An Impact Mapping Method to Generate Robust Qualitative Evaluation of Community-Based Research Programs for Youth and Adults

 , , ,
, , ,
Abstract
:1. Introduction
2. Methodology
2.1. Pre- Ripple Effect Mapping Session
2.1.1. Training
2.1.2. Participants
2.1.3. Required materials
2.2. Ripple Effect Mapping Session
2.2.1. Setting and Introduction
2.2.2. Icebreaker and Appreciative Inquiry Activities
2.2.3. Introduce REM Concepts
“This session will give us a better understanding of your experience with the [insert research program here] and how it impacted you individually and as a group and/or community. This map will be a tool for us to understand the effects this program has had on your families and in the community through a ‘rippling effect.’ This ‘ripple effect’ is like a pebble being dropped into a pond; one small pebble can make a large impact of ripples throughout a pond. Similarly, a singular program can make small and large impacts within a family and community by individuals passing on their new experiences and knowledge learned from the program to others.”
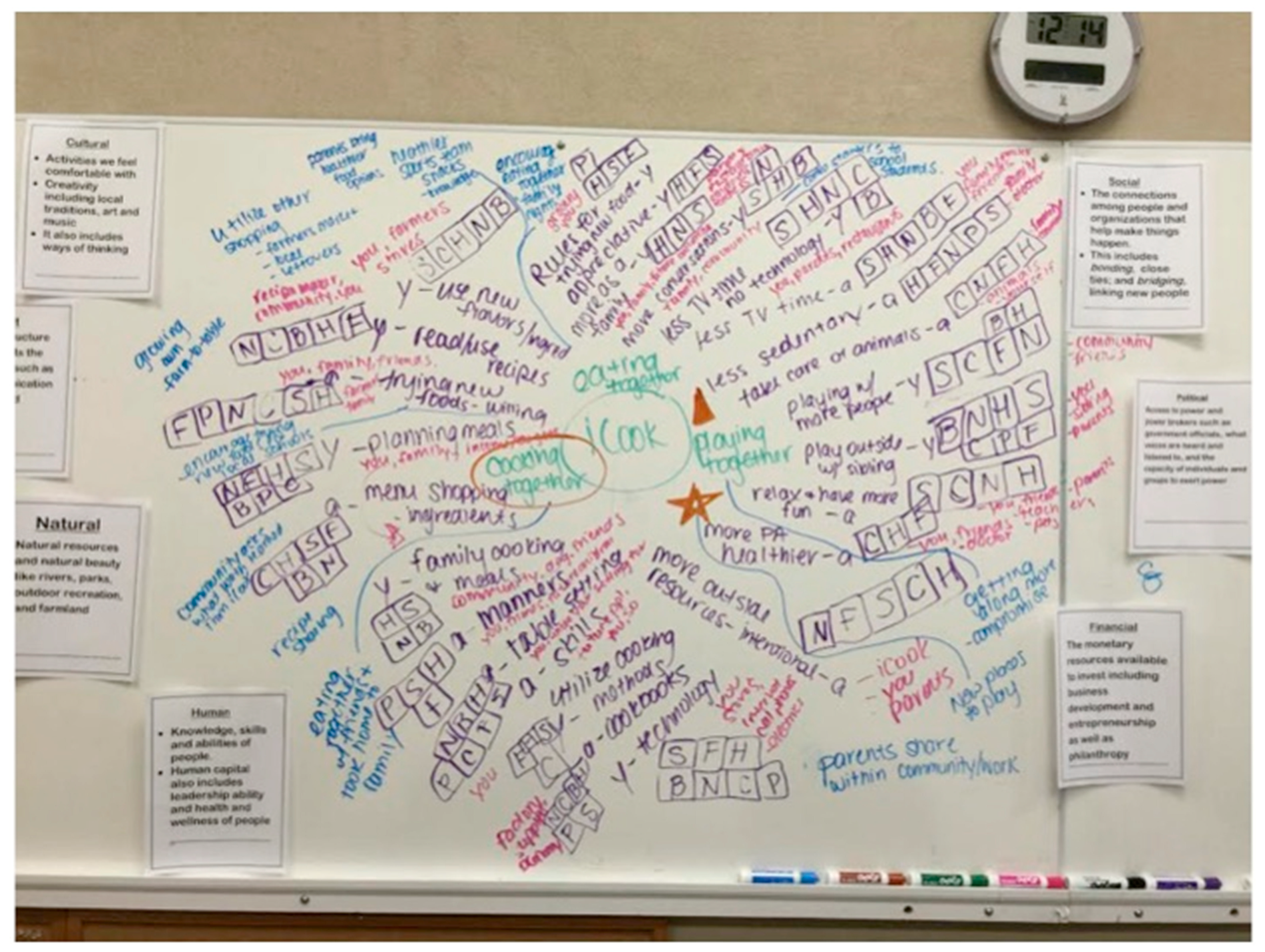
2.2.4. Mapping Process
2.3. Post Session
3. Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Meyers, D.C.; Durlak, J.A.; Wandersman, A. The quality implementation framework: A synthesis of critical steps in the implementation process. Am. J. Commun. Psychol. 2012, 50, 462–480. [Google Scholar] [CrossRef] [PubMed]
- Rennekamp, R.A.; Arnold, M.E. What progress, program evaluation? Reflections on a quarter-century of Extension evaluation practice. J. Ext. 2009, 47. 3COM1. [Google Scholar]
- Goodman, R.M. Bridging the gap in effective program implementation: From concept to application. J. Commun. Psychol. 2000, 28, 309–321. [Google Scholar] [CrossRef]
- Wandersman, A.; Duffy, J.; Flaspohler, P.; Noonan, R.; Lubell, K.; Stillman, L.; Blachman, M.; Dunville, R.; Saul, J. Bridging the gap between prevention research and practice: The interactive systems framework for dissemination and implementation. Am. J. Commun. Psychol. 2008, 41, 171–181. [Google Scholar] [CrossRef] [PubMed]
- Bauer, M.S.; Damschroder, L.; Hagedorn, H.; Smith, J.; Kilbourne, A.M. An introduction to implementation science for the non-specialist. BMC Psychol. 2015, 3, 32. [Google Scholar] [CrossRef] [PubMed]
- Darger, M. Capturing the ripples from community-driven business retention and expansion programs. J. Ext. 2014, 52. 2TOT6. [Google Scholar]
- Honeycutt, S.; Hermstad, A.; Carvalho, M.L.; Arriola, K.R.J.; Ballard, D.; Escoffery, C.; Kegler, M.C. Practice to evidence: Using evaluability assessment to generate practice-based evidence in rural South Georgia. Health Educ. Behav. 2017, 44, 454–462. [Google Scholar] [CrossRef] [PubMed]
- Lempa, M.; Goodman, R.M.; Rice, J.; Becker, A.B. Development of scales measuring the capacity of community-based initiatives. Health Educ. Behav. 2008, 35, 298–315. [Google Scholar] [CrossRef] [PubMed]
- Goodman, R.M. Principles and tools for evaluating community-based prevention and health promotion programs. J. Public Health Manag. Pract. 1998, 4, 37–47. [Google Scholar] [CrossRef] [PubMed]
- Butterfoss, F.; Goodman, R.; Wandersman, A.; Valois, R.; Chinman, M. The plan quality index: An empowerment research, consultation and feedback tool. In Empowerment Evaluation: Knowledge and Tools for Self-Assessment and Accountability; SAGE Publications: Thousand Oaks, CA, USA, 1995; pp. 304–331. [Google Scholar]
- Gaglio, B.; Shoup, J.A.; Glasgow, R.E. The RE-AIM framework: A systematic review of use over time. Am. J. Public Health 2013, 103, e38–e46. [Google Scholar] [CrossRef] [PubMed]
- Lobo, R.; Petrich, M.; Burns, S.K. Supporting health promotion practitioners to undertake evaluation for program development. BMC Public Health 2014, 14, 1315. [Google Scholar] [CrossRef] [PubMed]
- Emery, M.; Higgins, L.; Chazdon, S.; Hansen, D. Using ripple effect mapping to evaluate program impact: choosing or combining the methods that work best for you. J. Ext. 2015, 53, n2. [Google Scholar]
- Emery, M.; Flora, C. Spiraling-up: Mapping community transformation with community capitals framework. Commun. Dev. 2006, 37, 19–35. [Google Scholar] [CrossRef]
- Emery, M.; Fey, S.; Flora, C. Using community capitals to develop assets for positive community change. CD Pract. 2006, 13, 1–19. [Google Scholar]
- Nathaniel, K.C.; Kinsey, S.B. Contributions of youth engagement to the development of social capital through community mapping. J. Ext. 2013, 51, n1. [Google Scholar]
- Fey, S.; Bregendahl, C.; Flora, C. The measurement of community capitals through research. Online J. Rural Res. Policy 2006, 1, 1. [Google Scholar] [CrossRef]
- Kollock, D.H.; Flage, L.; Chazdon, S.; Paine, N.; Higgins, L. Ripple effect mapping: A “radiant” way to capture program impacts. J. Ext. 2012, 50, 1–5. [Google Scholar]
- Chazdon, S.; Emery, M.; Hansen, D.; Higgins, L.; Sero, R. A Field Guide to Ripple Effects Mapping; University of Minnesota Libraries Publishing: Minneapolis, MN, USA, 2017. [Google Scholar]
- Baker, B.; Johannes, E.M. Measuring social capital change using ripple mapping. New Dir. Stud. Leadersh. 2013, 2013, 31–47. [Google Scholar] [CrossRef] [PubMed]
- Kollock, D. Ripple Effects Mapping for Evaluation; Washington State University Curriculum Pullman: Washington, WA, USA, 2011. [Google Scholar]
- Welborn, R.; Downey, L.; Dyk, P.H.; Monroe, P.A.; Tyler-Mackey, C.; Worthy, S.L. Turning the tide on poverty: Documenting impacts through ripple effect mapping. Commun. Dev. 2016, 47, 385–402. [Google Scholar] [CrossRef]
- Bleich, S.N.; Segal, J.; Wu, Y.; Wilson, R.; Wang, Y. Systematic review of community-based childhood obesity prevention studies. Pediatrics 2013, 132, e201–e210. [Google Scholar] [CrossRef] [PubMed]
- Stice, E.; Shaw, H.; Marti, C.N. A meta-analytic review of obesity prevention programs for children and adolescents: The skinny on interventions that work. Psychol. Bull. 2006, 132, 667. [Google Scholar] [CrossRef] [PubMed]
- Thomas, H. Obesity prevention programs for children and youth: Why are their results so modest? Health Educ. Res. 2006, 21, 783–795. [Google Scholar] [CrossRef] [PubMed]
- Bandura, A. Social foundations of thought and action: a social cognitive theory; Prentice-Hall, Inc.: Englewood Cliffs, NJ, USA, 1986. [Google Scholar]
- Rolling, T.; Hong, M. The effect of social cognitive theory-based interventions on dietary behavior within children. J. Nutr. Health Food Sci. 2016, 4, 1–9. [Google Scholar]
- Lindsay, A.C.; Sussner, K.M.; Kim, J.; Gortmaker, S. The role of parents in preventing childhood obesity. Future Child. 2006, 169–186. [Google Scholar] [CrossRef]
- Dreisinger, M.L.; Boland, E.M.; Filler, C.D.; Baker, E.A.; Hessel, A.S.; Brownson, R.C. Contextual factors influencing readiness for dissemination of obesity prevention programs and policies. Health Educ. Res. 2011, 27, 292–306. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- White, A.; Franzen-Castle, L.; Kattelmann, K.; Colby, S.; Olfert, M. Outputs and outcomes at year 5 of the out-of-school program for youth and adult dyads: iCook 4-H. J. Nutr. Educ. Behav. 2017, 49, S123. [Google Scholar] [CrossRef]
- Ripple Effect Mapping Parts1-4: [Video Files]. Available online: http://ucanr.edu/sites/Social_Capital_Multi-State/Tools_for_Engagement_-_Evaluation/ (accessed on 12 January 2018).
- Barbour, R.; Kitzinger, J. Developing Focus Group Research: Politics, Theory and Practice; SAGE: London, UK, 2000. [Google Scholar]
- Whitney, D.; Cooperrider, D. Appreciative inquiry: A positive revolution in change; ReadHowYouWant.com Ltd.: Sydney, Australia, 2011. [Google Scholar]
- Cooperrider, D.L.; Barrett, F.; Srivastva, S. Social construction and appreciative inquiry: A journey in organizational theory. In Management and Organization: Relational Alternatives to Individualism; Hosking, D., Dachler, P., Gergen, K., Eds.; Avebury Press: Aldershot, UK, 1995; pp. 157–200. [Google Scholar]
- Priest, K.L.; Kaufman, E.K.; Brunton, K.; Seibel, M. Appreciative Inquiry: A tool for organizational, programmatic, and project-focused change. J. Leadersh. Educ. 2013, 12, 18–33. [Google Scholar] [CrossRef]
- Miller, A.; Franzen-Castle, L.; Aguirre, T.; Krehbiel, M.; Colby, S.; Kattelmann, K.; Olfert, M.D.; Mathews, D.; White, A. Food-related behavior and intake of adult main meal preparers of 9–10 year-old children participating in iCook 4-H: A five-state childhood obesity prevention pilot study. Appetite 2016, 101, 163–170. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Elo, S.; Kyngäs, H. The qualitative content analysis process. J. Adv. Nurs. 2008, 62, 107–115. [Google Scholar] [CrossRef] [PubMed]
- Hsieh, H.-F.; Shannon, S.E. Three approaches to qualitative content analysis. Qual. Health Res. 2005, 15, 1277–1288. [Google Scholar] [CrossRef] [PubMed]
- Dey, I. Qualitative Data Analysis: A User-Friendly Guide for Social Scientists; Routledge: London, UK, 1993. [Google Scholar]
- McCain, G.C. Content analysis: A method for studying clinical nursing problems. Appl. Nurs. Res. 1988, 1, 146–147. [Google Scholar] [CrossRef]
- Burnard, P. A method of analysing interview transcripts in qualitative research. Nurse Educ. Today 1991, 11, 461–466. [Google Scholar] [CrossRef]
- Thomas, E.; Magilvy, J.K. Qualitative rigor or research validity in qualitative research. J. Spec. Ped. Nurs. 2011, 16, 151–155. [Google Scholar] [CrossRef] [PubMed]
- Harris, J.R.; Cheadle, A.; Hannon, P.A.; Lichiello, P.; Forehand, M.; Mahoney, E.; Snyder, S.; Yarrow, J. A framework for disseminating evidence-based health promotion practices. Prev. Chronic Dis. 2012, 9, E22. [Google Scholar] [CrossRef] [PubMed]
- Kerner, J.; Rimer, B.; Emmons, K. Introduction to the special section on dissemination: Dissemination research and research dissemination: How can we close the gap? Health Psychol. 2005, 24, 443. [Google Scholar] [CrossRef] [PubMed]
- Wilansky, J.A. The effects of curriculum mapping on the instructional practices of professional collaboration, standards alignment, and* assessment; Dowling College: Oakdale, NY, USA, 2006. [Google Scholar]
- Glasgow, R.E.; Vogt, T.M.; Boles, S.M. Evaluating the public health impact of health promotion interventions: The RE-AIM framework. Am. J. Public Health 1999, 89, 1322–1327. [Google Scholar] [CrossRef] [PubMed]
- Kegler, M.C.; Rodine, S.; McLeroy, K.; Oman, R. Combining quantitative and qualitative techniques in planning and evaluating a community-wide project to prevent adolescent pregnancy. Int. Electron. J. Health Educ. 1998, 1, 39–48. [Google Scholar]
- Mattos, D. Community capitals framework as a measure of community development. 2015. Institute of Agriculture and Natural Resources, University of Nebraska-Lincoln. Available online: http://www.agecon.unl.edu/cornhuskereconomics (accessed on 18 March 2018).
- Haskell, J.; Baker, B.; Olfert M., D.; Colby, S.; Kattelmann, K.; Franzen-Castle, L.; White, A. Using Ripple Effects Maps to Identify Story Threads: A Framework to Link Private to Public Value. J. Hum. Sci. Ext. Submitted.
- Morris, A.M.; Hagedorn, R.L.; Barr, M.L.; King, S.J.; Famodu, O.A.; Clark, R.L.; Charlier, C.M.; White, A.; Colby, S.E.; Kattlemann, K. eb4CAST: Application of a novel forecasting and footprinting dissemination framework to a community based childhood obesity prevention program. FASEB J. 2017, 31. 302.307. [Google Scholar]
- Ritchie, J.; Lewis, J.; Nicholls, C.M.; Ormston, R. Qualitative Research Practice: A Guide for Social Science Students and Researchers; Sage: Los Angeles, CA, USA, 2013. [Google Scholar]




{kind=link}
{kind=link}
{kind=link}
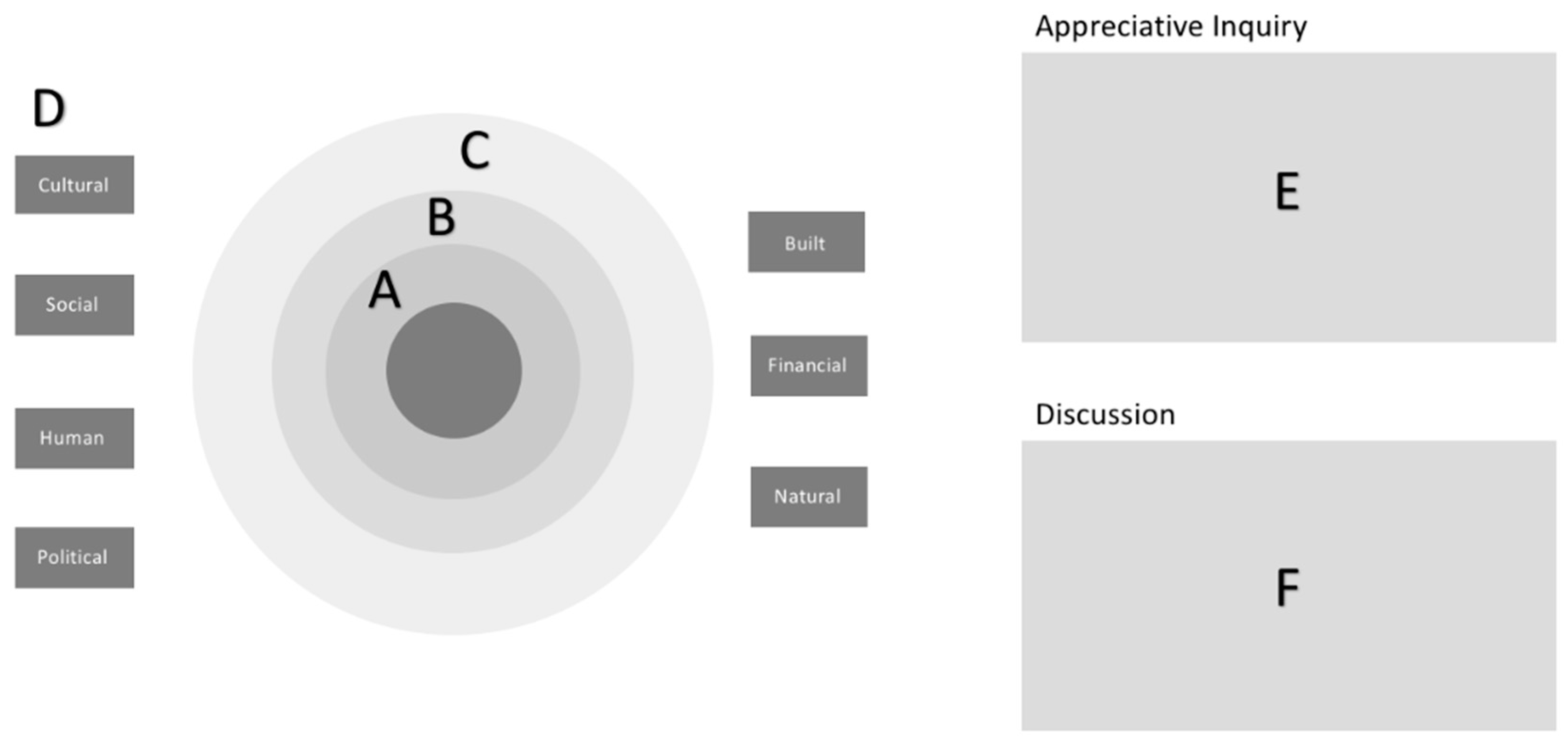
| Social: Connections among individuals and groups that help make things happen, including bonding with people you know and bridging to new people or seeing people in unfamiliar roles. |
| Natural: Natural resources and natural beauty like rivers, parks, outdoor recreation, and farmland. |
| Cultural: Activities, foods, creativity (local traditions, art, and music), and ways of thinking that are familiar. |
| Human: Knowledge, skills, and abilities of people; also includes leadership ability and health and wellness of people. |
| Political: Access to decision-makers, such as student council, school boards, or town councils. Power of individuals and groups to influence rules or budgets. |
| Financial: Money available to invest, including helping or starting businesses, as well as giving away money and goods to those who need it. |
| Built: Structures and facilities that support a community, such as communications, roads, and buildings. |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Olfert, M.D.; Hagedorn, R.L.; White, J.A.; Baker, B.A.; Colby, S.E.; Franzen-Castle, L.; Kattelmann, K.K.; White, A.A. An Impact Mapping Method to Generate Robust Qualitative Evaluation of Community-Based Research Programs for Youth and Adults. Methods Protoc. 2018, 1, 25. https://doi.org/10.3390/mps1030025
Olfert MD, Hagedorn RL, White JA, Baker BA, Colby SE, Franzen-Castle L, Kattelmann KK, White AA. An Impact Mapping Method to Generate Robust Qualitative Evaluation of Community-Based Research Programs for Youth and Adults. Methods and Protocols. 2018; 1(3):25. https://doi.org/10.3390/mps1030025
Chicago/Turabian StyleOlfert, Melissa D., Rebecca L. Hagedorn, Jade A. White, Barbara A. Baker, Sarah E. Colby, Lisa Franzen-Castle, Kendra K. Kattelmann, and Adrienne A. White. 2018. "An Impact Mapping Method to Generate Robust Qualitative Evaluation of Community-Based Research Programs for Youth and Adults" Methods and Protocols 1, no. 3: 25. https://doi.org/10.3390/mps1030025