Oxidative DNA Damage and Carotid Intima Media Thickness as Predictors of Cardiovascular Disease in Prediabetic Subjects


Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Subjects
- (a)
- Fasting plasma glucose level 100–125 mg/dL (IFG) and
- (b)
- 2-h plasma glucose (after giving 75 gm of glucose) level 140 mg/dL to 199 mg/dL (IGT).
2.2. Anthropometric Measurements
2.3. Blood Pressure Measurements
2.4. Biochemical Measurements
2.5. Measurement of CIMT
2.6. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Hackworth, N.; Moore, S.N.; Hardie, E.; Critchley, C.; Buzwell, S.; Crafti, N.; Kyrios, M. A Risk Factor Profile for Pre-diabetes: Biochemical, Behavioural, Psychosocial and Cultural Factors. J. Appl. Psychol. 2007, 3, 14–26. [Google Scholar] [CrossRef]
- Tabák, A.G.; Herder, C.; Rathmann, W.; Brunner, E.J.; Kivimäki, M. Prediabetes: A high-risk state for developing diabetes. Lancet 2012, 379, 2279–2290. [Google Scholar] [CrossRef]
- DeFronzo, R.A.; Abdul-Ghani, M. Assessment and treatment of cardiovascular risk in prediabetes: Impaired glucose tolerance and impaired fasting glucose. Am. J. Cardiol. 2011, 108, 3B–24B. [Google Scholar] [CrossRef] [PubMed]
- Fuller, J.H.; Shipley, M.J.; Rose, G.; Jarrett, R.J.; Keen, H. Coronary-heart disease risk and impaired glucose tolerance. The Whitehall study. Lancet 1980, 1, 1373–1376. [Google Scholar] [CrossRef]
- Fuller, J.H.; Shipley, M.J.; Rose, G.; Jarrett, R.J.; Keen, H. Mortality from coronary heart disease and stroke in relation to degree of glycaemia: The Whitehall study. Br. Med. J. (Clin. Res. Ed.) 1983, 287, 867–870. [Google Scholar] [CrossRef]
- DECODE Study Group, the European Diabetes Epidemiology Group. Glucose tolerance and cardiovascular mortality: Comparison of fasting and 2-hour diagnostic criteria. Arch. Intern. Med. 2001, 161, 397–405. [Google Scholar]
- International Diabetes Federation. IDF Diabetes Atlas, 6th ed.; International Diabetes Federation: Brussels, Belgium, 2013. [Google Scholar]
- American Diabetes Association. Classification and diagnosis of diabetes. Sec. 2. In Standards of Medical Care in Diabetes—2017. Diabetes Care 2017, 40, S11–S24. [Google Scholar]
- Fardoun, R.Z. The use of vitamin E in type 2 diabetes mellitus. Clin. Exp. Hypertens. 2007, 29, 135–148. [Google Scholar] [CrossRef] [PubMed]
- El-Wassef, M.; Gamila, S.; El-Saeed, M.; El-Tokhy, S.E.; Raslan, H.M.; Tawfeek, S.; Siam, I.; Salem, S.I. Oxidative DNA damage in patients with type 2 diabetes mellitus. Diabetol. Croat. 2012, 41, 121–127. [Google Scholar]
- Yoon, J.H.; Kim, J.Y.; Park, J.K.; Ko, S.B. Oxidative Damage Markers Are Significantly Associated with the Carotid Artery Intima-Media Thickness after Controlling for Conventional Risk Factors of Atherosclerosis in Men. PLoS ONE 2015, 10, e0119731. [Google Scholar] [CrossRef] [PubMed]
- Evans, M.D.; Dizdaroglu, M.; Cooke, M.S. Oxidative DNA damage and disease: Induction, repair and significance. Mutat. Res. 2004, 567, 1–61. [Google Scholar] [CrossRef] [PubMed]
- Martinet, W.; Knaapen, M.W.; DeMeyer, G.R.; Herman, A.G.; Kockx, M.M. Elevated levels of oxidative DNA damage and DNA repair enzymes in human atherosclerotic plaques. Circulation 2002, 106, 927–932. [Google Scholar] [CrossRef] [PubMed]
- Al-Aubaidy, H.A.; Jelinek, H.F. Oxidative stress and triglycerides as predictors of subclinical atherosclerosis in prediabetes. Redox Rep. 2014, 19, 87–91. [Google Scholar] [CrossRef] [PubMed]
- Agarwal, A.K.; Gupta, P.K.; Singla, S.; Garg, U.; Prasad, A.; Yadav, R. Carotid intimomedial thickness in type 2 diabetic patients and its correlation with coronary risk factors. J. Assoc. Phys. India 2008, 56, 581–586. [Google Scholar]
- Kasliwal, R.R.; Bansal, M.; Desai, D.; Sharma, M. Carotid intima–media thickness: Current evidence, practices, and Indian experience. Indian J. Endocrinol. Metab. 2014, 18, 13–22. [Google Scholar] [CrossRef] [PubMed]
- Altin, C.; Sade, L.E.; Gezmis, E.; Ozen, N.; Duzceker, O.; Bozbas, H.; Eroglu, S.; Muderrisoglu, H. Assessment of subclinical atherosclerosis by carotid intima-media thickness and epicardial adipose tissue thickness in prediabetes. Angiology 2016, 67, 961–969. [Google Scholar] [CrossRef] [PubMed]
- Lv, Y.; Zhang, Y.; Shi, W.; Liu, J.; Li, Y.; Zhou, Z.; He, Q.; Wei, S.; Liu, J.; Quan, J. The association between endocan levels and subclinical atherosclerosis in patients with type 2 diabetes mellitus. Am. J. Med. Sci. 2017, 353, 433–438. [Google Scholar] [CrossRef] [PubMed]
- Gao, L.; Bai, L.; Shi, M.; Ni, J.; Lu, H.; Wu, Y.; Tu, J.; Ning, X.; Wang, J.; Li, Y. Association between carotid intima-media thickness and fasting blood glucose level: A population-based cross-sectional study among low-income adults in rural China. J. Diabetes Investig. 2017, 8, 788–797. [Google Scholar] [CrossRef] [PubMed]
- Huang, S.; Peng, W.; Zhao, W.; Sun, B.; Jiang, X. Higher plasma C-reactive protein and lower plasma adiponectin are associated with increased carotid artery intima-media thickness in patients with impaired glucose regulation. Asian Biomed. 2013, 7, 399–405. [Google Scholar]
- Mohieldein, A.H.; Hasan, M.; Al-Harbi, K.K.; Alodailah, S.S.; Azahrani, R.M.; Al-Mushawwah, S.A. Dyslipidemia and reduced total antioxidant status in young adult Saudis with prediabetes. Diabetes Metab. Syndr. 2015, 9, 287–291. [Google Scholar] [CrossRef] [PubMed]
- Agarwal, A.; Hegde, A.; Yadav, C.; Ahmad, A.; Manjrekar, P.A.; Srikantiah, R.M. Assessment of oxidative stress and inflammation inprediabetes—A hospital based cross-sectional study. Diabetes Metab. Syndr. 2016, 10, S123–S126. [Google Scholar] [CrossRef] [PubMed]
- Ferrannini, E. Definition of intervention points in prediabetes. Lancet Diabetes Endocrinol. 2014, 2, 667–675. [Google Scholar] [CrossRef]
- Pereira, C.S.; Molz, P.; Palazzo, R.P.; de Freitas, T.A.B.; Maluf, S.W.; Horta, J.A.; Pra, D.; Franke, S.I.R. DNA damage and cytotoxicity in adult subjects with prediabetes. Mutat. Res. Genet. Toxicol. Environ. Mutagen. 2013, 753, 76–81. [Google Scholar] [CrossRef] [PubMed]
- Al-Aubaidy, H.A.; Jelinek, H.F. 8-Hydroxy-2-deoxy-guanosine identifies oxidative DNA damage in a rural prediabetes cohort. Redox Rep. 2010, 15, 155–160. [Google Scholar] [CrossRef] [PubMed]
- Al-Aubaidy, H.A.; Jelinek, H.F. Oxidative DNA damage and obesity in type 2 diabetes mellitus. Eur. J. Endocrinol. 2011, 164, 899–904. [Google Scholar] [CrossRef] [PubMed]
- Sen, S.; Kar, M.; Roy, A.; Chakraborti, A.S. Effect of nonenzymatic glycation on functional and structural properties of hemoglobin. Biophys. Chem. 2005, 113, 289–298. [Google Scholar] [CrossRef] [PubMed]
- Mercer, J.; Mahmoudi, M.; Bennett, M. DNA damage, p53, apoptosis and vascular disease. Mutat. Res. 2007, 621, 75–86. [Google Scholar] [CrossRef] [PubMed]
- Clarke, M.C.; Littlewood, T.D.; Figg, N.; Maguire, J.J.; Davenport, A.P.; Goddard, M.; Bennett, M.R. Chronic apoptosis of vascular smooth muscle cells accelerates atherosclerosis and promotes calcification and medial degeneration. Circ. Res. 2008, 102, 1529–1538. [Google Scholar] [CrossRef] [PubMed]
- Clarke, M.C.; Figg, N.; Maguire, J.J.; Davenport, A.P.; Goddard, M.; Littlewood, T.D.; Bennett, M.R. Apoptosis of vascular smooth muscle cells induces features of plaque vulnerability in atherosclerosis. Nat. Med. 2006, 12, 1075–1080. [Google Scholar] [CrossRef] [PubMed]
- Ari, E.; Kaya, Y.; Demir, H.; Cebi, A.; Alp, H.H.; Bakan, E.; Odabasi, D.; Keskin, S. Oxidative DNA damage correlates with carotid artery atherosclerosis in hemodialysis patients. Hemodial. Int. 2011, 15, 453–459. [Google Scholar] [CrossRef] [PubMed]
- Hinokio, Y.; Suzuki, S.; Hirai, M.; Suzuki, C.; Suzuki, M.; Toyota, T. Urinary excretion of 8-oxo-7,8-dihydro-2-deoxyguanosine as a predictor of the development of diabetic nephropathy. Diabetologia 2002, 45, 877–882. [Google Scholar] [CrossRef] [PubMed]
- Hinokio, Y.; Suzuki, M.; Hirai, M.; Chiba, M.; Hirai, A.; Toyota, T. Oxidative DNA damage in diabetes mellitus: Its association with diabetic complications. Diabetologia 1999, 42, 995–998. [Google Scholar] [CrossRef] [PubMed]
- Grobbe, D.E.; Bots, M.L. Carotid artery intima-media thickness as an indicator of generalized atherosclerosis. J. Intern. Med. 1994, 236, 567–573. [Google Scholar] [CrossRef]
- Ebrahim, S.; Papacosta, O.; Whincup, P.; Wannamethee, G.; Walker, M.; Nicolaides, A.N.; Dhanjil, S.; Griffin, M.; Belcaro, G.; Rumley, A.; et al. Carotid plaque, Intima medial thickness, cardiovascular risk factors and prevalent cardiovascular disease in men and women: The British Regional Heart Study. Stroke 1999, 30, 841–850. [Google Scholar] [CrossRef] [PubMed]
- Sainani, G.S.; Khan, N.R. Carotid artery intima media thickness—A correlative study of diabetics with postprandial hyperglycemia versus controls with euglycemia. Med. Update 2012, 22, 298–303. [Google Scholar]
- McGarry, P.A.; McMahan, C.A.; Montenegro, M.R. General findings of the International atherosclerosis project. Lab. Investig. 1968, 18, 498–502. [Google Scholar]
- Wong, M.; Edelstein, J.; Wollman, J.; Bond, M.G. Ultrasonic pathological comparison of the human arterial wall: Verification of intima-medial thickness. Arterioscler. Thromb. 1993, 3, 482–486. [Google Scholar] [CrossRef]
- Bhinder, H.P.S.; Kamble, T.K.; Acharya, S. The study of carotid intima media thickness in prediabetes and its correlation with cardiovascular risk factors. J. Evid. Based Med. Healthc. 2017, 4, 3712–3715. [Google Scholar] [CrossRef] [PubMed]
- Karbek, B.; Cakal, E.; Cakir, E.; Bozkurt, N.; Unsal, I.; Sahin, M.; Delibaşi, T. Cardiovascular risk factors, carotid artery intima media thickness, and HSCRP levels in patients with impaired glucose metabolism. Minerva Endocrinol. 2013, 38, 297–304. [Google Scholar] [PubMed]
- Aydin, Y.; Berker, D.; Ustün, I.; Gül, K.; Erden, G.; Kutlucan, A.; Yilmaz Aydin, L.; Güler, S. Evaluation of carotid intima media thickness in impaired fasting glucose and impaired glucose tolerance. Minerva Endocrinol. 2011, 36, 171–179. [Google Scholar] [PubMed]
- Touboul, P.J.; Grobbee, D.E.; den Ruijter, H. Assessment of subclinical atherosclerosis by carotid intima media thickness: Technical issues. Eur. J. Prev. Cardiol. 2012, 19, 18–24. [Google Scholar] [CrossRef] [PubMed]
- Ceriello, A. Postprandial hyperglycemia and diabetes complications: Is it time to treat? Diabetes 2005, 54, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Gomez-Marcos, M.A.; Gomez-Sanchez, L.; Patino-Alonso, M.C.; Recio-Rodriguez, J.; Regalado, N.G.; Ramos, R.; Mart, R.; Agudo-Conde, C.; Rodriguez-Sanchez, E.; Maderuelo-Fernandez, J.A.; et al. Association between markers of glycemia and carotid intima-media thickness: The MARK study. BMC Cardiovasc. Disord. 2016, 16, 203. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | Control Subjects (n = 100) | Prediabetic Subjects (n = 100) |
|---|---|---|
| Age (years) | 38.92 ± 7.85 | 39.43 ± 8.90 NS |
| Sex (M/F) | 55/45 | 51/49 NS |
| BMI (kg/m2) | 23.48 ± 1.05 | 29.07 ± 1.71 ** |
| WC (cm) | 82.5 ± 2.84 | 92.02 ± 3.95 ** |
| HC (cm) | 94.85 ± 2.35 | 95.96 ± 2.66 * |
| WHR | 0.87 ± 0.03 | 0.96 ± 0.03 ** |
| SBP (mmHg) | 116.34 ± 2.94 | 127.50 ± 5.65 ** |
| DBP (mmHg) | 76.50 ± 2.71 | 81.36 ± 3.60 ** |
| Variables | Control Subjects (n = 100) | Prediabetic Subjects (n = 100) | |
|---|---|---|---|
| Blood glucose (mg/dL) | Fasting | 90.13 ± 3.84 | 115.88 ± 3.48 ** |
| 2-h PG | 124.72 ± 6.23 | 148.20 ± 3.66 ** | |
| HbA1c (%) | 4.81 ± 0.14 | 5.81 ± 0.12 ** | |
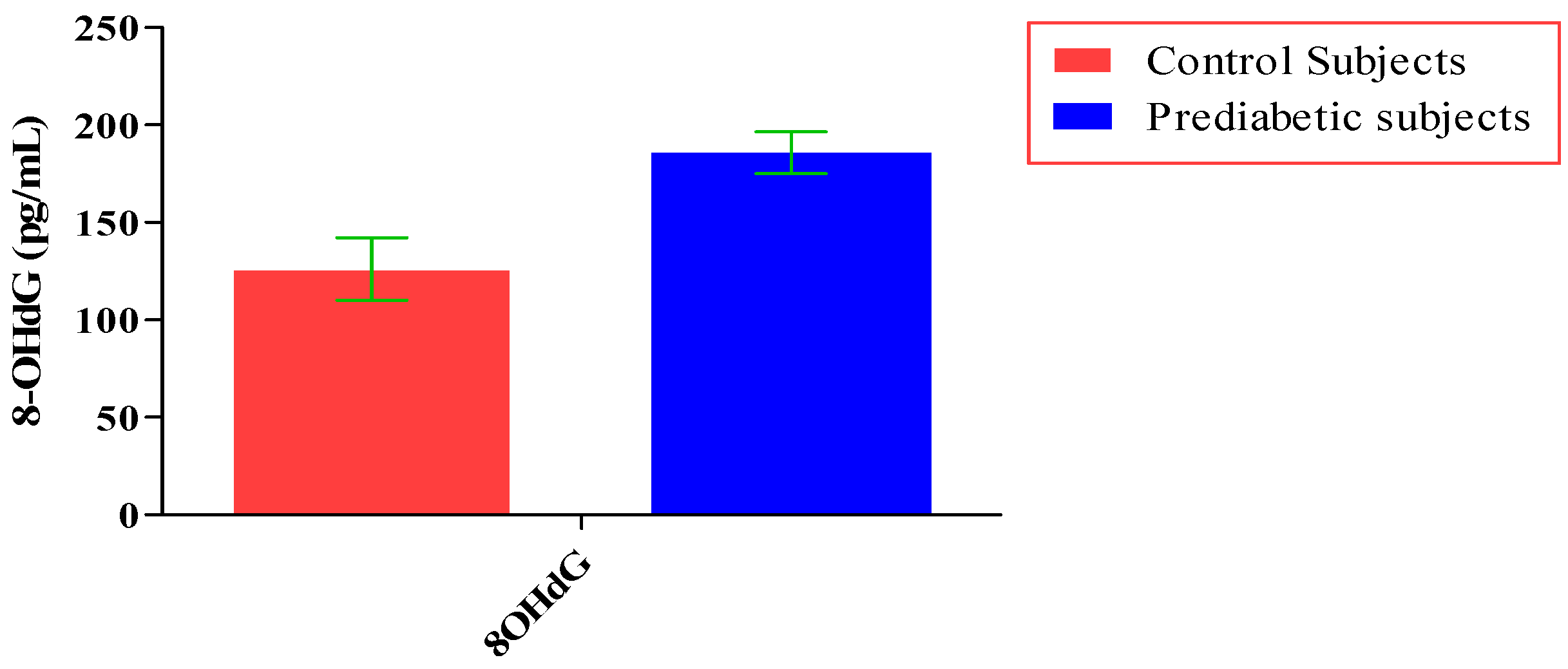
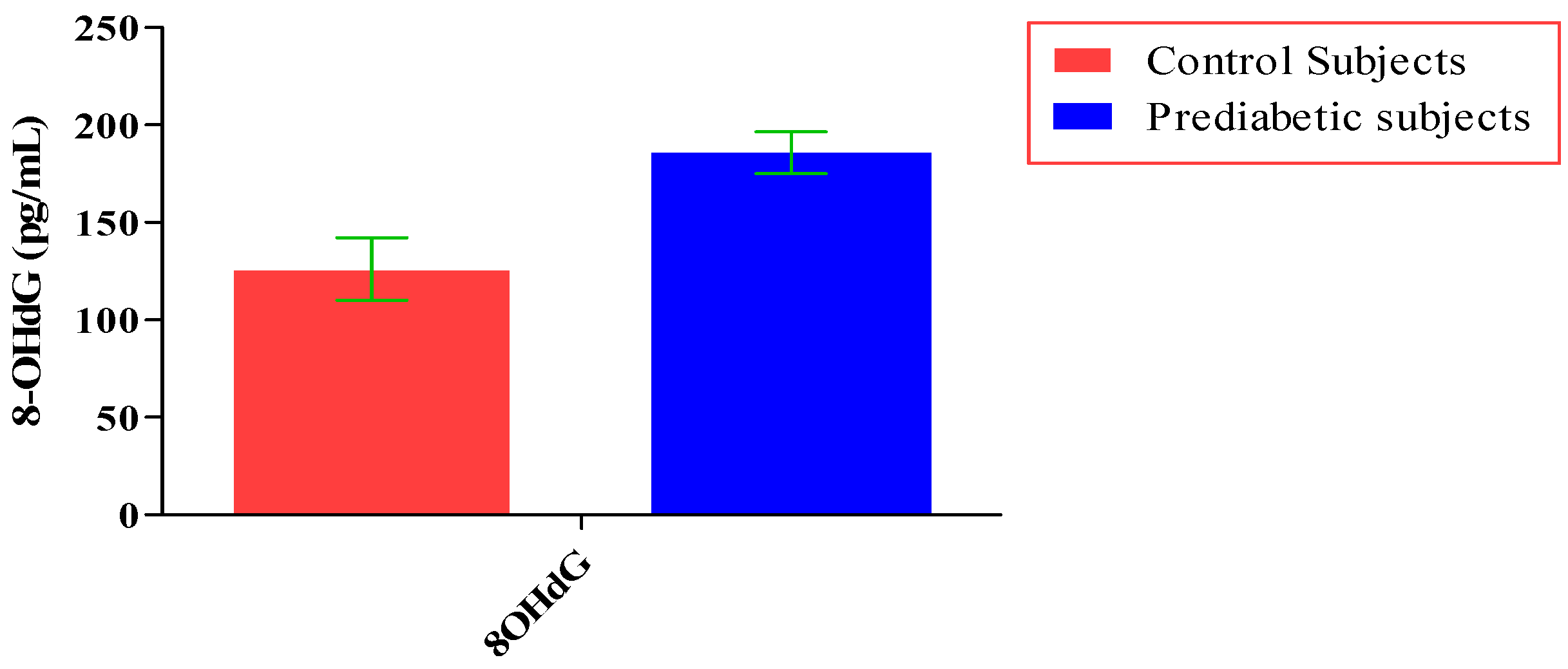
| 8-OHdG (pg/mL) | 126.13 ± 16.01 | 185.80 ± 10.72 ** | |
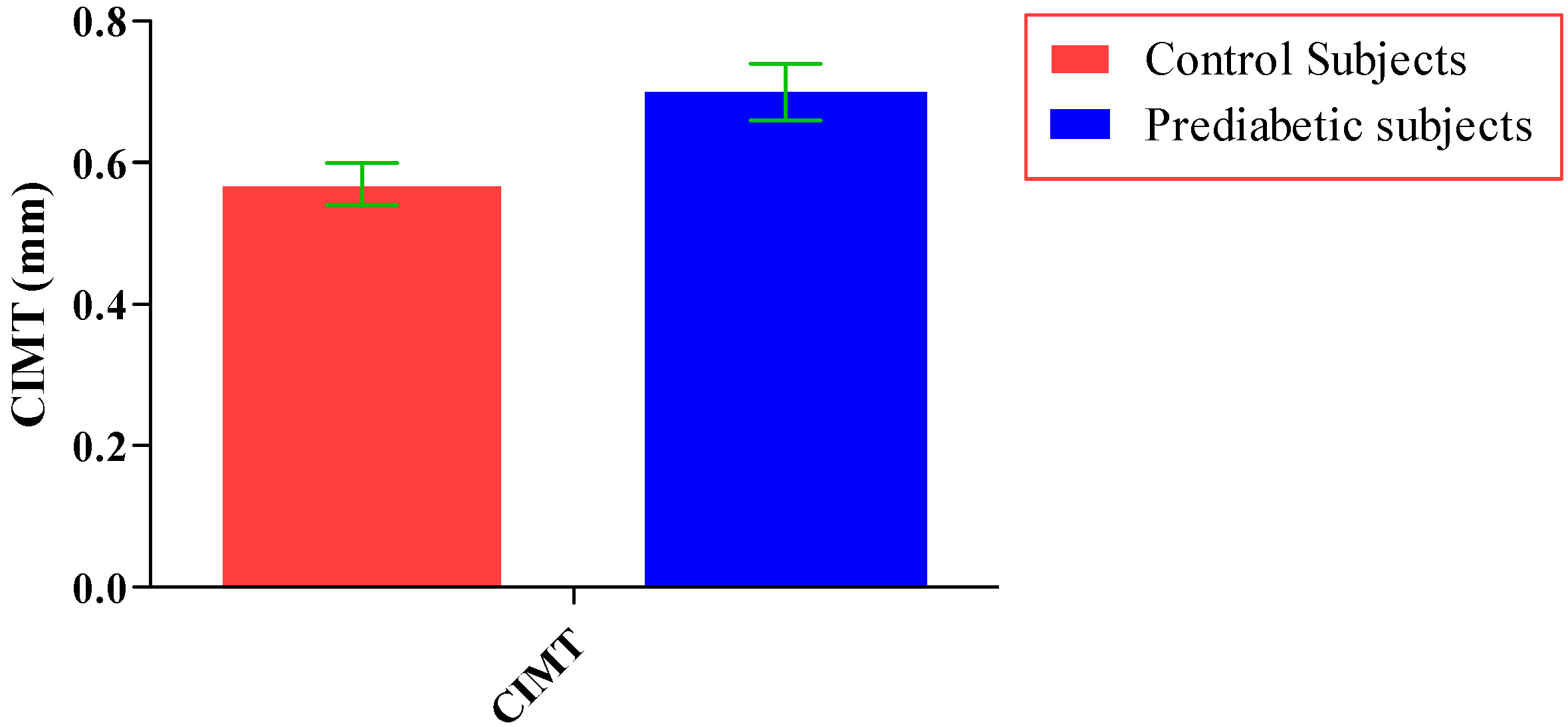
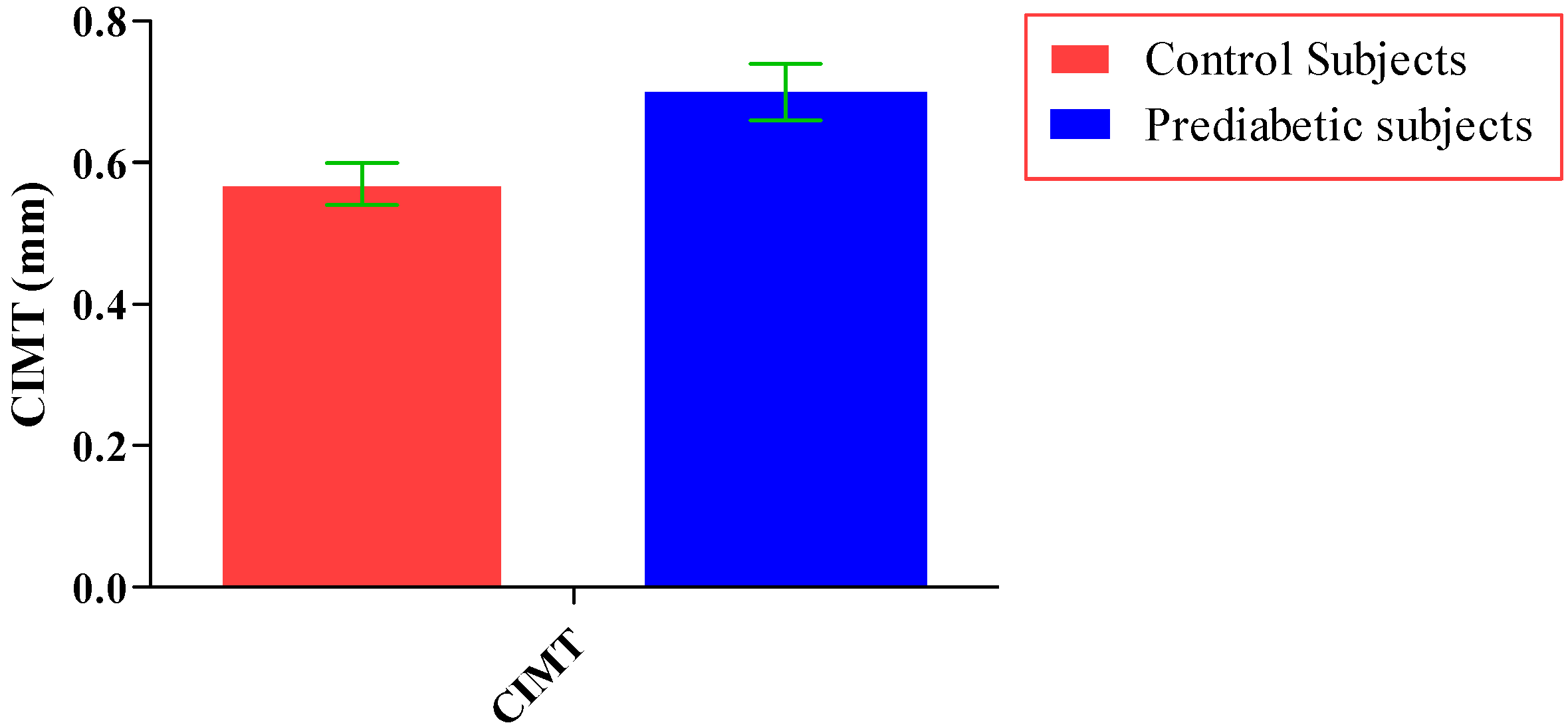
| CIMT (mm) | 0.57 ± 0.03 | 0.70 ± 0.04 ** | |
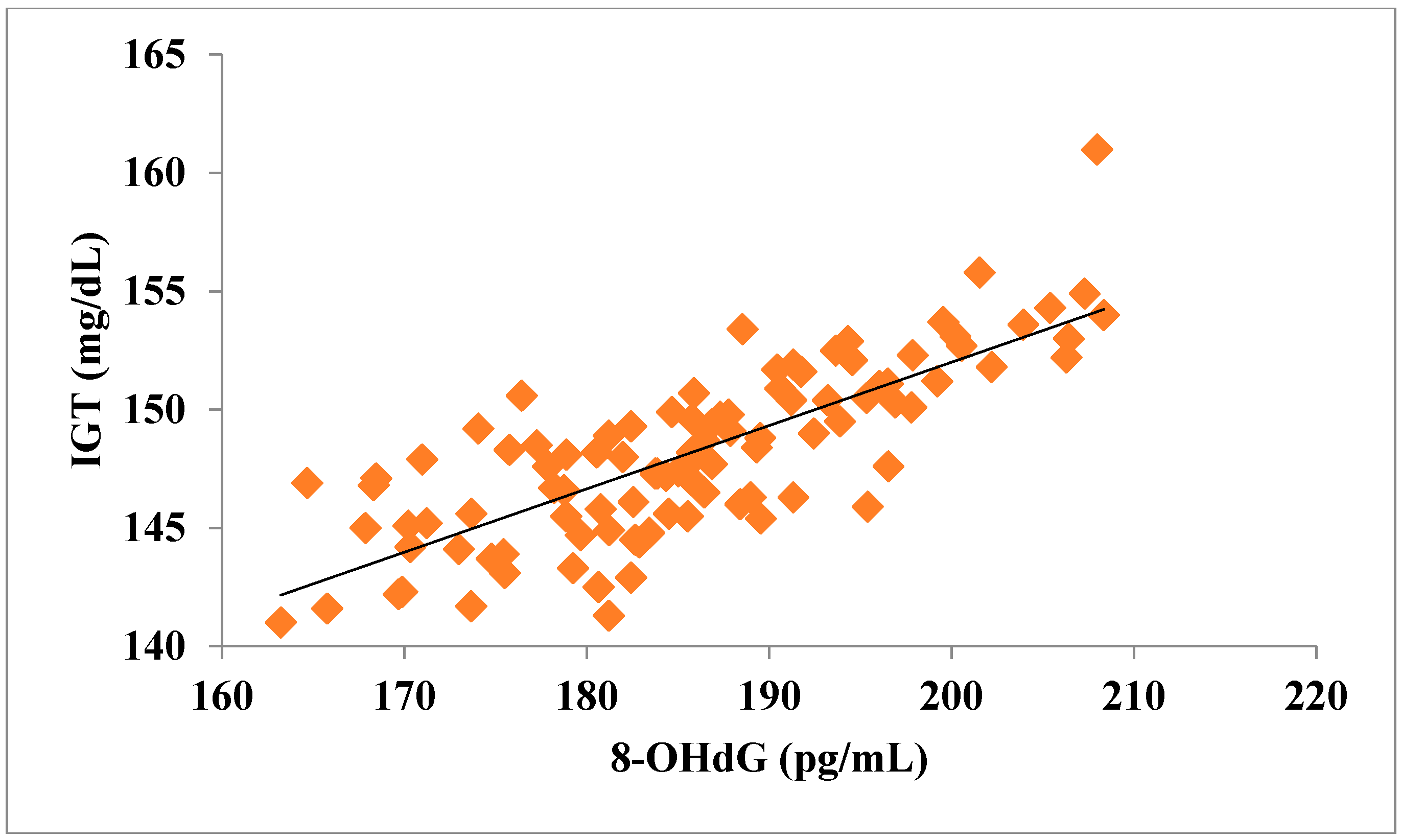
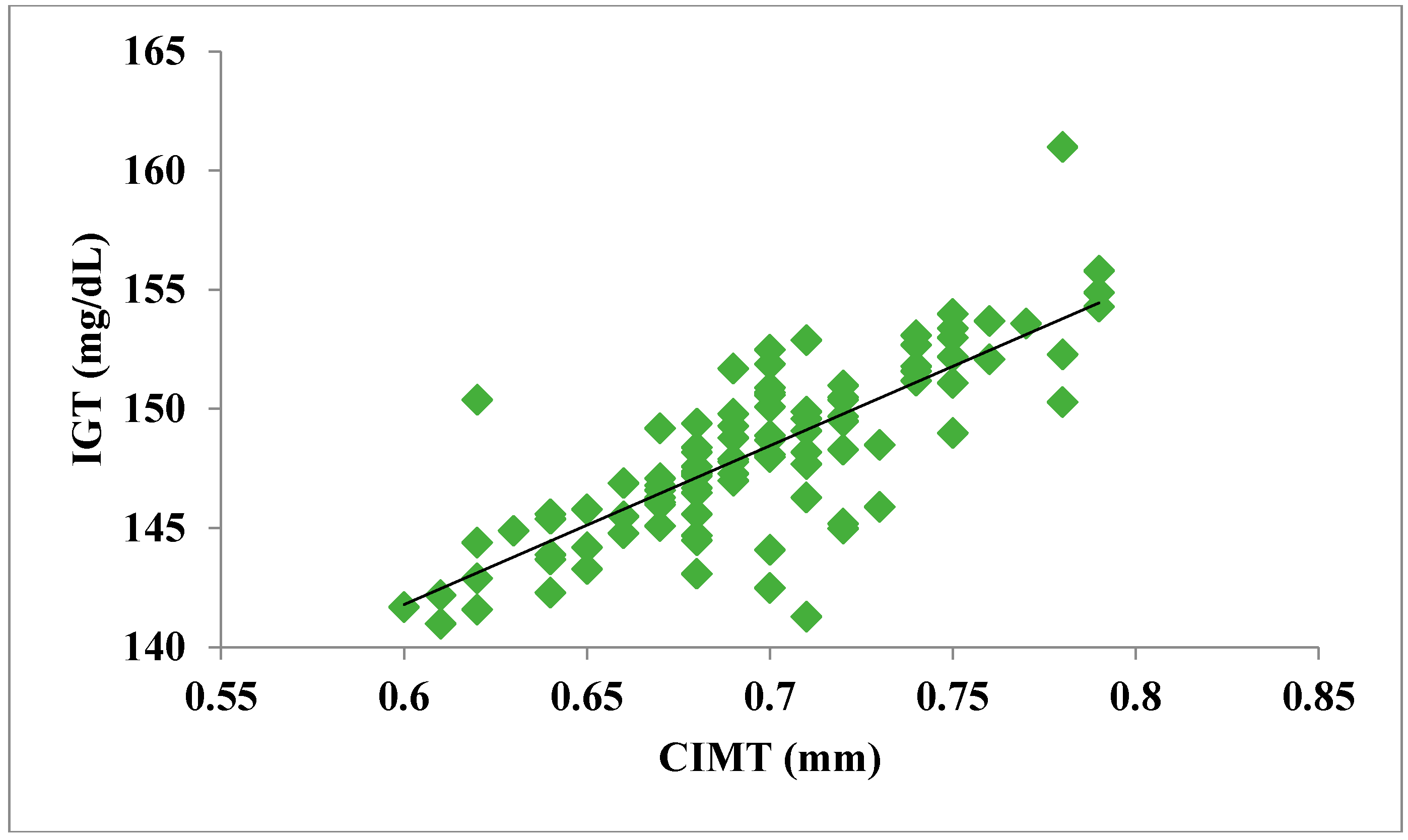
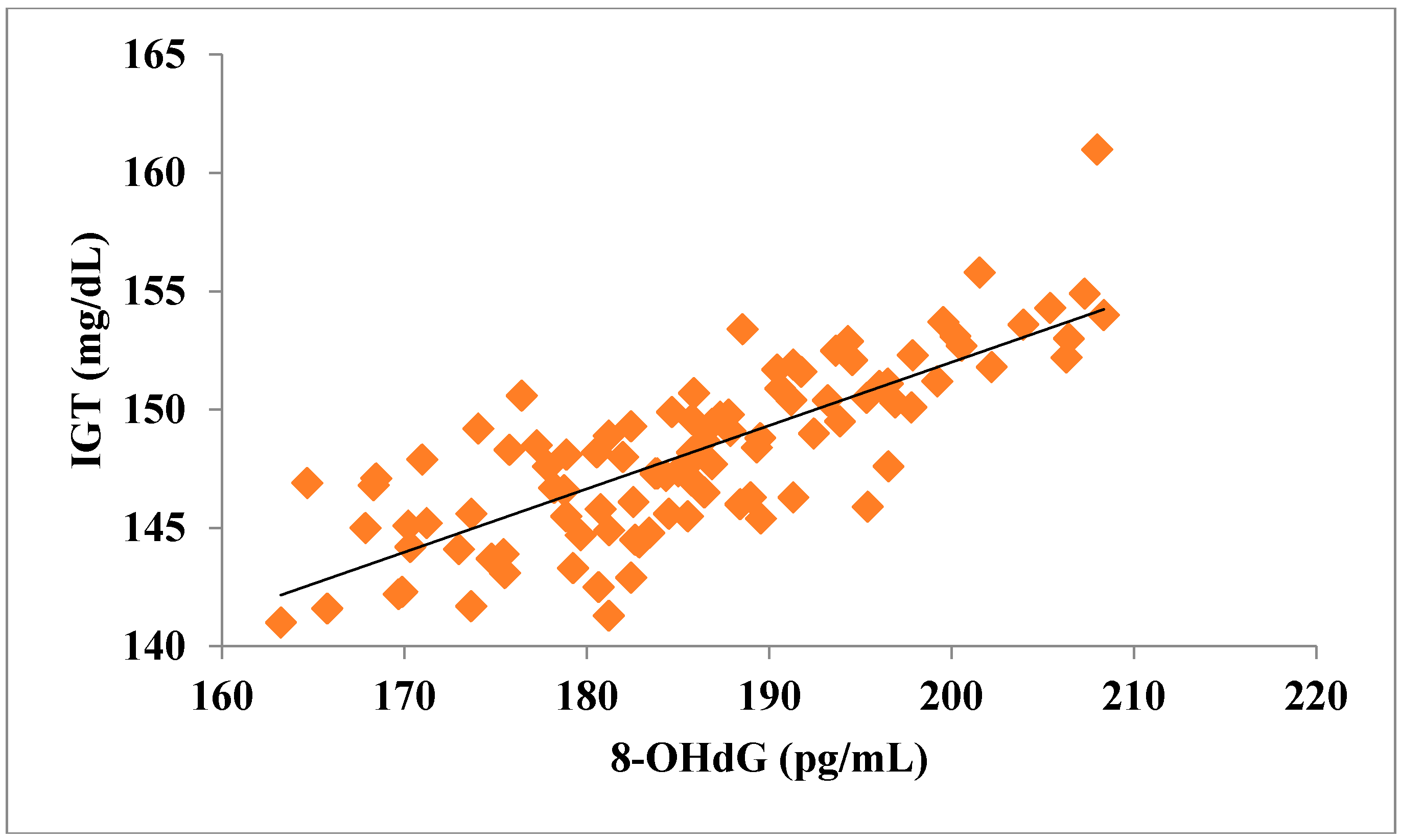
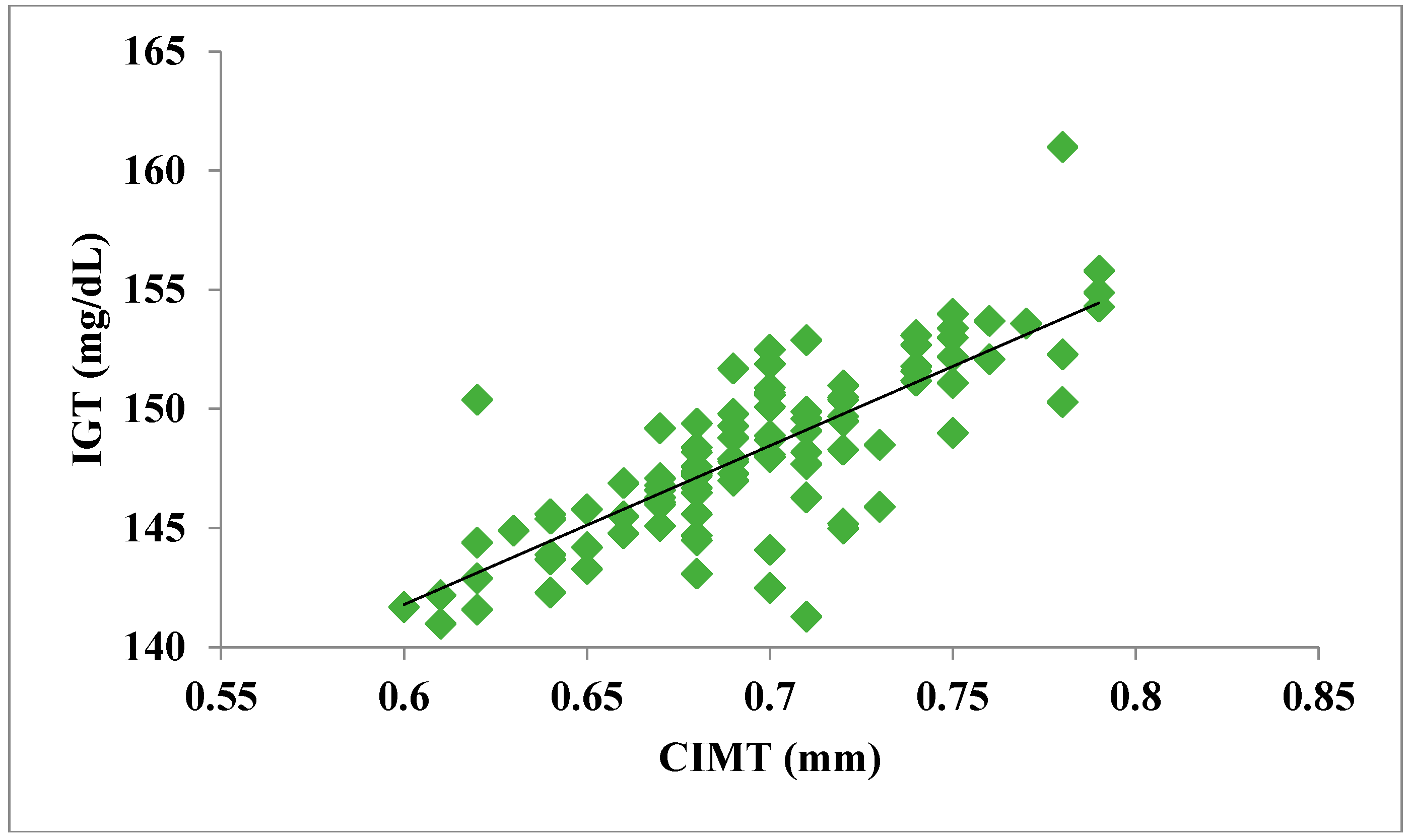
| Parameters | IGT | 8-OHdG | CIMT |
|---|---|---|---|
| IGT | 1 | 0.783 ** | 0.787 ** |
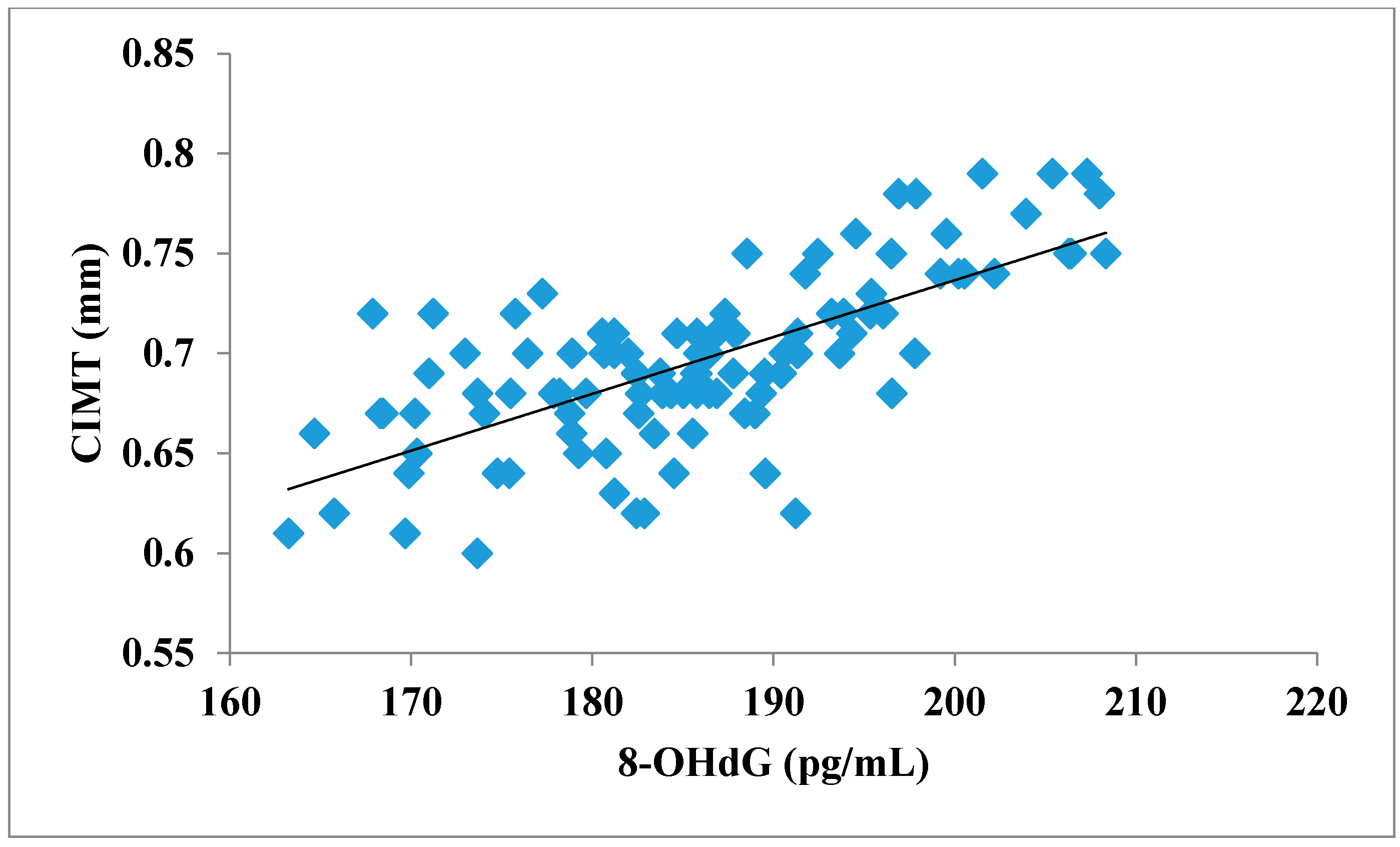
| 8-OHdG | 0.783 ** | 1 | 0.704 ** |
| CIMT | 0.787 ** | 0.704 ** | 1 |
| Variables | 8-OHdG | CIMT |
|---|---|---|
| Age | 0.486 ** | 0.469 ** |
| BMI | 0.450 ** | 0.344 ** |
| WHR | 0.368 ** | 0.241 * |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mahat, R.K.; Singh, N.; Gupta, A.; Rathore, V. Oxidative DNA Damage and Carotid Intima Media Thickness as Predictors of Cardiovascular Disease in Prediabetic Subjects. J. Cardiovasc. Dev. Dis. 2018, 5, 15. https://doi.org/10.3390/jcdd5010015
Mahat RK, Singh N, Gupta A, Rathore V. Oxidative DNA Damage and Carotid Intima Media Thickness as Predictors of Cardiovascular Disease in Prediabetic Subjects. Journal of Cardiovascular Development and Disease. 2018; 5(1):15. https://doi.org/10.3390/jcdd5010015
Chicago/Turabian StyleMahat, Roshan Kumar, Neelima Singh, Akshara Gupta, and Vedika Rathore. 2018. "Oxidative DNA Damage and Carotid Intima Media Thickness as Predictors of Cardiovascular Disease in Prediabetic Subjects" Journal of Cardiovascular Development and Disease 5, no. 1: 15. https://doi.org/10.3390/jcdd5010015