
Targeted Analysis of Plasma Polar Metabolites in Postmenopausal Depression

 , ,
, , 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Anthropometric Assessment
2.2. Assessment of Depression Status
2.3. Experimental Groups
- Pre ND: Premenopausal women, without depression symptoms (n = 21).
- Pre D: Premenopausal women with depression symptoms (n = 21).
- Post ND: Postmenopausal women without depression symptoms (n = 25).
- Post D: Postmenopausal women with depression symptoms (n = 42).
2.4. Polar Metabolites Analysis
2.5. Chromatographic Analysis Coupled to Mass Spectrometry (LC-MS/MS)
2.6. Statistical Analysis
3. Results
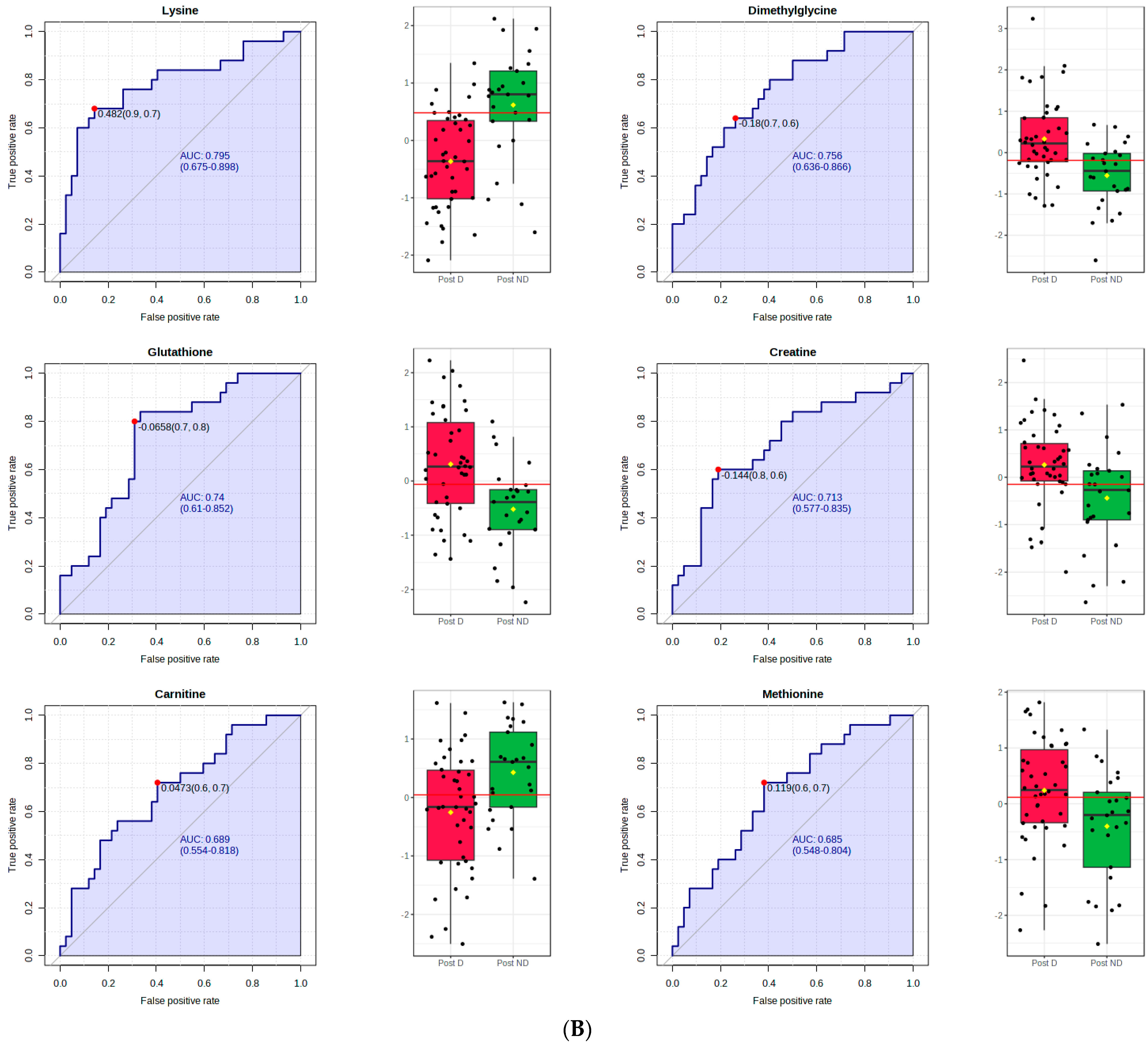
3.1. Postmenopausal Women
3.2. Premenopausal Women
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Gariepy, G.; Nitka, D.; Schmitz, N. The association between obesity and anxiety disorders in the population: A systematic review and meta-analysis. Int. J. Obes. 2010, 34, 407–419. [Google Scholar] [CrossRef] [PubMed]
- Alvaro, P.K.; Roberts, R.M.; Harris, J.K. The independent relationships between insomnia, depression, subtypes of anxiety, and chronotype during adolescence. Sleep Med. 2014, 15, 934–941. [Google Scholar] [CrossRef] [PubMed]
- Wassertheil-Smoller, S.; Shumaker, S.; Ockene, J.; Talavera, G.A.; Greenland, P.; Cochrane, B.; Robbins, J.; Aragaki, A.; Dunbar-Jacob, J. Depression and cardiovascular sequelae in postmenopausal women. The Women′s Health Initiative (WHI). Arch. Intern. Med. 2004, 164, 289–298. [Google Scholar] [CrossRef] [PubMed]
- Pan, A.; Keum, N.; Okereke, O.I.; Sun, Q.; Kivimaki, M.; Rubin, R.R.; Hu, F.B. Bidirectional association between depression and metabolic syndrome: A systematic review and meta-analysis of epidemiological studies. Diabetes Care 2012, 35, 1171–1180. [Google Scholar] [CrossRef] [PubMed]
- Pan, A.; Sun, Q.; Okereke, O.I.; Rexrode, K.M.; Hu, F.B. Depression and risk of stroke morbidity and mortality: A meta-analysis and systematic review. JAMA 2011, 306, 1241–1249. [Google Scholar] [CrossRef] [PubMed]
- Chisholm, D.; Sweeny, K.; Sheehan, P.; Rasmussen, B.; Smit, F.; Cuijpers, P.; Saxena, S. Scaling-up treatment of depression and anxiety: A global return on investment analysis. Lancet Psychiatry 2016, 3, 415–424. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization (WHO). 2010. Available online: http://www.who.int/mediacentre/factsheets/fs311/en/ (accessed on 1 February 2024).
- McElroy, S.L.; Kotwal, R.; Malhotra, S.; Nelson, E.B.; Keck, P.E.; Nemeroff, C.B. Are mood disorders and obesity related? A review for the mental health professional. J. Clin. Psychiatry 2004, 65, 634–651. [Google Scholar] [CrossRef] [PubMed]
- Elavsky, S.; McAuley, E. Physical activity and mental health outcomes during menopause; a randomized trial. Ann. Behav. Med. 2007, 33, 132–142. [Google Scholar] [CrossRef] [PubMed]
- Krishnan, V.; Nestler, E.J. The molecular neurobiology of depression. Nature 2008, 45, 894–902. [Google Scholar] [CrossRef]
- Wang, L.; Zhou, C.; Zhu, D.; Wang, X.; Fang, L.; Zhong, J.; Mao, Q.; Sun, L.; Gong, X.; Xia, J.; et al. Serotonin-1A receptor alteration in depression: A meta-analysis of molecular imaging studies. BMC Psychiatry 2016, 16, 319. [Google Scholar] [CrossRef]
- Naufel, M.F.; Boldarine, V.T.; Oyama, L.M.; do Nascimento, C.M.O.; dos Santos, S.G.M.; Hachul, H.; Ribeiro, E.B. Age and leptinemia association with anxiety and depression symptoms in overweight middle-aged women. Menopause 2019, 26, 317–324. [Google Scholar] [CrossRef]
- Naufel, M.F.; Pedroso, A.P.; Oyama, L.M.; Telles, M.M.; Hachul, H.; Ribeiro, E.B. Preliminary evidence of acylated ghrelin association with depression severity in postmenopausal women. Sci. Rep. 2021, 11, 5319. [Google Scholar] [CrossRef]
- Ancelin, M.L.; Scali, J.; Ritchie, K. Hormonal therapy and depression; are we overlooking an important therapeutic alternative? J. Psychosom. Res. 2007, 62, 473–485. [Google Scholar] [CrossRef] [PubMed]
- Wildman, R.P.; Sowers, M.R. Adiposity and the menopausal transition. Obstet. Gynecol. Clin. N. Am. 2011, 38, 441–454. [Google Scholar] [CrossRef] [PubMed]
- Dornellas, A.P.S.; Boldarine, V.T.; Pedroso, A.P.; Carvalho, L.O.T.; de Andrade, I.S.; Vulcani-Freitas, T.M.; dos Santos, C.C.C.; do Nascimento, C.M.D.P.O.; Oyama, L.M.; Ribeiro, E.B. High-fat feeding improves anxiety-type behavior induced by ovariectomy in rats. Front. Neurosci. 2018, 12, 557. [Google Scholar] [CrossRef] [PubMed]
- Boldarine, V.T.; Pedroso, A.P.; Neto, N.I.P.; Dornellas, A.P.S.; Nascimento, C.M.O.; Oyama, L.M.; Ribeiro, E.B. High-fat diet intake induces depressive-like behavior in ovariectomized rats. Sci. Rep. 2019, 9, 10551. [Google Scholar] [CrossRef] [PubMed]
- Christians, U.; Klawitter, J.; Hornberger, A.; Klawitter, J. How Unbiased is Non-Targeted Metabolomics and is Targeted Pathway Screening the Solution? Curr. Pharm. Biotechnol. 2011, 12, 1053–1066. [Google Scholar] [CrossRef] [PubMed]
- Kosmides, A.K.; Kamisoglu, K.; Calvano, S.E.; Corbett, S.A.; Androulakis, I.P. Metabolomic Fingerprinting: Challenges and Opportunities. Crit. Rev. Biomed. Eng. 2013, 41, 205–221. [Google Scholar] [CrossRef] [PubMed]
- Patti, G.J.; Yanes, O.; Siuzdak, G. Innovation: Metabolomics: The apogee of the omics trilogy. Nat. Rev. Mol. Cell Biol. 2012, 13, 263–269. [Google Scholar] [CrossRef]
- Ursell, L.K.; Haiser, H.J.; Treuren, W.V.; Garg, N.; Reddivari, L.; Vanamala, J.; Dorrestein, P.C.; Turnbaugh, P.J.; Knight, R. The intestinal metabolome: An intersection between microbiota and host. Gastroenterology 2014, 146, 1470–1476. [Google Scholar] [CrossRef]
- Lent-Schochet, D.; McLaughlin, M.; Ramakrishnan, N.; Jialal, I. Exploratory metabolomics of metabolic syndrome: A status report. World J. Diabetes 2019, 10, 23–36. [Google Scholar] [CrossRef] [PubMed]
- Urayama, S.; Zou, W.; Brooks, K.; Tolstikov, V. Comprehensive mass spectrometry based metabolic profiling of blood plasma reveals potent discriminatory classifiers of pancreatic cancer. Rapid Commun. Mass Spectrom. 2010, 24, 613–620. [Google Scholar] [CrossRef] [PubMed]
- Wang, T.J.; Larson, M.G.; Vasan, R.S.; Cheng, S.; Rhee, E.P.; McCabe, E.; Lewis, G.D.; Fox, C.S.; Jacques, P.F.; Fernandez, C.; et al. Metabolite profiles and the risk of developing diabetes. Nat. Med. 2011, 17, 448–453. [Google Scholar] [CrossRef]
- Naz, S.; Calderón, Á.A.; García, A.; Gallafrio, J.; Mestre, R.T.; González, E.G.; de Cabo, C.M.; Delgado, M.C.M.; Balanza, J.Á.L.; Simionato, A.V.C.; et al. Unveiling differences between patients with acute coronary syndrome with and without ST elevation through fingerprinting with CE-MS and HILIC-MS targeted analysis. Electrophoresis 2015, 36, 2303–2313. [Google Scholar] [CrossRef]
- Ibáñez, C.; Simó, C.; Martín-Álvarez, P.J.; Kivipelto, M.; Winblad, B.; Cedazo-Minguez, A.; Cifuentes, A. Toward a predictive model of Alzheimer’s disease progression using capillary electrophoresis-mass spectrometry metabolomics. Anal. Chem. 2012, 84, 8532–8540. [Google Scholar] [CrossRef]
- Demirkan, A.; Isaacs, A.; Ugocsai, P.; Liebisch, G.; Struchalin, M.; Rudan, I.; Wilson, J.F.; Pramstaller, P.P.; Gyllensten, U.; Campbell, H.; et al. Plasma phosphatidylcholine and sphingomyelin concentrations are associated with depression and anxiety symptoms in a Dutch family-based lipidomics study. J. Psychiatr. Res. 2013, 47, 357–362. [Google Scholar] [CrossRef]
- Huang, T.; Balasubramanian, R.; Yao, Y.; Clish, C.B.; Shadyab, A.H.; Liu, B.; Tworoger, S.S.; Rexrode, K.M.; Manson, J.E.; Kubzansky, L.D.; et al. Associations of depression status with plasma levels of candidate lipid and amino acid metabolites: A meta-analysis of individual data from three independent samples of US postmenopausal women. Mol. Psychiatry 2021, 26, 3315–3327. [Google Scholar] [CrossRef] [PubMed]
- Conselho Nacional de Saúde (Brasil). Norma Operacional nº. 001/2013. Brasília. 2013. Available online: http://www.conselho.saude.gov.br/web_comissoes/conep/index.html (accessed on 1 February 2024).
- Hurst, P.R.V.; Walsh, D.C.I.; Conlon, C.A.; Kruger, R.; Stonehouse, W. Validity and reliability of bioelectrical impedance analysis to estimate body fat percentage against air displacement plethysmography and dual-energy X-ray absorptiometry. Nutr. Diet. 2015, 73, 197–204. [Google Scholar] [CrossRef]
- Beck, A.T.; Ward, C.H.; Mendelson, M.; Mock, J.; Erbaugh, J. An inventory for measuring depression. Arch. Gen. Psychiatry 1961, 4, 561–571. [Google Scholar] [CrossRef]
- Cunha, J.A. Manual for the Portuguese Version of the Beck Scales; Casa do Psicólogo: São Paulo, SP, Brazil, 2001. [Google Scholar]
- Xia, J.; Wishart, D.S. Web-based inference of biological patterns, functions and pathways from metabolomic data using MetaboAnalyst. Nat. Protoc. 2011, 6, 743–760. [Google Scholar] [CrossRef]
- Li, Y.; Wang, C.; Chen, M. Metabolomics-based study of potential biomarkers of sepsis. Sci. Rep. 2023, 13, 585. [Google Scholar] [CrossRef] [PubMed]
- Cui, X.; Yu, X.; Sun, G.; Hu, T.; Likhodii, S.; Zhang, J.; Randell, E.; Gao, X.; Fan, Z.; Zhang, W. Differential metabolomics networks analysis of menopausal status. PLoS ONE 2019, 14, e0222353. [Google Scholar] [CrossRef] [PubMed]
- Borea, P.A.; Gessi, S.; Merighi, S.; Varani, K. Adenosine as a Multi-Signalling Guardian Angel in Human Diseases: When, Where and How Does it Exert its Protective Effects? Trends Pharmacol. Sci. 2016, 37, 419–434. [Google Scholar] [CrossRef] [PubMed]
- Gomes, J.I.; Farinha-Ferreira, M.; Rei, N.; Goncalves-Ribeiro, J.; Ribeiro, J.A.; Sebastiao, A.M.; Vaz, S.H. Of adenosine and the blues: The adenosinergic system in the pathophysiology and treatment of major depressive disorder. Pharmacol. Res. 2021, 163, 105363. [Google Scholar] [CrossRef] [PubMed]
- Serchov, T.; Clement, H.W.; Schwarz, M.K.; Iasevoli, F.; Tosh, D.K.; Idzko, M.; Jacobson, K.A.; de Bartolomeis, A.; Normann, C.; Biber, K.; et al. Increased Signaling via Adenosine A1 Receptors, Sleep Deprivation, Imipramine, and Ketamine Inhibit Depressive-like Behavior via Induction of Homer1a. Neuron 2015, 87, 549–562. [Google Scholar] [CrossRef] [PubMed]
- Rose′Meyer, R.B.; Mellick, A.S.; Garnham, B.G.; Harrison, G.J.; Massa, H.M.; Griffiths, L.R. The measurement of adenosine and estrogen receptor expression in rat brains following ovariectomy using quantitative PCR analysis. Brain Res. Protoc. 2003, 11, 9–18. [Google Scholar] [CrossRef] [PubMed]
- Bettio, L.E.; Gil-Mohapel, J.; Rodrigues, A.L. Guanosine and its role in neuropathologies. Purinergic Signal. 2016, 12, 411–426. [Google Scholar] [CrossRef] [PubMed]
- Camargo, A.; Bettio, L.E.B.; Rosa, P.B.; Rosa, J.M.; Altê, G.A.; Rodrigues, A.L.S. The antidepressant-like effect of guanosine involves the modulation of adenosine A1 and A2A receptors. Purinergic Signal. 2023, 19, 387–399. [Google Scholar] [CrossRef] [PubMed]
- Mocking, R.J.T.; Naviaux, J.C.; Li, K.; Wang, L.; Monk, J.M.; Bright, A.T.; Figueroa, C.A.; Schene, A.H.; Ruhé, H.G.; Assies, J.; et al. Metabolic features of recurrent major depressive disorder in remission, and the risk of future recurrence. Transl. Psychiatry 2021, 11, 37. [Google Scholar] [CrossRef]
- Rosa, P.B.; Bettio, L.E.B.; Neis, V.B.; Moretti, M.; Kaufmann, F.N.; Tavares, M.K.; Werle, I.; Dalsenter, Y.; Platt, N.; Rosado, A.F.; et al. Antidepressant-like effect of guanosine involves activation of AMPA receptor and BDNF/TrkB signaling. Purinergic Signal. 2021, 17, 285–301. [Google Scholar] [CrossRef]
- Krane, S.M. The importance of proline residues in the structure, stability and susceptibility to proteolytic degradation of colla-gens. Amino Acids 2008, 35, 703–710. [Google Scholar] [CrossRef]
- Nogimura, D.; Mizushige, T.; Taga, Y.; Nagai, A.; Shoji, S.; Azuma, N.; Kusubata, M.; Adachi, S.I.; Yoshizawa, F.; Kabuyama, Y. Prolyl-hydroxyproline, a collagen-derived dipeptide, enhances hippocampal cell proliferation, which leads to antidepressant-like effects in mice. FASEB J. 2020, 34, 5715–5723. [Google Scholar] [CrossRef] [PubMed]
- Mayneris-Perxachs, J.; Castells-Nobau, A.; Arnoriaga-Rodríguez, M.; Martin, M.; de la Vega-Correa, L.; Zapata, C.; Burokas, A.; Blasco, G.; Coll, C.; Escrichs, A.; et al. Microbiota alterations in proline metabolism impact depression. Cell Metab. 2022, 34, 681–701.e10. [Google Scholar] [CrossRef] [PubMed]
- Bian, X.; Zhou, N.; Zhao, Y.; Fang, Y.; Li, N.; Zhang, X.; Wang, X.; Li, Y.; Wu, J.L.; Zhou, T. Identification of proline, 1-pyrroline-5-carboxylate and glutamic acid as biomarkers of depression reflecting brain metabolism using carboxylomics, a new metabolomics method. Psychiatry Clin. Neurosci. 2023, 77, 196–204. [Google Scholar] [CrossRef] [PubMed]
- Lee, K.W.; Kim, S.J.; Park, J.B.; Lee, K.J. Relationship between depression anxiety stress scale (DASS) and urinary hydroxyproline and proline concentrations in hospital workers. J. Prev. Med. Public Health 2011, 44, 9–13. [Google Scholar] [CrossRef] [PubMed]
- Nam, S.Y.; Yoou, M.S.; Kim, H.M.; Jeong, H.J. Efficacy of proline in the treatment of menopause. Exp. Biol. Med. 2016, 241, 611–619. [Google Scholar] [CrossRef] [PubMed]
- Curis, E.; Nicolis, I.; Moinard, C.; Osowska, S.; Zerrouk, N.; Benazeth, S.; Cynober, L. Almost all about citrulline in mammals. Amino Acids 2005, 29, 177–205. [Google Scholar] [CrossRef] [PubMed]
- Celermajer, D.S.; Sorensen, K.E.; Spiegelhalter, D.J.; Georgakopoulos, D.; Robinson, J.; Deanfield, J.E. Aging is associated with endothelial dysfunction in healthy men years before the age-related decline in women. J. Am. Coll. Cardiol. 1994, 24, 471–476. [Google Scholar] [CrossRef] [PubMed]
- Maharaj, A.; Fischer, S.M.; Dillon, K.N.; Kang, Y.; Martinez, M.A.; Figueroa, A. Effects of L-Citrulline Supplementation on Endothelial Function and Blood Pressure in Hypertensive Postmenopausal Women. Nutrients 2022, 14, 4396. [Google Scholar] [CrossRef]
- Fan, M.; Gao, X.; Li, L.; Ren, Z.; Lui, L.M.W.; McIntyre, R.S.; Teopiz, K.M.; Deng, P.; Cao, B. The Association Between Concentrations of Arginine, Ornithine, Citrulline and Major Depressive Disorder: A Meta-Analysis. Front. Psychiatry 2021, 18, 686973. [Google Scholar] [CrossRef]
- Hess, S.; Baker, G.; Gyenes, G.; Tsuyuki, R.; Newman, S.; Le Melledo, J.M. Decreased serum L-arginine and L-citrulline levels in major depression. Psychopharmacology 2017, 234, 3241–3247. [Google Scholar] [CrossRef]
- Smriga, M.; Torii, K. L-Lysine acts like a partial serotonin receptor 4 antagonist and inhibits serotonin-mediated intestinal pathologies and anxiety in rats. Proc. Natl. Acad. Sci. USA 2003, 100, 15370–15375. [Google Scholar] [CrossRef]
- Jezova, D.; Makatsori, A.; Smriga, M.; Morinaga, Y.; Duncko, R. Subchronic treatment with amino acid mixture of L-lysine and L-arginine modifies neuroendocrine activation during psychosocial stress in subjects with high trait anxiety. Nutr. Neurosci. 2005, 8, 155–160. [Google Scholar] [CrossRef]
- Lin, J.C.; Chan, M.H.; Lee, M.Y.; Chen, Y.C.; Chen, H.H. N,N-dimethylglycine differentially modulates psychotomimetic and antidepressant-like effects of ketamine in mice. Prog. Neuropsychopharmacol. Biol. Psychiatry 2016, 71, 7–13. [Google Scholar] [CrossRef]
- Gawryluk, J.W.; Wang, J.F.; Andreazza, A.C.; Shao, L.; Young, L.T. Decreased levels of glutathione, the major brain antioxidant, in post-mortem prefrontal cortex from patients with psychiatric disorders. Int. J. Neuropsychopharmacol. 2011, 14, 123–130. [Google Scholar] [CrossRef]
- Lu, S.C. Glutathione synthesis. Biochim. Biophys. Acta 2013, 1830, 3143–3153. [Google Scholar] [CrossRef]
- Lindqvist, D.; Dhabhar, F.S.; James, S.J.; Hough, C.M.; Jain, F.A.; Bersani, F.S.; Reus, V.I.; Verhoeven, J.E.; Epel, E.S.; Mahan, L.; et al. Oxidative stress, inflammation and treatment response in major depression. Psychoneuroendocrinology 2017, 76, 197–205. [Google Scholar] [CrossRef]
- Tuura, R.O.; Buchmann, A.; Ritter, C.; Hase, A.; Haynes, M.; Noeske, R.; Hasler, G. Prefrontal Glutathione Levels in Major Depressive Disorder Are Linked to a Lack of Positive Affect. Brain Sci. 2023, 13, 1475. [Google Scholar] [CrossRef]
- Lapidus, K.A.; Gabbay, V.; Mao, X.; Johnson, A.; Murrough, J.W.; Mathew, S.J.; Shungu, D.C. In vivo 1H MRS study of potential associations between glutathione, oxidative stress and anhedonia in major depressive disorder. Neurosci. Lett. 2014, 569, 74–79. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Post ND (25) | Post D (42) | p | |
|---|---|---|---|
| Age (years) a | 55.9 ± 0.9 | 57.2 ± 0.6 | 0.221 |
| Years after menopause a | 7.6 ± 1.1 | 8.4 ± 0.95 | 0.549 |
| BMI (kg/m2) a | 28.0 ± 1.0 | 28.3 ± 0.7 | 0.799 |
| FSH (mUI/dL) a | 65.3 ± 5.6 | 79.8 ± 3.9 | 0.036 |
| Cortisol (ng/dL) b | 5.2 ± 0.4 | 8.1 ± 1.2 | 0.401 |
| BFP a | 39.0 ± 1.4 | 39.5 ± 1.2 | 0.816 |
| Muscle Mass (kg) a | 27.7 ± 1.9 | 28.7 ± 1.5 | 0.673 |
| BDI a | 5.7 ± 0.6 | 19.1 ± 1.2 | <0.001 |
| Diabetes c | 8.0% | 16.7% | 0.314 |
| Hypertension c | 8.0% | 35.7% | 0.012 |
| Exercise c | 40.0% | 57.1% | 0.174 |
| Fold-Change (D/ND) | VIP | |
|---|---|---|
| Proline | 0.3988 * | 1.8235 |
| Guanosine | 0.4174 * | 2.3990 |
| Adenosine | 0.4575 * | 2.4560 |
| Hypoxanthine | 1.6896 | 0.8120 |
| 4−Hydroxyproline | 1.6838 | 0.6588 |
| Lysine | 0.6382 * | 1.6433 |
| 2−Aminobutyric acid | 1.5059 | 1.0236 |
| Adenosine monophosphate | 1.5019 | 0.4053 |
| Dimethylglycine | 1.4936 * | 1.3144 |
| Citrulline | 0.6748 * | 1.5789 |
| Cystine | 1.4698 | 0.3894 |
| Creatine | 1.3278 * | 1.0478 |
| Pantothenic acid | 0.7708 | 0.8966 |
| Aspartic acid | 1.2737 | 1.1528 |
| Isocitric acid | 1.2533 | 0.9406 |
| Carnitine | 0.8020 * | 1.2326 |
| Fumaric acid | 1.2419 | 0.7060 |
| Glutamic acid | 1.2342 | 1.0623 |
| Histidine | 0.8436 | 0.8997 |
| Methionine | 1.1709 * | 1.0852 |
| Glycine | 1.1527 | 0.5705 |
| Kynurenic Acid | 0.8698 | 0.4935 |
| Arginine | 1.1479 | 0.9366 |
| Succinic acid | 0.8748 | 0.8084 |
| Uridine | 1.1425 | 0.4721 |
| Oxidized glutathione | 0.8785 | 0.6176 |
| Glutathione | 1.1354 * | 1.2642 |
| Valine | 0.8827 | 0.8552 |
| Isoleucine | 1.1221 | 0.7252 |
| Lactic acid | 0.8914 | 0.6723 |
| Glutamine | 1.1200 | 0.9857 |
| Ornitine | 0.8985 | 0.7312 |
| Phenylalanine | 1.1102 | 0.8767 |
| Tyrosine | 1.1094 | 0.7783 |
| Kynurenine | 1.1006 | 0.7979 |
| Serine | 1.0865 | 0.5120 |
| Asymmetric dimethylarginine | 1.0781 | 0.6698 |
| Asparagine | 1.0746 | 0.4758 |
| Tryptophan | 1.0737 | 0.7294 |
| Alanine | 1.0694 | 0.6352 |
| Cysteine | 0.9352 | 0.6616 |
| Choline | 1.0637 | 0.6512 |
| Creatinine | 1.0588 | 0.6533 |
| Uric acid | 1.0580 | 0.7031 |
| Threonine | 1.0480 | 0.5508 |
| 2−Ketoglutaric Acid | 0.9708 | 1.2005 |
| Acetylcarnitine | 1.0167 | 0.5066 |
| Leucine | 1.0074 | 0.6670 |
| TMAO | 0.9944 | 0.4392 |
| Taurine | 0.9964 | 0.6612 |
| Metabolite Name | Fold-Change (D/ND) | FDR | VIP |
|---|---|---|---|
| Adenosine | 0.4575 | 3.778 × 10−14 | 2.4560 |
| Guanosine | 0.4174 | 3.001 × 10−13 | 2.3990 |
| Proline | 0.3988 | 1.430 × 10−6 | 1.8235 |
| Citrulline | 0.6748 | 0.0001 | 1.5789 |
| Lysine | 0.6382 | 0.0004 | 1.6433 |
| Dimethylglycine | 1.4936 | 0.0022 | 1.3144 |
| Glutathione | 1.1354 | 0.0048 | 1.2642 |
| Creatine | 1.3278 | 0.0286 | 1.0478 |
| Carnitine | 0.8020 | 0.0331 | 1.2326 |
| Methionine | 1.1709 | 0.0484 | 1.0852 |
| Pre ND, (21) | Pre D (21) | p | |
|---|---|---|---|
| Age (years) a | 44.3 ± 0.7 | 44.8 ± 0.8 | 0.608 |
| BMI (kg/m2) a | 26.8 ± 1.2 | 29.3 ± 1.0 | 0.114 |
| FSH (mUI/dL) a | 8.6 ± 1.3 | 7.0 ± 0.9 | 0.318 |
| Cortisol (ng/dL) a | 6.6 ± 0.8 | 6.0 ± 0.8 | 0.620 |
| BFP a | 36.1 ± 1.6 | 40.3 ± 1.5 | 0.066 |
| Muscle Mass (kg) a | 25.2 ± 1.9 | 31.4 ± 2.0 | 0.034 |
| BDI (score) a | 4.7 ± 0.6 | 18.9 ± 1.7 | <0.000 |
| Diabetes b | 0.0% | 4.7% | 0.311 |
| Hypertension b | 19.0% | 14.3% | 0.679 |
| Exercise b | 57.1% | 14.3% | 0.004 |
| Fold-Change (D/ND) | VIP | |
|---|---|---|
| Proline | 0.9277 | 0.9943 |
| Guanosine | 1.1811 | 1.1250 |
| Adenosine | 0.9953 | 0.8699 |
| Hypoxanthine | 0.8934 | 0.5664 |
| 4−Hydroxyproline | 2.3518 * | 1.6441 |
| Lysine | 1.1013 | 1.0905 |
| 2−Aminobutyric acid | 0.9493 | 0.5869 |
| Adenosine monophosphate | 0.8173 | 0.4206 |
| Dimethylglycine | 1.6595 * | 1.4842 |
| Citrulline | 0.9509 | 1.2853 |
| Cystine | 1.3541 | 1.0062 |
| Creatine | 1.1235 | 0.7455 |
| Pantothenic acid | 0.7769 | 0.7956 |
| Aspartic acid | 1.1453 | 0.9636 |
| Isocitric acid | 1.1114 | 0.6755 |
| Carnitine | 1.1448 | 1.1767 |
| Fumaric acid | 1.1059 | 0.5928 |
| Glutamic acid | 1.2259 | 1.3787 |
| Histidine | 0.9470 | 1.3093 |
| Methionine | 0.9661 | 1.1109 |
| Glycine | 0.9465 | 0.8499 |
| Kynurenic Acid | 2.0251 | 1.0403 |
| Arginine | 1.1039 | 0.8819 |
| Succinic acid | 1.1559 | 0.9289 |
| Uridine | 1.0621 | 0.2917 |
| Oxidized glutathione | 0.4959 * | 2.1168 |
| Glutathione | 0.9976 | 0.5093 |
| Valine | 1.0977 | 1.2988 |
| Isoleucine | 1.1195 | 1.1936 |
| Lactic acid | 1.1035 | 0.8348 |
| Glutamine | 1.0049 | 0.9662 |
| Ornitine | 1.1609 | 0.8215 |
| Phenylalanine | 1.1102 | 1.3965 |
| Tyrosine | 1.1284 | 1.0349 |
| Kynurenine | 0.9203 | 0.8449 |
| Serine | 0.9467 | 0.9429 |
| Asymmetric dimethylarginine | 1.0518 | 0.6525 |
| Asparagine | 1.0584 | 0.9984 |
| Tryptophan | 1.0664 | 0.8062 |
| Alanine | 1.0021 | 0.7768 |
| Cysteine | 1.4670 | 0.8213 |
| Choline | 0.9744 | 0.8032 |
| Creatinine | 0.9942 | 0.8302 |
| Uric acid | 1.0402 | 1.1055 |
| Threonine | 0.9791 | 0.7418 |
| 2−Ketoglutaric Acid | 1.1100 | 0.3913 |
| Acetylcarnitine | 1.0655 | 1.2127 |
| Leucine | 0.8730 | 1.1372 |
| TMAO | 1.1001 | 0.3463 |
| Taurine | 1.1554 | 0.6501 |
| Metabolite Name | Fold-Change (D/ND) | FDR | VIP |
|---|---|---|---|
| Oxidized glutathione | 0.4959 | 0.0137 | 2.1168 |
| 4-Hydroxyproline | 2.3518 | 0.0406 | 1.6441 |
| Dimethylglycine | 1.6595 | 0.0433 | 1.4842 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Naufel, M.F.; Pedroso, A.P.; de Souza, A.P.; Boldarine, V.T.; Oyama, L.M.; Lo Turco, E.G.; Hachul, H.; Ribeiro, E.B.; Telles, M.M. Targeted Analysis of Plasma Polar Metabolites in Postmenopausal Depression. Metabolites 2024, 14, 286. https://doi.org/10.3390/metabo14050286
Naufel MF, Pedroso AP, de Souza AP, Boldarine VT, Oyama LM, Lo Turco EG, Hachul H, Ribeiro EB, Telles MM. Targeted Analysis of Plasma Polar Metabolites in Postmenopausal Depression. Metabolites. 2024; 14(5):286. https://doi.org/10.3390/metabo14050286
Chicago/Turabian StyleNaufel, Maria Fernanda, Amanda Paula Pedroso, Adriana Pereira de Souza, Valter Tadeu Boldarine, Lila Missae Oyama, Edson Guimarães Lo Turco, Helena Hachul, Eliane Beraldi Ribeiro, and Mônica Marques Telles. 2024. "Targeted Analysis of Plasma Polar Metabolites in Postmenopausal Depression" Metabolites 14, no. 5: 286. https://doi.org/10.3390/metabo14050286