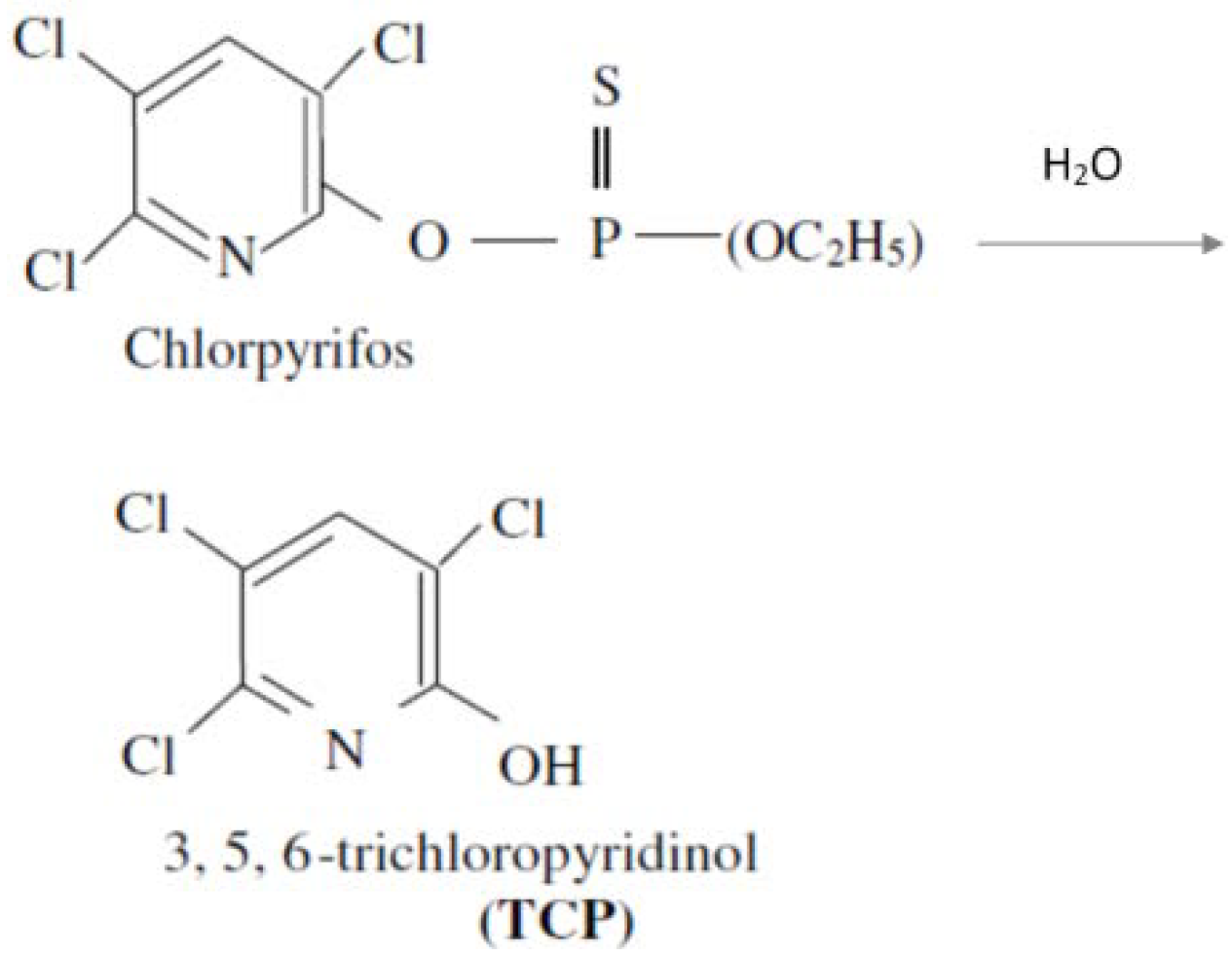
Assessment of Health Risk in Human Populations Due to Chlorpyrifos

Abstract
:1. Introduction

2. Methodology
2.1. Strategy Used for Risk Assessment
2.2. Sources of Exposure Data and Calculation of the Equivalent Chlorpyrifos Ingested Dose (ECID)
2.2.1. Background
2.2.2. Exposure from Chronic Nonoccupational Activities
2.2.3. Acute Exposure from an Application Event
2.3. Guideline Values (GV) Developed by Various Regulatory Agencies

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Guideline description (applicable population group) | Agency | Dose (log dose) (ng/kg/day) | Reference |
|---|---|---|---|
| ARfD a (acute exposure group) | USEPA | 5.0 × 103 (3.7) | [1] USEPA, 2000 |
| APAD b (acute exposure children and females 13–50 years) | 0.5 × 103 (2.7) | ||
| CRfD c (general) | USEPA | 0.3 × 103 (2.5) | |
| CPAD d (children and females 13–50 years) | USEPA | 0.03 ×103 (1.5) | |
| ADI e (general) | WHO | 10.0 × 103 (4.0) | [27] JMPR, 1999 |
| ADI e (general) | ADHA | 3.0 × 103 (3.5) | [28] Australian Government, 2008 |
3. Occurrence of Chlorpyrifos in International Populations
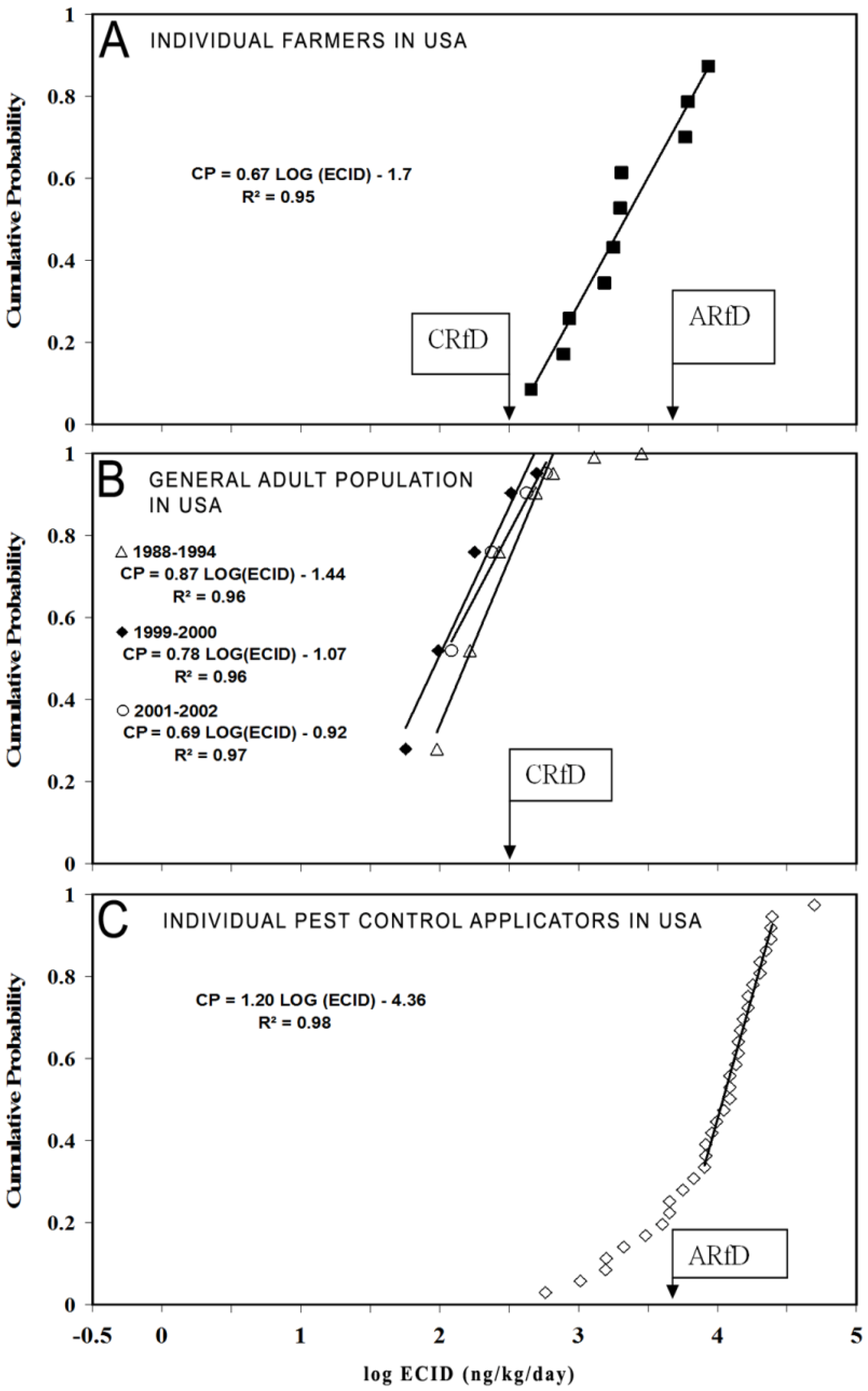
3.1. Equivalent Chlorpyrifos Ingested Dose (ECID) in Populations in the USA
3.1.1. Individual Farmers
3.1.2. General Adult Population

3.1.3. Pest Control Applicators
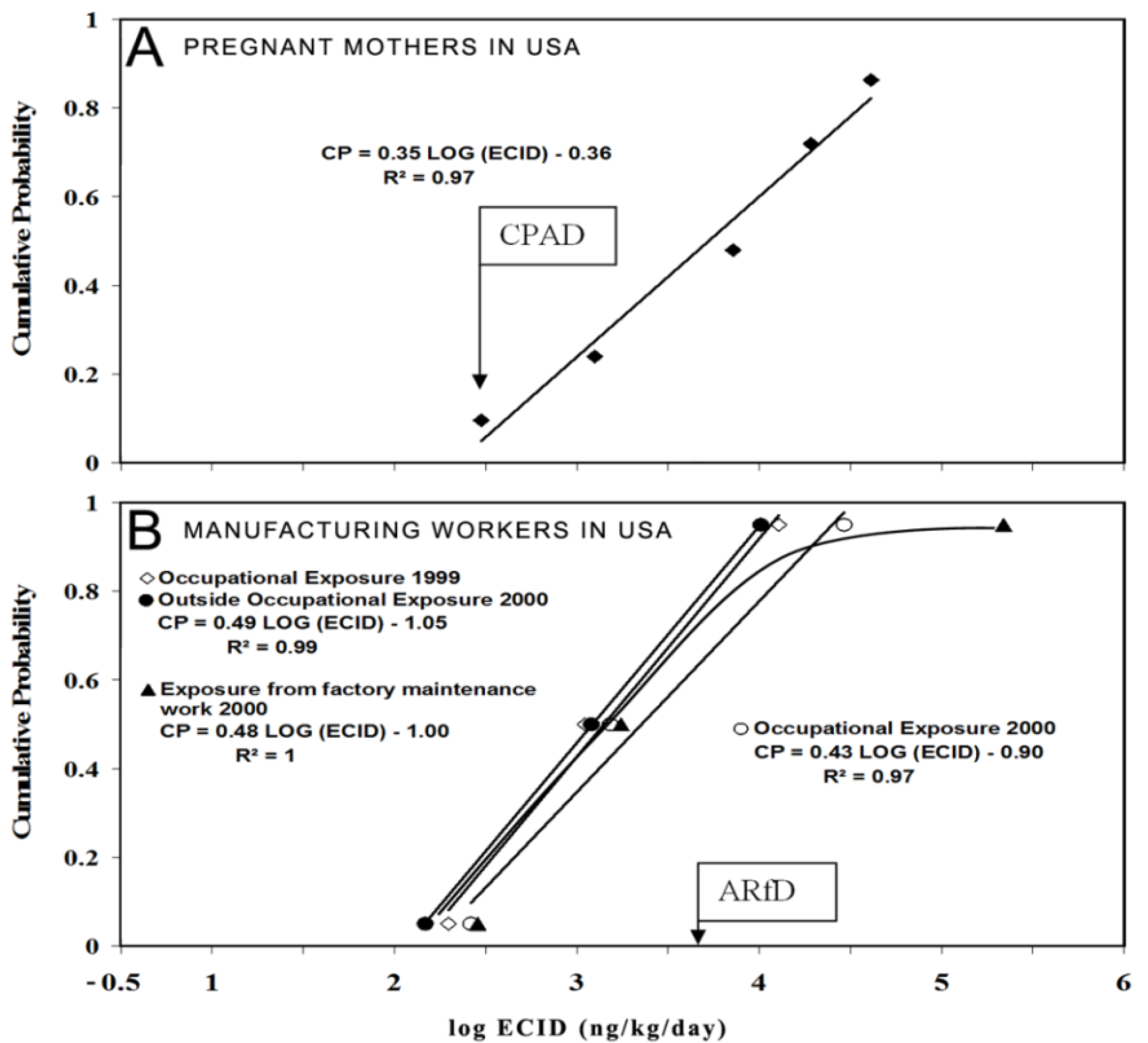
3.1.4. ECID in USA Pregnant Mothers and Children

3.1.5. ECID in Manufacturing Workers from USA
3.1.6. Overview of Chlorpyrifos Exposure in Populations of the USA
| Population | ECID (ng/kg/day) | CPD Plot characteristics a | ||
|---|---|---|---|---|
| Slope | Intercept | R2 | ||
| Farmers (2000–2001) | 8.4 × 103 | 0.7 | −1.7 | 0.95 |
| General population adults | ||||
| 1988–1994 | 0.6 × 103 | 0.9 | −1.4 | 0.97 |
| 1999–2000 | 0.5 × 103 | 0.8 | −1.1 | 0.96 |
| 2000–2001 | 0.6 × 103 | 0.7 | −0.9 | 0.98 |
| Pest control applicators (1998) | 26.0 × 103 | 1.2 | −4.3 | 0.98 |
| Manufacturing workers (1999–2000) | ||||
| Low exposure | 10.0 × 103 | 0.5 | −1.0 | 1.00 |
| High exposure | 210.0 × 103 | NA b | N/A | N/A b |
| Pregnant mothers (1998–2001) | 5.0 × 103 | 0.4 | −0.4 | 0.97 |
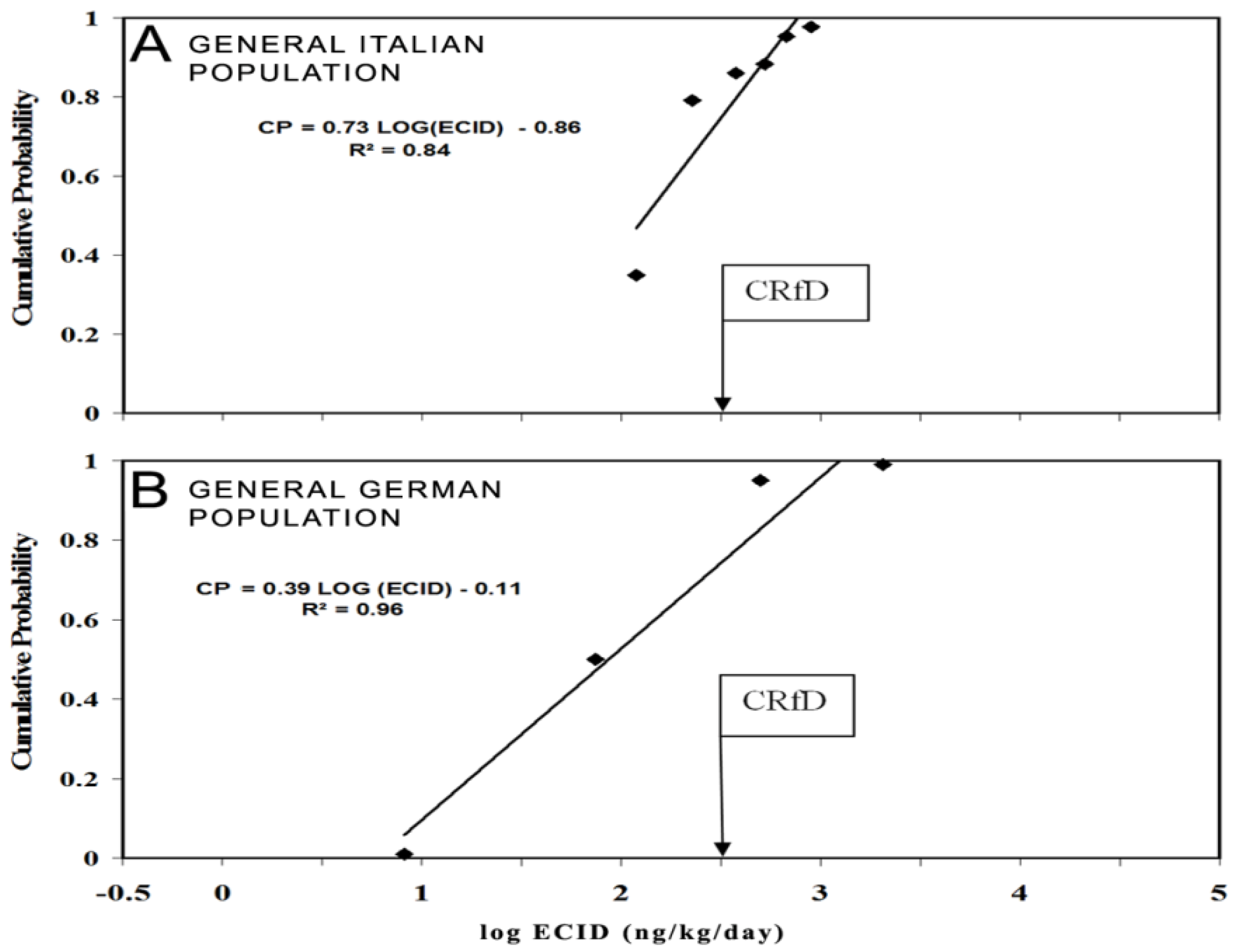
3.2. Equivalent Chlorpyrifos Ingested Doses (ECID) with Populations in Europe
3.2.1. ECID in the General Adult Population in Italy

3.2.2. ECID in German General Adult Population
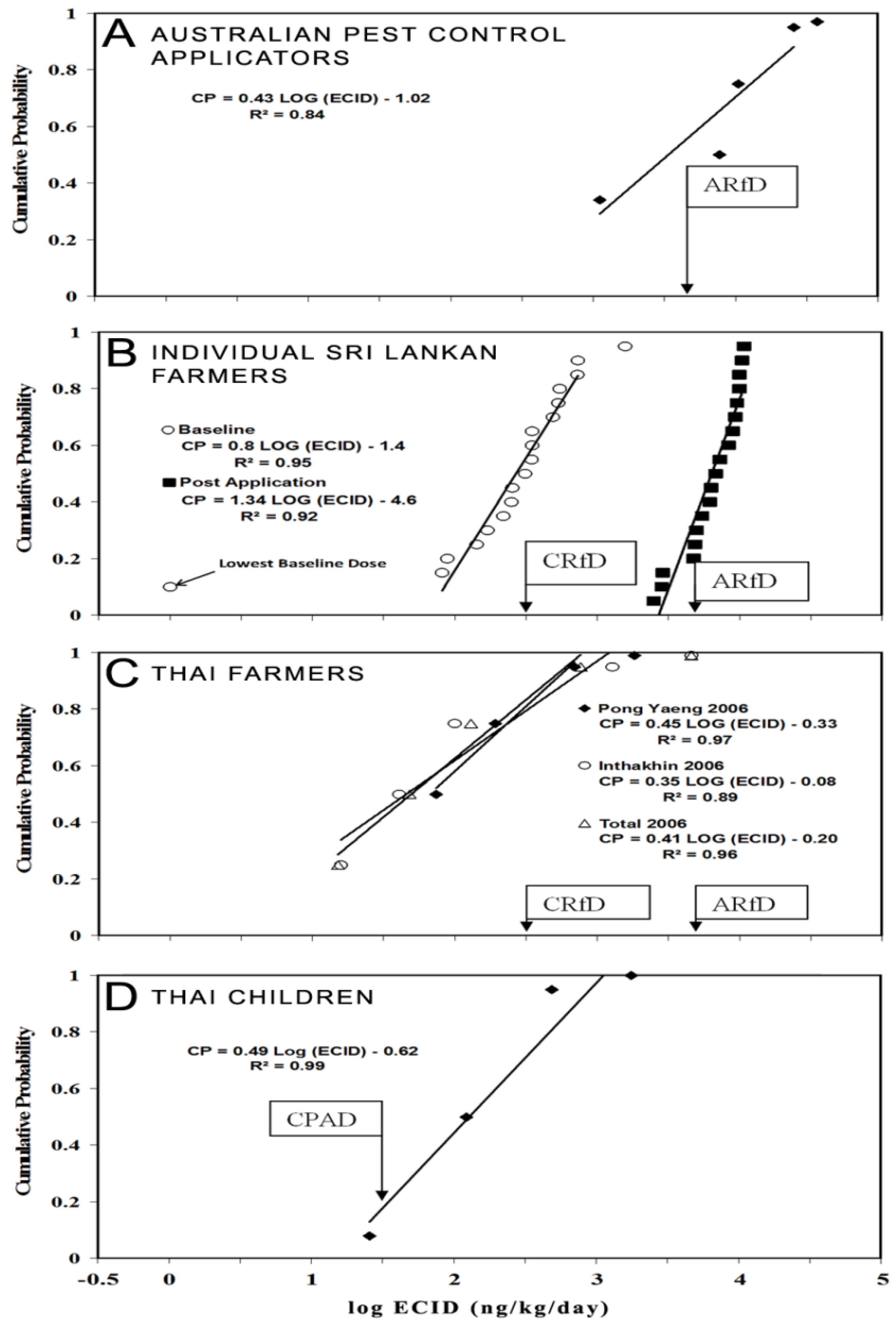
3.3. Equivalent Chlorpyrifos Ingested Doses (ECID) in Australian Pest Control Applicators

3.4. Equivalent Chlorpyrifos Ingested Dose (ECID) in Sri Lankan Farmers
3.5. Equivalent Chlorpyrifos Ingested Doses (ECID) in Thai Farmers and Children
3.5.1. ECID in Farmers
3.5.2. ECID in Children
3.6. Equivalent Chlorpyrifos Ingested Doses (ECID) in Vietnamese Farmers
| Cumulative Probability Level | Sri Lankan Farmer-Baseline, 2000 a (log dose) | Sri Lankan Farmer-Post Application, 2000 a (log dose) | Thai Farmer, 2006 b (log dose) | US Farmer–Post Application, 2000-2001 c (log dose) | Vietnam Farmer–Baseline, 2011 (log dose) | Vietnam Farmer–Post Application, 2011 (log dose) |
|---|---|---|---|---|---|---|
| 0.50 | 0.3 2 × 103 (2.5) | 6.8 × 103 (3.8) | 0.05 × 103 (1.7) | 2.0 × 103 (3.3) | 0.24 × 103 (2.4) | 19.4 × 103 (4.3) |
| 0.95 | 1.6 × 103 (3.2) | 11 × 103 (4.0) | 4.6 × 103 (3.6) | 8.4 × 103 (3.9) | 9.0 × 103 (3.95) | 97.7 × 103 (5.0) |
4. Overview of Equivalent Chlorpyrifos Ingested Dose (ECID) in Similar International Populations
4.1. Farmers from Sri Lanka, Thailand, USA and Vietnam
4.2. Pest Control Applicators and Manufacturing Workers in Australia and USA
| Cumulative probability level | US pest control applicators (1998) a (ng/kg/day) (log dose) | US manufacturing workers (1999–2000) b (ng/kg/day) | Australian pest control applicators (1998–1999) c (ng/kg/day) (log dose) | |
|---|---|---|---|---|
| Low Exposure (log dose) | High Exposure (log dose) | |||
| 0.50 | 12.0 × 103 (4.1) | 1.1 × 103 (3.04) | 1.8 × 103 (3.2) | 7.8 × 103 (3.9) |
| 0.95 | 26.0 × 103 (4.4) | 10.0 × 103 (4.0) | 210.0 × 103 (5.3) | 26.0 × 103 (4.4) |
4.3. General Populations of Europe, Sri Lanka, Thailand, USA and Vietnam
| Cumulative Probability Level | Sri Lankan Farmer–Baseline (2000) a (ng/kg/day) (log Dose) | USA General Population b (2001–2002) (ng/kg/day) (log Dose) | European General Population c (ng/kg/day) (log Dose) | USA Pregnant Mothers d (1998–2001) (ng/kg/day) (log Dose) | Thai Children e (2009) (ng/kg/day) (log Dose) | Vietnam Farmer–Baseline (2011) (ng/kg/ day) (log dose) | |
|---|---|---|---|---|---|---|---|
| Italy (1997) | Germany (2001) | ||||||
| 0.50 | 0.3 × 103 (2.5) | 0.1 × 103 (2.0) | 0.1 × 103 (2.0) | 0.1 × 103 (2.0) | 0.8 × 103 (2.9) | 0.24 × 103 (2.4) | 0.1 × 103 (2.0) |
| 0.95 | 1.6 × 103 (3.2) | 0.6 × 103 (2.8) | 0.6 (2.8) | 0.5 (2.7) | 5.0 × 103 (3.7) | 9.0 × 103 (3.95) | 0.5 × 103 (2.7) |
5. Risk Characterisation using the Hazard Quotient (HQ)
5.1. Background
5.2. Hazard Quotients (HQ) Calculated Using the US EPA Guideline Values (GVs)
| Cumulative Probability | Hazard Quotients (HQ) | Vietnamese farmer-Post Application b | |||||
|---|---|---|---|---|---|---|---|
| Sri Lankan farmer-Post Application b | US farmer b | US pest control applicator c | US manufacturing worker c | Australian pest control applicator c | |||
| Low Exposure | High Exposure | ||||||
| 0.50 | 1.3 | 0.4 | 2.4 | 0.2 | 0.3 | 1.5 | 3.9 |
| 0.95 | 2.2 | 1.7 | 5.2 | 2.6 | 42.0 | 5.2 | 19.5 |
6. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- USEPA. 2000; Chlorpyrifos; Human Health Risk Assessment, Health Effects Division (7509C), Office of Pesticide Programs, U.S. Environmental Protection Agency: Washington, DC, USA.
- Aponso, G.L.M.; Manuweera, G.K. Exposure and risk assessment for farmers occupationally exposed to chlorpyrifos. Ann. Sri. Lanka Dep. Agric. 2002, 4, 233–244. [Google Scholar]
- Ecobichon, D.J. Organophosphorus Ester Insecticides. In Pesticides and Neurological Diseases; Ecobichon, D.J., Joy, R.M., Eds.; CRC Press: Boca Raton, FL, USA, 1982; pp. 171–250. [Google Scholar]
- Garabrant, D.H.; Aylward, L.L.; Berent, S.; Chen, Q.; Timchalk, C.; Burns, C.J.; Hays, S.M.; Albers, J.W. Cholinesterase inhibition in chlorpyrifos workers: Characterization of biomarkers of exposure and response in relation to urinary TCPy. J. Expo. Environ. Epidemiol. 2008, 19, 634–642. [Google Scholar]
- Dyro, M. Organophosphates. Neurology, eMedicine. 2006. Available online: http://emedicine.medscape.com (accessed on 18 October 2008).
- Lotti, M. Treatment of acute organophosphate poisoning. Med. J. Aust. 1991, 154, 51–55. [Google Scholar]
- De Alwis, L.B.L.; Salgado, M.S.L. Agrochemical Poisoning in Sri Lanka. In Pesticides in Sri Lanka: Documentation of Selected Literature and Legal Aspects; Fernando, R., Ed.; Friedrich-Ebert-Stiftung: Berlin, Germany, 1989; pp. 281–304. [Google Scholar]
- Jeyaratnam, J. Acute pesticide poisoning: A major global health problem. World Health Stat. Q 1990, 43, 139–144. [Google Scholar]
- Sivayoganathan, C.; Gnanachandran, S.; Lewis, J.; Fernando, M. Protective measure use and symptoms among agro pesticide applicators in Sri Lanka. Soc. Sci. Med. 1995, 40, 431–436. [Google Scholar] [CrossRef]
- Van Der Hoek, W.; Konradsen, F.; Athukorala, K.; Wanigadewa, T. Pesticide poisoning: A major health problem in Sri Lanka. Soc. Sci. Med. 1998, 46, 495–504. [Google Scholar]
- Smit, L.A.M.; Van-Wendel-De-Joode, B.N.; Heederik, D.; Peiris-John, R.J.; Van Der Hoek, W. Neurological symptoms among Sri Lankan farmers occupationally exposed to acetyl cholinesterase-Inhibiting Insecticides. Am. J. Ind. Med. 2003, 44, 254–264. [Google Scholar] [CrossRef]
- Phung, D.T.; Connell, D.; Miller, G.; Hodge, M.; Patel, R.; Cheng, R.; Abeyewardene, M.; Chu, C. Biological monitoring of chlorpyrifos exposure to rice farmers in Vietnam. Chemosphere 2012, 87, 294–300. [Google Scholar] [CrossRef]
- Phung, D.T.; Connell, D.; Miller, G.; Chu, C. Probabilistic assessment of chlorpyrifos exposure to rice farmers in Viet Nam. J. Expo. Sci. Environ. Epidemiol. 2012, 22, 417–423. [Google Scholar] [CrossRef]
- Phung, D.T.; Connell, D.; Yu, Q.J.; Chu, C. Health risk characterization of chlorpyrifos using epidemiological dose-response data and probabilistic techniques: A case study with rice farmers in Vietnam. Risk Anal. 2013, 33, 1596–1607. [Google Scholar] [CrossRef]
- Yu, Q.J.; Cao, Q.; Connell, D.W. An overall risk probability-based method for quantification of synergistic and antagonistic effects in health risk assessment for mixtures: Theoretical concepts. Environ. Sci. Pollut. Res. 2012, 19, 2627–2633. [Google Scholar] [CrossRef]
- Giesy, J.P.; Solomon, K.R.; Coates, J.R.; Dixon, K.R.; Giddings, J.M.; Kenaga, E.E. Chlorpyrifos: Ecological risk assessment in North American aquatic environments. Rev. Environ. Contam. Toxicol. 1999, 160, 1–129. [Google Scholar]
- Eaton, D.L.; Daroff, R.B.; Autrup, H.; Bridges, J.; Buffer, P.; Costa, L.G.; Coyle, J.; Mckhann, G.; Mobley, W.C.; Nadel, L.; et al. Review of the toxicology of chlorpyrifos with an emphases on human exposure and neurodevelopment. Crit. Rev. Toxocol. 2008, S2, 1–125. [Google Scholar]
- CDC. Third National Report on Human Exposure to Environmental Chemicals; Department of Health and Human Services, Centers for Disease Control and Prevention: Atlanta, GA, USA, 2005.
- Cole, T.B.; Fisher, J.C.; Burbacher, T.M.; Costa, L.G.; Furlong, C.E. Neurobehavioral assessment of mice following repeated postnatal exposure to chlorpyrifos oxon. Neurotoxicol. Teratol. 2012, 34, 311–322. [Google Scholar] [CrossRef]
- Price, P.S.; Schnelle, K.D.; Cleveland, C.B.; Bartels, B.J.; Hinderliter, P.M.; Timchalk, C.; Poet, T.S. Application of a source-to-outcome model for the assessment of health impacts from dietary exposures to insecticide residues. Regul. Toxicol. Pharmacol. 2011, 61, 23–33. [Google Scholar]
- Mage, D.T.; Allen, R.H.; Kodali, A. Creatinine corrections for estimating children’s and adult’s pesticide intake doses in equilibrium with urinary pesticide and creatinine concentrations. J. Expo. Sci. Environ. Epidemiol. 2008, 18, 360–368. [Google Scholar] [CrossRef]
- Mage, D.T.; Allen, R.H.; Gondy, G.; Smith, W.; Barr, D.B.; Needham, L.L. Estimating pesticide dose from urinary pesticide concentration data by creatinine correction in the third National Health and Nutrition Examination Survey (NHANES-III). J. Expo. Anal. Environ. Epidemiol. 2004, 14, 457–465. [Google Scholar] [CrossRef]
- Nolan, R.J.; Rick, D.L.; Freshour, N.L.; Saunders, J.H. Chlorpyrifos: Pharmacokinetics in human volunteers. Toxicol. Appl. Pharmacol. 1984, 73, 8–15. [Google Scholar] [CrossRef]
- Attfield, K.R.; Hughes, M.D.; Spengler, J.D.; Chensheng, L. Within- and between-child Variation in repeated urinary pesticide metabolite measurements over a 1-year period. Environ. Health Perspect. 2014, 122, 201–206. [Google Scholar]
- Saieva, C.; Aprea, C.; Tumino, R.; Masala, G.; Salvini, S.; Frasca, G.; Giurdanella, M.C.; Zanna, I.; Decarli, A.; Sciarra, G.; Palli, D. Twenty four hour urinary excretion of ten pesticide metabolites in healthy adults in two different areas of Italy (Florence and Ragusa). Sci. Total Environ. 2004, 332, 71–80. [Google Scholar] [CrossRef]
- Scher, D.P.; Sawchuk, R.J.; Alexander, B.H.; Adgate, J.L. Estimating Absorbed Dose of pesticides in a field setting using biomonitoring data and pharmacokinetic models. J. Toxicol. Environ. Health A 2008, 71, 373–383. [Google Scholar] [CrossRef]
- Joint FAO/WHO Meeting on Pesticide Residues (JMPR). Chlopyrifos. In Pesticide Residues in Food-1999 Evaluations 1999 Part II—Toxicological WHO/PCS/00.4; International Programme on Chemical Safety, World Health Organization: Genava, Switzerland, 1999. [Google Scholar]
- Australian Department of Health and Aging. ADI List: Acceptable Daily Intakes for Agricultural and Veterinary Chemicals; Australian Government, Office of Chemical Safety, Department of Health and Ageing: Canberra, Australia, 2008.
- USEPA. Chlorpyrifos Preliminary Human Health Risk Assessment for Registration Review; Office of Chemical Safety and Pollution Prevention, DP No. D388070; U.S. Environmental Protection Agency: Washington, DC, USA, 2011.
- Hill, R.H., Jr.; Head, S.L.; Baker, S.; Gregg, M.; Shealy, D.B.; Bailey, S.L.; Williams, C.C.; Sampson, E.J.; Needham, L.L. Pesticide residues in urine of adults living in the United States: Reference range concentrations. Environ. Res. 1995, 71, 99–108. [Google Scholar] [CrossRef]
- Barr, D.B.; Allen, R.; Olsson, A.O.; Bravo, R.; Caltabiano, L.M.; Montesano, A.; Nguyen, J.; Udunka, S.; Walden, D.; Walker, R.D.; et al. Concentrations of selective metabolites of organophosphorous pesticides in the United States population. Environ. Res. 2005, 99, 314–326. [Google Scholar]
- Hines, C.; Deddens, J.A. Determinants of chlorpyrifos exposures and urinary 3,5,6-trichloro-2-pyridinol levels among termiticide applicators. Ann. Occup. Hyg. 2001, 45, 309–321. [Google Scholar]
- USEPA. Inrerim Reregristration Eligibility for Chlorpyrifos; United States Environmental Protection Agency: Washington, DC, USA, 2002.
- Berkowitz, G.S.; Obel, J.; Deych, E.; Lapinsid, R.; Godbold, J.; Liu, Z.; Landrigan, P.J.; Wolf, M.S. Exposure to indoor pesticides during pregnancy in a multiethnic, urban cohort. Environ. Health Perspect. 2003, 111, 79–84. [Google Scholar]
- Morgan, M.K.; Sheldon, L.S.; Croghan, C.W.; Jones, P.A.; Robertson, G.L.; Chuang, J.C.; Wilson, N.K.; Lyu, C.W. Exposure of preschool children to chlorpyrifos an its degradation. J. Expo. Anal. Environ. Epidemiol. 2005, 15, 297–309. [Google Scholar] [CrossRef]
- Morgan, M.K.; Sheldon, L.S.; Jones, P.A.; Croghan, C.W.; Chuang, J.C.; Wilson, N.K. The reliability of using urinary biomarkers to estimate children’s exposure to chlorpyrifos and diazinon. J. Expo. Sci. Environ. Epidemiol. 2011, 21, 280–290. [Google Scholar] [CrossRef]
- Rauh, V.; Arunajadai, S.; Horton, M.; Perera, F.; Hoepner, L.; Barr, D.B.; Wyatt, R. 7-Year neurodevelopmental scores and prenatal exposure to chlorpyrifos, a common agricultural pesticide. Environ. Health Perspect. 2011, 119, 1196–1201. [Google Scholar] [CrossRef]
- Aprea, C.; Betta, A.; Catenacci, G.; Lotti, A.; Magnaghi, S.; Barisano, A.; Passini, V.; Pavan, I.; Sciarra, G.; Vitalone, V.; Minola, C. Referene values of urinary 3,5,6-trichloro-2 pyridinol in the Italian population-validation of analytical method and preliminary results (multientric study). J. AOAC Int. 1999, 82, 305–312. [Google Scholar]
- Koch, M.; Hardt, J.; Angrer, J. Biological monitoring of exposure of the general population to the organophosphorus pesticides chlorpyrifos and chlorpyrifosmethyl by determination of their specific metabolite 3,5,6-trichloro-2-pyridinol. Int. J. Hyg. Environ. Health 2001, 204, 175–180. [Google Scholar] [CrossRef]
- Cattani, M. Exposure and Health Effects among Field Workers Using the Organophosphate Chlorpyrifos. Ph.D. Thesis, School of Environmental Science, Murdoch University, Perth, Western Australia, 2004. [Google Scholar]
- Panuwet, P.; Prapamontol, T.; Chantara, S.; Thavornyuthikarn, P.; Montesano, M.A.; Whitehead, R.D., Jr.; Barr, D.B. Concentrations of urinary pesticide metabolites in small-scale farmers in Chiang Mai Province, Thailand. Sci. Total Environ. 2008, 407, 655–668. [Google Scholar]
- Panuwet, P.; Prapamontol, T.; Chantara, S.; Barr, D.B. Urinary pesticides metabolites in school students from northern Thailand. Int. J. Hyg. Environ. Health 2009, 212, 288–297. [Google Scholar] [CrossRef]
- Van Wendelde Joode, B.; Barraza, D.; Ruepert, C.; Mora, A.M.; Cordoba, L.; Oberg, M.; Wesseling, C.; Mergler, D.; Lindh, C.H. Indigenous children living nearby plantations with chlorpyrifos-treated bags have elevated 3,5,6-trichloro-2-pyridinol (TCPy) urinary concentrations. Environ. Res. 2012, 117, 17–26. [Google Scholar] [CrossRef]
- Liu, P.; Wu, C.-H.; Chang, X.-L.; Qi, X.-J.; Zheng, M.-L.; Zhou, Z.-J. Assessment of chlorpyrifos exposure and absorbed daily doses among infants living in an agricultural area of the Province of Jiangsu, China. Int. Arch. Occup. Environ. Health 2013. [Google Scholar] [CrossRef]
© 2014 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/3.0/).
Share and Cite
Marasinghe, J.; Yu, Q.; Connell, D. Assessment of Health Risk in Human Populations Due to Chlorpyrifos. Toxics 2014, 2, 92-114. https://doi.org/10.3390/toxics2020092
Marasinghe J, Yu Q, Connell D. Assessment of Health Risk in Human Populations Due to Chlorpyrifos. Toxics. 2014; 2(2):92-114. https://doi.org/10.3390/toxics2020092
Chicago/Turabian StyleMarasinghe, Jeevani, Qiming Yu, and Des Connell. 2014. "Assessment of Health Risk in Human Populations Due to Chlorpyrifos" Toxics 2, no. 2: 92-114. https://doi.org/10.3390/toxics2020092