
Quantitative Analysis of Velopharyngeal Movement by Applying Principal Component Analysis to Range Images Produced by a Three-Dimensional Endoscope

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Methods
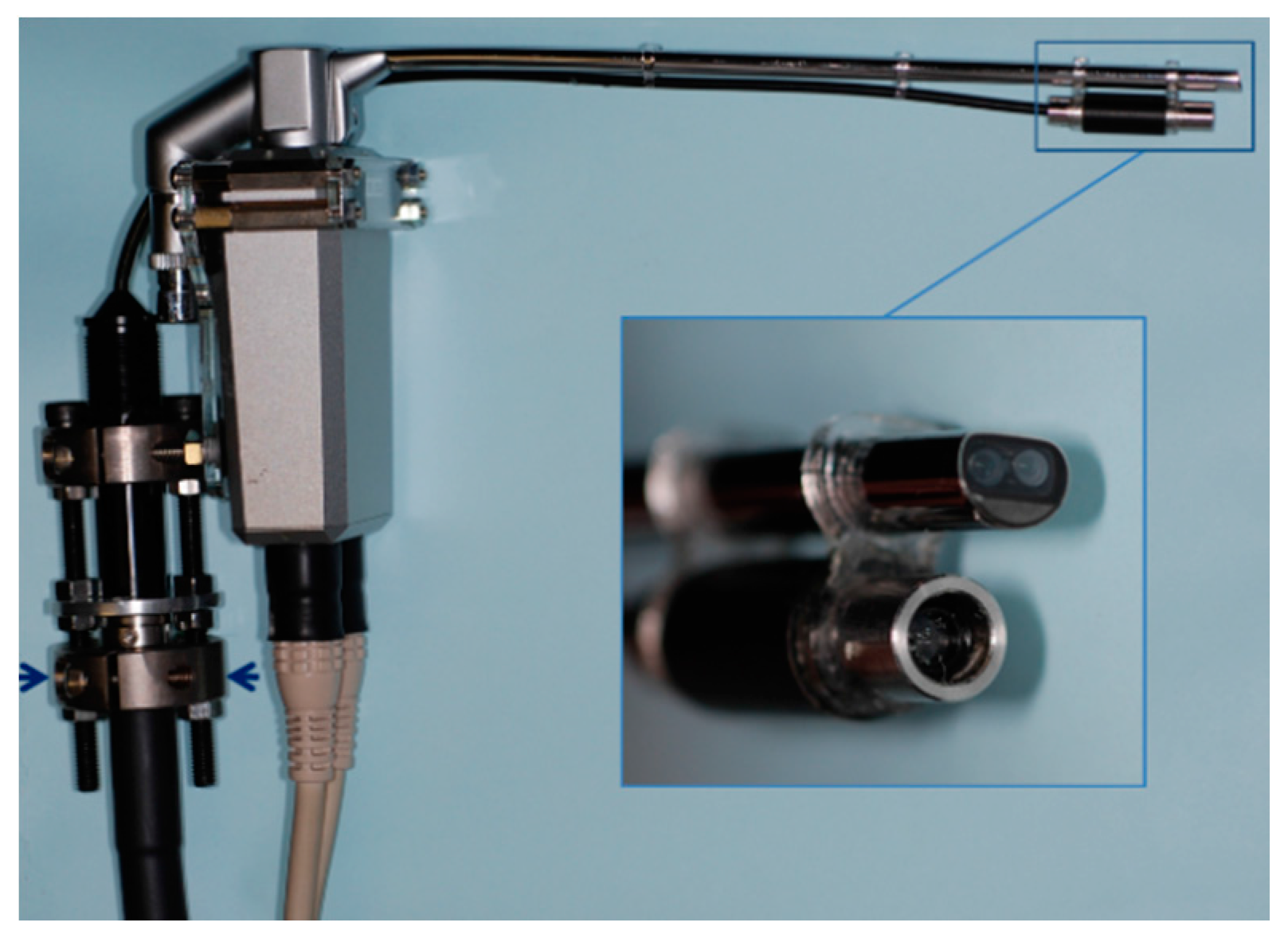
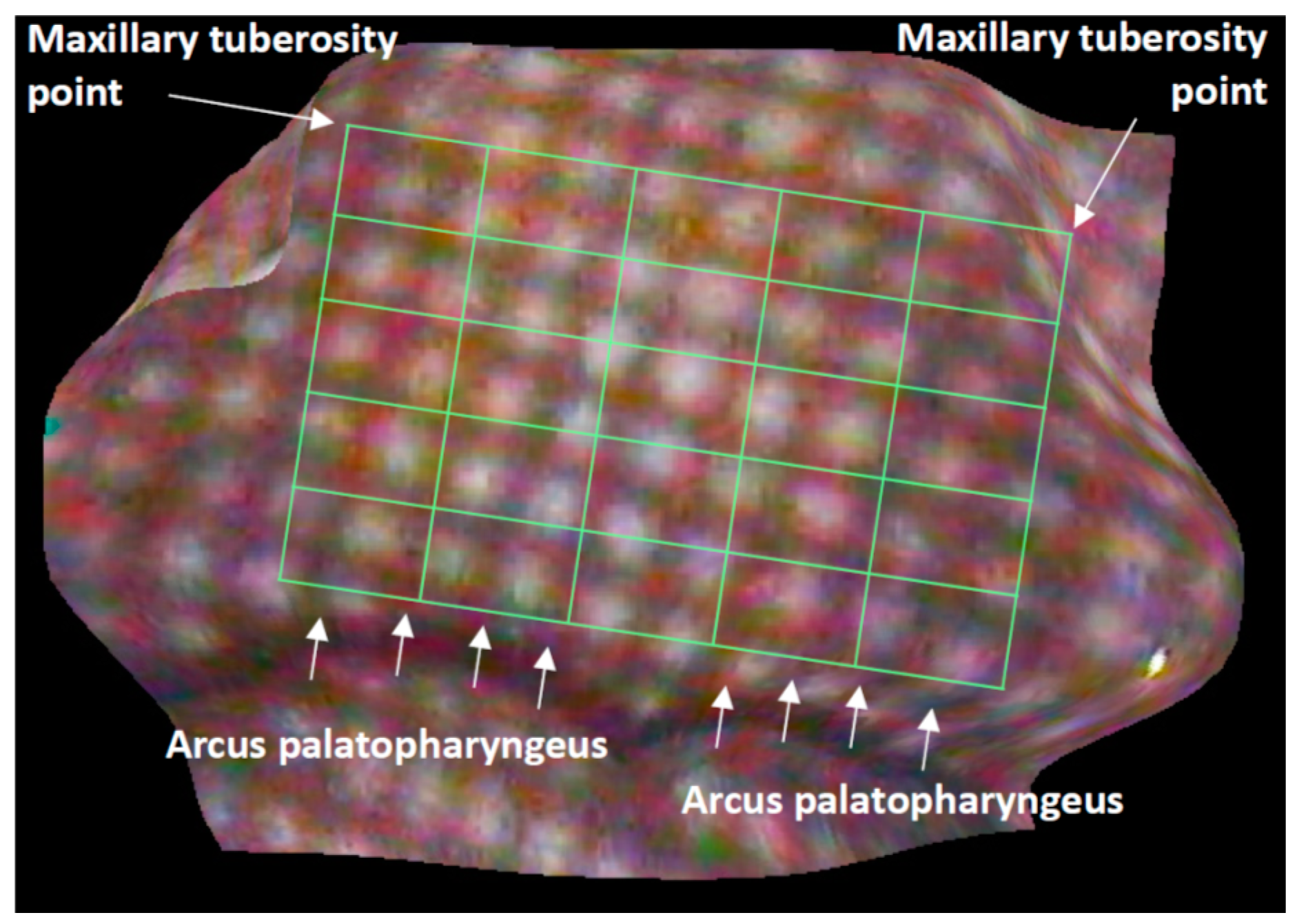
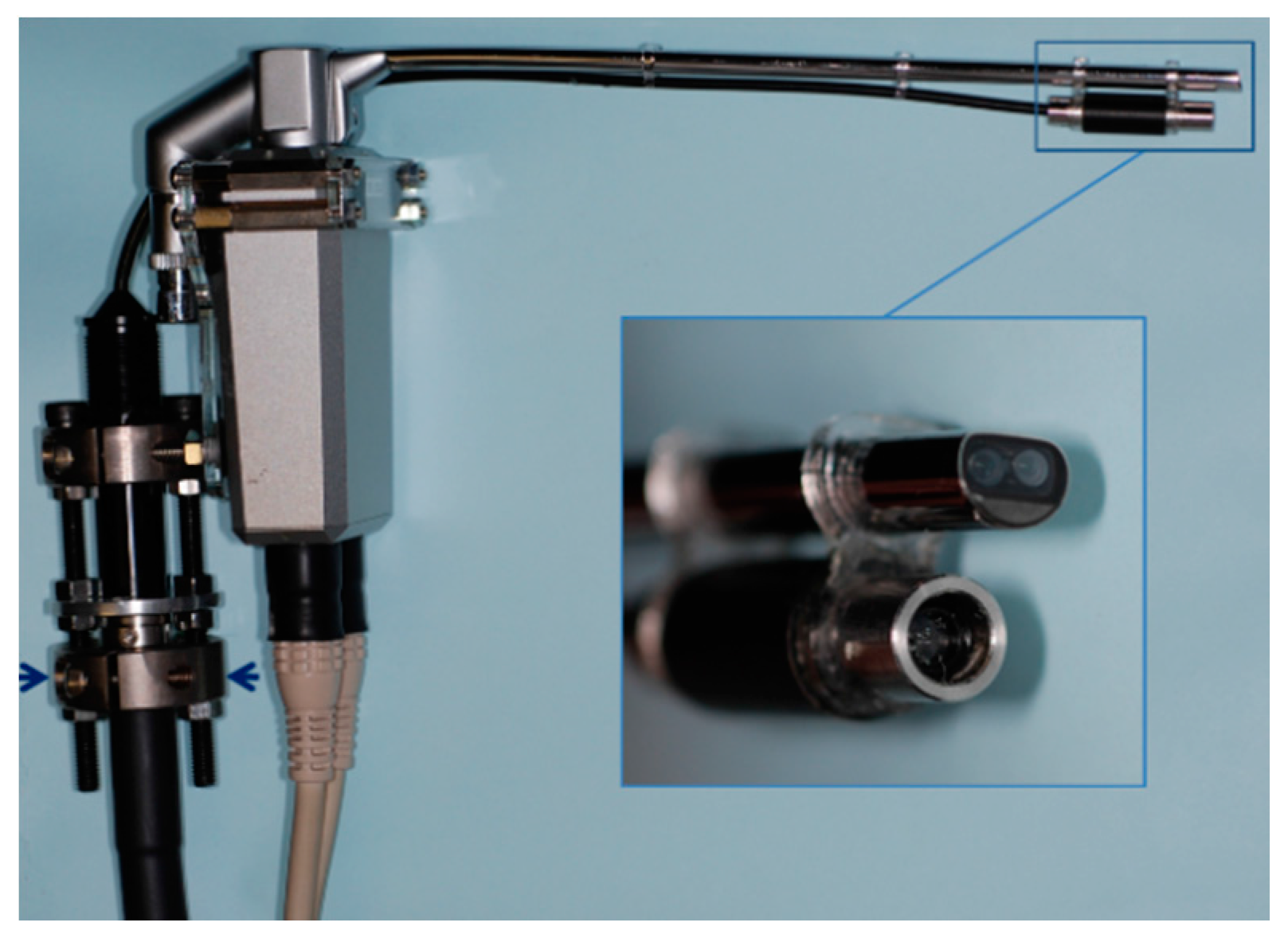
2.1. Production of Range Images
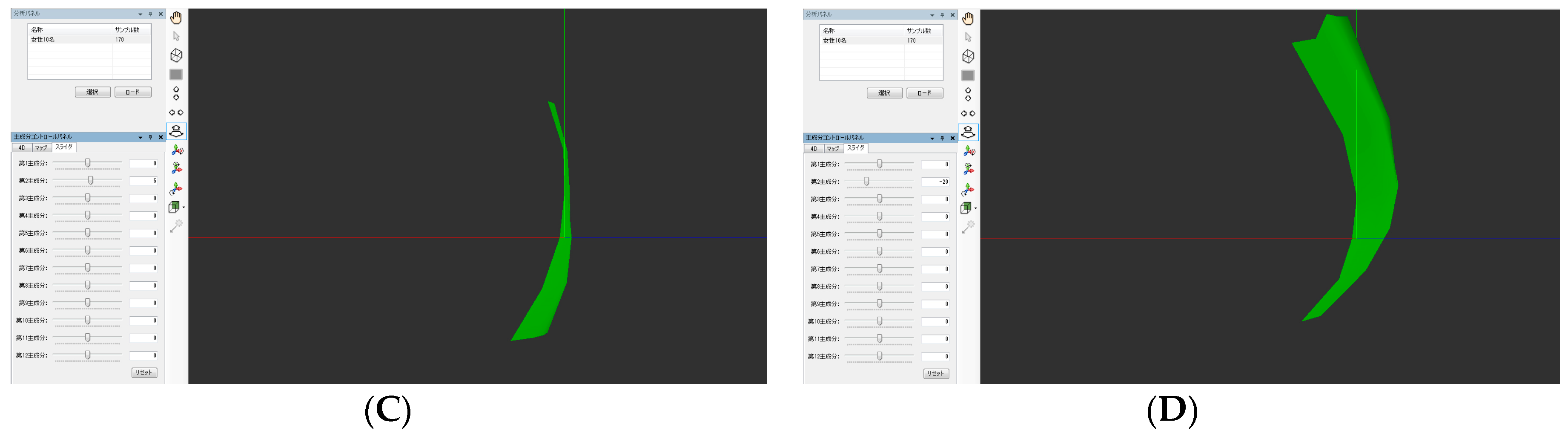
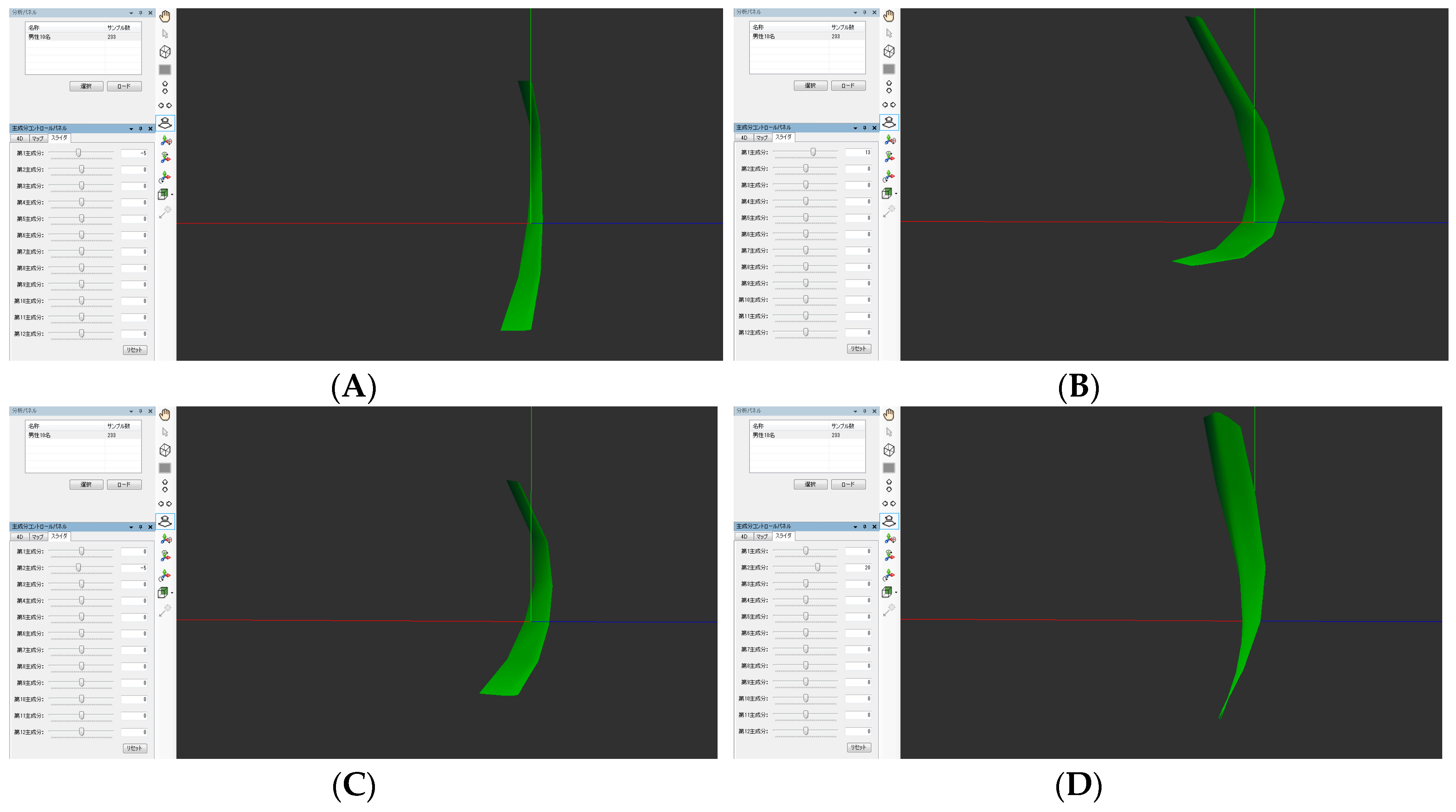
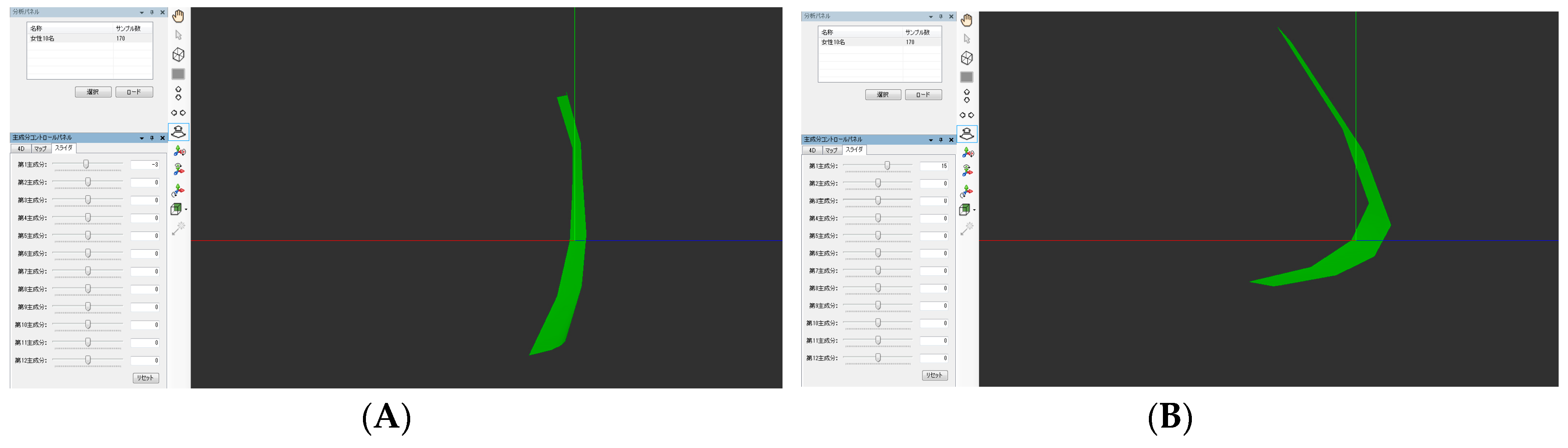
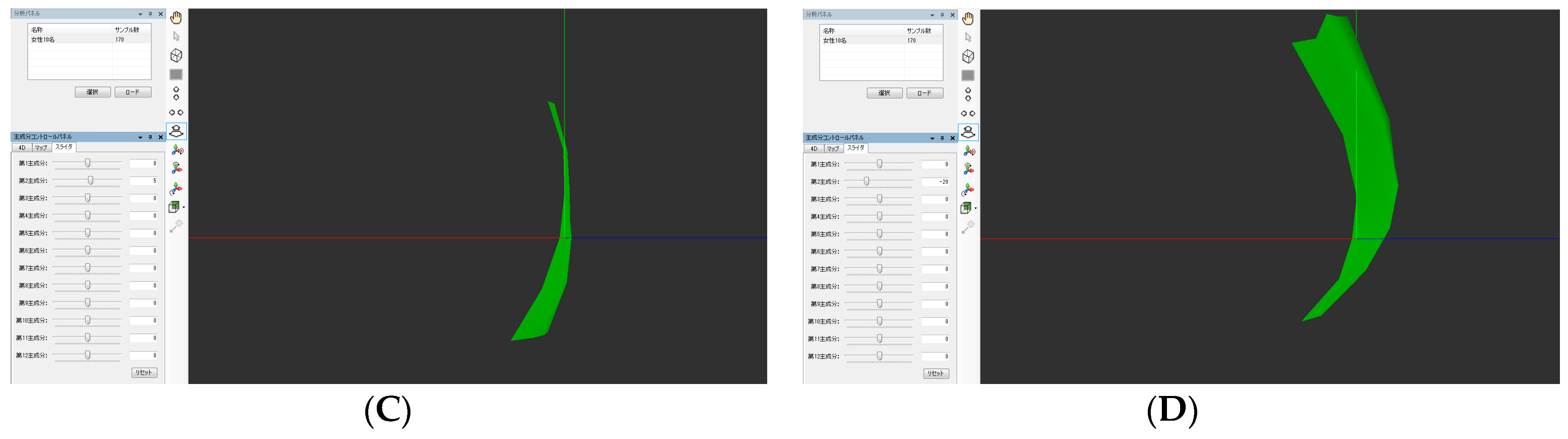
2.2. Analyses of Velopharyngeal Motion
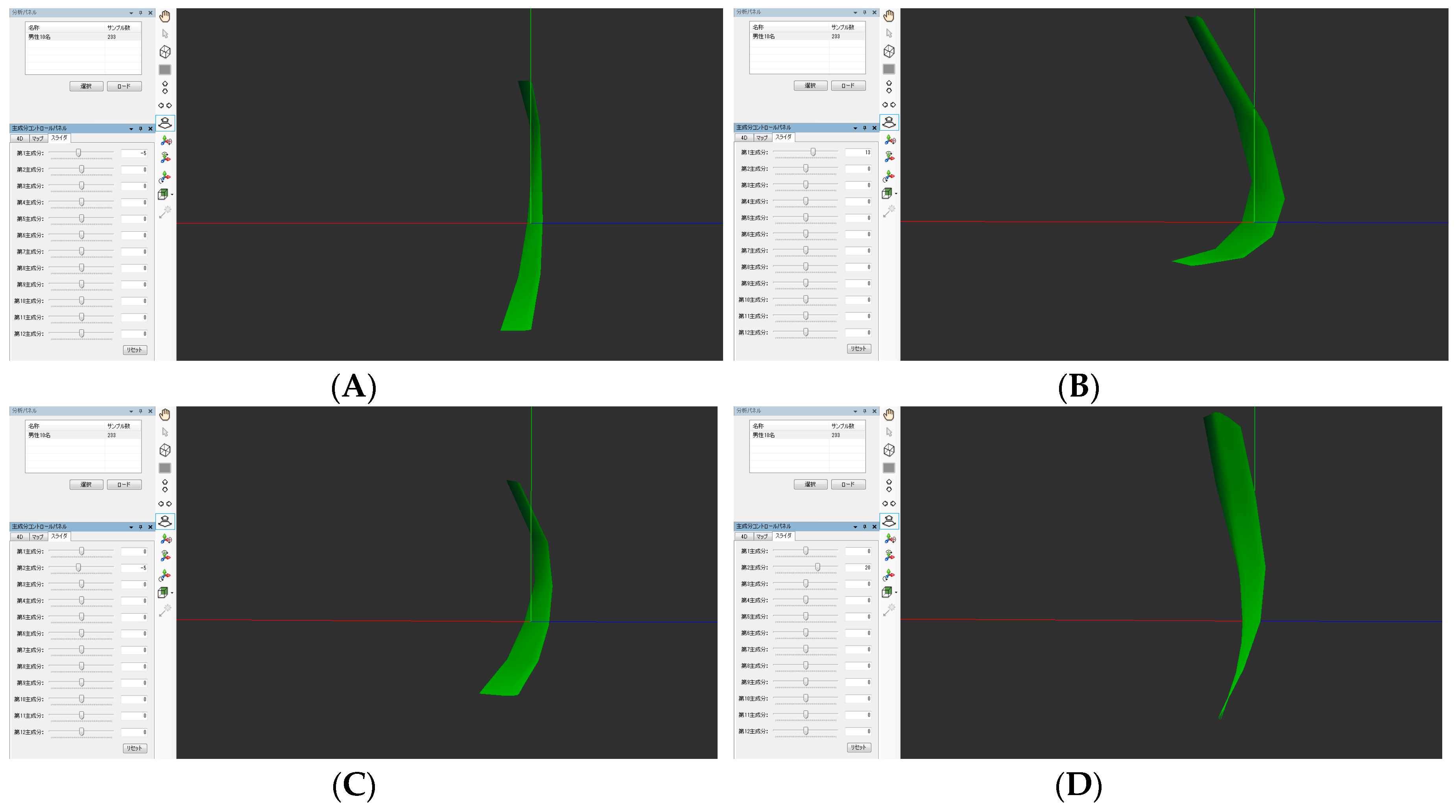
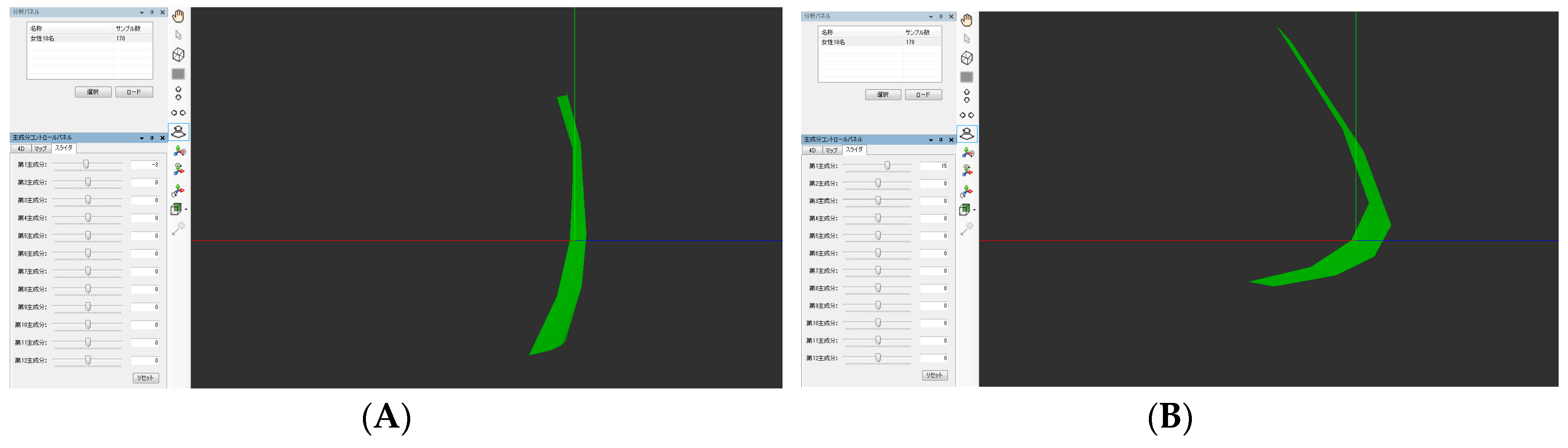
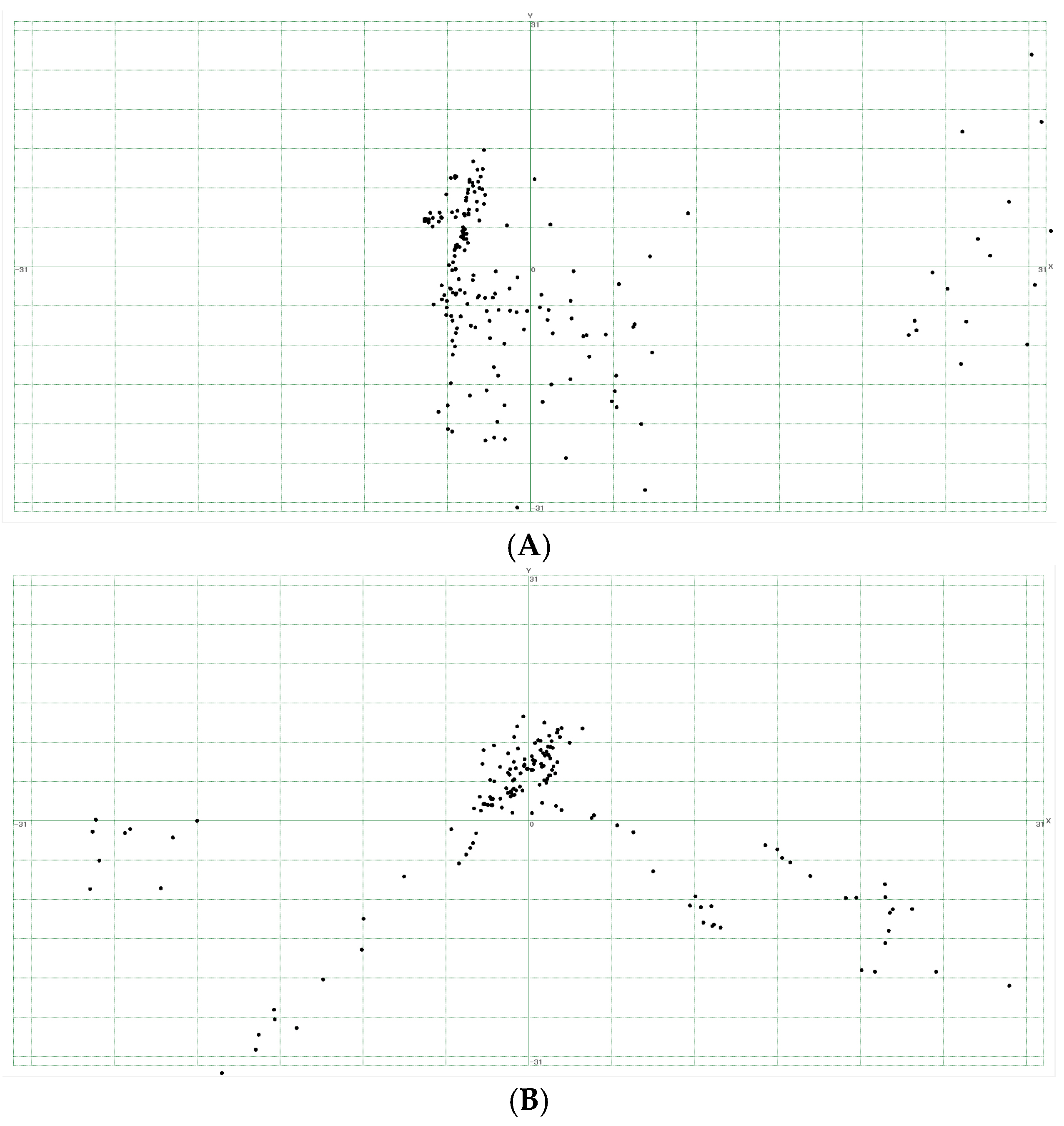
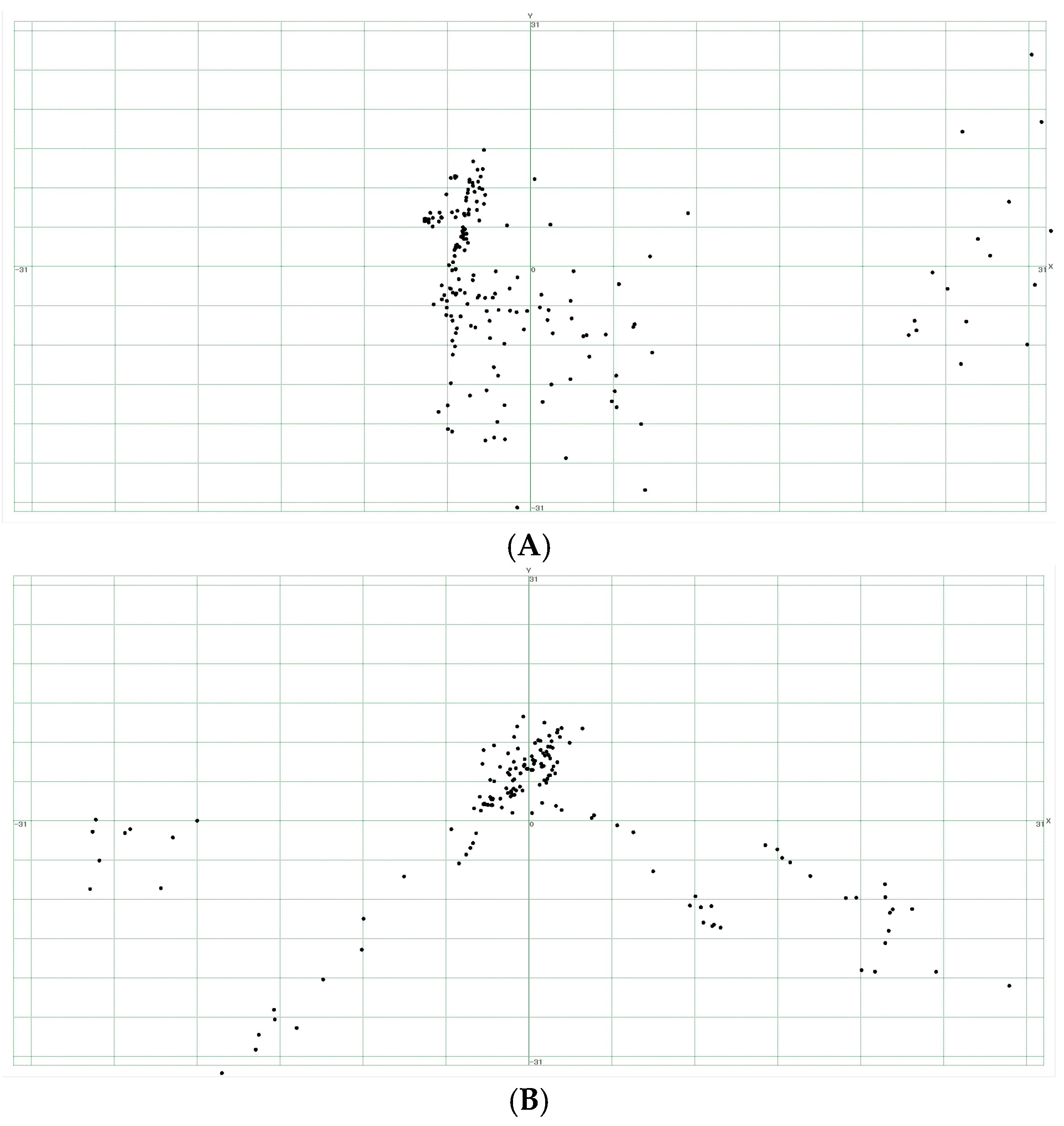
2.3. Principal Component Analyses
3. Results
4. Discussion
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Phua, Y.S.; de Chalain, T. Incidence of oronasal fistulae and velopharyngeal insufficiency after cleft palate repair: An audit of 211 children born between 1990 and 2004. Cleft Palate Craniofac. J. 2008, 45, 172–178. [Google Scholar] [CrossRef] [PubMed]
- Inman, D.S.; Thomas, P.; Hodgkinson, P.D.; Reid, C.A. Oro-nasal fistula development and velopharyngeal insufficiency following primary cleft palate surgery—An audit of 148 children born between 1985 and 1997. Br. J. Plast. Surg. 2005, 58, 1051–1054. [Google Scholar] [CrossRef] [PubMed]
- Hoopes, J.E.; Dellon, A.L.; Fabrikant, J.L.; Soliman, A.H. Cineradiographic assessment of combined island flap pushback and pharyngeal flap in the surgical management of submucous cleft palate. Br. J. Plast. Surg. 1970, 23, 39–44. [Google Scholar] [CrossRef]
- Pegoraro-Krook, M.I.; Dutka-Souz, J.C.; Marino, V.C. Nasoendoscopy of velopharynx before and during diagnostic therapy. J. Appl. Oral Sci. 2008, 16, 181–188. [Google Scholar] [CrossRef] [PubMed]
- Pannbacker, M.D.; Lass, N.J.; Hansen, G.G.; Mussa, A.M.; Robison, K.L. Survey of speech-language pathologists’ training, experience, and opinions on nasopharyngoscopy. Cleft Palate Craniofac. J. 1993, 30, 40–45. [Google Scholar] [CrossRef]
- Mishima, K.; Nakano, A.; Shiraishi, R.; Ueyama, Y. Range image of the velopharynx produced using a 3D endoscope with pattern projection. Laryngoscope 2013, 123, 122–126. [Google Scholar] [CrossRef] [PubMed]
- Nakano, A.; Mishima, K.; Shiraishi, R.; Ueyama, Y. Quantitative analysis of velopharyngeal movement using a stereoendoscope: Accuracy and reliability of range images. Comput. Aided Surg. 2015, 20, 29–33. [Google Scholar] [CrossRef] [PubMed]
- Trotman, C.-A.; Faraway, J.J. Modeling facial movement. I. A dynamic analysis of differences based on skeletal characteristics. J. Oral Maxillofac. Surg. 2004, 62, 1372–1379. [Google Scholar] [CrossRef] [PubMed]
- Popat, H.; Henley, E.; Richmond, S.; Benedikt, L.; Marshall, D.; Rosim, P.L. A comparison of the reproducibility of verbal and nonverbal facial gestures using three-dimensional motion analysis. Otolaryngol. Head Neck Surg. 2010, 142, 867–872. [Google Scholar] [CrossRef] [PubMed]
- Mishima, K.; Yamada, T.; Matsumura, T.; Moritani, N. Analysis of lip motion using principal component analyses. J. Craniomaxillofac. Surg. 2011, 39, 232–236. [Google Scholar] [CrossRef] [PubMed]
- Tsai, R.Y. A versatile camera calibration technique for high-accuracy 3D machine vision metrology using off-the-shelf TV camera and lenses. IEEE J. Robot. Autom. 1987, 3, 323–344. [Google Scholar] [CrossRef]
- Birchfield, S.; Tomasi, C. Depth discontinuities by pixel-to-pixel stereo. Int. J. Comput. Vis. 1999, 35, 269–293. [Google Scholar] [CrossRef]
- Mishima, K.; Yamada, T.; Ohura, A.; Sugahara, T. Production of a range image for facial motion analysis: A method for analyzing lip motion. Comput. Med. Imag. Graph. 2006, 30, 53–59. [Google Scholar] [CrossRef] [PubMed]
- Bettens, K.; Wuyts, F.L.; Van Lierde, K.M. Instrumental assessment of velopharyngeal function and resonance: A review. J. Commun. Disord. 2014, 52, 170–183. [Google Scholar] [CrossRef] [PubMed]
- Kao, D.S.; Soltysik, D.A.; Hyde, J.S.; Gosain, A.K. Magnetic resonance imaging as an aid in the dynamic assessment of the velopharyngeal mechanism in children. Plast. Reconstr. Surg. 2008, 122, 572–577. [Google Scholar] [CrossRef] [PubMed]
- Perry, J.L.; Kuehn, D.P. Magnetic resonance imaging and computer reconstruction of the velopharyngeal mechanism. J. Craniofac. Surg. 2009, 20, 1739–1746. [Google Scholar] [CrossRef] [PubMed]
- Rahimian, P.; Perry, J.L.; Kollara, L.; Tabrizi, N.M. Using Synchronized Audio Mapping to Track and Predict Velar and Pharyngeal Wall Locations during Dynamic MRI Sequences. Int. J. Speech Lang. Pathol. Audiol. 2016, 4, 1–10. [Google Scholar]
- Jolliffe, I.T. Principal Component Analysis; Springer: New York, NY, USA, 2002. [Google Scholar]


© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nakano, A.; Mishima, K.; Shiraishi, M.; Umeda, H.; Nakano, H.; Ueyama, Y. Quantitative Analysis of Velopharyngeal Movement by Applying Principal Component Analysis to Range Images Produced by a Three-Dimensional Endoscope. Dent. J. 2017, 5, 14. https://doi.org/10.3390/dj5020014
Nakano A, Mishima K, Shiraishi M, Umeda H, Nakano H, Ueyama Y. Quantitative Analysis of Velopharyngeal Movement by Applying Principal Component Analysis to Range Images Produced by a Three-Dimensional Endoscope. Dentistry Journal. 2017; 5(2):14. https://doi.org/10.3390/dj5020014
Chicago/Turabian StyleNakano, Asuka, Katsuaki Mishima, Mami Shiraishi, Hirotsugu Umeda, Hiroyuki Nakano, and Yoshiya Ueyama. 2017. "Quantitative Analysis of Velopharyngeal Movement by Applying Principal Component Analysis to Range Images Produced by a Three-Dimensional Endoscope" Dentistry Journal 5, no. 2: 14. https://doi.org/10.3390/dj5020014