss in their VA was 0.108 in LogMar units (more than one line) at a distance of 65 cm, and 0.287 at a distance of 40 cm (lost two lines and more than four letters). In the case of the IOL design of Xceed, when the PP was taken out, then at a distance of 65 cm the patients lost 0.2285 (two lines and more than one letter), and at a distance of 40 cm they lost on average 0.402 (about four lines). Therefore, the average loss in respect to VA in the case when the patients were using Xceed’s IOL design, and it was taken out from the spectacles frames, was significantly larger than the loss in the case of Restor design (when it was taken out from the spectacles frames): Xceed’s IOL design gave on average better results by one line and one letter at a distance of 65 cm and by one line and three letters at a distance of 40 cm.
Conclusions
The clinical results of Xceed’s IOL design #426 showed significant improvement of VA in all tested near and intermediate distances without decreasing the distance VA. The clinical results of IOL design #426 were better for all distances in respect to Restor design, especially at a distance of 65 cm, where IOL #426 excelled in comparison to the Restor 3 PP, improving VA by about one line on average.

 ,
, 
{kind=link}
{kind=link}