Paediatric Strongyloidiasis in Central Australia

1
BBioMedSci MBBS Hons, Paediatric Senior Registrar, Department of Paediatrics, Alice Springs Hospital, P.O. Box 2234, Alice Springs NT 0871, Australia
2
FRACP, Head of Department, Department of Paediatrics, Alice Springs Hospital, P.O. Box 2234, Alice Springs NT 0871, Australia
*
Author to whom correspondence should be addressed.
Trop. Med. Infect. Dis. 2018, 3(2), 64; https://doi.org/10.3390/tropicalmed3020064
Submission received: 30 April 2018
/
Revised: 6 June 2018
/
Accepted: 6 June 2018
/
Published: 13 June 2018
(This article belongs to the Special Issue Control of Communicable Diseases in Human and in Animal Populations: 70th Anniversary Year of the Birth of Professor Rick Speare (2 August 1947 – 5 June 2016))
Abstract
:Few published studies are available describing the prevalence of paediatric strongyloidiasis in endemic areas within Australia. This literature review and exploratory clinical audit presents the first seroprevalence data for paediatric patients in Central Australia. A total of 16.1% (30/186) of paediatric inpatients tested for Strongyloides stercoralis in 2016 were seropositive (95% CI: 11.5% to 22.1%). Eosinophilia of unknown aetiology was the most common indication for testing (91.9%). Seropositive patients were significantly more likely to reside in communities outside of Alice Springs (p = 0.02). Seropositive patients were noted to have higher mean eosinophil counts with a mean difference of 0.86 × 109/L (95% CI: 0.56 to 1.16, p < 0.0001), although the limited utility of eosinophilia as a surrogate marker of strongyloidiasis has been described previously. All seropositive patients were Indigenous. There was no significant difference in ages between groups. There was a male predominance in the seropositive group, although this was not significant (p = 0.12). Twelve patients had known human T-lymphotropic virus 1 (HTLV-1) status and all were seronegative. Further research describing the epidemiology of strongyloidiasis in Central Australia is required.
1. Introduction
The soil-transmitted helminth Strongyloides stercoralis has been described as one of the most neglected of the neglected tropical diseases [1]. Globally, strongyloidiasis is estimated to affect 30 to 370 million people, although data are limited [2,3]. S. stercoralis can cause decades-long infection in human hosts [4]. Infection may be clinically silent or cause a range of respiratory, skin, and gastrointestinal symptoms, or fulminant hyperinfection, typically in the setting of immune compromise [5,6,7].
The Strongyloides genus includes over fifty species capable of establishing parasitic infections in a range of animal hosts, and two species are known to infect humans [8]. Strongyloides fuelleborni is present in Papua New Guinea and Africa, while S. stercoralis is endemic throughout southern Europe, Africa, Asia, the Americas, and the northern two-thirds of Australia [2,9].
Some remote Australian Indigenous communities have S. stercoralis seroprevalences approaching 60%, putting them amongst the highest in the world [2,10,11]. Within these communities, Indigenous children have a higher documented prevalence of strongyloidiasis than any other age group [9,12,13,14,15,16].
S. stercoralis disproportionately affects resource-poor populations [17]. Remote Indigenous communities face an inequitable burden of poor health, socioeconomic disadvantage, and barriers to environmental control that impair disease control at a population level [8,18].
Human T-cell lymphotropic virus type 1 (HTLV-1) is an oncogenic virus that infects CD4+ T cells and interferes with Th2 immune responses [19]. HTLV-1 is endemic in Central Australia, and co-infection with S. stercoralis is associated with severe strongyloidiasis, Strongyloides treatment failure, and increased likelihood of developing T cell lymphoma [5,7,20]. HTLV-1 prevalence in Central Australia is estimated to be approximately from 7.2% to 13.9% among Indigenous adults [20].
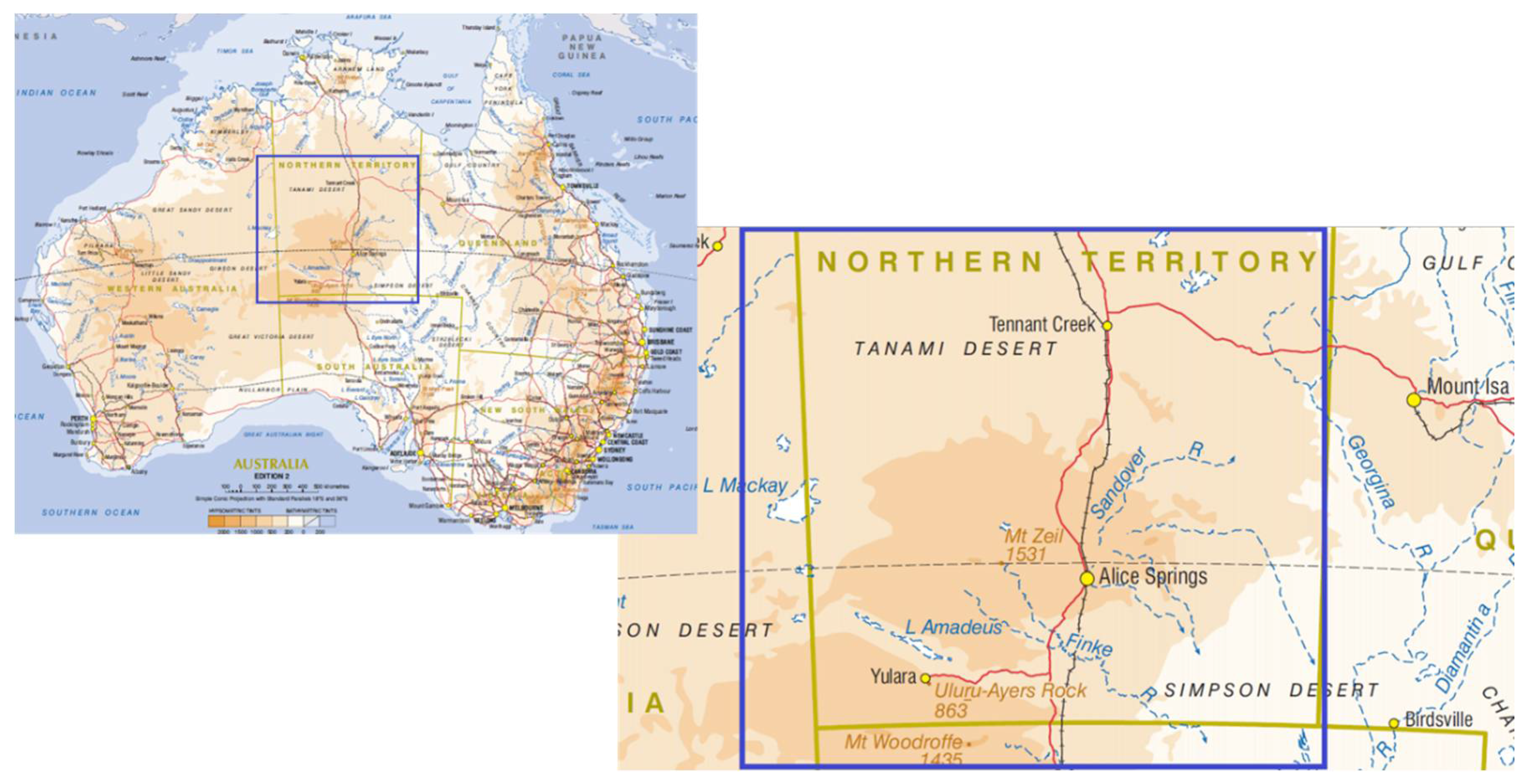
Alice Springs Hospital services an extremely remote area of Central Australia that includes the southern half of the Northern Territory and adjacent parts of Western Australia and South Australia. It has a catchment area of approximately 900,000 square km with a population of 48,000 people, of whom 44% are Indigenous Australians (see Figure 1) [21].
Over the last three years, the paediatric department has increasingly tested patients with unexplained eosinophilia or other growth, respiratory, or abdominal symptoms for strongyloidiasis, and is in the process of formalising a policy to improve the recognition and management of this condition. HTLV-1 serology is performed on patients with clinical suspicion of immune compromise, particularly in children with chronic suppurative lung disease.
This paper will review of the literature relevant to S. stercoralis epidemiology in endemic areas of Australia, and present the results of an audit of S. stercoralis testing of paediatric inpatients at Alice Springs Hospital.
2. Review of Endemic Strongyloidiasis Epidemiology in Australia
S. stercoralis has been recognised as a pathogen in Australia for almost a century [23]. Studies examining the prevalence of strongyloidiasis in Australia can be divided into those undertaken in endemic areas and those describing prevalence in groups that have likely acquired it overseas (including migrants and refugee groups and returned military service personnel) [2]. This paper will focus on strongyloidiasis epidemiology in endemic areas within Australia.
The life cycle of S. stercoralis is complex and directly relevant to estimates of prevalence [24]. Male and female adults are capable of a single generation of free-living sexual reproduction outside of hosts, and non-infectious rhabditiform larvae moult into parasitic filariform larvae capable of surviving for up to two to three weeks in the environment under optimal conditions [25].
Filariform larvae penetrate host skin and migrate through the lymphatic or venous system to the lungs. They ascend the respiratory tree, are swallowed and migrate to the intestine. Parthenogenic female adults mature and invade the wall of the duodenum and jejunum where they lay up to fifty eggs per day [24]. Eggs hatch into rhabditiform larvae that migrate back into the intestinal lumen. Larvae may pass into the stool or mature into filariform larvae within the intestine and penetrate back into the host, establishing an auto-infective cycle [24].
A review of existing original research relating to the epidemiology of strongyloidiasis in endemic areas of Australia is presented in Table 1. This table is adapted from [11,18] with additional papers identified from Medline search and reference lists. Articles were located using Medical Subject Headings (MeSH) and text-word terms ‘Strongyloides’ or ‘Strongyloidiasis’ and ‘Australia’. Papers presenting epidemiological data from S. stercoralis endemic areas within Australia were included. Case reports and papers presenting data from other populations were excluded.
Estimates of strongyloidiasis prevalence within endemic areas in Australia vary widely depending on diagnostic method, population surveyed, and season. Community-based studies using faecal larval detection report prevalence rates from <1% to 41%, with substantial increases during the wet season in some locations [10,11,15,26,27]. Agar plate culture for a single stool sample is reported to be less than 60% sensitive [28]. Yield improves with multiple stool examinations and specialised microbiological techniques such as Baermann concentration [28], although this is not available at our health service.
Serology is more sensitive than stool detection of S. stercoralis larvae [28]. The sensitivities of various serological assays range from 75.4% to 93.9%, and specificities from 92.2% to 100% [29]. Flannery and White [30] reported the highest seropositivity rate in Australia of 59.6% of individuals tested in one small Northern Territory community. In Central Australia, Einsedel and colleagues reported a seroprevalence of 23.9% among 1126 hospitalised Indigenous adults [20]. No studies examining the seroprevalence of S. stercoralis in children in Central Australia were identified.
Children are over-represented in population estimates of strongyloidiasis. A Territory-wide study examining faecal larval detection between 2002 and 2012 found that children under five represented 42.2% of diagnoses, with rates of 3–6% of stool samples examined compared to 1.7% of samples overall [9]. A study of patients diagnosed with strongyloidiasis by faecal microscopy at Royal Darwin Hospital also identified that patients under five years of age were disproportionately represented, with 54% of cases falling in this age group [13].
Growth faltering remains a serious problem in the Northern Territory, affecting about 1 in 7 children under 5 years old in remote communities [31]. Associations between strongyloidiasis and malnutrition are well established but debate remains as to whether strongyloidiasis alone can cause growth faltering or represents an opportunistic infection in a compromised host [1]. The criteria for malnutrition were met by 80% of children diagnosed with strongyloidiasis in one study [13]. In another, Indigenous children with malnutrition were 6.5 times (95% confidence interval [CI]: 1.6 to 26.7) more likely to have S. stercoralis than a control group of well-nourished children [14].
Eosinophilia may be the only feature of strongyloidiasis in otherwise asymptomatic hosts, but remains an unreliable marker of strongyloidiasis. Mayer-Cloverdale and colleagues [9] found that just 40.8% of all patients with detectable S. stercoralis larvae in their stool had eosinophil counts of 0.5 × 109 cells/L or greater. Eosinophilia was more common in patients under five and was present in 65.5% of positive cases (p < 0.0001) [9].
3. Clinical Audit Methods
Retrospective admission data from Alice Springs Hospital for the 2016 calendar year were obtained. The records of 2071 patients under the age of 16 years old admitted to the paediatric ward were reviewed as part of a departmental audit. Of these, 186 patients who had been tested for S. stercoralis were identified. Nonidentifiable coded data relating to patient demographics, clinical presentation, indication for testing, haemoglobin, mean corpuscular volume, eosinophil count, Strongyloides serology results, HTLV-1 status (if known), and faecal examination results were collated.
Symptoms at presentation were noted for each patient, with specific reference to growth faltering and gastrointestinal, respiratory, dermatological, and blood stream infections that might be attributable to strongyloidiasis. Growth faltering was defined as weight for age below the 3rd centile, standard weight for height less than two standard deviations below the mean, or crossing of two or more centile lines. Gastrointestinal symptoms included abdominal pain, altered bowel habit, vomiting, and anorexia. Respiratory symptoms included cough, dyspnoea, tachypnoea, chest pain, and pharyngitis. Dermatological manifestations were limited to urticarial rash or larva currens. Pruritus was not included due to the endemic nature of scabies and head lice in this population.
S. stercoralis serology was performed by Western Diagnostic Pathology, using an IgG enzyme-linked immunosorbent assay (ELISA) produced commercially by DRG Instruments. This assay detects IgG directed against the soluble fraction of filariform S. stercoralis larvae. The sensitivity of this assay is reported to be 91.2% with a specificity of 93.3% [37]. An optical density of 0.2 or greater is considered positive. In patients from nonendemic areas, a result of 0.2 to 0.4 is considered equivocal.
Statistical analysis was conducted using GraphPad software. Continuous data sets were analysed using unpaired t-tests. Confidence intervals for categorical data were calculated using the modified Wald method, and p values were determined using Chi-square calculations.
This study was conducted in accordance with the Declaration of Helsinki. No identifiable patient data was collected or retained by the investigators.
4. Results
Eosinophilia of unknown aetiology was the indication for testing in 91.9% (171/186) of patients, and seven were tested because of previous eosinophilia. Of the remaining patients, one patient had growth concerns, one was commenced on immunosuppressant medications, and six had gastrointestinal or respiratory presentations suggestive of strongyloidiasis.
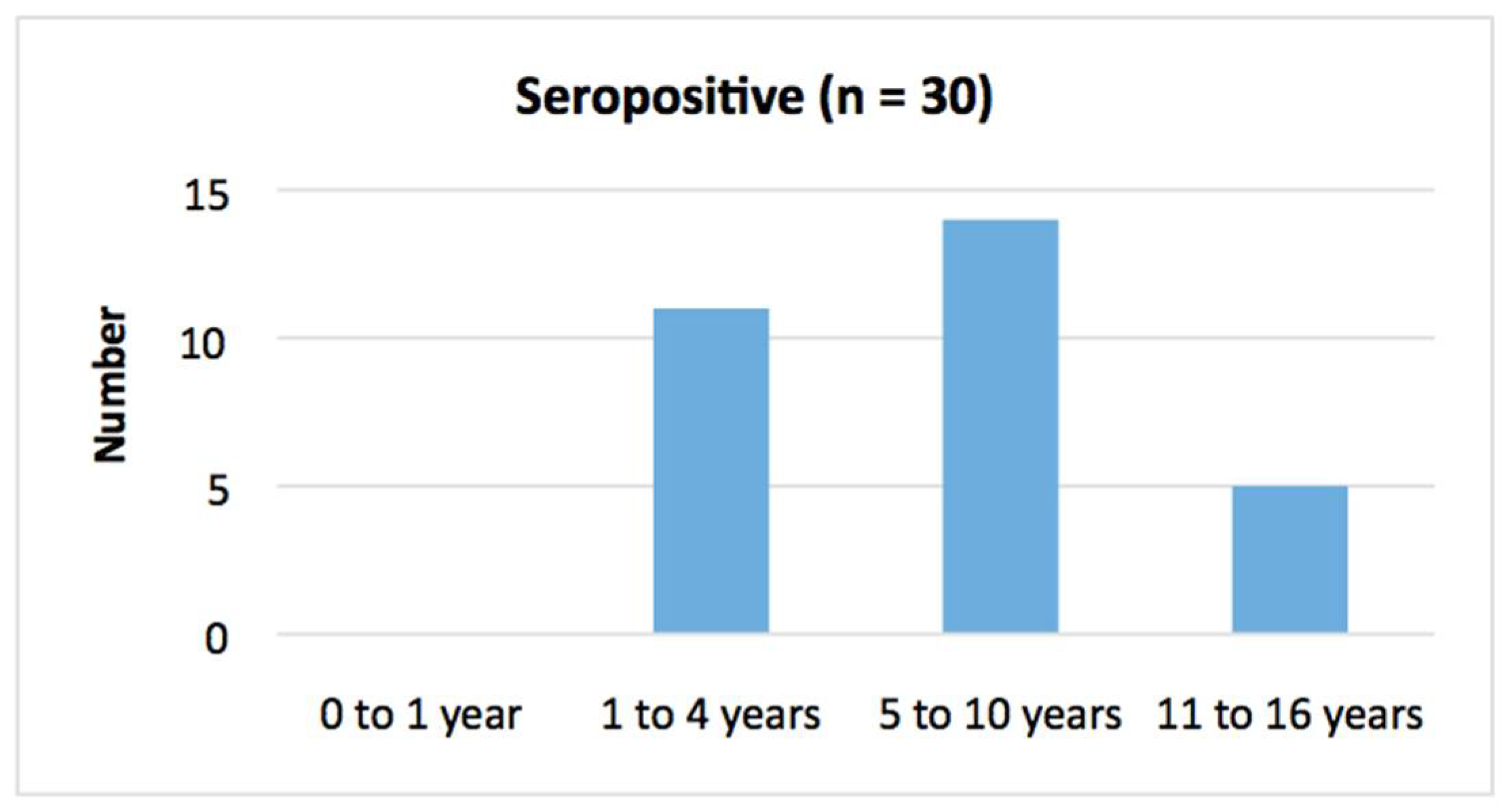
Overall, 16.1% (30/186) of patients tested were seropositive for S. stercoralis (95% CI: 11.5% to 22.1%). There was no significant age difference between seropositive and seronegative groups (p = 0.55) (Table 2, Figure 2 and Figure 3). A male predominance in the seropositive group was observed although the difference was not significant (p = 0.12). Seropositive patients were significantly more likely to reside in communities outside of Alice Springs (p = 0.02).
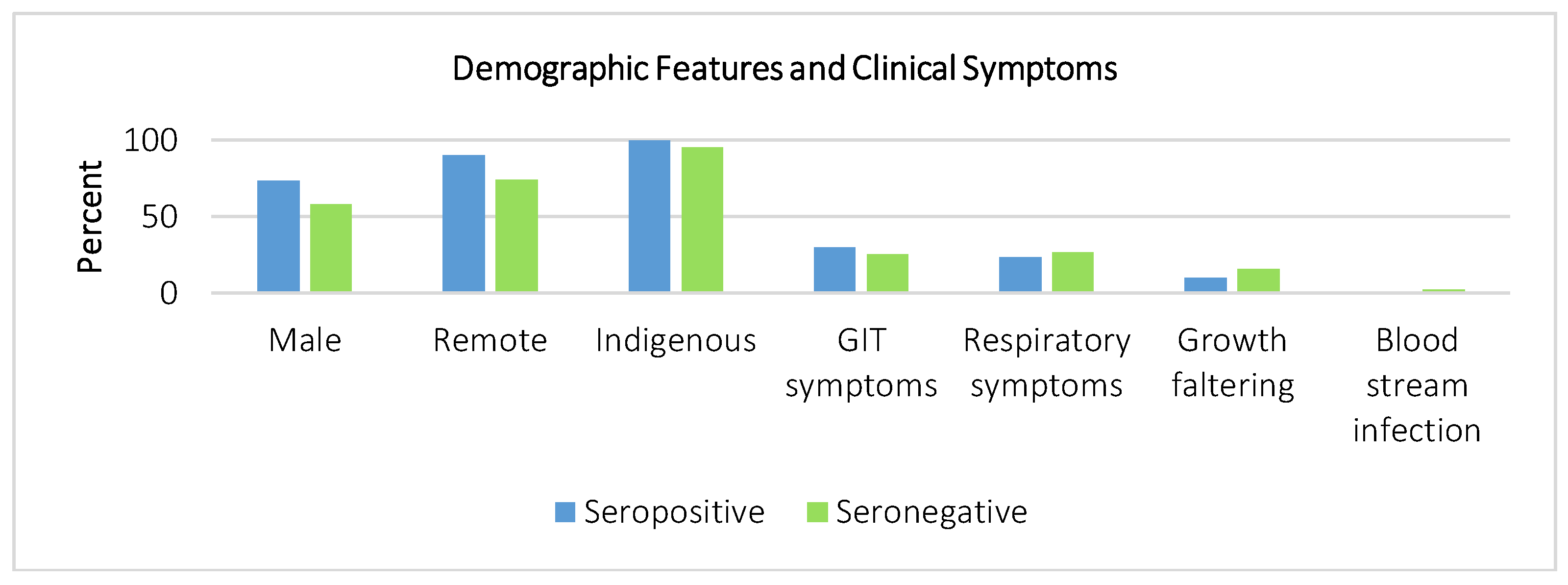
The data did not support any significant differences in clinical presentation, haemoglobin, or mean corpuscular volume (Figure 4). Four seronegative patients had bloodstream infections, including one patient with cryptococcal disease and three patients with Staphylococcus aureus bacteraemia. No patients in either group presented with urticaria or larva currens. No cases of hyperinfection were identified, and none of the 12 patients who had HTLV-1 testing were seropositive.
Within the group of patients tested because of eosinophilia, seropositive patients were noted to have a significantly higher mean eosinophil count with a mean difference of 0.86 × 109/L (95% CI: 0.56 to 1.16, p < 0.0001). Of the 55 patients that had a stool sample sent, none had S. stercoralis larvae detected (Table 3). There was no significant difference in the rate of other stool pathogens identified between groups (p = 0.09).
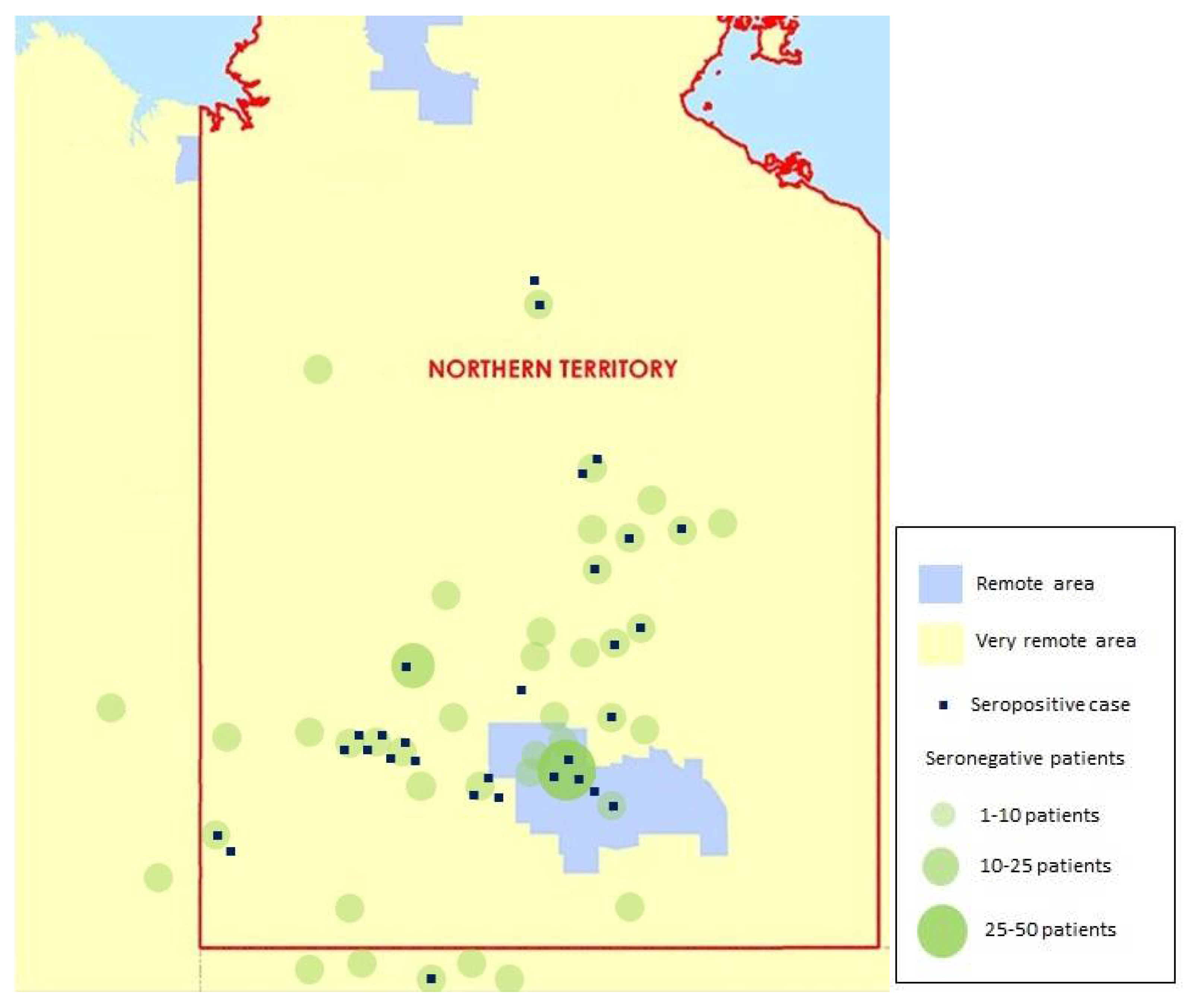
The geographical distribution of seropositive and seronegative patients is shown in Figure 5.
5. Discussion
This exploratory audit highlights many of the universal challenges of understanding and managing S. stercoralis. Robust epidemiological data are lacking, clinical features and surrogate markers for infection are poorly sensitive and specific, and microbiological diagnosis is difficult. Although there was a significant difference in mean eosinophil counts, wide ranges and substantial overlap between data sets highlight the limitations of eosinophilia as a clinically useful indicator of possible strongyloidiasis. Further investigation is required to better understand the burden and epidemiology of strongyloidiasis in children in Central Australia.
This audit is limited by small patient numbers, retrospective data collection, and selective population sampling. No reliable conclusions regarding the prevalence of strongyloidiasis among the general paediatric inpatient population or paediatric population in Central Australia can be drawn from this audit. The geographical distribution of cases cannot be used to infer community prevalence but may suggest a clustering of cases in western and northern communities. This is also likely to reflect in part the relative distribution of the remote populations surrounding Alice Springs.
The predominance of remote diagnoses is likely to reflect the ability of S. stercoralis to thrive in infrastructure-poor areas, and strongyloidiasis remains a disease predominantly of the poorly resourced in Central Australia [17]. The social determinants of health are starkly relevant in this context, and Einsiedel and Fernandez summarise some of the challenges that remote Indigenous communities face in controlling strongyloidiasis at a population level [5]:
Ultimately, strongyloidiasis is a disease of poverty that reflects the appalling socioeconomic situation of Indigenous Australia. In some communities, a median number of 17 persons live in each house, and nearly 50% of dwellings do not have functioning facilities to remove faeces. The endemicity of both S. stercoralis and HTLV-1... renders public education and improvements to housing imperative.
Socioeconomic disadvantage is associated with higher rates of morbidity and mortality from strongyloidiasis, particularly where this leads to overcrowding, breakdown in sanitation systems, and environmental disease reservoirs from soil contamination [17]. Addressing water, sewerage, and garbage management systems remains fundamental to breaking the cycle of infection and reinfection [8].
Reviews examining other barriers to strongyloidiasis control in Indigenous communities have identified several points for intervention, including the need for improved reporting protocols, increased testing of at-risk individuals, health professional engagement, and community-based monitoring and control programs [8,18,42]. Collaborative community-based initiatives incorporating mass deworming, infrastructure improvements, and culturally safe health education (Figure 6) have demonstrated significant reductions in Strongyloides seroprevalences [16,18,42]. One Western Australian study saw the seropositivity in 259 Indigenous adults fall from 35.3% to 5.8% in three years using these strategies [43]. A study in Arnhem Land in the Northern Territory saw seropositivity fall from 21% at baseline to 2% after 18 months of annual mass drug administration [16].
Evidence is emerging that dogs may act as hosts for human strongyloidiasis in some settings [44,45]. Animal services in remote communities are often limited, leading to animal over-population in some areas [46]. Community-based interventions may need to consider incorporating animal management into programs to address this potential reservoir [44].
Within community-based initiatives, further research is needed to inform practices relating to the testing and treatment of Indigenous children. Universal testing of Indigenous people living in endemic areas has been recommended [18,42]. The logistical challenges of implementing universal paediatric testing are substantial in our context. Paediatric blood collection is time-consuming and distressing for patients. Opportunistic blood collection is possible but carries additional costs to health services. Results are rarely available prior to discharge and locating patients for follow-up dosing and serology testing in remote communities is often difficult. Blood spot serology testing is under development and may make this investigation substantially more acceptable to parents and facilitate testing in nurse-led remote clinics where staff may have limited capacity to do paediatric venepuncture [28].
The safety and tolerability of ivermectin in paediatric patients also requires further investigation. Ivermectin is the mainstay of treatment for strongyloidiasis in adults and older children and has been used in this setting for almost 30 years [47]. The use of ivermectin in children under 15 kilograms or five years of age remains problematic due to a lack of safety data [48], although many health services (including our own) routinely use ivermectin in children under five years old and between ten and fifteen kilograms in weight, at the discretion of the treating specialist.
6. Conclusions
Almost 1 in 6 paediatric patients tested for strongyloidiasis at our health service were found to be seropositive. Remote communities experience an intersection of risk factors that predispose them to a disproportionate burden of disease from S. stercoralis. These include poorer sanitation infrastructure, inadequate and overcrowded housing, limited access to health services, very limited access to animal control services, high HTLV-1 prevalence and rates of other chronic comorbidities, and minimal disease surveillance [2,8,17,18,42].
These reflect the global experience of strongyloidiasis as a disease that predominantly affects and exploits the poorly resourced. Management of strongyloidiasis remains inextricably linked to improving the social determinants of health experienced by these communities and controlling environmental reservoirs to reduce the risk of reinfection [17].
Continued advocacy for improvements in basic infrastructure, health service resources and awareness, proactive disease monitoring, and access to effective treatment remains fundamental to the control of strongyloidiasis and other neglected diseases in the most vulnerable communities both within Australia and overseas [3,18].
Author Contributions
Conceptualization, A.W.; methodology, A.W.; formal analysis, A.W.; investigation, A.W.; data curation, A.W.; writing—original draft preparation, A.W.; writing—review & editing, A.W. and D.F.; visualization, A.W.; supervision, D.F.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Olsen, A.; van Lieshout, L.; Marti, H.; Polderman, T.; Polman, K.; Steinmann, P.; Stothard, R.; Thybo, R.; Verweij, J.; Magnussen, P. Strongyloidiasis—The most neglected of the neglected tropical diseases? Trans. R. Soc. Trop. Med. Hyg. 2009, 103, 967–972. [Google Scholar] [CrossRef] [PubMed]
- Schar, F.; Trotsdorf, U.; Giardina, F.; Khieu, V.; Muth, S.; Marti, H.; Vounatsou, U.; Odermatt, P. Strongyloides stercoralis: Global distribution and risk factors. PLoS Negl. Trop. Dis. 2013, 7, 1–17. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bisoffi, Z.; Buonfrate, D.; Montresor, A.; Requena-Mendes, A.; Munoz, J.; Krolewiecki, A.J.; Gotuzzo, E.; Mena, M.A.; Chiodini, P.L.; Anselmi, M.; et al. Strongyloides stercoralis: A plea for action. PLoS Negl. Trop. Dis. 2013, 7, e2214. [Google Scholar] [CrossRef] [PubMed]
- Rahmanian, H.; MacFarlane, A.C.; Rowland, K.E.; Einsiedel, L.J.; Neuhaus, S.J. Seroprevalence of Strongyloides stercoralis in a South Australian Vietnam veteran cohort. Aust. N. Z. J. Public Health 2015, 39, 331–335. [Google Scholar] [CrossRef] [PubMed]
- Einsiedel, L.; Fernandes, L. Strongyloides stercoralis: A cause of morbidity and mortality for indigenous people in Central Australia. Intern. Med. J. 2008, 38, 697–703. [Google Scholar] [CrossRef] [PubMed]
- Page, W.; Speare, R. Chronic strongyloidiasis—Don’t look and you won’t find. Aust. Fam. Phys. 2016, 45, 40–44. [Google Scholar]
- Buonfrate, D.; Requena-Mendez, A.; Angheben, A.; Munoz, J.; Gobbi, F.; Van Den Ende, J.; Bisoffi, Z. Severe strongyloidiasis: A systematic review of case reports. BMC Infect. Dis. 2013, 13, 78. [Google Scholar] [CrossRef] [PubMed]
- Taylor, M.J.; Garrard, T.A.; O’Donahoo, F.J.; Ross, K.E. Human strongyloidiasis: Identifying knowledge gaps, with emphasis on environmental control. Res. Rep. Trop. Med. 2014, 2014, 55–63. [Google Scholar] [CrossRef]
- Mayer-Coverdale, J.; Crowe, A.; Smith, P.; Baird, R. Trends in Strongyloides stercoralis fecal larvae detections in the Northern Territory, Australia: 2002 to 2012. Trop. Med. Infect. Dis. 2017, 2, 18. [Google Scholar] [CrossRef]
- Adams, M.; Page, W.; Speare, R. Strongyloidiasis: An issue in Aboriginal communities. Rural Remote Health 2003, 3, 152. [Google Scholar] [PubMed]
- Johnston, F.H.; Morris, P.S.; Speare, R.; McCarthy, J.; Currie, B.; Ewald, D.; Page, W.; Dempsey, K. Strongyloidiasis: A review of the evidence for Australian practitioners. Aust. J. Rural Health 2005, 13, 247–254. [Google Scholar] [CrossRef] [PubMed]
- Meloni, B.P.; Thompson, R.C.; Hopkins, R.M.; Reynoldson, J.A.; Gracey, M. The prevalence of Giardia and other intestinal parasites in children, dogs and cats from aboriginal communities in the Kimberley. Med. J. Aust. 1993, 158, 157–159. [Google Scholar] [PubMed]
- Fisher, D.; McCarry, F.; Currie, B. Strongyloidiasis in the Northern Territory. Under-recognised and under-treated? Med. J. Aust. 1993, 159, 88–90. [Google Scholar] [PubMed]
- Kukuruzovic, R.; Robins-Browne, R.M.; Anstey, N.M.; Brewster, D.R. Enteric pathogens, intestinal permeability and nitric oxide production in acute gastroenteritis. Pediatr. Infect. Dis. J. 2002, 21, 730–739. [Google Scholar] [CrossRef] [PubMed]
- Shield, J.; Aland, K.; Kearns, T.; Gongdjalk, G.; Holt, D.; Currie, B.; Prociv, P. Intestinal parasites of children and adults in a remote Aboriginal community of the Northern Territory, Australia, 1994–1996. West. Pac. Surveill. Response J. 2015, 6, 44–51. [Google Scholar] [CrossRef] [Green Version]
- Kearns, T.M.; Currie, B.J.; Cheng, A.C.; McCarthy, J.; Carapetis, J.C.; Holt, D.C.; Page, W.; Shield, J.; Gundjirryirr, R.; Mulholland, E.; et al. Strongyloides seroprevalence before and after an ivermectin mass drug administration in a remote Australian Aboriginal community. PLoS Negl. Trop. Dis. 2017, 11, e0005607. [Google Scholar] [CrossRef] [PubMed]
- Beknazarova, M.; Whiley, H.; Ross, K. Strongyloidiasis: A disease of socioeconomic disadvantage. Int. J. Environ. Res. Public Health 2016, 13, 517–532. [Google Scholar] [CrossRef] [PubMed]
- Miller, A.; Smith, M.L.; Judd, J.A.; Speare, R. Strongyloides stercoralis: Systematic review of barriers to controlling strongyloidiasis for Australian indigenous communities. PLoS Negl. Trop. Dis. 2014, 8, e3141. [Google Scholar] [CrossRef] [PubMed]
- Mirdha, B.R. Human strongyloidiasis: Often brushed under the carpet. Trop. Gastroenterol. 2009, 30, 1–4. [Google Scholar] [PubMed]
- Einsiedel, L.; Spelman, T.; Goeman, E.; Cassar, O.; Arundell, M.; Gessain, A. Clinical associations of humanT-type 1 infection in an indigenous Australian population. PLoS Negl. Trop. Dis. 2014, 8, e2643. [Google Scholar] [CrossRef] [PubMed]
- Northern Territory Government. NT Health Governance: Central Australia Health Service (CAHS). Available online: https://health.nt.gov.au/health-governance/central-australia-health-service (accessed on 5 April 2018).
- Commonwealth of Australia. 1:20M Australia General Reference Map (A4). Available online: https://ecat.ga.gov.au/geonetwork/srv/eng/search#!a05f7892-cff3-7506-e044-00144fdd4fa6 (accessed on 6 April 2018).
- Lambert, S.M. Intestinal parasites in north Queensland. Med. J. Aust. 1921, 1921, 332–336. [Google Scholar]
- Jourdan, P.M.; Lamberton, P.H.L.; Fenwick, A.; Addiss, D.G. Soil-transmitted helminth infections. Lancet 2017, 391, 252–265. [Google Scholar] [CrossRef]
- Page, W.; Judd, J.A.; Bradbury, R.D. The unique life cycle of Strongyloides stercoralis and implications for public health action. Trop. Med. Infect. Dis. 2018, 3, 53. [Google Scholar] [CrossRef]
- Jones, H.I. Intestinal parasite infections in Western Australian Aborigines. Med. J. Aust. 1980, 2, 375–380. [Google Scholar] [PubMed]
- Prociv, P.; Luke, R. Observations on strongyloidiasis in Queensland aboriginal communities. Med. J. Aust. 1993, 158, 160–163. [Google Scholar] [PubMed]
- Requena-Mendez, A.; Chiodini, P.; Bisoffi, Z.; Buonfrate, D.; Gotuzzo, E.; Munoz, J. The laboratory diagnosis and follow up of strongyloidiasis: A systematic review. PLoS Negl. Trop. Dis. 2013, 7, e2002. [Google Scholar] [CrossRef] [PubMed]
- Bisoffi, Z.; Buonfrate, D.; Sequi, M.; Mejia, R.; Cimino, R.O.; Krolewiecki, A.J.; Albonico, M.; Gobbo, M.; Bonafini, S.; Angheben, A.; et al. Diagnostic accuracy of five serologic tests for Strongyloides stercoralis Infection. PLoS Negl. Trop. Dis. 2014, 8, e2640. [Google Scholar] [CrossRef] [PubMed]
- Flannery, G.; White, N. Immunological parameters in northeast Arnhem Land aborigines: Consequences of changing settlement patterns and lifestyles. In Urban Ecology and Health in the Third World; Cambridge University Press: Cambridge, UK, 1993; pp. 202–220. [Google Scholar]
- McDonald, E.L.; Bailie, R.S.; Rumbold, A.R.; Morris, P.S.; Paterson, B.A. Preventing growth faltering among Australian Indigenous children: Implications for policy and practice. Med. J. Aust. 2008, 188 (Suppl. 8), S84. [Google Scholar]
- Gunzburg, S.; Gracey, M.; Burke, V.; Chang, B. Epidemiology and microbiology of diarrhoea in young Aboriginal children in the Kimberley region of Western Australia. Epidemiol. Infect. 1992, 108, 67–76. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yiannakou, J.; Croese, J.; Ashdown, L.R.; Prociv, P. Strongyloidiasis in North Queensland: Re-emergence of a forgotten risk group? Med. J. Aust. 1992, 156, 24–27. [Google Scholar] [PubMed]
- Page, W.A.; Dempsey, K.; McCarthy, J.S. Utility of serological follow-up of chronic strongyloidiasis after anthelminthic chemotherapy. Trans. R. Soc. Trop. Med. Hyg. 2006, 100, 1056–1062. [Google Scholar] [CrossRef] [PubMed]
- Einsedel, L.; Fernandez, L.; Woodman, R.J. Racial disparities in infection-related mortality at Alice Springs Hospital, Central Australia, 2000–2005. Med. J. Aust. 2008, 188, 568–571. [Google Scholar]
- Hays, R.; Esterman, A.; Giacomin, P.; Loukas, A.; McDermott, R. Does Strongyloides stercoralis infection protect against type 2 diabetes in humans? Evidence from Australian Aboriginal adults. Diabetes Res. Clin. Pract. 2015, 107, 355–361. [Google Scholar] [CrossRef] [PubMed]
- Bon, B.; Houze, S.; Talabani, H.; Magne, D.; Belkadi, G.; Develoux, M.; Senghor, Y.; Chandenier, J.; Ancelle, T.; Hennequin, C. Evaluation of a rapid enzyme-linked immunosorbent assay for diagnosis of strongyloidiasis. J. Clin. Microbiol. 2010, 48, 1716–1719. [Google Scholar] [CrossRef] [PubMed]
- Turkeltaub, J.A.; McCarty, T.R., III; Hotez, P.J. The intestinal protozoa: Emerging impact on global health and development. Curr. Opin. Gastroenterol. 2015, 31, 38–44. [Google Scholar] [CrossRef] [PubMed]
- Meloni, D.; Mantini, C.; Goustille, J.; Desoubeaux, G.; Maakaroun-Vermesse, Z.; Chandenier, J.; Gantois, N.; Duboucher, C.; Fiori, P.L.; Deicas, E.; et al. Molecular identification of Pentatrichomonas hominis in two patients with gastrointestinal symptoms. J. Clin. Pathol. 2011, 64, 933–935. [Google Scholar] [CrossRef] [PubMed]
- Calegar, D.A.; Nunes, B.C.; Monteiro, K.J.; Pereira dos Santos, J.; Toma, H.K.; Gomes, T.F.; Lima, M.M.; Boia, M.N.; Carvalho-Costa, F.A. Frequency and molecular characterisation of Entamoeba histolytica, Entamoeba dispar, Entamoeba moshkovskii, and Entamoeba hartmanni in the context of water scarcity in northeastern Brazil. Mem. Inst. Oswaldo Cruz 2016, 111, 114–119. [Google Scholar] [CrossRef] [PubMed]
- Zavala, G.A.; Garcia, O.P.; Campos-Ponce, M.; Ronquillo, D.; Caamano, M.C.; Doak, C.M.; Rosado, J.L. Children with moderate-high infection with Entamoeba coli have higher percentage of body and abdominal fat than non-infected children. Pediatr. Obes. 2016, 11, 443–449. [Google Scholar] [CrossRef] [PubMed]
- Ross, K.E.; Bradbury, R.S.; Garrard, T.A.; O’Donahoo, F.J.; Shield, J.; Page, W.; Miller, A.; Robertson, G.; Judd, J.A.; Speare, R. The National Strongyloides Working Group in Australia 10 workshops on: Commendations and recommendations. Aust. N. Z. J. Public Health 2017, 41, 221–223. [Google Scholar] [CrossRef] [PubMed]
- Hays, R.; Esterman, A.; McDermott, R. Control of chronic Strongyloides stercoralis infection in an endemic community may be possible by pharmacological means alone: Results of a three-year cohort study. PLoS Negl. Trop. Dis. 2017, 11, e0005825. [Google Scholar] [CrossRef] [PubMed]
- Beknazarova, M.; Whiley, H.; Ross, K. Mass drug administration for the prevention of human strongyloidiasis should consider concomitant treatment of dogs. PLoS Negl. Trop. Dis. 2017, 11, e0005735. [Google Scholar] [CrossRef] [PubMed]
- Jaleta, T.G.; Zhou, S.; Bemm, F.M.; Schar, F.; Khieu, V.; Muth, S.; Odermatt, P.; Lok, J.B.; Streit, A. Different but overlapping populations of Strongyloides stercoralis in dogs and humans—Dogs as possible source for zoonotic strongyloidiasis. PLoS Negl. Trop. Dis. 2017, 11, e0005752. [Google Scholar] [CrossRef] [PubMed]
- Bradbury, L.; Corlette, S. Dog health program in Numbulwar, a remote aboriginal community in east Arnhem Land. Aust. Vet. J. 2006, 84, 317–320. [Google Scholar] [CrossRef] [PubMed]
- Caumes, E.; Datry, A.; Mayorga, R.; Gaxotte, P.; Danis, M.; Gentilini, M. Efficacy of ivermectin in the therapy of larva currens. Arch. Dermatol. 1994, 130, 932. [Google Scholar] [CrossRef] [PubMed]
- Wilkins, A.L.; Steer, A.C.; Cranswick, N.; Gwee, A. Is it safe to use ivermectin in children less than five years of age and weighing less than 15 kg? Arch. Dis. Child. 2018, 103, 514–519. [Google Scholar] [CrossRef] [PubMed]

Figure 2.
Age distribution in S. stercoralis seropositive group.

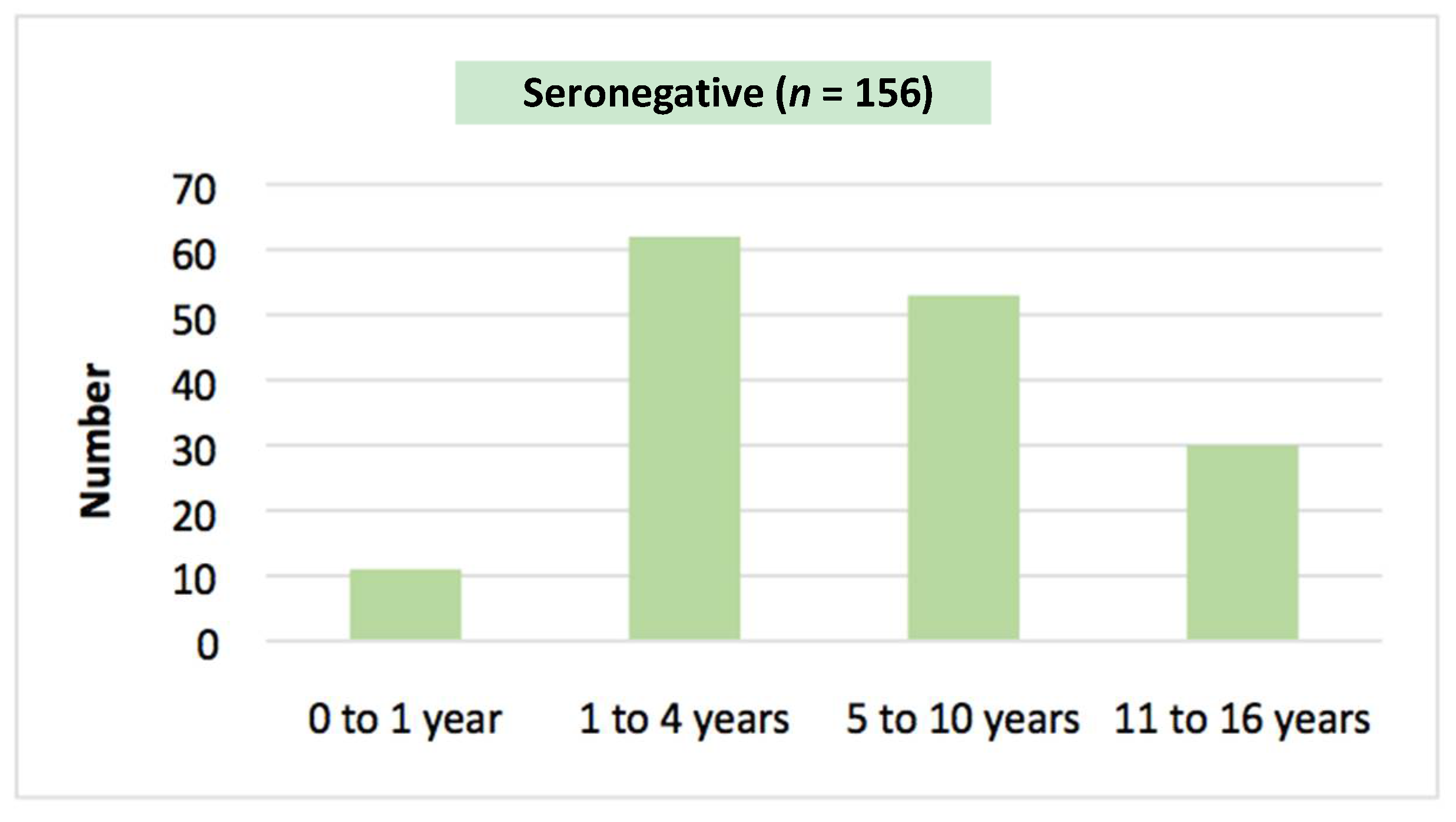
Figure 3.
Age distribution in S. stercoralis seronegative group.

Figure 4.
Clinical features during admission. GIT: Gastrointestinal tract.

Figure 5.
Geographical distribution of seropositive and seronegative cases in Central Australia.

Figure 6.
Community education resources produced by Menzies School of Health Research in English and Yolngu.
Figure 6.
Community education resources produced by Menzies School of Health Research in English and Yolngu.


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Table 1.
Summary of original research describing S. stercoralis epidemiology in endemic areas in Australia.
Table 1.
Summary of original research describing S. stercoralis epidemiology in endemic areas in Australia.
| Author | Location | Sample Size and Demographics | Years Studied | Diagnostic Test | Key Findings |
|---|---|---|---|---|---|
| Frith et al., 1974 [26] | NSW: Central Coast | Not stated | 1966–1967 | Stool examination | 4.7% positive on stool microscopy |
| Jones, 1980 [26] | WA: 20 remote communities | 1683 adults and children | 1973–1978 | Stool microscopy with formol-ether concentration | 2% positive on faecal microscopy Highest infection rate in 15–19 year old age group |
| Prociv and Luke, 1993 [27] | QLD: 122 remote communities | Children <15 years providing 32,145 faecal samples for diagnosis and disease surveillance | 1972–1991 | Stool microscopy with formol-ether concentration | Overall infection prevalence of 1.97% positive Cases found in 52/122 communities Peak prevalence of 27.5% in one area during wet season vs average prevalence of 12% Reduction in prevalence from 26.2% to 7% with thiabendazole treatment of infected children |
| Meloni et al., 1993 [12] | WA: Kimberly region | 247 adults and children in five communities | 1987–1991 | Stool examination | 0.25% positive on microscopy 0.3% in children aged 0 to 13 |
| Gunzburg et al., 1992 [32] | WA: Kimberly region | 104 Indigenous children under 5 years old | Not stated | Stool concentration and microscopy | 1.2% of samples from children with diarrhoea and 2.1% of samples from well children positive |
| Fisher et al., 1993 [13] | NT: Darwin | ~2000 stool samples from adult and paediatric patients | 1991–1992 | Stool examination | 68 cases of S. stercoralis identified 54% of diagnoses were in children under 5 years Eosinophilia noted in 57% of cases |
| Yiannakou et al., 1992 [33] | QLD: Townsville | 14 adult and paediatric cases from 5 year audit | Not stated | Stool examination | 9 Indigenous cases, 2 refugees from Vietnam, 1 returned veteran and 2 non-Indigenous patients with no significant travel history |
| Flannery and White, 1993 [30] | NT: Arnhem Land | 29 participants | Not stated | Single stool microscopy; Serology | 41% positive on faecal microscopy 59.6% positive by serological diagnosis |
| Shield et al., 2015 [15] | NT: Arnhem Land | 314 participants including 129 children; 39 underwent serology | 1994–1996 | Stool microscopy; Serology | 19% positive on microscopy 28% seropositive and 18% equivocal |
| Aland et al., 1996 [11] | NT: Arnhem Land | 300 participants | Not stated | Single stool microscopy | 15% positive on faecal microscopy |
| Page et al., 2006 [34] | NT: Arnhem Land | 508 adult and adolescent participants | 1996–2002 | Serology | 35% positive by serological diagnosis at baseline 78% seroreversion rate of cases with treatment |
| Kukuruzovic et al., 2002 [14] | NT: Darwin | 291 children admitted with diarrhoea and 84 controls | 1998–2000 | Stool examination | 7.2% of stool samples had S. stercoralis detected 87 children with wasting were 6.5 times (95% CI 1.6 to 26.7) more likely to have S. stercoralis Hypokalaemia significantly associated with S. stercoralis infection |
| Einsiedel et al., 2008 [35] | NT: Alice Springs | 206 Indigenous adults admitted with blood stream infections | 2001–2005 | Serology | 35.4% were positive by serological diagnosis |
| Einsiedel and Fernandez, 2008 [5] | NT: Alice Springs | 18 Indigenous adults admitted with severe strongyloidiasis | 2000–2006 | Stool examination; Serology | 7/11 patients with severe disease tested for HTLV-1 were positive |
| Einsiedel et al., 2014 [20] | NT: Alice Springs | 1126 Indigenous adult inpatients | 2000–2010 | Serology | 23.9% positive by serological diagnosis HTLV-1 positive patients trending towards higher seropositivity rates but not significant (p = 0.063) |
| Mayer-Coverdale et al., 2017 [9] | NT: Territory-wide | 22,892 adult and paediatric stool samples provided to NT pathology services | 2002–2012 | Microscopy with formol-ether concentration | 97.7% of cases Indigenous, overall 1.7% positive 42.2% of diagnoses in children under 5 years of age (3–6% positive) Declining rates of diagnosis over time noted |
| Kearns et al., 2017 [16] | NT: Arnhem Land | 859 Indigenous children and adults | 2010–2011 | Microscopy/culture; Serology | 21% seropositive at baseline with 15% equivocal Peak seropositivity in 5–14 year old cohort 89% patients had eosinophilia at baseline 11% had positive faecal microscopy/culture Seroprevalence 2% at 18 months after two mass drug administrations |
| Hays et al., 2015 [36] | WA: Kimberly region | 259 Indigenous adults | 2012–2015 | Serology | 35.3% positive by serological diagnosis (OD > 0.3) Reduction to 5.8% after three years of targeted treatment and follow up of seropositive patients |
Abbreviations: NT: Northern Territory; QLD: Queensland; WA: Western Australia; NSW: New South Wales; OD: optic density; HTLV-1: human T-lymphotrophic virus 1.
Table 2.
Demographic data, clinical presentation, and investigation results.
| Variable | Seronegative (n = 156) Number (%) | Seropositive (n = 30) Number (%) | p Value |
|---|---|---|---|
| Mean Age | 6 years 1 month | 6 years 7 months | p = 0.55 |
| Male Gender | 91 (58.3%) | 22 (73.3%) | p = 0.12 |
| Remote | 109 (69.9%) | 27 (90.0%) | p = 0.02 |
| Indigenous | 149 (95.5%) | 30 (100%) | p = 0.24 |
| Mean serology | N/A | Optic density = 0.84 ± 1.54 | |
| Stool pathogens | 17 (36.2%), n = 47 | 5 (62.5%), n = 8 | p = 0.16 |
| Haemoglobin | 117.63 ± 25.92 g/L | 116.77 ± 27.22 g/L | p = 0.74 |
| Mean corpuscular volume | 76.578 ± 10.18 fL | 76.66 ± 7.72 fL | p = 0.93 |
| Mean eosinophil count * | 0.96 × 109/L ± 2.13 × 109/L (Range 0.5 × 109/L to 5.3 × 109/L) | 1.83 × 109/L ± 1.32 × 109/L (Range 0.6 × 109/L to 4.8 × 109/L) | p < 0.0001 |
| Gastrointestinal symptoms | 40 (25.6%) | 9 (30%) | p = 0.62 |
| Respiratory symptoms | 42 (26.9%) | 7 (23.3%) | p = 0.68 |
| Blood stream infection | 4 (2.6%) | 0 (0%) | p = 0.37 |
| Growth faltering | 25 (16%) | 3 (10%) | p = 0.4 |
| HTLV-1 seroprevalence | 0/10 (0%) | 0/2 (0%) |
* Mean eosinophil count in patients tested for unexplained eosinophilia of ≥0.5 × 109/L (seropositive group n = 29, seronegative group n = 142).
Table 3.
Faecal examination results.
| Seronegative (n = 47/156) Number (%) | Seropositive (n = 8/30) Number (%) | |
|---|---|---|
| Organism/virus identified | 17 (36%) | 5 (62.5%) |
| Strongyloides stercoralis | 0 | 0 |
| Giardia species | 5 | 2 |
| Cryptosporidium parvum | 3 | 2 |
| Blastocystis hominis * | 1 | 0 |
| Trichomonas hominis ** | 1 | 0 |
| Entamoeba coli ** | 1 | 0 |
| Entamoeba hartmanni ** | 1 | 0 |
| Salmonella species | 3 | 0 |
| Campylobacter jejuni | 1 | 0 |
| Norovirus | 4 | 0 |
| Rotavirus | 1 | 0 |
| Adenovirus | 1 | 2 |
| Hymenolepis nana | 1 | 0 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Wilson, A.; Fearon, D. Paediatric Strongyloidiasis in Central Australia. Trop. Med. Infect. Dis. 2018, 3, 64. https://doi.org/10.3390/tropicalmed3020064
AMA Style
Wilson A, Fearon D. Paediatric Strongyloidiasis in Central Australia. Tropical Medicine and Infectious Disease. 2018; 3(2):64. https://doi.org/10.3390/tropicalmed3020064
Chicago/Turabian StyleWilson, Angela, and Deborah Fearon. 2018. "Paediatric Strongyloidiasis in Central Australia" Tropical Medicine and Infectious Disease 3, no. 2: 64. https://doi.org/10.3390/tropicalmed3020064