Trends in Deaths from Rheumatic Heart Disease in the Eastern Mediterranean Region: Burden and Challenges

Abstract
:1. Introduction
2. Methods
- High income countries (HIC): Bahrain, Kuwait, Qatar, Saudi Arabia, UAE, and Oman.
- Middle income countries (MIC): Egypt, Jordan, Iran, Iraq, Lebanon, Libya, Morocco, Syria, Tunisia, and Palestine.
- Low income countries (LIC): Afghanistan, Djibouti, Pakistan, Somalia, Sudan, and Yemen.
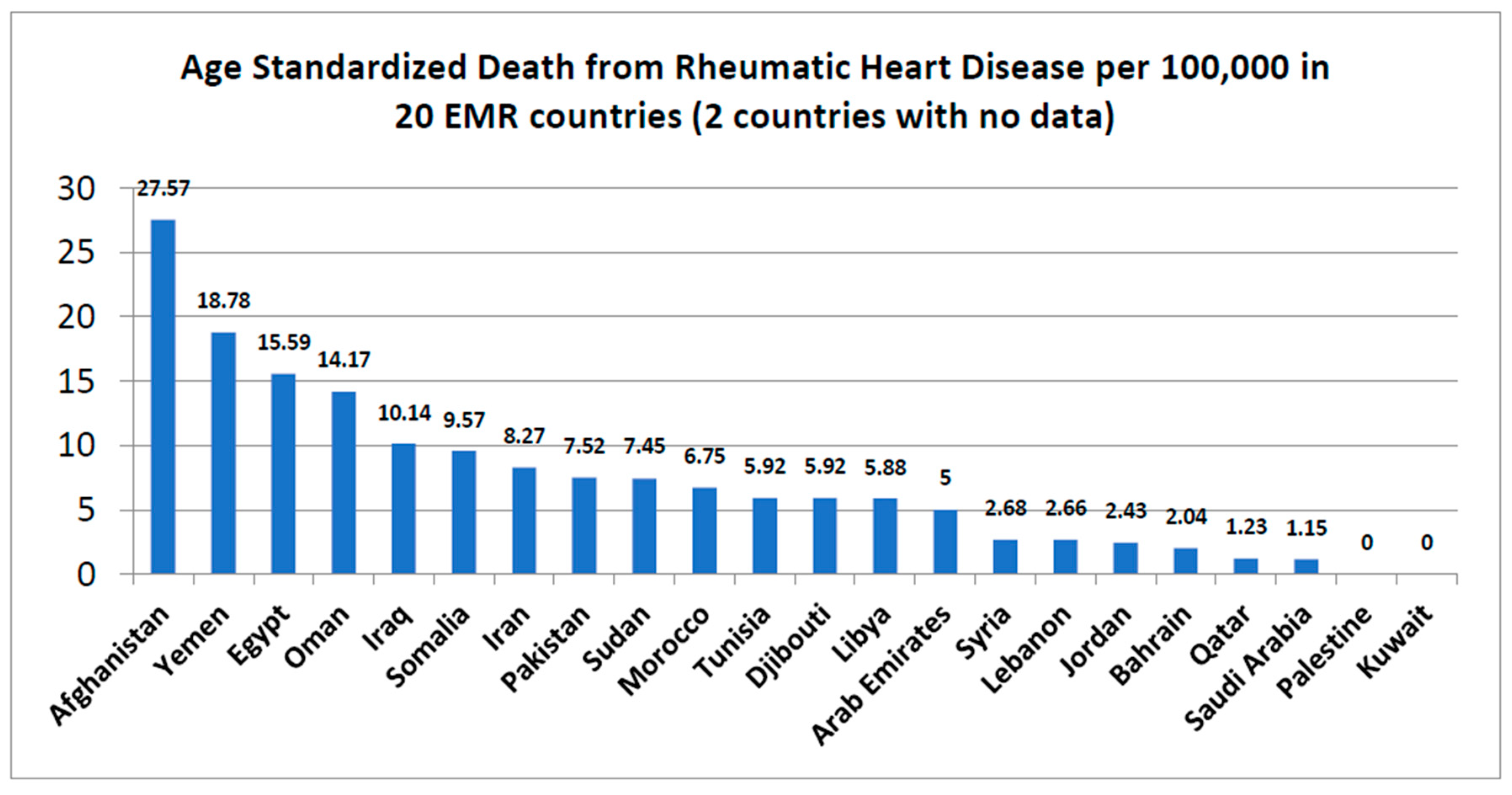
3. Results
4. Discussion
5. Conclusions
Author Contributions
Conflicts of Interest
References and Notes
- World Health Organization. Rheumatic Diseases: First Report of the Expert Committee; WHO Technical Report Series No. 78; World Health Organization: Geneva, Switzerland, 1954. [Google Scholar]
- RHD Australia (ARF/RHD Writing Group); National Heart Foundation of Australia and the Cardiac Society of Australia and New Zealand. Australian Guideline for Prevention, Diagnosis and Management of Acute Rheumatic Fever and Rheumatic Heart Disease, 2nd ed.; National Heart Foundation of Australia: Melbourne, Australia, 2012; ISBN 978-0-9587722-9-7.
- Heart Foundation of New Zealand. Group A Streptococcal Sore Throat Management Guideline; Heart Foundation of New Zealand: Auckland, New Zealand, 2014.
- Abdin, Z.; Eissa, A.M. Rheumatic fever and rheumatic heart disease in children below the age of 5 years in the tropics. Ann. Rheum. Dis. 1965, 24, 389. [Google Scholar] [CrossRef] [PubMed]
- Toor, D.; Sharma, N. T cell subsets: An integral component in pathogenesis of rheumatic heart disease. Immunol. Res. 2018, 66, 18–30. [Google Scholar] [CrossRef] [PubMed]
- Abul-Fadl, A.M.A.; Mourad, M.K. A systemic review of screening methods for rheumatic heart disease in Egypt: Potential role of echocardiography for community based surveys. In Proceedings of the Euro Eco Imaging 2014 18th Annual Meeting of the European Association of Cardiovascular Imaging, Vienna, Austria, 3–6 December 2014. [Google Scholar]
- Mokdad, A.H. Burden of cardiovascular disease in the Eastern Mediterranean region 1990–2015: Findings from the Global Burden of Disease 2015 study. Int. J. Public Health 2017, 1–13. [Google Scholar] [CrossRef]
- Nordet, P.; Lopez, R.; Dueñas, A.; Sarmiento, L. Prevention and control of rheumatic fever and rheumatic heart disease: The Cuban experience (1986–1996–2002). Cardiovasc. J. Afr. 2008, 19, 135–140. [Google Scholar] [PubMed]
- Watkin, D.; Johnson, C.A.; Colquhoun, S.M.; Karthikeyan, G.; Beaton, A.; Bukhman, G.; Forouzanfar, M.H.; Longenecker, C.; Mayosi, B.M.; Mensah, G.A.; et al. Global, Regional, and National Burden of Rheumatic Heart Disease, 1990–2015. N. Engl. J. Med. 2017, 377, 713–722. [Google Scholar] [CrossRef] [PubMed]
- Marijon, E.; Celermajer, D.S.; Jouven, X. Rheumatic heart disease-an iceberg in tropical waters. N. Engl. J. Med. 2017, 377, 780–781. [Google Scholar] [CrossRef] [PubMed]
- Marijon, E.; Ou, P.; Celermajer, D.S.; Mocumbi, A.O.; Jani, D.; Paquet, C.; Jacob, S.; Sidi, D.; Jouven, X. Prevalence of rheumatic heart disease detected by echocardiographic screening. N. Engl. J. Med. 2007, 357, 470–476. [Google Scholar] [CrossRef] [PubMed]
- Nascimento, B.R.; Beaton, A.Z.; Nunes, M.C.; Diamantino, A.C.; Carmo, G.A.; Oliveira, K.K.; Oliveira, C.M.; Meira, Z.M.; Castilho, S.R.; Lopes, E.; et al. Echocardiographic prevalence of rheumatic heart disease in Brazilian schoolchildren: Data from the PROVAR study. Int. J. Cardiol. 2016, 219, 439–445. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Global Action Plan for the Prevention and Control of Noncommunicable Diseases 2013–2020; World Health Organization: Geneva, Switzerland, 2013. [Google Scholar]
- Remenyi, B.; Carapetis, J.; Wyber, R.; Taubert, K.; Mayosi, B.M. Position statement of the World Heart Federation on the prevention and control of rheumatic heart disease. Nat. Rev. Cardiol. 2013, 10, 284–292. [Google Scholar] [CrossRef] [PubMed]
- Carapetis, J.R.; Steer, A.C.; Mulholland, E.K.; Weber, M. The global burden of group A streptococcal diseases. Lancet Infect. Dis. 2005, 5, 685–694. [Google Scholar] [CrossRef]
- Dougherty, S.; Beaton, A.; Nascimento, B.R.; Zühlke, L.J.; Khorsandi, M.; Wilson, N. Prevention and control of rheumatic heart disease: Overcoming core challenges in resource-poor environments. Ann. Pediatr. Cardiol. 2018, 11, 68–78. [Google Scholar] [CrossRef] [PubMed]
- Sohrabi, B.; Ranjbar, A. Correspondence to “Global Burden of Rheumatic Heart Disease”.
- Jain, Y.; Juneja, R.; Patil, S. Correspondence to “Global Burden of Rheumatic Heart Disease”.
- Dickinson, J.A.; Johnston, I. Correspondence to “Global Burden of Rheumatic Heart Disease”.
- Rossi, G.; Lee, V.S.W. Call for preventive care for rheumatic heart disease in refugee children. BMJ 2016, 353, i2312. [Google Scholar] [CrossRef] [PubMed]
- De Maio, G.; Lupiz, M.; Condemi, F.; Pagano, A.; Al-Rousan, A.; Rossi, G. Screening for Rheumatic Heart Disease in Refugee Children in Europe—MSF Leads, Will Others Please Follow? MSF Paediatric Days: Stockholm, Sweden, 2016. [Google Scholar]
- Belton, S.; Kruske, S.; Pulver, L.J.; Sherwood, J.; Tune, K.; Carapetis, J.; Vaughan, G.; Peek, M.; McLintock, C.; Sullivan, E. Rheumatic heart disease in pregnancy: How can health services adapt to the needs of Indigenous women? A qualitative study. Aust. N. Z. J. Obstet. Gynaecol. 2017, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Saleh, S.; Alameddine, M.; Mourad, Y.; Natafg, N. Quality of care in primary health care settings in the Eastern Mediterranean region: A systematic review of the literature. Int. J. Qual. Health Care 2015, 27, 79–88. [Google Scholar] [CrossRef] [PubMed]
- Ralph, A.; Fittock, M.; Schultz, R.; Thompson, D.; Dowden, M.; Clemens, T.; Parnaby, M.G.; Clark, M.; McDonald, M.I.; Edwards, K.N.; et al. Improvement in rheumatic fever and rheumatic heart disease management and prevention using a health-centre based continuous quality improvement approach. BMC Health Serv. Res. 2013, 13, 525. [Google Scholar] [CrossRef] [PubMed]
- Moloi, A.H.; Watkins, D.; Engel, M.E.; Mall, S.; Zühlke, L. Epidemiology, health systems and stakeholders in rheumatic heart disease in Africa: A systematic review protocol. BMJ Open 2016, 6, e011266. [Google Scholar] [CrossRef] [PubMed]
- El-Jardali, F.; Saleh, S.; Khodor, R.; Abu Al Rub, R.; Arfa, C.; Ben Romdhane, H.; Hamadeh, R.R. An institutional approach to support the conduct and use of health policy and systems research: The Nodal Institute in the Eastern Mediterranean Region. Health Res. Policy Syst. 2015, 13, 1229–1238. [Google Scholar] [CrossRef] [PubMed]
- Bergmark, R.; Bergmark, B.; Blander, J.; Fataki, M.; Janabi, M. Burden of disease and barriers to the diagnosis and treatment of group a beta-hemolytic streptococcal pharyngitis for the prevention of rheumatic heart disease in Dar Es Salaam, Tanzania. Pediatr. Infect. Dis. J. 2010, 29, 1135–1137. [Google Scholar] [CrossRef] [PubMed]
- Zühlke, L.; Engel, M.E.; Karthikeyan, G.; Rangarajan, S.; Mackie, P.; Cupido, B.; Mauff, K.; Islam, S.; Joachim, A.; Daniels, R.; et al. Characteristics, complications, and gaps in evidence-based interventions in rheumatic heart disease: The Global Rheumatic Heart Disease Registry (the REMEDY study). Eur. Heart J. 2015, 36, 1115–1122. [Google Scholar] [CrossRef] [PubMed]
- McDonald, M.; Brown, A.; Noonan, S.; Carapetis, J.R. Preventing recurrent rheumatic fever: The role of register based programmes. Heart 2005, 91, 1131–1133. [Google Scholar] [CrossRef] [PubMed]
- Wyber, R.; Zühlke, L.; Carapetis, J. The case for global investment in rheumatic heart-disease control. Bull. World Health Organ. 2014, 92, 768–770. [Google Scholar] [CrossRef] [PubMed]
- Carapetis, J. Rheumatic heart disease in developing countries. N. Engl. J. Med. 2007, 357, 439–441. [Google Scholar] [CrossRef] [PubMed]
- Krahwinkel, W.; Schuler, E.; Liebetrau, M.; Meier-Hellmann, A.; Zacher, J.; Kuhlen, R. For the Helios Medical Board and Helios Working Group on Peer Reviewing. The effect of peer review on mortality rates. Int. J. Qual. Health Care 2016, 28, 594–600. [Google Scholar] [CrossRef] [PubMed]
- Katzenellenbogen, J.M.; Ralph, A.P.; Wyber, R.; Carapetis, J.R. Rheumatic heart disease: Infectious disease origin, chronic care approach. BMC Health Serv. Res. 2017, 17, 793. [Google Scholar] [CrossRef] [PubMed]
- Kronfol, N.M. Delivery of health services in Arab countries: A review. East. Mediterr. Health J. 2012, 18, 1229–1238. [Google Scholar] [CrossRef] [PubMed]
- Nkgudi, B.; Robertson, K.A.; Volmink, J.; Mayosi, B.M. Notification of rheumatic fever in South Africa–Evidence for underreporting by health care professionals and administrators. S. Afr. Med. J. 2006, 96, 206–208. [Google Scholar] [PubMed]
- Chamberlain-Salaun, J.; Mills, J.; Kevat, P.M.; Rémond, M.G.W.; Maguire, G.P. Sharing success–understanding barriers and enablers to secondary prophylaxis delivery for rheumatic fever and rheumatic heart disease. BMC Cardiovasc. Disord. 2016, 16, 166. [Google Scholar] [CrossRef] [PubMed]
- Wagstaff, A. Poverty and health sector inequalities. Bull. World Health Organ. 2002, 80, 97–105. [Google Scholar] [PubMed]
- Peters, D.H.; Garg, A.; Bloom, G.; Walker, D.G.; Brieger, W.R.; Rahman, M.H. Poverty and access to health care in developing countries. Ann. N. Y Acad. Sci. 2008, 1136, 161–171. [Google Scholar] [CrossRef] [PubMed]
- Zühlke, L.; Karthikeyan, G.; Engel, M.E.; Rangarajan, S.; Mackie, P.; Cupido-Katya Mauff, B.; Islam, S.; Daniels, R.; Francis, V.; Ogendo, S.; et al. Clinical outcomes in 3343 children and adults with rheumatic heart disease from 14 low- and middle-income countries: Two-year follow-up of the global rheumatic heart disease registry (the REMEDY study). Circulation 2016, 134, 1456–1466. [Google Scholar] [CrossRef] [PubMed]
- Carapetis, J.R.; Hardy, M.; Fakakovikaetau, T.; Taib, R.; Wilkinson, L.; Penny, D.J.; Steer, A.C. Evaluation of a screening protocol using auscultation and portable echocardiography to detect asymptomatic rheumatic heart disease in Tongan school children. Nat. Clin. Pract. Cardiovasc. Med. 2008, 5, 411–417. [Google Scholar] [CrossRef] [PubMed]
- Guilfoyle, J. Out of sight, out of mind. Can. Fam. Physician 2015, 61, 833–834. [Google Scholar] [PubMed]
- Johnston, I.; Gittens, C.; Dickinson, J.A. Pharyngitis complications in North America in the 21st century. In Proceedings of the Third Preventing Overdiagnosis Conference, Bethesda, MD, USA, 1–3 September 2015. [Google Scholar]
- World Health Organization (WHO). Rheumatic Heart Disease; Report by Secret EXECUTIVE BOARD EB141/4 141st Session 1 May 2017 Provisional Agenda Item 6.2; World Health Organization: Geneva, Switzerland, 2017. [Google Scholar]
- World Health Organization (WHO). Rheumatic Fever and Rheumatic Heart Disease; Seventy-First World Health Assembly A71/25. Resolution adopted on 25 May 2018 for provisional agenda 12.8 by Director General on 12 April 2018; World Health Organization: Geneva, Switzerland, 2017. [Google Scholar]
- Murray, C.J.; Vos, T.; Lozano, R.; Naghavi, M.; Flaxman, A.D.; Michaud, C.; Ezzati, M.; Shibuya, K.; Salomon, J.A.; Abdalla, S.; et al. Disability-adjusted life years (DALYs) for 291 diseases and injuries in 21 regions, 1990-2010: A systematic analysis for the Global Burden of Disease Study 2010. Lancet 2012, 380, 2197–2223. [Google Scholar] [CrossRef]
- Yusuf, S.; Wood, D.; Ralston, J.; Reddy, K.S. The World Heart Federation’s vision for worldwide cardiovascular disease prevention. Lancet 2015, 386, 399–402. [Google Scholar] [CrossRef]
- Palafox, B.; Mocumbi, A.O.; Kumar, R.K.; Ali, S.K.M.; Kennedy, E.; Haileamlak, A.; Watkins, D.; Petricca, K.; Wyber, R.; Timeon, P.; et al. The WHF Roadmap for Reducing CV Morbidity and Mortality through Prevention and Control of RHD. Glob. Heart. 2017, 12, 47–62. [Google Scholar] [CrossRef] [PubMed]
- Watkins, D.; Zuhlke, L.; Engel, M.; Daniels, R.; Francis, V.; Shaboodien, G.; Kango, M.; Abul-Fadl, A.; Adeoye, A.; Ali, S.; et al. Seven key actions to eradicate rheumatic heart disease in Africa: The Addis Ababa communiqué. Cardiovasc. J. Afr. 2016, 3, 184–187. [Google Scholar] [CrossRef] [PubMed]
- Sorour, K. Rheumatic heart disease in Egypt: Gloomy past and promising future. Egypt. Heart J. 2014, 66, 139–142. [Google Scholar] [CrossRef]
- Sriha Belguith, A.; Koubaa Abdelkafi, A.; El Mhamdi, S.; Ben Fredj, M.; Abroug, H.; Ben Salah, A.; Bouanene, I.; Hassine, F.; Amara, A.; Bhiri, S.; et al. Rheumatic heart disease in a developing country: Incidence and trend (Monastir; Tunisia: 2000–2013). Int. J. Cardiol. 2017, 228, 628–632. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Indicators | Total (20) | HIC (5) | MIC (9) | LIC (6) |
|---|---|---|---|---|
| Age Standardized Death Rate (ASDR) from RHD (mean ± SDs) | 7.31 ± 6.76 | 3.93 ± 5.29 | 6.0 ± 4.54 | 12.80 ± 8.58 |
| Correlative studies of ASDR with selected socio-demographic indicators | ||||
| Literacy (total) | r-0.58 * | r-0.877 * | r-0.877 * | r-0.084 |
| Literacy (in females) | r-0.51 * | r-0.836 * | r-0.537 * | r-0.328 |
| Total fertility rate (TFR) | r0.57 | r0.89 * | r0.08 | r0.27 |
| Deaths from household & ambient air pollution (MAAP) | r0.6 * | r-0.11 | r0.81 * | r0.31 |
| Anaemia during Pregnancy | r0.74 * | r0.832 * | r0.83 * | r0.52 * |
| Maternal mortality ratio (MMR) | r0.49 | r0.5 * | r-0.07 | r0.19 |
| Low birth weight (LBW) | r0.46 | r0.22 | r-0.05 | r0.07 |
| Correlative studies of ASDR with selected health service indicators | ||||
| Physician per 1000 population | r-0.43 | r-0.84 * | r-0.61 * | r0.66 * |
| Nursing and midwifery per 1000 population | r-0.48 * | r-0.76 * | r-0.15 | r0.13 |
| Per capita total expenditure on health (US$ exchange rate) | r-0.49 * | r-0.69 * | r-0.28 | r-0.29 |
| Out of pocket expenditure as a percentage of total health expenditure | r0.53 * | r-0.42 | r0.46 | r0.40 |
| Primary Health Care facilities per 10,000 population | r-0.28 | r0.798 * | r-0.39 | r-0.32 |
| Hospital beds per 10,000 population | r-0.10 | r-0.4 | r-0.12 | r-0.4 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Abul-Fadl, A.M.A.M.; Mourad, M.M.; Ghamrawy, A.; Sarhan, A.E. Trends in Deaths from Rheumatic Heart Disease in the Eastern Mediterranean Region: Burden and Challenges. J. Cardiovasc. Dev. Dis. 2018, 5, 32. https://doi.org/10.3390/jcdd5020032
Abul-Fadl AMAM, Mourad MM, Ghamrawy A, Sarhan AE. Trends in Deaths from Rheumatic Heart Disease in the Eastern Mediterranean Region: Burden and Challenges. Journal of Cardiovascular Development and Disease. 2018; 5(2):32. https://doi.org/10.3390/jcdd5020032
Chicago/Turabian StyleAbul-Fadl, Azza M. A. M., Maha M. Mourad, Alaa Ghamrawy, and Ayah Ebada Sarhan. 2018. "Trends in Deaths from Rheumatic Heart Disease in the Eastern Mediterranean Region: Burden and Challenges" Journal of Cardiovascular Development and Disease 5, no. 2: 32. https://doi.org/10.3390/jcdd5020032