
Latest Advances in Regional Anaesthesia
by
 , , , and
, , , and
Frances Fallon
1,
Aneurin Moorthy
2,3,
Conor Skerritt
2,
Gillian G. Crowe
4 and
Donal J. Buggy
1,3,5,* 1
Department of Anaesthesia, Mater Misericordiae University Hospital, Eccles St, D07 WKW8 Dublin, Ireland
2
Department of Anaesthesia, National Orthopaedic Hospital Cappagh/Mater Misericordiae University Hospital, Eccles St, D07 WKW8 Dublin, Ireland
3
School of Medicine, University College Dublin, D04 V1W8 Dublin, Ireland
4
Department of Anaesthesia, Cork University Hospital, Wilton, T12 DC4A Cork, Ireland
5
The ESA-IC Oncoanaesthesiology Research Group and Outcomes Research, Cleveland, OH 44195, USA
*
Author to whom correspondence should be addressed.
Medicina 2024, 60(5), 735; https://doi.org/10.3390/medicina60050735
Submission received: 28 March 2024
/
Revised: 22 April 2024
/
Accepted: 26 April 2024
/
Published: 28 April 2024
(This article belongs to the Special Issue Latest Advances in Regional Anesthesia)
{kind=link}
{kind=link}
Abstract
:Training and expertise in regional anaesthesia have increased significantly in tandem with increased interest over the past two decades. This review outlines the most recent advances in regional anaesthesia and focuses on novel areas of interest including fascial plane blocks. Pharmacological advances in the form of the prolongation of drug duration with liposomal bupivacaine are considered. Neuromodulation in the context of regional anaesthesia is outlined as a potential future direction. The growing use of regional anaesthesia outside of the theatre environment and current thinking on managing the rebound plane after regional block regression are also discussed. Recent relevant evidence is summarised, unanswered questions are outlined, and priorities for ongoing investigation are suggested.
1. Introduction
Regional anaesthesia is a subspecialty of anaesthesia which has undergone a renaissance in recent years. Regional anaesthesia is the application of transiently nerve-inhibiting drugs, usually local anaesthetic (LA), to an individual nerve, plexus of nerves, or anatomical plane through which nerves pass, in order to render a distal site (away from the needle site) anaesthetised. It can be used for surgical anaesthesia or analgesia, especially postoperatively. Over the last two decades, a growing appreciation for the application of regional techniques has evolved within the anaesthesia community. This is echoed in the literature with original investigations and new innovations. Since the introduction of ultrasound technology, regional anaesthesia has become more efficacious, safer, and more accessible to anaesthetists in many different fields of work [1]. It is often incorporated as part of a multimodal approach to both anaesthesia and analgesia, with much of its popularity related to its opioid-sparing effects [2]. Its use, particularly in trauma-related injuries, has gained a lot of momentum in recent years. This has seen its application extended to both surgical and non-surgical patients with encouraging data regarding analgesic effects and outcomes for patients [3]. Such is the appreciation for regional anaesthesia, that it has also featured in a number of surgical Enhanced Recovery After Surgery (ERAS) protocols, contributing to reduced recovery times, lengths of stay, and morbidities [4,5]. A trend has emerged in favour of motor-sparing blocks for lower limb surgeries in recent years, and for the role of regional anaesthesia in patients with significant comorbidities undergoing surgery [6,7]. This article will consider some recent advances in regional anaesthesia, including fascial plane blocks, local anaesthetic pharmacology, neuromodulation for acute pain, and regional anaesthesia in non-surgical patients. Finally, we will consider the potential future course of regional anaesthesia and highlight some questions that remain unanswered.
2. Fascial Plane Blocks
The fascial plane has become an anatomical target for regional anaesthesia over the past decade [8]. Fascial plane blocks are characteristically large-volume blocks that target musculofascial planes through which different nerves pass, as opposed to traditional distinct nerve targets. An overall consensus on how these blocks work has yet to be established. It is hypothesised that a number of factors contribute to the mechanism of analgesia: the blockade of both sensory afferent nerves travelling within the fascia and nociceptors in nearby tissue, the systemic absorption of LA, and the inhibition of sympathetic nerves travelling within the fascial plane may have a role [9,10]. The trajectory of these different nerves through fascial planes varies considerably, making the predictability of blockade a challenge [11]. Further adding to the unpredictability of fascial plane blocks is the wide variability of fascia itself. Generally, the effectiveness of a fascial plane block is thought to be influenced by its spread. This spread relies on the anatomical structure of the fascia which is not synonymous across all patients. The composition of fascia is affected by ageing, trauma, and conditions such as diabetes mellitus. Lines of fusion can form secondary to adhesion formation and these too have been theorised as a hindrance to the spread of LA, resulting in an unpredictable block [11].
Despite the lack of a precise in-depth understanding of the mechanism of some fascial plane blocks, evidence of their effectiveness in clinical practice has increased in recent years, as has their popularity [12,13,14]. Chest wall-specific blocks have been shown to be beneficial for patients in breast and thoracic surgery by minimising recovery times and reducing opioid requirements [15,16]. Foremost is the erector spinae (ESP) block which was first described in 2016 [17]. Its popularity continues to increase, largely owing to its relative technical ease and reassuring safety profile. It is a posterior chest wall block that targets the space between the erector spinae muscle sheath and the transverse process of vertebrae [18]. This results in analgesia from the back to the midline of the axilla. The extension of analgesia to the anterior chest may also occur but is unreliable [19]. The primary target of the LA agent is the dorsal rami of the spinal nerve, with extensions to the ventral rami and the intercostal and paravertebral spaces also seen [9,20,21]. As such, the ESP block is often compared with the paravertebral block (PVB), due to their similar target areas, but is associated with fewer complications [13,14]. ESP blocks (Figure 1) are also favoured for the wide anatomical area they can cover with a single injection resulting in effects at multiple vertebral levels: typically three in a cranial and three in a caudal direction [9,21,22,23,24]. For example, evidence shows that an ESP block performed at the level of T5 will result in analgesia from T3–T9 [17]. The block can be performed at all levels of the spine resulting in analgesia to a very wide variety of regions [19]. Another attractive characteristic of this block is its safety profile in the setting of anti-thrombotic drugs. As the ESP block is considered a superficial block, it is safe in patients undergoing such therapies, in contrast with deeper paravertebral or epidural blocks [25,26].
In two randomised controlled trials (RCTs), the ESP block was superior to the serratus anterior plane block for video-assisted thoracoscopic surgery (VATS), including reduced opioid consumption for up to 48 h postoperatively [27,28]. One used the patient-centric outcome quality of recovery-15 score (QoR-15), with ESP patients showing superior quality of recovery and a lower rate of postoperative complications as measured using the Comprehensive Complications Index [27]. The QoR-15 was also the primary outcome in an RCT investigating the effect of ESP block in thoracolumbar decompressive surgery, which showed that compared to no block, patients with bilateral ESP block had improved recovery and reduced pain up to 24 h postoperatively [29]. It was also compared with PVB in VATS, where ESP block was performed by an anaesthetist whilst the video-assisted PVB was performed by a surgeon. Both groups received an initial bolus followed by a continuous infusion of levobupivacaine over 48 h. The results showed a statistically significant improvement in the QoR-15 score at 24 and 48 h postoperatively in favour of the ESP block. No significant difference in opioid consumption was found [30]. A new question for the fascial plane block is whether LA delivered via a programmed intermittent bolus (PIB) regimen is better than via continuous infusion. PIB is well established as superior to continuous infusion in labour epidurals, for example [31]. Our group has just completed an RCT investigating continuous infusion versus intermittent bolus in the setting of ESP block in VATS. This showed the equivalence of QoR-15 and opioid consumption with either PIB or continuous infusion. While the PIB group had a marginally higher QoR-15 at 24 h postoperatively, it was not statistically significant (p = 0.29) [32].
With respect to breast surgery, meta-analyses have demonstrated that ESP block provides better analgesia, decreased pain scores, and statistically significant reduced opioid consumption at 24 h when compared with general anaesthesia alone [14]. The same analysis reported that when compared with PVB, patients with ESP blocks had high pain scores in the first 2 h postoperatively but at no other time point. Opioid consumption did not differ statistically. There was also a higher pooled incidence of pneumothorax in the PVB group (2.58% vs. 0% in the ESP group) [14]. When compared with intercoastal nerve block in thoracic surgery, a single-injection ESP block provided similar analgesia compared to a six-level ultrasound-guided intercostal nerve block with respect to opioid consumption and pain scores postoperatively [33]. Further studies in thoracic surgery are highlighted in a systematic review which identified 6 RCTs comparing ESP in thoracic surgery to either no block or PVB. This analysis showed that in ESP vs. no block, 24 h opioid consumption was reduced significantly in the ESP group but was equivalent when compared with PVB [16].
A number of limitations of facial plane blocks are outlined above including the unpredictability of spread and the anatomical variances that may result in patchy blocks. Circumventing these issues is a challenge that has not been explored extensively yet. It may be argued that current research regarding our understanding of the spread of LA in fascial plane blocks, and regional blocks in general is limited by the subjects in which much of these studies are performed, i.e., cadaveric patients. In these studies, variables such as intrathoracic pressure changes and tissue tension are not easily recreated [11]. Novel approaches to address these limitations are needed, and consensus on what constitutes a successful or failed block would improve consistency. Further clarification is also needed regarding the choice of equipment in fascial plane blocks and the standardisation of technique. Technical factors such as needle size, orientation, and injection pressure are largely underexplored. In addition, the influence of needle endpoint and injection speed has yet to be fully elucidated in these blocks [34]. Considering these are large-volume blocks, a stronger evidence base for optimal dose and concertation for fascial plane blocks would further add to their already promising safety profile [9].
Despite the number of unanswered questions that exist with respect to ESP blocks, there is a widespread appetite for it in the anaesthesia community [12]. With this wave of interest and positivity should also come a degree of caution with respect to publication bias. One narrative review reported that when investigating the clinical uses for ESP block, of 23 RCTs, only 7 were high quality. Weaknesses in the remaining 16 RCTs were attributed to faults such as discrepancies in protocols and errors in registered versus reported protocols [35]. Caution should always be employed without evidence that any new block is at least equivalent or superior to our existing methods [36].
3. Neuromodulation Techniques for Acute Pain
While the concept of neuromodulation is well established in the field of chronic pain, recent advances in the technology are being investigated for its application in the management of acute pain [37]. Neuromodulation is defined as the “modification of neurological function, including both neuronal and glial cell activity, through delivery of an electrical, magnetic or chemical stimulus, to specific neurological targets” [38]. There are many different approaches to neuromodulation including spinal cord stimulation, transcutaneous electrical nerve stimulation (TENS), and peripheral nerve stimulation (PNS) [39,40]. PNS is a method that has gained increasing attention in the field of regional anaesthesia for its application in managing acute postoperative pain [37,41,42,43,44,45]. PNS involves the implantation of electrodes in the close vicinity of a target nerve. An external pulse generator is responsible for the delivery of electrical pulses through the implanted electrode [46]. The last decade has seen the development of minimally invasive percutaneous peripheral nerve stimulation (pPNS), which consists of the ultrasound-guided percutaneous implantation of small (0.2 mm) monopolar, coiled electrical leads [47].
The mechanism by which PNS is understood to work (Figure 2) is largely grounded in the Gate Theory of pain [48,49]. More recently, both alternative and complementary mechanisms have been proposed, including theories at both peripheral and central levels [46,50,51]. At a peripheral level, PNS acts to reduce local inflammatory mediators and blood flow. It has also been shown to downregulate inflammatory neurotransmitters and endorphins, while electrophysiological studies have shown it reduces the transmission of efferent nociception [50,52]. While these mechanisms likely contribute to analgesia, the dominant mechanism of action is believed to be through the stimulation of Aβ fibres. When activated, these inhibit pain transmission at the dorsal root ganglion (DRG) between the first- and second-order neurons via an inhibitory interneuron in the substantia gelatinosa of the spinal cord [53].
In 2018, the Food and Drug Administration approved the use of pPNS for use in acute postoperative pain [41]. It has potentially beneficial qualities with respect to acute pain management including opioid sparing and the absence of sensory, motor, or proprioceptive deficits which may benefit patient rehabilitation [42,43]. The risk of infection is <1 per 32,000 indwelling days, and the leads are approved for use for up to 60 days [54]. Lead placement is typically 1–2 cm away from the target nerve which may reduce the risk of neurological injury [45]. The leads are also a potential limitation, however, because they can fracture or dislodge and may be left in situ [44]. Other questions such as the optimal distance between the lead and target nerve, the implications of tissue impendence, the consistency of electrical current, the and long-term effects of prolonged use remain unanswered [55,56].
A role for pPNS in ambulatory orthopaedic surgery has been proposed in a pilot randomised sham-controlled trial. Preoperatively, a lead was placed percutaneously to target the sciatic nerve for major foot or ankle surgery or anterior cruciate ligament repair. The brachial plexus was targeted for patients undergoing rotator cuff repair. Postoperatively, patients were randomised to a sham or electrical stimulation group via an external pulse generator in a double-blinded approach [45]. The authors concluded that pPNS led to a statistically significant improvement in analgesia and reduced opioid requirement, which lasted for 7 days postoperatively. Of note, all patients in this study received a single-injection peripheral nerve block immediately after the lead implantation and before the start of surgery [45]. Some individuals from the same research team had previously published their findings regarding the use of peripheral nerve stimulators for rotator cuff repair. In this study, patients were randomised to either a stimulation or sham group and did not receive any peripheral nerve block. Eleven of a total of sixteen patients, however, required a rescue block prior to discharge and overall no analgesic effect immediately postoperatively was appreciated [42]. These were small studies limited by a number of technical challenges. Overall, superiority over current methods cannot be inferred from the current research and future comparative studies are warranted.
4. Pharmacological Advances
The pursuit of the pharmacological agent(s) that will result in the “ideal block” continues. With such an agent, one could theoretically prolong a good-quality block duration in a predictable manner without side effects for patients [57]. Duration is one of the greatest limitations of regional anaesthesia and traditional one-injection blocks last for a maximum of 8–14 h [58]. Increasing efforts are being made to address this through both pharmacological and non-pharmacological approaches in the form of catheters [59]. Three main pharmacological avenues have been explored with respect to block prolongation, namely intravenous adjuncts, perineural adjuncts, and sustained-release LA molecules.
Sustained-release LA molecules constitute the most recent advance in pharmacology for regional anaesthesia [60]. Liposomal bupivacaine was approved by the Food and Drug Administration in 2011 for surgical site infiltration. In November 2023, two further indications were approved—adductor canal and sciatic nerve block [61]. The availability of this agent is currently limited and it is costly [62]. Initial studies on liposomal bupivacaine were in the context of local infiltration [63]. Liposomal bupivacaine was compared with bupivacaine hydrochloride in interscalene block where “modest” effects in favour of the liposomal agent were reported in the highest pain scores during the first week postoperatively [64]. A meta-analysis investigating liposomal versus non-liposomal bupivacaine for peripheral nerve blockade encompassing nine trials had a primary outcome of the difference in rest pain score 24–72 h post-blockade. Liposomal bupivacaine did not meet the predefined threshold for clinical significance. For all other secondary outcomes, liposomal bupivacaine was similar to non-liposomal [65]. Therefore, there seems to be no benefit of liposomal agents over current drugs, and this combined with their high cost makes them unlikely to be adopted in the near future.
5. Regional Anaesthesia outside the Operating Theatre
The expansion in regional anaesthesia techniques in recent years is appreciated both inside and outside the surgical theatre environment. Regional anaesthesia has become well established outside of the theatre environment, both in the emergency department and through the establishment of acute pain services. In emergency departments, regional techniques can be used for the management of pain relating to trauma such as rib and hip fractures. This has been shown to have positive effects with respect to opioid use, patient satisfaction, and hospital length of stay [24,66,67]. An acute pain service is an integral function in large institutions dealing with major surgery and trauma [68]. The administration of opioids has long been the mainstay analgesic strategy for acute trauma; however, the inappropriate and prolonged use of opioids may be an important factor implicated in the current opioid epidemic [69,70,71]. An acute pain service plays a critical role in ensuring appropriate opioid prescribing stewardship and early regional anaesthesia interventions which provide immediate, short and long-term benefits [3].
An acute pain service is not limited to surgical patients and may also manage injuries that warrant conservative management. Equally, these injuries may be managed earlier in a patient’s presentation by non–anaesthetists in the emergency department [24]. Examples of such injuries include, but are not limited to rib fractures, pubic rami fractures, clavicle fractures, and soft tissue injuries. Rib fractures are associated with increased morbidity and mortality, especially among the elderly. In the majority of cases, treatment is conservative and satisfactory analgesia is paramount to prevent associated respiratory complications [72]. For some time, thoracic epidural has been considered the “gold-standard” regional anaesthesia technique for managing severe pain in this patient cohort [73]. One of the useful features it offers is bilateral analgesia after a single procedure [74]. However, its use is limited by a number of contraindications such as coagulopathy and the presence of paraspinal infection [26,75]. However, in comparison to a thoracic epidural, ESP block is a fascial plane block with a needle injection site far away from the epidural space. Therefore, the risk of a devastating neuraxial haematoma following the insertion of an ESP catheter in the presence of coagulopathy is very rare and, thus, offers a more favourable safety profile [26]. Early retrospective studies highlighted that ESP block improves pulmonary function, pain scores, and opioid requirements in trauma patients [76,77]. ESP catheter use has been well received by patients, with one small quality assurance initiative report involving 29 patients highlighting that patient satisfaction was dramatically improved after the placement of an ESP catheter [78].
A small RCT (n = 50 patients) demonstrated that continuous ESP block was equivalent to thoracic epidural analgesia for thoracic trauma with respect to a number of parameters including analgesic effect and pulmonary function. The only statistically significant difference between the two interventions was a lower recorded mean arterial pressure in the epidural group (p < 0.001) [79]. Incorporating a continuous ESP catheter as part of a multimodal analgesia appears to be a promising intervention in thoracic trauma patients but at present, there is a lack of high-quality level 1 evidence to support this. A large multicentre RCT (ESPEAR TRIAL) is currently underway, comparing the continuous ESP catheter technique plus multimodal analgesia versus sham ESP catheter plus multimodal analgesia [80]. Results from this trial should further guide the role of regional anaesthesia in thoracic trauma.
Another example of an orthopaedic traumatic injury, often managed conservatively, is pubic rami fractures. This type of pelvic injury is commonly encountered in patients who are female, 80 years of age or older, and have a history of osteoporosis; and it may occur in low- or high-energy traumas [81,82]. Pain associated with this type of injury can be very severe and limits mobilisation. Regional anaesthesia for this injury is challenging because of the desired goal of adequate analgesia while avoiding inadvertent motor block. With this in mind, the pericapsular nerve group (PENG) block may possibly have a role. The PENG block is a novel fascial plane block recently described and utilised as an analgesic option for traumatic hip fractures and for elective hip arthroplasty [83,84]. This nerve block targets the articular branches of the femoral, obturator, and accessory obturator nerves to the hip capsule while sparing the motor branches [85]. A recent case report described the successful implementation of this block by an acute pain service for a patient with traumatic superior and inferior public rami fractures, allowing the patient to mobilise [86]. This finding is echoed in another case series of PENG blocks for pelvic bone fractures, involving in one case an inferior pubic rami fracture and in another case both superior and inferior public rami fractures. Both cases in this series were regarding blocks carried out by emergency medicine physicians [87]. Further studies examining the PENG block for this indication are warranted. However, this technique requires rigorous evaluation in an RCT comparing its efficacy and safety with an established regional technique such as ilioinguinal and iliohypogastric blocks combined.
6. Rebound Pain after Regional Anaesthesia
A significant challenge that is largely unaddressed in regional anaesthesia is rebound pain. Rebound pain is a transient acute, clinically significant pain that arises upon the regression of a peripheral nerve block [88]. Its incidence is unclear, but given the increase in regional anaesthesia use, it is likely to be common. The phenomenon of rebound pain is not fully understood but is associated with single-injection peripheral nerve blocks, and frequently occurs at night, which may be explained by a daytime block regressing after 6–12 h [89]. A question regarding rebound pain remains unanswered—is it due to the re-emergence of previously blocked surgical pain, or is it an exaggerated nociceptive response somehow caused by regional anaesthesia? Patient factors, systemic inflammation, brain cortical processing, surgical factors, and regional anaesthetic techniques have all been hypothesised as explanations [90].
Continuous catheter techniques may mitigate rebound pain by prolonging block effects long enough to allow for more healing, reduced inflammation, and a less sudden offset of analgesia [90,91]. A randomised control trial of patients (n = 71) undergoing rotator cuff repair had three arms: general anaesthesia only, single regional interscalene injection, or continuous catheter interscalene block. The general anaesthesia-only patients received a standardised general anaesthetic. The single-injection block group received 20 mL of 0.5% ropivacaine through a needle. The continuous catheter group received the same initial 20 mL block through a catheter followed by a continuous infusion of 0.2% ropivacaine at 5 mL/h with a patient-controlled bolus of 5 mL hourly for 48 h. The data were collected on postoperative days 1, 2, 3, and 7. Severe pain, i.e., 8–10 on a numerical rating scale (NRS) on day 1 postoperatively was reported in 40%, 78%, and 15% in these respective groups. On day 2 postoperatively, the trend in favour of the continuous catheter continued with just 10% reporting severe pain compared to 35% in the other two groups. By the end of the seven days, just 26% of patients with a continuous catheter had reported NRS ≥4 compared to 58% in the general anaesthesia group, and 83% in the single-injection group (p ≤ 0.05) [92]. Continuous catheter techniques, however, are technically challenging, are associated with complications such as failure and infection, and are labour-intensive to manage making them less accessible in some circumstances [93].
Efforts to optimise catheter techniques are ongoing. Until recently, the most common technique of using regional anaesthesia catheters was by continuous infusion or patient-controlled boluses. Whether programmed intermittent bolusing is advantageous remains uninvestigated [94]. Nuanced approaches such as using start-delay timers have been proposed for their ability to prolong the duration of analgesia [95]. A retrospective study among patients undergoing wrist surgery receiving a continuous infraclavicular block suggested that after an initial bolus, the delayed onset of LA infusion maximised LA availability and prolonged the block. This proposal warrants an RCT [96].
7. Future Directions
The interest that regional anaesthesia has generated amongst anaesthetists is reflected in the growing memberships of societies such as the European Society of Regional Anaesthesia (ESRA) [97,98]. As the weight of supporting evidence for the use of regional anaesthesia has grown in recent years, so too has the emphasis on its integration into core teaching as part of the anaesthesia training systems both in the UK and Ireland [99,100]. While regional anaesthesia in the past was often limited to enthusiasts, it is now evolving into an expected component of a trained anaesthetist’s skillset. The UK’s “plan A blocks” concept focuses training on a core set of well-established blocks that serve as a basic skillset for the trainee anaesthetist to improve patient outcomes [36]. Given its relative lack of technical complexity, the ESP block is one of the seven such plan A blocks, and yet, when surveyed, trainee anaesthetists reported that only 10% of them felt confident about performing an ESP block with remote supervision compared to 60% for axillary blocks [101]. Future anaesthesiology training programmes should aim to deliver competency in the basic skills of ultrasound, needling technique, and core blocks.
Given the rate at which artificial intelligence is developing across all systems across the globe, its role in regional anaesthesia will likely increase in the future. Indeed, a number of recent publications have already looked at the role of such technologies in regional anaesthesia education and training [102,103]. Image interpretation is essential for successful and safe regional anaesthesia. Assistive technology has the potential to aid in defining structures and identifying targets using colour overlay. This is something that has briefly been explored in small studies thus far [103,104]. Future technology may enhance psychomotor competencies such as needle visualisation, image optimisation, image interpretation, and mapping the spread of LA. Just as ultrasound led to increased uptake and improved outcomes in regional anaesthesia, new technology might potentially add further improvement. Quality control and rigorous RCTs should remain the priority for regional anaesthesia developments [104].
Author Contributions
Manuscript concept design: A.M., C.S. and D.J.B. Literature review: F.F. Manuscript writing: F.F., A.M., C.S. and D.J.B. Development of illustrations: G.G.C. Critical revisions of the manuscript: F.F., A.M. and D.J.B. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Mariano, E.R.; Marshall, Z.J.; Urman, R.D.; Kaye, A.D. Ultrasound and its evolution in perioperative regional anesthesia and analgesia. Best Pract. Res. Clin. Anaesthesiol. 2014, 28, 29–39. [Google Scholar] [CrossRef]
- O’Neill, A.; Lirk, P. Multimodal Analgesia. Anesthesiol. Clin. 2022, 40, 455–468. [Google Scholar] [CrossRef]
- Choi, J.J.; Lin, E.; Gadsden, J. Regional anesthesia for trauma outside the operating theatre. Curr. Opin. Anesthesiol. 2013, 26, 495–500. [Google Scholar] [CrossRef] [PubMed]
- Mancel, L.; Van Loon, K.; Lopez, A.M. Role of regional anesthesia in Enhanced Recovery After Surgery (ERAS) protocols. Curr. Opin. Anesthesiol. 2021, 34, 616–625. [Google Scholar] [CrossRef]
- Simpson, J.C.; Bao, X.; Agarwala, A. Pain Management in Enhanced Recovery after Surgery (ERAS) Protocols. Clin. Colon Rectal Surg. 2019, 32, 121–128. [Google Scholar] [CrossRef] [PubMed]
- Admiraal, M.; Marhofer, P.; Hopkins, P.M.; Hollmann, M.W. Peripheral regional anaesthesia and outcomes: A narrative review of the literature from 2013 to 2023. Br. J. Anaesth. 2023, 132, 1082–1096. [Google Scholar] [CrossRef]
- Chin, K.; Mariano, E.; El-Boghdadly, K. Advancing towards the next frontier in regional anaesthesia. Anaesthesia 2021, 76, 3–7. [Google Scholar] [CrossRef]
- Huang, X.; Zeng, Y.; Sandeep, B.; Yang, J. Clinical impact of fascial plane blocks: Defining the research agenda. Br. J. Anaesth. 2023, 131, e180–e183. [Google Scholar] [CrossRef] [PubMed]
- Chin, K.; Versyck, B.; Pawa, A. Ultrasound-guided fascial plane blocks of the chest wall: A state-of-the-art review. Anaesthesia 2021, 76, 110–126. [Google Scholar] [CrossRef]
- Dam, M.; Moriggl, B.; Hansen, C.K.; Hoermann, R.; Bendtsen, T.F.; Børglum, J. The pathway of injectate spread with the transmuscular quadratus lumborum block: A cadaver study. Anesth. Analg. 2017, 125, 303–312. [Google Scholar] [CrossRef]
- Black, N.D.; Stecco, C.; Chan, V.W. Fascial plane blocks: More questions than answers? Anesth. Analg. 2021, 132, 899–905. [Google Scholar] [CrossRef] [PubMed]
- De Cassai, A.; Geraldini, F.; Mariano, E.R.; Kou, A.; Matava, C. Believe the hype? An evaluation of Twitter activity and publication trends related to the erector spinae plane block. J. Clin. Anesth. 2021, 75, 110499. [Google Scholar] [CrossRef] [PubMed]
- Koo, C.-H.; Lee, H.-T.; Na, H.-S.; Ryu, J.-H.; Shin, H.-J. Efficacy of erector spinae plane block for analgesia in thoracic surgery: A systematic review and meta-analysis. J. Cardiothorac. Vasc. Anesth. 2022, 36, 1387–1395. [Google Scholar] [CrossRef] [PubMed]
- Leong, R.; Tan, E.; Wong, S.; Tan, K.; Liu, C. Efficacy of erector spinae plane block for analgesia in breast surgery: A systematic review and meta-analysis. Anaesthesia 2021, 76, 404–413. [Google Scholar] [CrossRef] [PubMed]
- De Cassai, A.; Bonvicini, D.; Correale, C.; Sandei, L.; Tulgar, S.; Tonetti, T. Erector spinae plane block: A systematic qualitative review. Minerva Anestesiol. 2019, 85, 308–319. [Google Scholar] [CrossRef] [PubMed]
- Huang, W.; Wang, W.; Xie, W.; Chen, Z.; Liu, Y. Erector spinae plane block for postoperative analgesia in breast and thoracic surgery: A systematic review and meta-analysis. J. Clin. Anesth. 2020, 66, 109900. [Google Scholar] [CrossRef] [PubMed]
- Forero, M.; Adhikary, S.D.; Lopez, H.; Tsui, C.; Chin, K.J. The erector spinae plane block: A novel analgesic technique in thoracic neuropathic pain. Reg. Anesth. Pain Med. 2016, 41, 621–627. [Google Scholar] [CrossRef] [PubMed]
- Kwon, H.-M.; Kim, D.-H.; Jeong, S.-M.; Choi, K.T.; Park, S.; Kwon, H.-J.; Lee, J.-H. Does erector spinae plane block have a visceral analgesic effect?: A randomized controlled trial. Sci. Rep. 2020, 10, 8389. [Google Scholar] [CrossRef]
- Pawa, A.; King, C.; Thang, C.; White, L. Erector spinae plane block: The ultimate ‘plan A’block? Br. J. Anaesth. 2023, 130, 497–502. [Google Scholar] [CrossRef]
- Dautzenberg, K.H.; Zegers, M.J.; Bleeker, C.P.; Tan, E.C.; Vissers, K.C.; van Geffen, G.-J.; van der Wal, S.E. Unpredictable injectate spread of the erector spinae plane block in human cadavers. Anesth. Analg. 2019, 129, e163–e166. [Google Scholar] [CrossRef]
- Jinn, C.K.; Kariem, E.-B. Mechanisms of action of the erector spinae plane (ESP) block: A narrative review. Can. J. Anesth. 2021, 68, 387–408. [Google Scholar]
- Yang, H.M.; Choi, Y.; Kwon, H.J.; O, J.; Cho, T.; Kim, S. Comparison of injectate spread and nerve involvement between retrolaminar and erector spinae plane blocks in the thoracic region: A cadaveric study. Anaesthesia 2018, 73, 1244–1250. [Google Scholar] [CrossRef] [PubMed]
- Adhikary, S.D.; Bernard, S.; Lopez, H.; Chin, K.J. Erector spinae plane block versus retrolaminar block: A magnetic resonance imaging and anatomical study. Reg. Anesth. Pain Med. 2018, 43, 756–762. [Google Scholar] [CrossRef] [PubMed]
- Malik, A.; Thom, S.; Haber, B.; Sarani, N.; Ottenhoff, J.; Jackson, B.; Rance, L.; Ehrman, R. Regional anesthesia in the emergency department: An overview of common nerve block techniques and recent literature. Curr. Emerg. Hosp. Med. Rep. 2022, 10, 54–66. [Google Scholar] [CrossRef]
- Kietaibl, S.; Ferrandis, R.; Godier, A.; Llau, J.; Lobo, C.; Macfarlane, A.J.; Schlimp, C.J.; Vandermeulen, E.; Volk, T.; von Heymann, C. Regional anaesthesia in patients on antithrombotic drugs: Joint ESAIC/ESRA guidelines. Eur. J. Anaesthesiol. | EJA 2022, 39, 100–132. [Google Scholar] [CrossRef] [PubMed]
- Horlocker, T.T.; Vandermeuelen, E.; Kopp, S.L.; Gogarten, W.; Leffert, L.R.; Benzon, H.T. Regional anesthesia in the patient receiving antithrombotic or thrombolytic therapy: American Society of Regional Anesthesia and Pain Medicine Evidence-Based Guidelines. Obstet. Anesth. Dig. 2019, 39, 28–29. [Google Scholar] [CrossRef]
- Finnerty, D.T.; McMahon, A.; McNamara, J.R.; Hartigan, S.D.; Griffin, M.; Buggy, D.J. Comparing erector spinae plane block with serratus anterior plane block for minimally invasive thoracic surgery: A randomised clinical trial. Br. J. Anaesth. 2020, 125, 802–810. [Google Scholar] [CrossRef] [PubMed]
- Ekinci, M.; Ciftci, B.; Gölboyu, B.E.; Demiraran, Y.; Bayrak, Y.; Tulgar, S. A randomized trial to compare serratus anterior plane block and erector spinae plane block for pain management following thoracoscopic surgery. Pain Med. 2020, 21, 1248–1254. [Google Scholar] [CrossRef] [PubMed]
- Finnerty, D.; Ní Eochagáin, A.; Ahmed, M.; Poynton, A.; Butler, J.; Buggy, D. A randomised trial of bilateral erector spinae plane block vs. no block for thoracolumbar decompressive spinal surgery. Anaesthesia 2021, 76, 1499–1503. [Google Scholar] [CrossRef]
- Moorthy, A.; Eochagáin, A.N.; Dempsey, E.; Wall, V.; Marsh, H.; Murphy, T.; Fitzmaurice, G.J.; Naughton, R.A.; Buggy, D.J. Postoperative recovery with continuous erector spinae plane block or video-assisted paravertebral block after minimally invasive thoracic surgery: A prospective, randomised controlled trial. Br. J. Anaesth. 2023, 130, e137–e147. [Google Scholar] [CrossRef]
- Tan, H.S.; Zeng, Y.; Qi, Y.; Sultana, R.; Tan, C.W.; Sia, A.T.; Sng, B.L.; Siddiqui, F.J. Automated mandatory bolus versus basal infusion for maintenance of epidural analgesia in labour. Cochrane Database Syst. Rev. 2023, 5, CD011344. [Google Scholar]
- Eochagain, A.N.; Moorthy, A.; O’Gara, A.; Buggy, D.J. Ultrasound-guided, continuous erector spinae plane (ESP) block in minimally invasive thoracic surgery-comparing programmed intermittent bolus (PIB) vs continuous infusion on quality of recovery and postoperative respiratory function: A double-blinded randomised controlled trial. Trials 2022, 23, 792. [Google Scholar] [CrossRef] [PubMed]
- Chen, N.; Qiao, Q.; Chen, R.; Xu, Q.; Zhang, Y.; Tian, Y. The effect of ultrasound-guided intercostal nerve block, single-injection erector spinae plane block and multiple-injection paravertebral block on postoperative analgesia in thoracoscopic surgery: A randomized, double-blinded, clinical trial. J. Clin. Anesth. 2020, 59, 106–111. [Google Scholar] [CrossRef] [PubMed]
- Behr, A.U.; Chan, V.W.; Stecco, C. Living versus cadaver fascial plane injection. Reg. Anesth. Pain Med. 2019, 45, 157–158. [Google Scholar] [CrossRef]
- Saadawi, M.; Layera, S.; Aliste, J.; Bravo, D.; Leurcharusmee, P.; Tran, D.Q. Erector spinae plane block: A narrative review with systematic analysis of the evidence pertaining to clinical indications and alternative truncal blocks. J. Clin. Anesth. 2021, 68, 110063. [Google Scholar] [CrossRef]
- Turbitt, L.; Mariano, E.; El-Boghdadly, K. Future directions in regional anaesthesia: Not just for the cognoscenti. Anaesthesia 2020, 75, 293–297. [Google Scholar] [CrossRef] [PubMed]
- Tsui, B.C.; Gupta, R.K. Role of neuromodulation in acute pain settings. Reg. Anesth. Pain Med. 2023, 48, 338–342. [Google Scholar] [CrossRef] [PubMed]
- North, R.B.; Lempka, S.F.; Guan, Y.; Air, E.L.; Poree, L.R.; Shipley, J.; Arle, J.; Rigoard, P.; Thomson, S. Glossary of neurostimulation terminology: A collaborative neuromodulation foundation, institute of neuromodulation, and international neuromodulation society project. Neuromodul. Technol. Neural Interface 2022, 25, 1050–1058. [Google Scholar] [CrossRef] [PubMed]
- Deer, T.R.; Mekhail, N.; Provenzano, D.; Pope, J.; Krames, E.; Leong, M.; Levy, R.M.; Abejon, D.; Buchser, E.; Burton, A. The appropriate use of neurostimulation of the spinal cord and peripheral nervous system for the treatment of chronic pain and ischemic diseases: The Neuromodulation Appropriateness Consensus Committee. Neuromodul. Technol. Neural Interface 2014, 17, 515–550. [Google Scholar] [CrossRef]
- Wang, J.; Chen, Z. Neuromodulation for pain management. Neural Interface Front. Appl. 2019, 1101, 207–223. [Google Scholar]
- Ilfeld, B.M.; Finneran, J.J., IV. Cryoneurolysis and percutaneous peripheral nerve stimulation to treat acute pain: A narrative review. Anesthesiology 2020, 133, 1127–1149. [Google Scholar] [CrossRef] [PubMed]
- Ilfeld, B.M.; Finneran, J.J.; Gabriel, R.A.; Said, E.T.; Nguyen, P.L.; Abramson, W.B.; Khatibi, B.; Sztain, J.F.; Swisher, M.W.; Jaeger, P. Ultrasound-guided percutaneous peripheral nerve stimulation: Neuromodulation of the suprascapular nerve and brachial plexus for postoperative analgesia following ambulatory rotator cuff repair. A proof-of-concept study. Reg. Anesth. Pain Med. 2019, 44, 310–318. [Google Scholar] [CrossRef]
- Ilfeld, B.M.; Gabriel, R.A.; Said, E.T.; Monahan, A.M.; Sztain, J.F.; Abramson, W.B.; Khatibi, B.; Finneran, J.J.; Jaeger, P.T.; Schwartz, A.K. Ultrasound-guided percutaneous peripheral nerve stimulation: Neuromodulation of the sciatic nerve for postoperative analgesia following ambulatory foot surgery, a proof-of-concept study. Reg. Anesth. Pain Med. 2018, 43, 580–589. [Google Scholar] [CrossRef] [PubMed]
- Ilfeld, B.M.; Grant, S.A. Ultrasound-guided percutaneous peripheral nerve stimulation for postoperative analgesia: Could neurostimulation replace continuous peripheral nerve blocks? Reg. Anesth. Pain Med. 2016, 41, 720–722. [Google Scholar] [CrossRef]
- Ilfeld, B.M.; Plunkett, A.; Vijjeswarapu, A.M.; Hackworth, R.; Dhanjal, S.; Turan, A.; Cohen, S.P.; Eisenach, J.C.; Griffith, S.; Hanling, S. Percutaneous peripheral nerve stimulation (neuromodulation) for postoperative pain: A randomized, sham-controlled pilot study. Anesthesiology 2021, 135, 95–110. [Google Scholar] [CrossRef] [PubMed]
- Ong Sio, L.C.; Hom, B.; Garg, S.; Abd-Elsayed, A. Mechanism of action of peripheral nerve stimulation for chronic pain: A narrative review. Int. J. Mol. Sci. 2023, 24, 4540. [Google Scholar] [CrossRef] [PubMed]
- Gabriel, R.A.; Swisher, M.W.; Ilfeld, B.M. Percutaneous peripheral nerve stimulation for acute postoperative pain. Pain Manag. 2019, 9, 347–354. [Google Scholar] [CrossRef]
- Melzack, R.; Wall, P.D. Pain mechanisms: A new theory. Surv. Anesthesiol. 1967, 11, 89–90. [Google Scholar] [CrossRef]
- Mendell, L.M. Constructing and deconstructing the gate theory of pain. Pain® 2014, 155, 210–216. [Google Scholar] [CrossRef]
- Lin, T.; Gargya, A.; Singh, H.; Sivanesan, E.; Gulati, A. Mechanism of Peripheral Nerve Stimulation in Chronic Pain. Pain Med. 2020, 21 (Suppl. S1), S6–S12. [Google Scholar] [CrossRef]
- Meyer-Frießem, C.H.; Wiegand, T.; Eitner, L.; Maier, C.; Mainka, T.; Vollert, J.; Enax-Krumova, E.K. Effects of spinal cord and peripheral nerve stimulation reflected in sensory profiles and endogenous pain modulation. Clin. J. Pain 2019, 35, 111–120. [Google Scholar] [CrossRef] [PubMed]
- Papuć, E.; Rejdak, K. The role of neurostimulation in the treatment of neuropathic pain. Ann. Agric. Environ. Med. 2013, 1, 14–17. [Google Scholar]
- Melzack, R.; Wall, P.D. Pain Mechanisms: A New Theory: A gate control system modulates sensory input from the skin before it evokes pain perception and response. Science 1965, 150, 971–979. [Google Scholar] [CrossRef] [PubMed]
- Ilfeld, B.M.; Gabriel, R.A.; Saulino, M.F.; Chae, J.; Peckham, P.H.; Grant, S.A.; Gilmore, C.A.; Donohue, M.C.; deBock, M.G.; Wongsarnpigoon, A. Infection rates of electrical leads used for percutaneous neurostimulation of the peripheral nervous system. Pain Pract. 2017, 17, 753–762. [Google Scholar] [CrossRef] [PubMed]
- Strand, N.H.; D’Souza, R.; Wie, C.; Covington, S.; Maita, M.; Freeman, J.; Maloney, J. Mechanism of action of peripheral nerve stimulation. Curr. Pain Headache Rep. 2021, 25, 47. [Google Scholar] [CrossRef] [PubMed]
- Deer, T.R.; Naidu, R.; Strand, N.; Sparks, D.; Abd-Elsayed, A.; Kalia, H.; Hah, J.M.; Mehta, P.; Sayed, D.; Gulati, A. A review of the bioelectronic implications of stimulation of the peripheral nervous system for chronic pain conditions. Bioelectron. Med. 2020, 6, 9. [Google Scholar] [CrossRef]
- Desai, N.; Kirkham, K.; Albrecht, E. Local anaesthetic adjuncts for peripheral regional anaesthesia: A narrative review. Anaesthesia 2021, 76, 100–109. [Google Scholar] [CrossRef]
- Fredrickson, M.J.; Abeysekera, A.; White, R. Randomized study of the effect of local anesthetic volume and concentration on the duration of peripheral nerve blockade. Reg. Anesth. Pain Med. 2012, 37, 495–501. [Google Scholar] [CrossRef]
- Albrecht, E.; Chin, K. Advances in regional anaesthesia and acute pain management: A narrative review. Anaesthesia 2020, 75, e101–e110. [Google Scholar] [CrossRef] [PubMed]
- Prabhakar, A.; Ward, C.T.; Watson, M.; Sanford, J.; Fiza, B.; Moll, V.; Kaye, R.J.; Hall, O.M.; Cornett, E.M.; Urman, R.D. Liposomal bupivacaine and novel local anesthetic formulations. Best Pract. Res. Clin. Anaesthesiol. 2019, 33, 425–432. [Google Scholar] [CrossRef]
- Biosciences, P. Pacira Announces FDA Approval of Expanded Exparel Label to Include Two Additional Nerve Block Indications. 2023. Available online: https://investor.pacira.com/news-releases/news-release-details/pacira-announces-fda-approval-expanded-exparel-label-include-two#:~:text=(NASDAQ%3A%20PCRX)%2C%20the,liposome%20injectable%20suspension)%20label%20to (accessed on 14 March 2024).
- McCann, M.E. Liposomal Bupivacaine: Effective, Cost-effective, or (Just) Costly? Anesthesiology 2021, 134, 139–142. [Google Scholar] [CrossRef] [PubMed]
- Ilfeld, B.M.; Gabriel, R.A.; Eisenach, J.C. Liposomal bupivacaine infiltration for knee arthroplasty: Significant analgesic benefits or just a bunch of fat? Anesthesiology 2018, 129, 623–626. [Google Scholar] [CrossRef] [PubMed]
- Vandepitte, C.; Kuroda, M.; Witvrouw, R.; Anne, L.; Bellemans, J.; Corten, K.; Vanelderen, P.; Mesotten, D.; Leunen, I.; Heylen, M. Addition of liposome bupivacaine to bupivacaine HCl versus bupivacaine HCl alone for interscalene brachial plexus block in patients having major shoulder surgery. Reg. Anesth. Pain Med. 2017, 42, 334–341. [Google Scholar] [CrossRef] [PubMed]
- Hussain, N.; Brull, R.; Sheehy, B.; Essandoh, M.K.; Stahl, D.L.; Weaver, T.E.; Abdallah, F.W. Perineural liposomal bupivacaine is not superior to nonliposomal bupivacaine for peripheral nerve block analgesia: A systematic review and meta-analysis. Anesthesiology 2021, 134, 147–164. [Google Scholar] [CrossRef] [PubMed]
- Kolodychuk, N.; Krebs, J.C.; Stenberg, R.; Talmage, L.; Meehan, A.; DiNicola, N. Fascia iliaca blocks performed in the emergency department decrease opioid consumption and length of stay in patients with hip fracture. J. Orthop. Trauma 2022, 36, 142–146. [Google Scholar] [CrossRef] [PubMed]
- Scurrah, A.; Shiner, C.; Stevens, J.; Faux, S. Regional nerve blockade for early analgesic management of elderly patients with hip fracture–a narrative review. Anaesthesia 2018, 73, 769–783. [Google Scholar] [CrossRef] [PubMed]
- Faculty of Pain Medicine of the Royal College of Anaesthetists. Core Standards for Pain Management Services in the UK, 2nd ed.; Faculty of Pain Medicine of the Royal College of Anaesthetists: London, UK, 2021; Available online: https://fpm.ac.uk/sites/fpm/files/documents/2022-01/FPM-Core-Standards-Dec-2021_0.pdf (accessed on 19 March 2024).
- Fabbri, A.; Voza, A.; Riccardi, A.; Serra, S.; Iaco, F.D. The pain management of trauma patients in the emergency department. J. Clin. Med. 2023, 12, 3289. [Google Scholar] [CrossRef]
- Macintyre, P.E. The opioid epidemic from the acute care hospital front line. Anaesth. Intensive Care 2022, 50, 29–43. [Google Scholar] [CrossRef]
- Mauck, M.C.; Zhao, Y.; Goetzinger, A.M.; Tungate, A.S.; Spencer, A.B.; Lal, A.; Barton, C.E.; Beaudoin, F.; McLean, S.A. Incidence of persistent opioid use following traumatic injury. Reg. Anesth. Pain Med. 2024, 49, 79–86. [Google Scholar] [CrossRef]
- Martin, T.J.; Eltorai, A.S.; Dunn, R.; Varone, A.; Joyce, M.F.; Kheirbek, T.; Adams, C., Jr.; Daniels, A.H.; Eltorai, A.E. Clinical management of rib fractures and methods for prevention of pulmonary complications: A review. Injury 2019, 50, 1159–1165. [Google Scholar] [CrossRef]
- Bulger, E.M.; Edwards, T.; Klotz, P.; Jurkovich, G.J. Epidural analgesia improves outcome after multiple rib fractures. Surgery 2004, 136, 426–430. [Google Scholar] [CrossRef] [PubMed]
- Coblentz, I.J.; Ilfeld, B.M.; Finneran Iv, J.J. Thoracic Epidural as a Rescue Analgesic in a Patient with a Continuous Erector Spinae Plane Block for Rib Fractures: A Case Report. Am. J. Case Rep. 2023, 24, e938875. [Google Scholar] [CrossRef] [PubMed]
- Malekpour, M.; Hashmi, A.; Dove, J.; Torres, D.; Wild, J. Analgesic choice in management of rib fractures: Paravertebral block or epidural analgesia? Anesth. Analg. 2017, 124, 1906–1911. [Google Scholar] [CrossRef] [PubMed]
- Mladenovic, J.; Erskine, R.N.; Riley, B.; Mitchell, A.; Abi-Fares, C.; Basson, W.; Anstey, C.; White, L. The association between erector spinae plane block timing and reduced rib fracture related respiratory complications: A cohort study. J. Clin. Anesth. 2022, 82, 110940. [Google Scholar] [CrossRef]
- Adhikary, S.; Liu, W.-M.; Fuller, E.; Cruz-Eng, H.; Chin, K.J. The effect of erector spinae plane block on respiratory and analgesic outcomes in multiple rib fractures: A retrospective cohort study. Anaesthesia 2019, 74, 585–593. [Google Scholar] [CrossRef] [PubMed]
- Moorthy, A.; Perry-Nguyen, D.; Zhou, L.; Meng, H.; Choi, S.; Niazi, A.U. Evaluation of the effect of erector spinae plane block catheter for traumatic rib fractures on patient experience: A quality assurance initiative. Reg. Anesth. Pain Med. 2023; rapm-2023-104549. [Google Scholar] [CrossRef]
- El-Sherbiny, S.M.; Kamal, R.A.; Elhadary, I.H.; Abdallah, M.Y. Erector spinae plane block versus thoracic epidural block as analgesic techniques for chest trauma: A randomized controlled trial. Res. Opin. Anesth. Intensive Care 2022, 9, 220–227. [Google Scholar]
- Hewson, D.W.; Nightingale, J.; Ogollah, R.; Ollivere, B.J.; Costa, M.L.; Craxford, S.; Bates, P.; Bedforth, N.M. Erector Spinae Plane Blocks for the Early Analgesia of Rib Fractures in Trauma (ESPEAR): Protocol for a multicentre pilot randomised controlled trial with feasibility and embedded qualitative assessment. BMJ Open 2022, 12, e062935. [Google Scholar] [CrossRef] [PubMed]
- Rommens, P.M.; Hopf, J.C.; Herteleer, M.; Devlieger, B.; Hofmann, A.; Wagner, D. Isolated pubic ramus fractures are serious adverse events for elderly persons: An observational study on 138 patients with fragility fractures of the pelvis type I (FFP type I). J. Clin. Med. 2020, 9, 2498. [Google Scholar] [CrossRef] [PubMed]
- Studer, P.; Suhm, N.; Zappe, B.; Bless, N.; Jakob, M. Pubic rami fractures in the elderly–a neglected injury? Swiss Med. Wkly. 2013, 143, w13859. [Google Scholar] [CrossRef]
- Pascarella, G.; Costa, F.; Del Buono, R.; Pulitanò, R.; Strumia, A.; Piliego, C.; De Quattro, E.; Cataldo, R.; Agrò, F.; Carassiti, M. Impact of the pericapsular nerve group (PENG) block on postoperative analgesia and functional recovery following total hip arthroplasty: A randomised, observer-masked, controlled trial. Anaesthesia 2021, 76, 1492–1498. [Google Scholar] [CrossRef]
- Lin, D.-Y.; Morrison, C.; Brown, B.; Saies, A.A.; Pawar, R.; Vermeulen, M.; Anderson, S.R.; Lee, T.S.; Doornberg, J.; Kroon, H.M. Pericapsular nerve group (PENG) block provides improved short-term analgesia compared with the femoral nerve block in hip fracture surgery: A single-center double-blinded randomized comparative trial. Reg. Anesth. Pain Med. 2021, 46, 398–403. [Google Scholar] [CrossRef] [PubMed]
- Girón-Arango, L.; Peng, P.W.; Chin, K.J.; Brull, R.; Perlas, A. Pericapsular nerve group (PENG) block for hip fracture. Reg. Anesth. Pain Med. 2018, 43, 859–863. [Google Scholar] [CrossRef]
- Moorthy, A.; Choi, S.; Safa, B.; McHardy, P.G.; Niazi, A.U. Novel use of continuous pericapsular nerve group (PENG) block technique for traumatic superior and inferior pubic rami fractures: A case report. Reg. Anesth. Pain Med. 2023, 48, 230–233. [Google Scholar] [CrossRef] [PubMed]
- Luftig, J.; Dreyfuss, A.; Mantuani, D.; Howell, K.; White, A.; Nagdev, A. A new frontier in pelvic fracture pain control in the ED: Successful use of the pericapsular nerve group (PENG) block. Am. J. Emerg. Med. 2020, 38, 2761.e2765–2761.e2769. [Google Scholar] [CrossRef] [PubMed]
- Henningsen, M.; Sort, R.; Møller, A.; Herling, S. Peripheral nerve block in ankle fracture surgery: A qualitative study of patients’ experiences. Anaesthesia 2018, 73, 49–58. [Google Scholar] [CrossRef] [PubMed]
- Lavand’homme, P. Rebound pain after regional anesthesia in the ambulatory patient. Curr. Opin. Anesthesiol. 2018, 31, 679–684. [Google Scholar] [CrossRef] [PubMed]
- Muñoz-Leyva, F.; Cubillos, J.; Chin, K.J. Managing rebound pain after regional anesthesia. Korean J. Anesthesiol. 2020, 73, 372–383. [Google Scholar] [CrossRef] [PubMed]
- Ding, D.Y.; Manoli III, A.; Galos, D.K.; Jain, S.; Tejwani, N.C. Continuous popliteal sciatic nerve block versus single injection nerve block for ankle fracture surgery: A prospective randomized comparative trial. J. Orthop. Trauma 2015, 29, 393–398. [Google Scholar] [CrossRef] [PubMed]
- Salviz, E.A.; Xu, D.; Frulla, A.; Kwofie, K.; Shastri, U.; Chen, J.; Shariat, A.N.; Littwin, S.; Lin, E.; Choi, J. Continuous interscalene block in patients having outpatient rotator cuff repair surgery: A prospective randomized trial. Anesth. Analg. 2013, 117, 1485–1492. [Google Scholar] [CrossRef]
- Hauritz, R.W.; Hannig, K.E.; Balocco, A.L.; Peeters, G.; Hadzic, A.; Børglum, J.; Bendtsen, T.F. Peripheral nerve catheters: A critical review of the efficacy. Best Pract. Res. Clin. Anaesthesiol. 2019, 33, 325–339. [Google Scholar] [CrossRef]
- Finneran, J.J., IV; Ilfeld, B.M. Continuous peripheral nerve blocks for analgesia following painful ambulatory surgery: A review with focus on recent developments in infusion technology. Curr. Opin. Anesthesiol. 2023, 36, 525–532. [Google Scholar] [CrossRef] [PubMed]
- Finneran, J.J., IV; Said, E.T.; Curran, B.P.; Swisher, M.W.; Black, J.R.; Gabriel, R.A.; Sztain, J.F.; Abramson, W.B.; Alexander, B.; Donohue, M.C. Basal infusion versus automated boluses and a delayed start timer for “continuous” sciatic nerve blocks after ambulatory foot and ankle surgery: A randomized clinical trial. Anesthesiology 2022, 136, 970–982. [Google Scholar] [CrossRef] [PubMed]
- Finneran, J.J., IV; Baskin, P.; Kent, W.T.; Hentzen, E.R.; Schwartz, A.K.; Ilfeld, B.M. Automated Boluses and Delayed-Start Timers Prolong Perineural Local Anesthetic Infusions and Analgesia Following Ankle and Wrist Orthopedic Surgery: A Case-Control Series. Med. Sci. Monit. Int. Med. J. Exp. Clin. Res. 2021, 27, e933190-1–e933190-6. [Google Scholar] [CrossRef] [PubMed]
- The European Society of Regional Anaesthesia. Advancing Regional Anaesthesia and Pain Therapy in Europe. 2023. Available online: https://esraeurope.org/about/ (accessed on 5 March 2024).
- Lobo, C. Welcome to ESRA International Committee Members 2021 [Issue 07:[ESRA Updates]. Available online: https://esraeurope.org/newsletter/article-posts/welcome-esra-international-committee-members/ (accessed on 6 March 2024).
- Royal College of Anaesthetists. Stage 3 Curriculum. 2021. Available online: https://rcoa.ac.uk/documents/2021-curriculum-learning-syllabus-stage-3/regional-anaesthesia (accessed on 15 March 2024).
- College of Anaesthesiologists of Ireland. Curriculum for the National Specialist Anaesthesiologists Training Programme. 2020. Available online: https://www.anaesthesia.ie/curriculum/?page=50 (accessed on 15 March 2024).
- Luff, D.; Moosa, F.; Sadavarte, N.; Pinnamaneni, N.; Bedforth, N. 136 Which blocks can you do? An assessment of anaesthetic trainee confidence performing common peripheral nerve blocks. Reg. Anesth. Pain Med. 2021, 70, A71. [Google Scholar]
- McKendrick, M.; Yang, S.; McLeod, G. The use of artificial intelligence and robotics in regional anaesthesia. Anaesthesia 2021, 76, 171–181. [Google Scholar] [CrossRef] [PubMed]
- Bowness, J.S.; Burckett-St Laurent, D.; Hernandez, N.; Keane, P.A.; Lobo, C.; Margetts, S.; Moka, E.; Pawa, A.; Rosenblatt, M.; Sleep, N. Assistive artificial intelligence for ultrasound image interpretation in regional anaesthesia: An external validation study. Br. J. Anaesth. 2023, 130, 217–225. [Google Scholar] [CrossRef]
- Bowness, J.; El-Boghdadly, K.; Burckett-St Laurent, D. Artificial intelligence for image interpretation in ultrasound-guided regional anaesthesia. Anaesthesia 2021, 76, 602–607. [Google Scholar] [CrossRef]
Figure 1.
The Erector Spinae Plane (ESP) Block. (A) Axial cross section demonstrating US probe position and anatomical structures in ESP block. (B) Posterior dermatomes and expected spread (green) of ESP block at the level of T5 (yellow). (C) Anterior dermatomes and expected spread (green) of ESP block at the level of T5 (yellow).
Figure 1.
The Erector Spinae Plane (ESP) Block. (A) Axial cross section demonstrating US probe position and anatomical structures in ESP block. (B) Posterior dermatomes and expected spread (green) of ESP block at the level of T5 (yellow). (C) Anterior dermatomes and expected spread (green) of ESP block at the level of T5 (yellow).
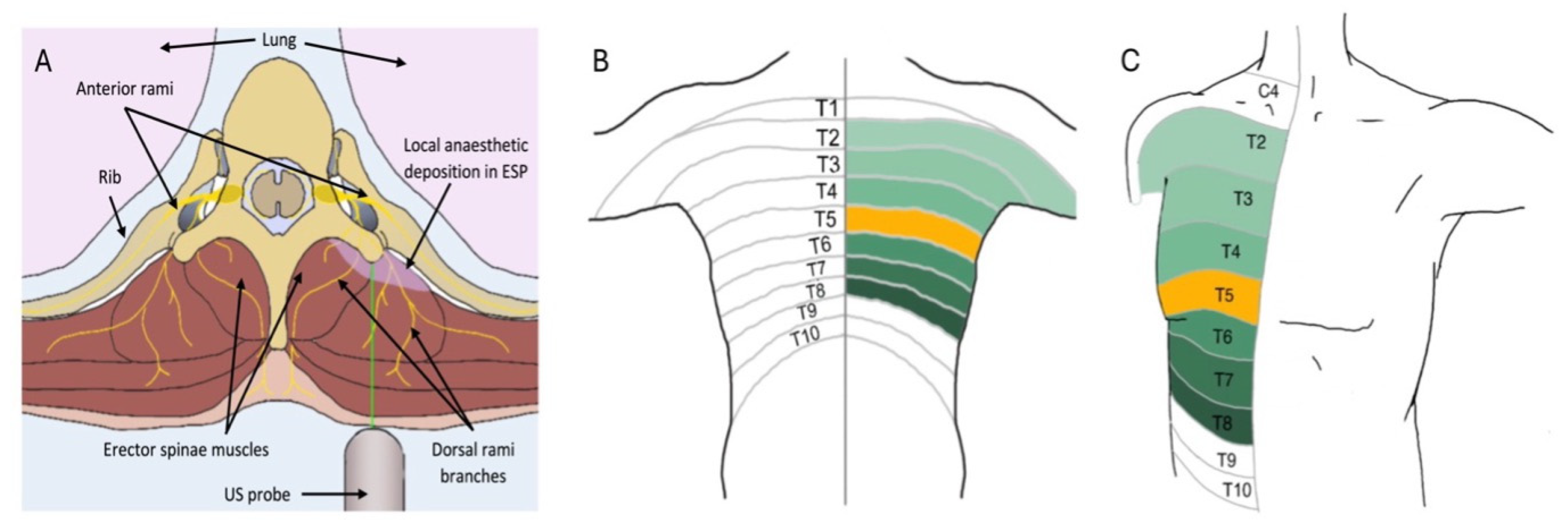
Figure 2.
Neuromodulation via percutaneous peripheral nerve stimulation for acute pain management. Stimulation of A Beta fibres peripherally increases the action of the inhibitory interneuron, thus reducing the transmission of pain signals from A Delta and/or C fibres onto the second (blue)- and third (orange)-order neurons.
Figure 2.
Neuromodulation via percutaneous peripheral nerve stimulation for acute pain management. Stimulation of A Beta fibres peripherally increases the action of the inhibitory interneuron, thus reducing the transmission of pain signals from A Delta and/or C fibres onto the second (blue)- and third (orange)-order neurons.

Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Fallon, F.; Moorthy, A.; Skerritt, C.; Crowe, G.G.; Buggy, D.J. Latest Advances in Regional Anaesthesia. Medicina 2024, 60, 735. https://doi.org/10.3390/medicina60050735
AMA Style
Fallon F, Moorthy A, Skerritt C, Crowe GG, Buggy DJ. Latest Advances in Regional Anaesthesia. Medicina. 2024; 60(5):735. https://doi.org/10.3390/medicina60050735
Chicago/Turabian StyleFallon, Frances, Aneurin Moorthy, Conor Skerritt, Gillian G. Crowe, and Donal J. Buggy. 2024. "Latest Advances in Regional Anaesthesia" Medicina 60, no. 5: 735. https://doi.org/10.3390/medicina60050735