Cadmium Exposure Disrupts Periodontal Bone in Experimental Animals: Implications for Periodontal Disease in Humans

Abstract
:1. Introduction
2. Materials and Methods
2.1. Animal Studies
2.2. Collection and Preparation of Jaw Samples
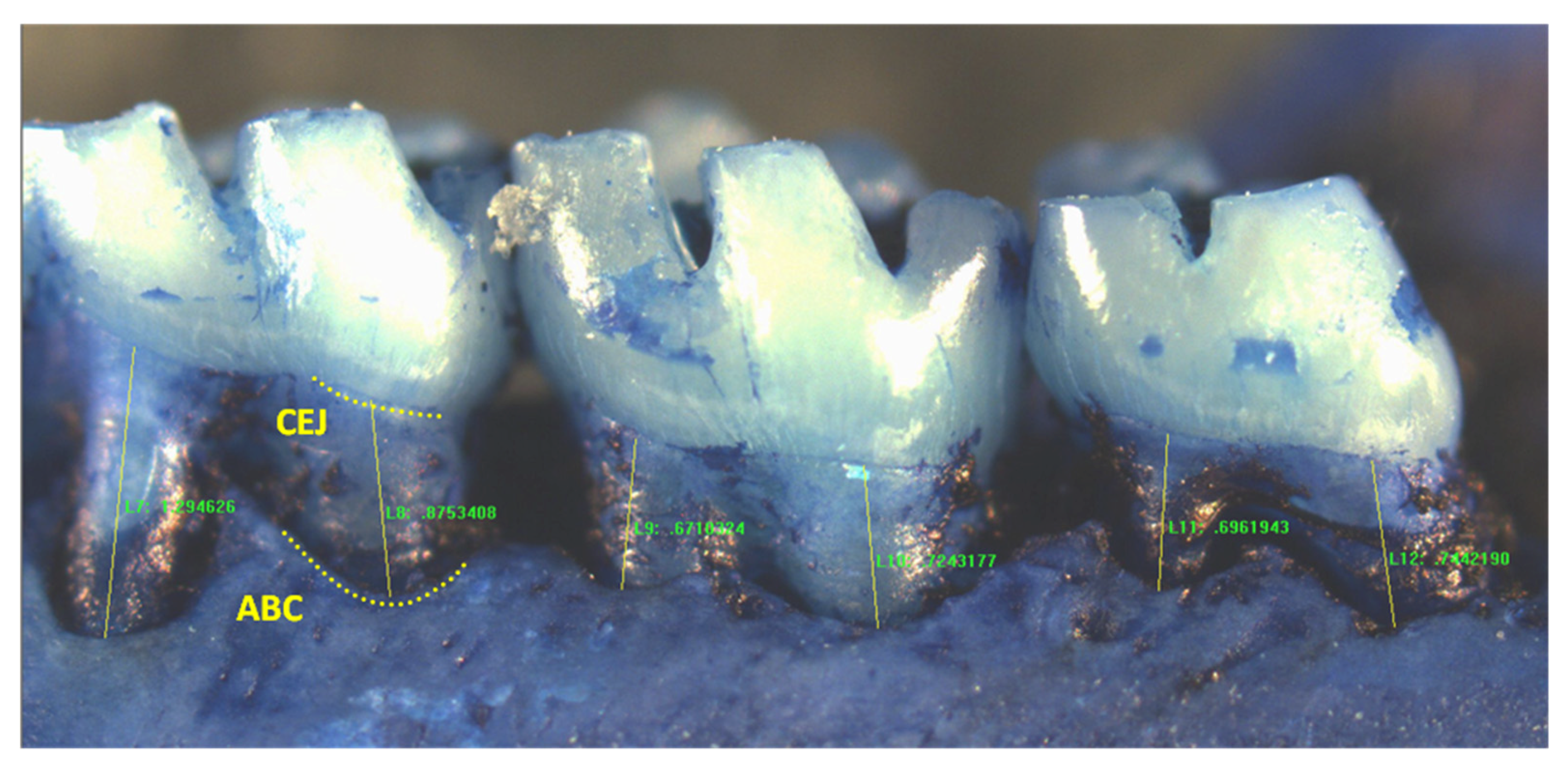
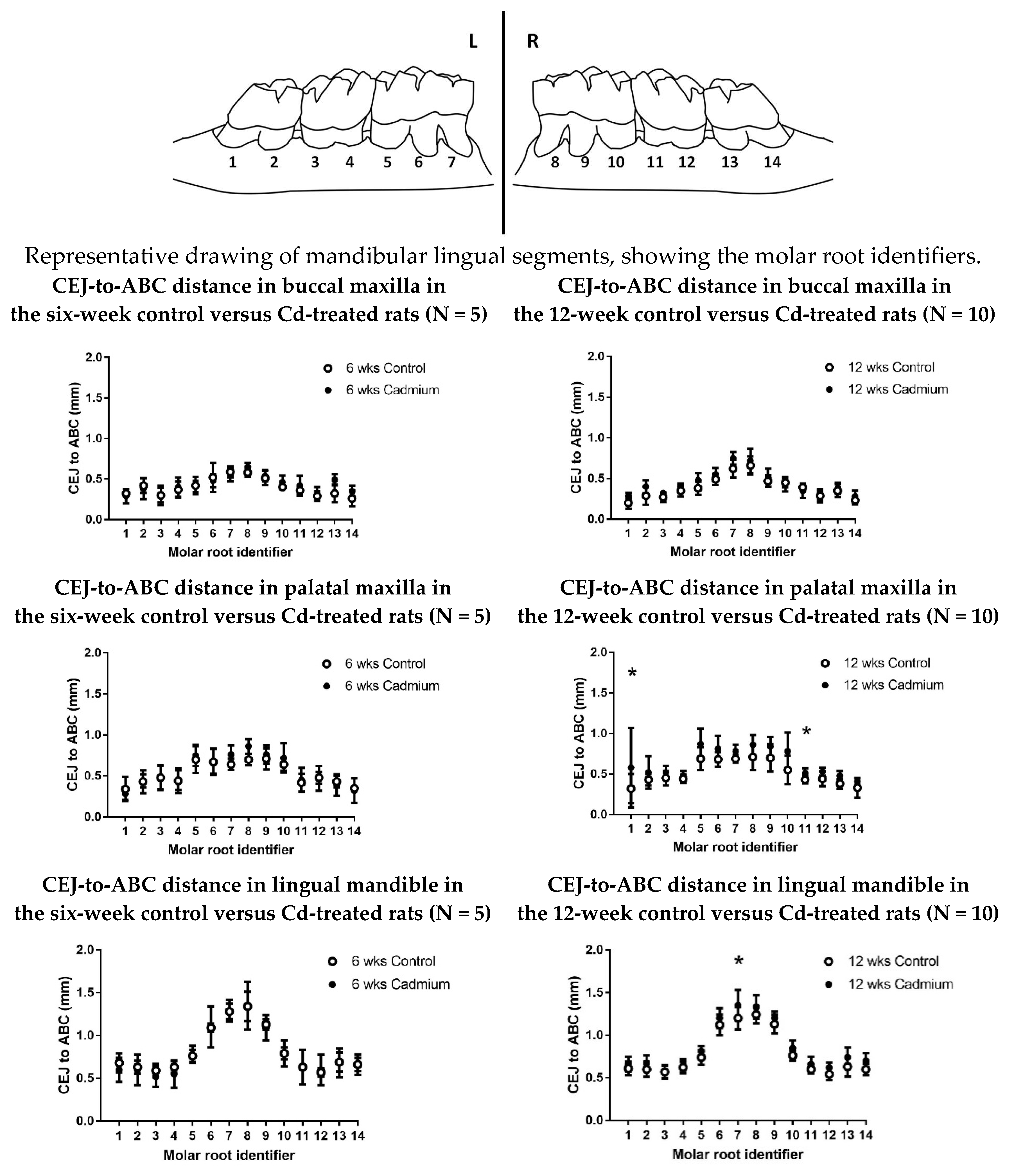
2.3. Morphometric Analysis of Periodontal Bone Levels
2.4. Statistical Analysis
3. Results
4. Discussion
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Facing the Facts #1, Chronic Diseases and Their Common Risk Factors. Available online: http://www.who.int/chp/chronic_disease_report/media/Factsheet1.pdf (accessed on 26 January 2018).
- Burt, B. Position paper: Epidemiology of periodontal diseases. J. Periodontol. 2005, 76, 1406–1419. [Google Scholar] [PubMed]
- Cekici, A.; Kantarci, A.; Hasturk, H.; Van Dyke, T.E. Inflammatory and immune pathways in the pathogenesis of periodontal disease. Periodontology 2000 2014, 64, 57–80. [Google Scholar] [CrossRef] [PubMed]
- Eke, P.I.; Dye, B.A.; Wei, L.; Thornton-Evans, G.O.; Genco, R.J. CDC Periodontal Disease Surveillance workgroup: James Beck, Gordon Douglass, Roy Page, 2012. Prevalence of periodontitis in adults in the United States: 2009 and 2010. J. Dent. Res. 2012, 91, 914–920. [Google Scholar] [CrossRef] [PubMed]
- Tomar, S.L.; Asma, S. Smoking-attributable periodontitis in the United States: Findings from NHANES III. J. Periodontol. 2000, 71, 743–751. [Google Scholar] [CrossRef] [PubMed]
- Borojevic, T. Smoking and periodontal disease. Mater. Sociomed. 2012, 24, 274–276. [Google Scholar] [CrossRef] [PubMed]
- Jarup, L.; Berglund, M.; Elinder, C.G.; Nordberg, G.; Vahter, M. Health effects of cadmium exposure—A review of the literature and a risk estimate. Scand. J. Work Environ. Health 1998, 24 (Suppl. 1), 1–51. [Google Scholar] [PubMed]
- Paschal, D.C.; Burt, V.; Caudill, S.P.; Gunter, E.W.; Pirkle, J.L.; Sampson, E.J.; Miller, D.T.; Jackson, R.J. Exposure of the U.S. population aged 6 years and older to cadmium: 1988–1994. Arch. Environ. Contam. Toxicol. 2000, 38, 377–383. [Google Scholar] [CrossRef] [PubMed]
- Edwards, J.; Ackerman, C. A review of diabetes mellitus and exposure to the environmental toxicant cadmium with an emphasis on likely mechanisms of action. Curr. Diabetes Rev. 2016, 12, 252–258. [Google Scholar] [CrossRef] [PubMed]
- Satarug, S.; Swaddiwudhipong, W.; Ruangyuttikarn, W.; Nishijo, M.; Ruiz, P. Modeling cadmium exposures in low- and high-exposure areas in Thailand. Environ. Health Perspect. 2013, 121, 531–536. [Google Scholar] [CrossRef] [PubMed]
- Prozialeck, W.C.; Edwards, J.R. Early biomarkers of cadmium exposure and nephrotoxicity. Biometals 2010, 23, 793–809. [Google Scholar] [CrossRef] [PubMed]
- Prozialeck, W.C.; Edwards, J.R. Mechanisms of cadmium-induced proximal tubule injury: New insights with implications for biomonitoring and therapeutic interventions. J. Pharmacol. Exp. Ther. 2012, 343, 2–12. [Google Scholar] [CrossRef] [PubMed]
- Friberg, L. Cadmium and the kidney. Environ. Health Perspect. 1984, 54, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Bhattacharyya, M.H. Cadmium osteotoxicity in experimental animals: Mechanisms and relationship to human exposures. Toxicol. Appl. Pharmacol. 2009, 238, 258–265. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schutte, R.; Nawrot, T.S.; Richart, T.; Thijs, L.; Vanderschueren, D.; Kuznetsova, T.; Van Hecke, E.; Roels, H.A.; Staessen, J.A. Bone resorption and environmental exposure to cadmium in women: A population study. Environ. Health Perspect. 2008, 116, 777–783. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nishijo, M.; Nambunmee, K.; Suvagandha, D.; Swaddiwudhipong, W.; Ruangyuttikarn, W.; Nishino, Y. Gender-specific impact of cadmium exposure on bone metabolism in older people living in a cadmium-polluted area in Thailand. Int. J. Environ. Res. Public Health 2017, 14, 401. [Google Scholar] [CrossRef] [PubMed]
- Penoni, D.C.; Fidalgo, T.K.; Torres, S.R.; Varela, V.M.; Masterson, D.; Leao, A.T.; Maia, L.C. Bone density and clinical periodontal attachment in postmenopausal women: A systematic review and meta-analysis. J. Dent. Res. 2017, 96, 261–269. [Google Scholar] [CrossRef] [PubMed]
- Arora, M.; Weuve, J.; Schwartz, J.; Wright, R.O. Association of environmental cadmium exposure with periodontal disease in U.S. adults. Environ. Health Perspect. 2009, 117, 739–744. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Han, D.H.; Lee, H.J.; Lim, S. Smoking induced heavy metals and periodontitis: Findings from the Korean National Health and Nutrition Examination Surveys 2008–2010. J. Clin. Periodontol. 2013, 40, 850–858. [Google Scholar] [CrossRef] [PubMed]
- Won, Y.S.; Kim, J.H.; Kim, Y.S.; Bae, K.H. Association of internal exposure of cadmium and lead with periodontal disease: A study of the fourth Korean National Health and Nutrition Examination Survey. J. Clin. Periodontol. 2013, 40, 118–124. [Google Scholar] [CrossRef] [PubMed]
- Alhasmi, A.M.; Gondal, M.A.; Nasr, M.M.; Shafik, S.; Habibullah, Y.B. Detection of toxic elements using laser-induced breakdown spectroscopy in smokers’ and nonsmokers’ teeth and investigation of periodontal parameters. Appl. Opt. 2015, 54, 7342–7349. [Google Scholar] [CrossRef] [PubMed]
- Kim, Y.; Lee, B.K. Association between blood lead and mercury levels and periodontitis in the Korean general population: Analysis of the 2008–2009 Korean national health and nutrition examination survey data. Int. Arch. Occup. Environ. Health 2013, 86, 607–613. [Google Scholar] [CrossRef] [PubMed]
- Herman, M.; Golasik, M.; Piekoszewski, W.; Walas, S.; Napierala, M.; Wyganowska-Swiatkowska, M.; Kurhanska-Flisykowska, A.; Wozniak, A.; Florek, E. Essential and toxic metals in oral fluid—A potential role in the diagnosis of periodontal diseases. Biol. Trace Elem. Res. 2016, 173, 275–282. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dye, B.A.; Dillon, C.F. Elevated cadmium exposure may be associated with periodontal bone loss. J. Evid. Based Dent. Pract. 2010, 10, 109–111. [Google Scholar] [CrossRef] [PubMed]
- Prozialeck, W.C.; VanDreel, A.; Ackerman, C.D.; Stock, I.; Papaeliou, A.; Yasmine, C.; Wilson, K.; Lamar, P.C.; Sears, V.L.; Gasiorowski, J.Z.; et al. Evaluation of cystatin C as an early biomarker of cadmium nephrotoxicity in the rat. Biometals 2016, 29, 131–146. [Google Scholar] [CrossRef] [PubMed]
- Albandar, J.M.; Brunelle, J.A.; Kingman, A. Destructive periodontal disease in adults 30 years of age and older in the United States, 1988–1994. J. Periodontol. 1999, 70, 13–29. [Google Scholar] [CrossRef] [PubMed]
- Ainamo, J.; Barmes, D.; Beagrie, G.; Cutress, T.; Martin, J.; Sardo-Infirri, J. Development of the World Health Organization (WHO) Community Periodontal Index of Treatment needs (CPITN). Int. Dent. J. 1982, 32, 281–291. [Google Scholar] [PubMed]
- Eke, P.I.; Thornton-Evans, G.O.; Wei, L.; Borgnakke, W.S.; Dye, B.A. Accuracy of NHANES periodontal examination protocols. J. Dent. Res. 2010, 89, 1208–1213. [Google Scholar] [CrossRef] [PubMed]
- Miller, N.A.; Benamghar, L.; Roland, E.; Martin, G.; Penaud, J. An analysis of the community periodontal index of treatment needs. Studies on adults in France. III—Partial examinations versus full-mouth examinations. Community Dent. Health 1990, 7, 249–253. [Google Scholar] [PubMed]
- Costich, E.R. A Quantitative Evaluation of the Effect of Copper on Alveolar Bone Loss in the Syrian Hamster. J. Periodontol. 1955, 26, 301–305. [Google Scholar] [CrossRef]
- Prozialeck, W.C.; Vaidya, V.S.; Liu, J.; Waalkes, M.P.; Edwards, J.R.; Lamar, P.C.; Bernard, A.M.; Dumont, X.; Bonventre, J.V. Kidney injury molecule-1 is an early biomarker of cadmium nephrotoxicity. Kidney Int. 2007, 72, 985–993. [Google Scholar] [CrossRef] [PubMed]
- Prozialeck, W.C.; Edwards, J.R.; Lamar, P.C.; Liu, J.; Vaidya, V.S.; Bonventre, J.V. Expression of kidney injury molecule-1 (Kim-1) in relation to necrosis and apoptosis during the early stages of Cd-induced proximal tubule injury. Toxicol. Appl. Pharmacol. 2009, 238, 306–314. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aoyagi, T.; Hayakawa, K.; Miyaji, K.; Ishikawa, H.; Hata, M. Cadmium nephrotoxicity and evacuation from the body in a rat modeled subchronic intoxication. Int. J. Urol. 2003, 10, 332–338. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dudley, R.E.; Gammal, L.M.; Klaassen, C.D. Cadmium-induced hepatic and renal injury in chronically exposed rats: Likely role of hepatic cadmium-metallothionein in nephrotoxicity. Toxicol. Appl. Pharmacol. 1985, 77, 414–426. [Google Scholar] [CrossRef]
- Goyer, R.A.; Miller, C.R.; Zhu, S.Y.; Victery, W. Non-metallothionein-bound cadmium in the pathogenesis of cadmium nephrotoxicity in the rat. Toxicol. Appl. Pharmacol. 1989, 101, 232–244. [Google Scholar] [CrossRef]
- Shaikh, Z.A.; Northup, J.B.; Vestergaard, P. Dependence of cadmium-metallothionein nephrotoxicity on glutathione. J. Toxicol. Environ. Health A 1999, 57, 211–222. [Google Scholar] [PubMed]
- Carlsson, L.; Lundholm, C.E. Characterisation of the effects of cadmium on the release of calcium and on the activity of some enzymes from neonatal mouse calvaria in culture. Comp. Biochem. Physiol. C Pharmacol. Toxicol. Endocrinol. 1996, 115, 251–256. [Google Scholar] [CrossRef]
- Romare, A.; Lundholm, C.E. Cadmium-induced calcium release and prostaglandin E2 production in neonatal mouse calvaria are dependent on COX-2 induction and protein kinase C activation. Arch. Toxicol. 1999, 73, 223–228. [Google Scholar] [CrossRef] [PubMed]
- Suzuki, Y.; Morita, I.; Yamane, Y.; Murota, S. Cadmium stimulates prostaglandin E2 production and bone resorption in cultured fetal mouse calvaria. Biochem. Biophys. Res. Commun. 1989, 158, 508–513. [Google Scholar] [CrossRef]
- Marth, E.; Barth, S.; Jelovcan, S. Influence of cadmium on the immune system. Description of stimulating reactions. Cent. Eur. J. Public Health 2000, 8, 40–44. [Google Scholar] [PubMed]
- Marth, E.; Jelovcan, S.; Kleinhappl, B.; Gutschi, A.; Barth, S. The effect of heavy metals on the immune system at low concentrations. Int. J. Occup. Med. Environ. Health 2001, 14, 375–386. [Google Scholar] [PubMed]
- Hemdan, N.Y.; Emmrich, F.; Sack, U.; Wichmann, G.; Lehmann, J.; Adham, K.; Lehmann, I. The in vitro immune modulation by cadmium depends on the way of cell activation. Toxicology 2006, 222, 37–45. [Google Scholar] [CrossRef] [PubMed]
- Horiguchi, H.; Oguma, E.; Sasaki, S.; Miyamoto, K.; Ikeda, Y.; Machida, M.; Kayama, F. Environmental exposure to cadmium at a level insufficient to induce renal tubular dysfunction does not affect bone density among female Japanese farmers. Environ. Res. 2005, 97, 83–92. [Google Scholar] [CrossRef] [PubMed]
- Guzzi, G.; Pigatto, P.D.; Ronchi, A. Periodontal disease and environmental cadmium exposure. Environ. Health Perspect. 2009, 117, A535–A536. [Google Scholar] [CrossRef] [PubMed]
- Rivaldo, E.G.; Padilha, D.P.; Hugo, F.N. Alveolar bone loss and aging: A model for the study in mice. J. Periodontol. 2005, 76, 1966–1971. [Google Scholar] [CrossRef] [PubMed]
- Abe, T.; Hajishengallis, G. Optimization of the ligature-induced periodontitis model in mice. J. Immunol. Methods 2013, 394, 49–54. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Crawford, J.M.; Taubman, M.A.; Smith, D.J. The natural history of periodontal bone loss in germfree and gnotobiotic rats infected with periodontopathic microorganisms. J. Periodontal Res. 1978, 13, 316–325. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Treatment | Week 6 | Week 9 | Week 12a | Week 12b |
|---|---|---|---|---|
| N control | 5 | 5 * | 6 | 4 ** |
| N experimental | 5 | 5 * | 6 | 4 ** |
| Segment | Treatment | 6-Week Mean (mm) N = 5 Per Group | SD | 12-Week Mean (mm) N = 10 Per Group | SD |
|---|---|---|---|---|---|
| Maxilla/Buccal | Control | 0.404 | ±0.134 | 0.398 | ±0.151 |
| Cd-treated | 0.431 | ±0.127 | 0.441 | ±0.168 | |
| Maxilla/Palatal | Control | 0.531 | ±0.171 | 0.527 | ±0.180 |
| Cd-treated | 0.558 | ±0.216 | 0.645 * p < 0.0001, # p < 0.0001 | ±0.235 | |
| Mandible/Lingual | Control | 0.820 | ±0.273 | 0.785 | ±0.269 |
| Cd-treated | 0.803 | ±0.316 | 0.858 * p < 0.0001, # p = 0.053 | ±0.290 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Browar, A.W.; Koufos, E.B.; Wei, Y.; Leavitt, L.L.; Prozialeck, W.C.; Edwards, J.R. Cadmium Exposure Disrupts Periodontal Bone in Experimental Animals: Implications for Periodontal Disease in Humans. Toxics 2018, 6, 32. https://doi.org/10.3390/toxics6020032
Browar AW, Koufos EB, Wei Y, Leavitt LL, Prozialeck WC, Edwards JR. Cadmium Exposure Disrupts Periodontal Bone in Experimental Animals: Implications for Periodontal Disease in Humans. Toxics. 2018; 6(2):32. https://doi.org/10.3390/toxics6020032
Chicago/Turabian StyleBrowar, Andrew W., Emily B. Koufos, Yifan Wei, Landon L. Leavitt, Walter C. Prozialeck, and Joshua R. Edwards. 2018. "Cadmium Exposure Disrupts Periodontal Bone in Experimental Animals: Implications for Periodontal Disease in Humans" Toxics 6, no. 2: 32. https://doi.org/10.3390/toxics6020032