A Rapid Appraisal of Factors Influencing Praziquantel Treatment Compliance in Two Communities Endemic for Schistosomiasis in Côte d’Ivoire


Abstract
:1. Introduction
2. Material and Methods
2.1. Ethical Approval and Study Setting
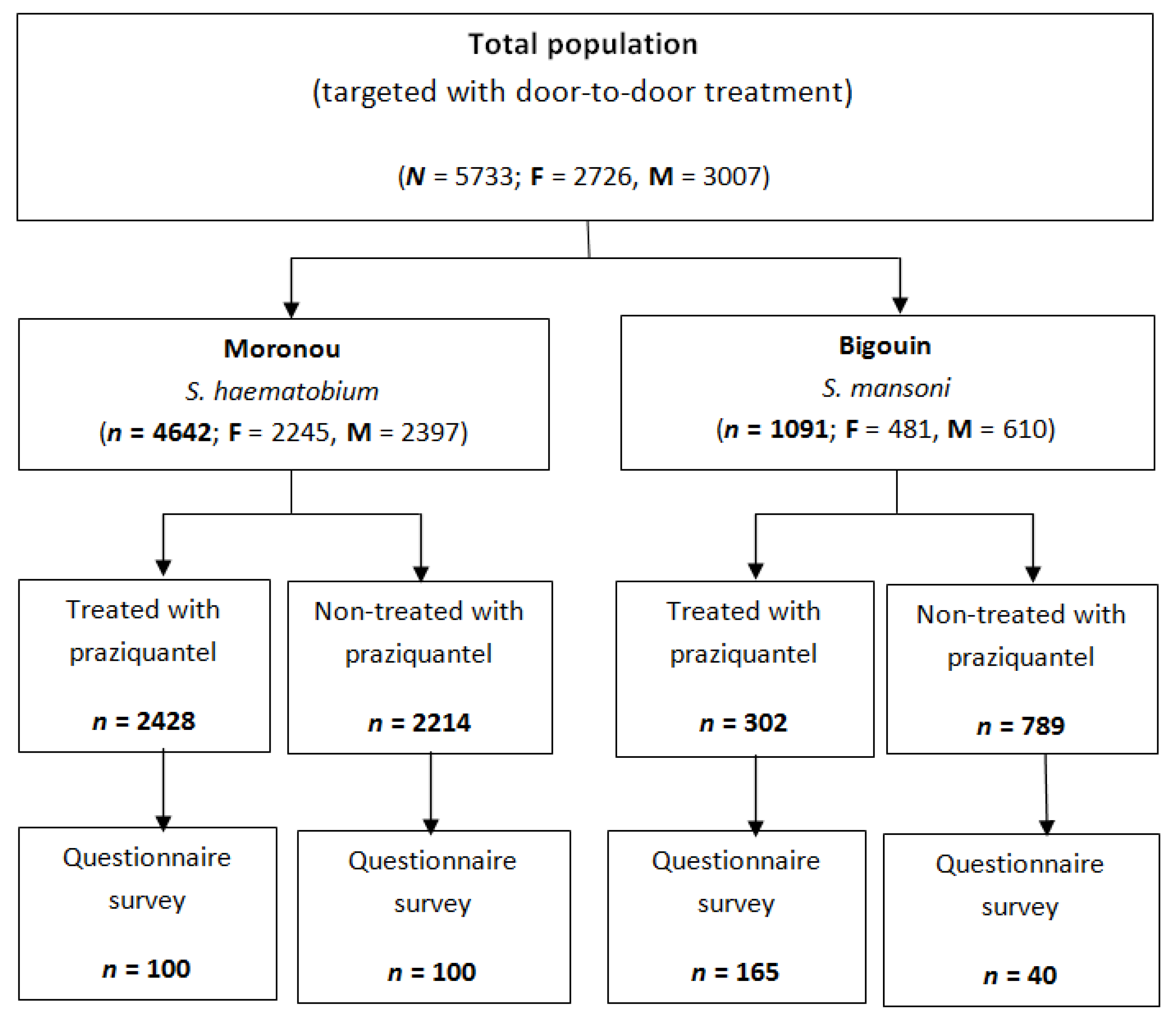
2.2. Sample Size Calculation
2.3. Praziquantel Treatment
2.4. Questionnaire Assessing Factors Influencing Treatment Compliance
2.5. Statistical Analysis
3. Results
3.1. Treatment Compliance
3.2. Factors Associated with Coverage of Praziquantel Treatment
4. Discussion
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Steinmann, P.; Keiser, J.; Bos, R.; Tanner, M.; Utzinger, J. Schistosomiasis and water resources development: Systematic review, meta-analysis, and estimates of people at risk. Lancet Infect. Dis. 2006, 6, 411–425. [Google Scholar] [CrossRef]
- Hotez, P.J.; Alvarado, M.; Basáñez, M.G.; Bolliger, I.; Bourne, R.; Boussinesq, M.; Brooker, S.J.; Brown, A.S.; Buckle, G.; Budke, C.M.; et al. The Global Burden of Disease study 2010: Interpretation and implications for the neglected tropical diseases. PLoS Negl. Trop. Dis. 2014, 8, e2865. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- GBD 2016 DALYs and HALE Collaborators. Global, regional, and national disability-adjusted life-years (DALYs) for 333 diseases and injuries and healthy life expectancy (HALE) for 195 countries and territories, 1990–2016: A systematic analysis for the Global Burden of Disease study 2016. Lancet 2017, 390, 1260–1344. [Google Scholar]
- Hotez, P.J. Mass drug administration and integrated control for the world’s high-prevalence neglected tropical diseases. Clin. Pharmacol. Ther. 2009, 85, 659–664. [Google Scholar] [CrossRef] [PubMed]
- Ezeamama, A.E.; Bustinduy, A.L.; Nkwata, A.K.; Martinez, L.; Pabalan, N.; Boivin, M.J.; King, C.H. Cognitive deficits and educational loss in children with schistosome infection-a systematic review and meta-analysis. PLoS Negl. Trop. Dis. 2018, 12, e0005524. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization (WHO). Prevention and control of schistosomiasis and soil-transmitted helminthiasis: Report of a WHO expert committee. WHO Tech. Rep. Ser. 2002, 912, 1–57. [Google Scholar]
- Savioli, L.; Gabrielli, A.F.; Montresor, A.; Chitsulo, L.; Engels, D. Schistosomiasis control in Africa: 8 years after World Health Assembly resolution 54.19. Parasitology 2009, 136, 1677–1681. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization (WHO). Schistosomiasis: Progress Report 2001–2011 and Strategic Plan 2012–2020; WHO: Geneva, Switzerland, 2013. [Google Scholar]
- World Health Organization (WHO). Schistosomiasis and soil-transmitted helminthiases: Number of people treated in 2016. Wkly. Epidemiol. Rec. 2017, 92, 749–760. [Google Scholar]
- Parker, M.; Allen, T.; Hastings, J. Resisting control of neglected tropical diseases: Dilemmas in the mass treatment of schistosomiasis and soil-transmitted helminths in north-west Uganda. J. Biosoc. Sci. 2008, 40, 161–181. [Google Scholar] [CrossRef] [PubMed]
- Stothard, J.R.; Chitsulo, L.; Kristensen, T.K.; Utzinger, J. Control of schistosomiasis in sub-Saharan Africa: Progress made, new opportunities and remaining challenges. Parasitology 2009, 136, 1665–1675. [Google Scholar] [CrossRef] [PubMed]
- Barda, B.; Coulibaly, J.T.; Puchkov, M.; Huwyler, J.; Hattendorf, J.; Keiser, J. Efficacy and safety of moxidectin, synriam, synriam-praziquantel versus praziquantel against Schistosoma haematobium and S. mansoni infections: A randomized, exploratory phase 2 trial. PLoS Negl. Trop. Dis. 2016, 10, e0005008. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Utzinger, J.; Keiser, J. Research and development for neglected diseases: More is still needed, and faster. Lancet Glob. Health 2013, 1, e317–e318. [Google Scholar] [CrossRef]
- Ross, A.G.P.; Chau, T.N.; Inobaya, M.T.; Olveda, R.M.; Li, Y.; Harn, D.A. A new global strategy for the elimination of schistosomiasis. Int. J. Infect. Dis. 2017, 54, 130–137. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sokolow, S.H.; Wood, C.L.; Jones, I.J.; Lafferty, K.D.; Kuris, A.M.; Hsieh, M.H.; De Leo, G.A. To reduce the global burden of human schistosomiasis, use ‘old fashioned’ snail control. Trends Parasitol. 2018, 34, 23–40. [Google Scholar] [CrossRef] [PubMed]
- Bonfoh, B.; Raso, G.; Koné, I.; Dao, D.; Girardin, O.; Cissé, G.; Zinsstag, J.; Utzinger, J.; Tanner, M. Research in a war zone. Nature 2011, 474, 569–571. [Google Scholar] [CrossRef] [PubMed]
- Tchuem Tchuenté, L.A.; N’Goran, E.K. Schistosomiasis and soil-transmitted helminthiasis control in Cameroon and Côte d’Ivoire: Implementing control on a limited budget. Parasitology 2009, 136, 1739–1745. [Google Scholar] [CrossRef] [PubMed]
- Chami, G.F.; Kontoleon, A.A.; Bulte, E.; Fenwick, A.; Kabatereine, N.B.; Tukahebwa, E.M.; Dunne, D.W. Profiling nonrecipients of mass drug administration for schistosomiasis and hookworm infections: A comprehensive analysis of praziquantel and albendazole coverage in community-directed treatment in Uganda. Clin. Infect. Dis. 2016, 62, 200–207. [Google Scholar] [CrossRef] [PubMed]
- Knopp, S.; Person, B.; Ame, S.M.; Ali, S.M.; Muhsin, J.; Juma, S.; Khamis, I.S.; Rabone, M.; Blair, L.; Fenwick, A.; et al. Praziquantel coverage in schools and communities targeted for the elimination of urogenital schistosomiasis in Zanzibar: A cross-sectional survey. Parasit Vectors 2016, 9, 5. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ross, A.G.P.; Olveda, R.M.; Chy, D.; Olveda, D.U.; Li, Y.; Harn, D.A.; Gray, D.J.; McManus, D.P.; Tallo, V.; Chau, T.N.P.; et al. Can mass drug administration lead to the sustainable control of schistosomiasis? J. Infect. Dis. 2015, 211, 283–289. [Google Scholar] [CrossRef] [PubMed]
- Krentel, A.; Fischer, P.U.; Weil, G.J. A review of factors that influence individual compliance with mass drug administration for elimination of lymphatic filariasis. PLoS Negl. Trop. Dis. 2013, 7, e2447. [Google Scholar] [CrossRef] [PubMed]
- Shuford, K.V.; Turner, H.C.; Anderson, R.M. Compliance with anthelmintic treatment in the neglected tropical diseases control programmes: A systematic review. Parasit Vectors 2016, 9, 29. [Google Scholar] [CrossRef] [PubMed]
- Recensement général de la population et de l’habitat 2014 (RGPH). 2014, p. 26. Available online: http://www.ins.ci/n/documents/RGPH2014_expo_dg.pdf (accessed on 6 June 2018).
- Lemeshow, S.; Hosmer, D.W.J.; Klar, J.; Lwanga, S.K. Adequacy of Sample Size in Health Studies; Wiley: Chichester, UK, 1990; p. 233. [Google Scholar]
- World Health Organization (WHO). Helminth Control in School-Age Children. A Guide for Managers of Control Programmes; WHO: Geneva, Switzerland, 2011. [Google Scholar]
- Montresor, A.; Engels, D.; Chitsulo, L.; Bundy, D.A.P.; Brooker, S.; Savioli, L. Development and validation of a ’tablet pole’ for the administration of praziquantel in sub-Saharan Africa. Trans. R. Soc. Trop. Med. Hyg. 2001, 95, 542–544. [Google Scholar] [CrossRef]
- Colley, D.G.; Bustinduy, A.L.; Secor, W.E.; King, C.H. Human schistosomiasis. Lancet 2014, 383, 2253–2264. [Google Scholar] [CrossRef] [Green Version]
- Lo, N.C.; Addiss, D.G.; Hotez, P.J.; King, C.H.; Stothard, J.R.; Evans, D.S.; Colley, D.G.; Lin, W.; Coulibaly, J.T.; Bustinduy, A.L.; et al. A call to strengthen the global strategy against schistosomiasis and soil-transmitted helminthiasis: The time is now. Lancet Infect. Dis. 2017, 17, e64–e69. [Google Scholar] [CrossRef]
- Rollinson, D.; Knopp, S.; Levitz, S.; Stothard, J.R.; Tchuem Tchuenté, L.A.; Garba, A.; Mohammed, K.A.; Schur, N.; Person, B.; Colley, D.G.; et al. Time to set the agenda for schistosomiasis elimination. Acta Trop. 2013, 128, 423–440. [Google Scholar] [CrossRef] [PubMed]
- Parker, M.; Allen, T. Does mass drug administration for the integrated treatment of neglected tropical diseases really work? Assessing evidence for the control of schistosomiasis and soil-transmitted helminths in Uganda. Health Res. Policy Syst. 2011, 9, 3. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Babu, B.V.; Babu, G.R. Coverage of, and compliance with, mass drug administration under the programme to eliminate lymphatic filariasis in India: A systematic review. Trans. R. Soc. Trop. Med. Hyg. 2014, 108, 538–549. [Google Scholar] [CrossRef] [PubMed]
- Colley, D.G.; Andros, T.S.; Campbell, C.H., Jr. Schistosomiasis is more prevalent than previously thought: What does it mean for public health goals, policies, strategies, guidelines and intervention programs? Infect. Dis. Poverty 2017, 6, 63. [Google Scholar] [CrossRef] [PubMed]
- Burnim, M.; Ivy, J.A.; King, C.H. Systematic review of community-based, school-based, and combined delivery modes for reaching school-aged children in mass drug administration programs for schistosomiasis. PLoS Negl. Trop. Dis. 2017, 11, e0006043. [Google Scholar] [CrossRef] [PubMed]
- Coulibaly, J.T.; N’Gbesso, Y.K.; Knopp, S.; Keiser, J.; N’Goran, E.K.; Utzinger, J. Efficacy and safety of praziquantel in preschool-aged children in an area co-endemic for Schistosoma mansoni and S. haematobium. PLoS Negl. Trop. Dis. 2012, 6, e1917. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Meyer, T.; Sekljic, H.; Fuchs, S.; Bothe, H.; Schollmeyer, D.; Miculka, C. Taste, a new incentive to switch to (R)-praziquantel in schistosomiasis treatment. PLoS Negl. Trop. Dis. 2009, 3, e357. [Google Scholar] [CrossRef] [PubMed]
- Danso-Appiah, A.; Olliaro, P.L.; Donegan, S.; Sinclair, D.; Utzinger, J. Drugs for treating Schistosoma mansoni infection. Cochrane Database Syst. Rev. 2013, CD000528. [Google Scholar] [CrossRef] [PubMed]
- Kramer, C.V.; Zhang, F.; Sinclair, D.; Olliaro, P.L. Drugs for treating urinary schistosomiasis. Cochrane Database Syst. Rev. 2014, CD000053. [Google Scholar] [CrossRef] [PubMed]
- Tuhebwe, D.; Bagonza, J.; Kiracho, E.E.; Yeka, A.; Elliott, A.M.; Nuwaha, F. Uptake of mass drug administration programme for schistosomiasis control in Koome islands, central Uganda. PLoS ONE 2015, 10, e0123673. [Google Scholar] [CrossRef] [PubMed]
- Dabo, A.; Bary, B.; Kouriba, B.; Sankare, O.; Doumbo, O. Factors associated with coverage of praziquantel for schistosomiasis control in the community-direct intervention (CDI) approach in Mali (West Africa). Infect. Dis. Poverty 2013, 2, 11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sangho, H.; Dabo, A.; Sidibe, A.; Dembele, R.; Diawara, A.; Diallo, A.; Konate, S. Coverage rate and satisfaction of populations after mass treatment with praziquantel and albendazole in Mali. Mali Med. 2009, 24, 21–24. [Google Scholar] [PubMed]
- Tallo, V.L.; Carabin, H.; Alday, P.P.; Balolong, E., Jr.; Olveda, R.M.; McGarvey, S.T. Is mass treatment the appropriate schistosomiasis elimination strategy? Bull. World Health Organ. 2008, 86, 765–771. [Google Scholar] [CrossRef] [PubMed]
- Coulibaly, J.T.; N’Gbesso, Y.K.; N’Guessan, N.A.; Winkler, M.S.; Utzinger, J.; N’Goran, E.K. Epidemiology of schistosomiasis in two high-risk communities of south Côte d’Ivoire with particular emphasis on pre-school-aged children. Am. J. Trop. Med. Hyg. 2013, 89, 32–41. [Google Scholar] [CrossRef] [PubMed]
- Gurarie, D.; Yoon, N.; Li, E.; Ndeffo-Mbah, M.; Durham, D.; Phillips, A.E.; Aurelio, H.O.; Ferro, J.; Galvani, A.P.; King, C.H. Modelling control of Schistosoma haematobium infection: Predictions of the long-term impact of mass drug administration in Africa. Parasit Vectors 2015, 8, 529. [Google Scholar] [CrossRef] [PubMed]
- Asaolu, S.O.; Ofoezie, I.E. The role of health education and sanitation in the control of helminth infections. Acta Trop. 2003, 86, 283–294. [Google Scholar] [CrossRef]
- Utzinger, J.; Bergquist, R.; Xiao, S.H.; Singer, B.H.; Tanner, M. Sustainable schistosomiasis control—The way forward. Lancet 2003, 362, 1932–1934. [Google Scholar] [CrossRef]
- Ziegelbauer, K.; Speich, B.; Mäusezahl, D.; Bos, R.; Keiser, J.; Utzinger, J. Effect of sanitation on soil-transmitted helminth infection: Systematic review and meta-analysis. PLoS Med. 2012, 9, e1001162. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yuan, H.; Jiang, Q.; Zhao, G.; He, N. Achievements of schistosomiasis control in China. Mem. Inst. Oswaldo Cruz 2002, 97 (Suppl. 1), 187–189. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
| Characteristic | Total Population | χ2 | p | No. of People Treated | Treatment Coverage % | χ2 | p |
|---|---|---|---|---|---|---|---|
| Bigouin | |||||||
| Male | 610 | 212 | 34.8 | ||||
| Female | 481 | 10.19 | 0.001 | 90 | 18.7 | 19.96 | <0.001 |
| Total | 1091 | 302 | 27.7 | ||||
| Moronou | |||||||
| Male | 2397 | 1266 | 52.8 | ||||
| Female | 2245 | 1162 | 51.8 | 0.16 | 0.104 | ||
| Total | 4642 | 3.32 | 0.069 | 2428 | 52.3 | ||
| Total | 5733 | 2730 | 47.6 | 85.39 | <0.001 | ||
| Participant Characteristics | Moronou (n = 200) | Bigouin (n = 205) | Total (N = 405) | ||||||
|---|---|---|---|---|---|---|---|---|---|
| n (%) | χ2 | p | n (%) | χ2 | p | n (%) | χ2 | p | |
| Sex | |||||||||
| Female | 97 (48.5) | 60 (29.3) | 157 (38.8) | ||||||
| Male | 103 (51.5) | 0.12 | 0.729 | 145 (70.7) | 23.95 | <0.001 | 248 (61.2) | 13.71 | <0.001 |
| Average Age (SD) | |||||||||
| 6–15 years | 11.9 (2.5) | 11.3 (2.2) | 11.6 (2.4) | ||||||
| ≥16 years | 36.6 (14.0) | 40.1 (14.3) | 38.4 (14.3) | ||||||
| Occupation | |||||||||
| Cash crops (cocoa, coffee, hevea) (1) | 107 (53.5) | 100 (48.8) | 207 (51.1) | ||||||
| Vegetable and rice crops (2) | 41 (20.5) | 40 (19.5) | 81 (20.0) | ||||||
| Combined activities (1 & 2) | 18 (9.0) | 50 (24.4) | 68 (16.8) | ||||||
| Other activity (trade, civil servant, etc.) | 34 (17.0) | 66.84 | <0.001 | 15 (7.3) | 57.15 | <0.001 | 49 (12.1) | 109.87 | <0.001 |
| Associated Factor | Moronou (n = 200) | Bigouin (n = 205) | Total (N = 405) | ||||||
|---|---|---|---|---|---|---|---|---|---|
| n (%) | χ2 | p | n (%) | χ2 | p | n (%) | χ2 | p | |
| Accepted Praziquantel Treatment (MDA) | |||||||||
| Yes | 100 (50.0) | 40 (19.5) | 140 (34.6) | ||||||
| No | 100 (50.0) | n.a. | n.a. | 165 (80.5) | 53.00 | <0.001 | 265 (65.4) | 26.00 | <0.001 |
| Reason for Denial of Treatment | n = 100 | n = 165 | n = 265 | ||||||
| Not sick | 4 (4.0) | 13 (7.9) | 17 (6.4) | ||||||
| Adverse events of previous treatment | 25 (25.0) | 3 (1.8) | 28 (10.6) | ||||||
| Busy with field activities | 70 (70.0) | 148 (89.7) | 218 (82.3) | ||||||
| Not informed about the treatment | 1 (1.0) | 87.42 | <0.001 | 1 (0.6) | 237.48 | <0.001 | 2 (0.7) | 306.93 | <0.001 |
| Reason of Treatment’s Acceptance | n = 100 | n = 40 | n = 140 | ||||||
| Sick | 7 (7.0) | 2 (5.0) | 9 (6.4) | ||||||
| Knowledge on schistosomiasis/disease | 68 (68.0) | 11 (27.5) | 79 (56.4) | ||||||
| Emulation | 25 (25.0) | 42.57 | <0.001 | 27 (67.5) | 17.86 | <0.001 | 52 (37.1) | 43.33 | <0.001 |
| What you did not like with the drug? | n = 100 | n = 40 | n = 140 | ||||||
| The taste | 26 (26.0) | 15 (37.5) | 41 (29.3) | ||||||
| The size of the tablet | 12 (12.0) | 4 (10.0) | 16 (11.4) | ||||||
| Adverse events | 62 (62.0) | 28.69 | <0.001 | 21 (52.5) | 8.98 | <0.008 | 63 (45.0) | 22.06 | <0.001 |
| Impact of the drug on your wellbeing | n = 100 | n = 40 | n = 140 | ||||||
| No effect | 15 (15.0) | 4 (10.0) | 19 (13.6) | ||||||
| Improvement | 85 (85.0) | 34.55 | <0.001 | 36 (90.0) | 18.37 | <0.001 | 121 (86.4) | 52.65 | <0.001 |
| Could you accept a new treatment? | n = 100 | n = 40 | n = 140 | ||||||
| Yes | 16 (16.0) | 8 (20.0) | 24 (9.2) | ||||||
| No | 84 (84.0) | 32.50 | <0.001 | 32 (80.0) | 10.00 | <0.002 | 116 (44.4) | 48.61 | <0.001 |
| Appropriate period for the treatment | n = 200 | n = 205 | n = 405 | ||||||
| Rainy season | 2 (1.0) | 7 (3.4) | 9 (2.2) | ||||||
| Dry season | 198 (99.0) | 143.35 | <0.001 | 198 (96.6) | 131.30 | <0.001 | 396 (97.8) | 274.37 | <0.001 |
| Appropriate time for the treatment | n = 200 | n = 205 | n = 405 | ||||||
| Early in the morning | 15 (7.5) | 2 (1.0) | 17 (4.2) | ||||||
| In the evening | 14 (7.0) | 26 (12.7) | 40 (9.9) | ||||||
| At any time, if I am informed | 171 (85.5) | 164.12 | <0.001 | 177 (86.3) | 179.78 | <0.001 | 348 (85.9) | 340.58 | <0.001 |
| What is the best place to facilitate treatment? | n = 200 | n = 205 | n = 405 | ||||||
| Central part of the village | 16 (8.0) | 78 (38.0) | 94 (23.2) | ||||||
| House-to-house distribution | 137 (68.5) | 55 (26.8) | 192 (47.4) | ||||||
| Health centre | 47 (23.5) | 84.39 | <0.001 | 72 (35.1) | 3.19 | 0.200 | 119 (29.4) | 27.90 | <0.001 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Coulibaly, J.T.; Ouattara, M.; Barda, B.; Utzinger, J.; N’Goran, E.K.; Keiser, J. A Rapid Appraisal of Factors Influencing Praziquantel Treatment Compliance in Two Communities Endemic for Schistosomiasis in Côte d’Ivoire. Trop. Med. Infect. Dis. 2018, 3, 69. https://doi.org/10.3390/tropicalmed3020069
Coulibaly JT, Ouattara M, Barda B, Utzinger J, N’Goran EK, Keiser J. A Rapid Appraisal of Factors Influencing Praziquantel Treatment Compliance in Two Communities Endemic for Schistosomiasis in Côte d’Ivoire. Tropical Medicine and Infectious Disease. 2018; 3(2):69. https://doi.org/10.3390/tropicalmed3020069
Chicago/Turabian StyleCoulibaly, Jean T., Mamadou Ouattara, Beatrice Barda, Jürg Utzinger, Eliézer K. N’Goran, and Jennifer Keiser. 2018. "A Rapid Appraisal of Factors Influencing Praziquantel Treatment Compliance in Two Communities Endemic for Schistosomiasis in Côte d’Ivoire" Tropical Medicine and Infectious Disease 3, no. 2: 69. https://doi.org/10.3390/tropicalmed3020069