
Exogenous Ketone Supplement Administration Abrogated Isoflurane-Anesthesia-Induced Increase in Blood Glucose Level in Female WAG/Rij Rats





Abstract
:1. Introduction
2. Methods
2.1. Experimental Animals
2.2. Experimental Design
2.3. Blood R-βHB and Glucose Levels, as Well as Body Weight
2.4. Statistics
3. Results
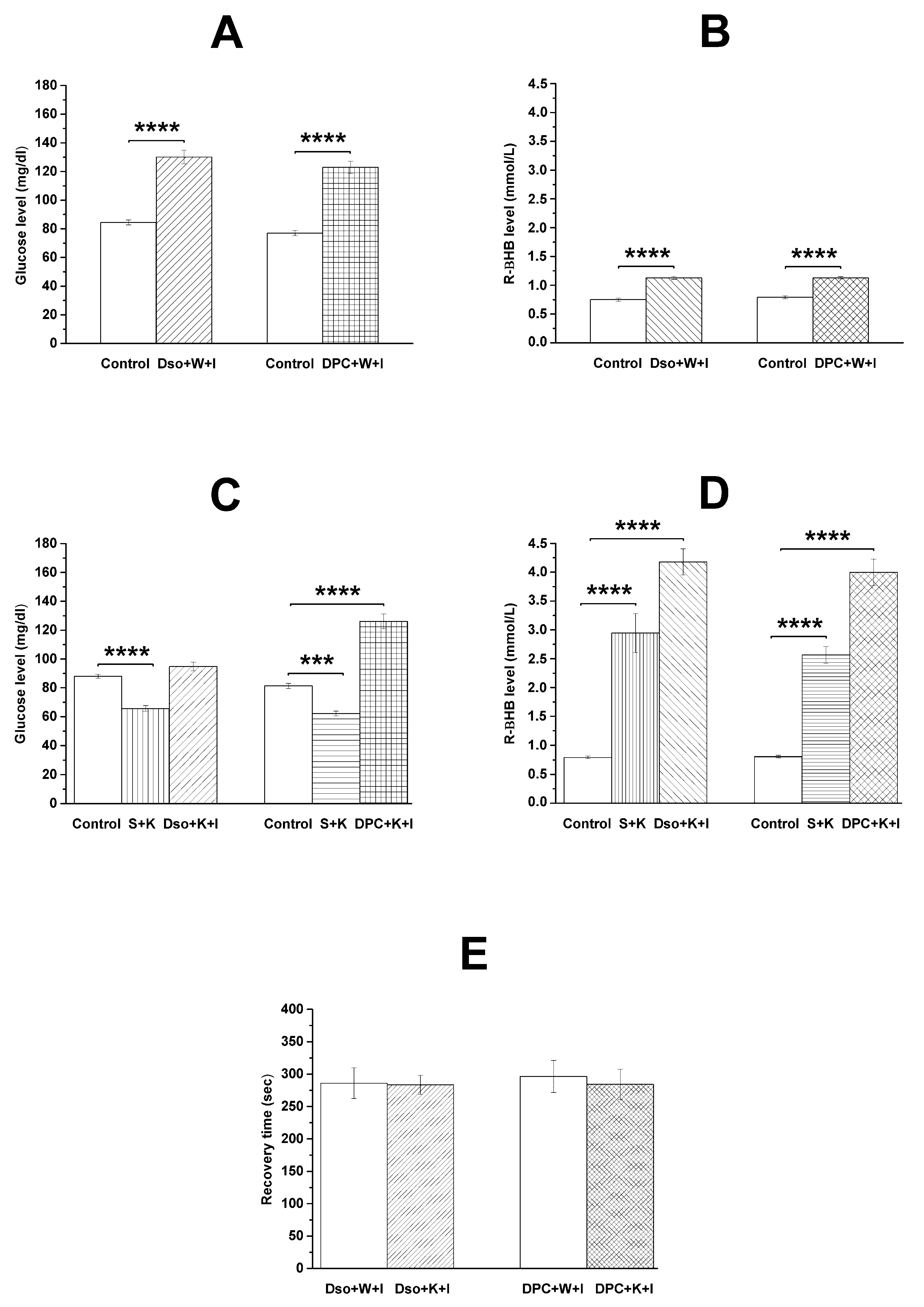
3.1. Influence of DPCPX and KEMCT on Isoflurane-Anesthesia-Evoked Alterations in Level of Blood Glucose and R-βHB and on Body Weight
3.2. Effects of DPCPX and KEMCT on Recovery Time
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
References
- Franks, N.P. General anaesthesia: From molecular targets to neuronal pathways of sleep and arousal. Nat. Rev. Neurosci. 2008, 9, 370–386. [Google Scholar] [CrossRef]
- Hao, X.; Ou, M.; Zhang, D.; Zhao, W.; Yang, Y.; Liu, J.; Yang, H.; Zhu, T.; Li, Y.; Zhou, C. The Effects of General Anesthetics on Synaptic Transmission. Curr. Neuropharmacol. 2020, 18, 936–965. [Google Scholar] [CrossRef] [PubMed]
- Deng, J.; Lei, C.; Chen, Y.; Fang, Z.; Yang, Q.; Zhang, H.; Cai, M.; Shi, L.; Dong, H.; Xiong, L. Neuroprotective gases—Fantasy or reality for clinical use? Prog. Neurobiol. 2014, 115, 210–245. [Google Scholar] [CrossRef] [PubMed]
- Altay, O.; Suzuki, H.; Hasegawa, Y.; Ostrowski, R.P.; Tang, J.; Zhang, J.H. Isoflurane on brain inflammation. Neurobiol. Dis. 2014, 62, 365–371. [Google Scholar] [CrossRef] [PubMed]
- Bickler, P.E.; Warner, D.S.; Stratmann, G.; Schuyler, J.A. Gamma-Aminobutyric acid-A receptors contribute to isoflurane neuroprotection in organotypic hippocampal cultures. Anesth. Analg. 2003, 97, 564–571. [Google Scholar] [CrossRef] [PubMed]
- Wang, L.; Traystman, R.J.; Murphy, S.J. Inhalational anesthetics as preconditioning agents in ischemic brain. Curr. Opin. Pharmacol. 2008, 8, 104–110. [Google Scholar] [CrossRef]
- Jiang, J.; Jiang, H. Effect of the inhaled anesthetics isoflurane, sevoflurane and desflurane on the neuropathogenesis of Alzheimer’s disease (review). Mol. Med. Rep. 2015, 12, 3–12. [Google Scholar] [CrossRef] [PubMed]
- Tadler, S.C.; Mickey, B.J. Emerging evidence for antidepressant actions of anesthetic agents. Curr. Opin. Anaesthesiol. 2018, 31, 439–445. [Google Scholar] [CrossRef] [PubMed]
- Newberg, L.A.; Milde, J.H.; Michenfelder, J.D. The cerebral metabolic effects of isoflurane at and above concentrations that suppress cortical electrical activity. Anesthesiology 1983, 59, 23–28. [Google Scholar] [CrossRef]
- Sakai, E.M.; Connolly, L.A.; Klauck, J.A. Inhalation anesthesiology and volatile liquid anesthetics: Focus on isoflurane, desflurane, and sevoflurane. Pharmacotherapy 2005, 25, 1773–1788. [Google Scholar] [CrossRef]
- Lattermann, R.; Schricker, T.; Wachter, U.; Georgieff, M.; Goertz, A. Understanding the mechanisms by which isoflurane modifies the hyperglycemic response to surgery. Anesth. Analg. 2001, 93, 121–127. [Google Scholar] [CrossRef] [PubMed]
- Saha, J.K.; Xia, J.; Grondin, J.M.; Engle, S.K.; Jakubowski, J.A. Acute hyperglycemia induced by ketamine/xylazine anesthesia in rats: Mechanisms and implications for preclinical models. Exp. Biol. Med. Maywood. 2005, 230, 777–7784. [Google Scholar] [CrossRef] [PubMed]
- Ljungqvist, O.; Jonathan, E. Rhoads lecture 2011: Insulin resistance and enhanced recovery after surgery. J. Parenter. Enteral. Nutr. 2012, 36, 389–398. [Google Scholar] [CrossRef] [PubMed]
- Tanaka, K.; Kehl, F.; Gu, W.; Krolikowski, J.G.; Pagel, P.S.; Warltier, D.C.; Kersten, J.R. Isoflurane-induced preconditioning is attenuated by diabetes. Am. J. Physiol. Heart Circ. Physiol. 2002, 282, 2018–2023. [Google Scholar] [CrossRef]
- Tanaka, K.; Weihrauch, D.; Ludwig, L.M.; Kersten, J.R.; Pagel, P.S.; Warltier, D.C. Mitochondrial adenosine triphosphate-regulated potassium channel opening acts as a trigger for isoflurane-induced preconditioning by generating reactive oxygen species. Anesthesiology 2003, 98, 935–943. [Google Scholar] [CrossRef]
- Ari, C.; Kovács, Z.; Juhasz, G.; Murdun, C.; Goldhagen, C.R.; Koutnik, A.M.; Poff, A.M.; Kesl, S.L.; D’Agostino, D. Exogenous ketone supplements reduce anxiety-related behavior in Sprague-Dawley and Wistar Albino Glaxo/Rijswijk rats. Front. Mol. Neurosci. 2016, 9, 137. [Google Scholar] [CrossRef] [PubMed]
- Hashim, S.A.; VanItallie, T.B. Ketone body therapy: From the ketogenic diet to the oral administration of ketone ester. J. Lipid Res. 2014, 55, 1818–1826. [Google Scholar] [CrossRef]
- Stubbs, B.J.; Cox, P.J.; Evans, R.D.; Santer, P.; Miller, J.J.; Faull, O.K.; Magor-Elliott, S.; Hiyama, S.; Stirling, M.; Clarke, K. On the metabolism of exogenous ketones in humans. Front. Physiol. 2017, 8, 848. [Google Scholar] [CrossRef]
- Kovács, Z.; D’Agostino, D.P.; Dobolyi, A.; Ari, C. Adenosine A1 receptor antagonism abolished the anti-seizure effects of exogenous ketone supplementation in Wistar Albino Glaxo Rijswijk rats. Front. Mol. Neurosci. 2017, 10, 235. [Google Scholar] [CrossRef]
- Kovács, Z.; D’Agostino, D.P.; Ari, C. Anxiolytic effect of exogenous ketone supplementation is abolished by adenosine A1 receptor inhibition in Wistar Albino Glaxo/Rijswijk rats. Front. Behav. Neurosci. 2018, 12, 29. [Google Scholar] [CrossRef]
- Constantinides, C.; Murphy, K. Molecular and integrative physiological effects of isoflurane anesthesia: The paradigm of cardiovascular studies in rodents using magnetic resonance imaging. Front. Cardiovasc. Med. 2016, 3, 23. [Google Scholar] [CrossRef] [PubMed]
- Hallböök, T.; Lundgren, J.; Rosén, I. Ketogenic diet improves sleep quality in children with therapy-resistant epilepsy. Epilepsia 2007, 48, 59–65. [Google Scholar] [CrossRef] [PubMed]
- Kovács, Z.; D’Agostino, D.P.; Ari, C. Ketone supplementation abolished isoflurane anesthesia-induced elevation in blood glucose level and increased recovery time from anesthesia in Wistar Albino Glaxo Rijswijk rats. BMC Anesthesiol. 2023, 23, 43. [Google Scholar] [CrossRef] [PubMed]
- Kovács, Z.; Brunner, B.; D’Agostino, D.P.; Ari, C. Inhibition of adenosine A1 receptors abolished the nutritional ketosis-evoked delay in the onset of isoflurane-induced anesthesia in Wistar Albino Glaxo Rijswijk rats. BMC Anesthesiol. 2020, 20, 30. [Google Scholar] [CrossRef] [PubMed]
- Sharma, A.K.; Rani, E.; Waheed, A.; Rajput, S.K. Pharmacoresistant epilepsy: A current update on non-conventional pharmacological and non-pharmacological interventions. J. Epilepsy Res. 2015, 5, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Yang, Q.; Guo, M.; Wang, X.; Zhao, Y.; Zhao, Q.; Ding, H.; Dong, Q.; Cui, M. Ischemic preconditioning with a ketogenic diet improves brain ischemic tolerance through increased extracellular adenosine levels and hypoxia-inducible factors. Brain Res. 2017, 1667, 11–18. [Google Scholar] [CrossRef] [PubMed]
- Kawamura, M., Jr.; Ruskin, D.N.; Masino, S.A. Metabolic autocrine regulation of neurons involves cooperation among pannexin hemichannels, adenosine receptors, and KATP channels. J. Neurosci. 2010, 30, 3886–3895. [Google Scholar] [CrossRef] [PubMed]
- Ribeiro, J.A. Purinergic inhibition of neurotransmitter release in the central nervous system. Pharmacol. Toxicol. 1995, 77, 299–305. [Google Scholar] [CrossRef] [PubMed]
- Gettys, G.C.; Liu, F.; Kimlin, E.; Baghdoyan, H.A.; Lydic, R. Adenosine A(1) receptors in mouse pontine reticular formation depress breathing, increase anesthesia recovery time, and decrease acetylcholine release. Anesthesiology 2013, 118, 327–336. [Google Scholar] [CrossRef]
- Kovács, Z.; Brunner, B.; D’Agostino, D.P.; Ari, C. Age- and Sex-Dependent Modulation of Exogenous Ketone Supplement-Evoked Effects on Blood Glucose and Ketone Body Levels in Wistar Albino Glaxo Rijswijk Rats. Front. Neurosci. 2021, 14, 618422. [Google Scholar] [CrossRef]
- Leung, L.S.; Luo, T.; Ma, J.; Herrick, I. Brain areas that influence general anesthesia. Prog. Neurobiol. 2014, 122, 24–44. [Google Scholar] [CrossRef]
- Wang, L.; Holland, L.; Fong, R.; Khokhar, S.; Fox, A.P.; Xie, Z. A pilot study showing that repeated exposure to stress produces alterations in subsequent responses to anesthetics in rats. PLoS ONE 2019, 14, e0214093. [Google Scholar] [CrossRef] [PubMed]
- Turina, M.; Miller, F.N.; Tucker, C.F.; Polk, H.C. Short-term hyperglycemia in surgical patients and a study of related cellular mechanisms. Ann. Surg. 2006, 243, 845–851. [Google Scholar] [CrossRef] [PubMed]
- Warner, D.S.; Gionet, T.X.; Todd, M.M.; McAllister, A.M. Insulin-induced normoglycemia improves ischemic outcome in hyperglycemic rats. Stroke 1992, 23, 1775–1780. [Google Scholar] [CrossRef] [PubMed]
- Tanaka, T.; Nabatame, H.; Tanifuji, Y. Insulin secretion and glucose utilization are impaired under general anesthesia with sevoflurane as well as isoflurane in a concentration-independent manner. J. Anesth. 2005, 19, 277–281. [Google Scholar] [CrossRef] [PubMed]
- Tanaka, K.; Kawano, T.; Tomino, T.; Kawano, H.; Okada, T.; Oshita, S.; Takahashi, A.; Nakaya, Y. Mechanisms of impaired glucose tolerance and insulin secretion during isoflurane anesthesia. Anesthesiology 2009, 111, 1044–1051. [Google Scholar] [CrossRef]
- Kashiwaya, Y.; Pawlosky, R.; Markis, W.; King, M.T.; Bergman, C.; Srivastava, S.; Murray, A.; Clarke, K.; Veech, R.L. A ketone ester diet increases brain malonyl-CoA and Uncoupling proteins 4 and 5 while decreasing food intake in the normal Wistar Rat. J. Biol. Chem. 2010, 285, 25950–25956. [Google Scholar] [CrossRef] [PubMed]
- Sato, K.; Kashiwaya, Y.; Keon, C.; Tsuchiya, N.; King, M.T.; Radda, G.K.; Chance, B.; Clarke, K.; Veech, R.L. Insulin, ketone bodies, and mitochondrial energy transduction. FASEB J. 1995, 9, 651–658. [Google Scholar] [CrossRef] [PubMed]
- Faulhaber-Walter, R.; Jou, W.; Mizel, D.; Li, L.; Zhang, J.; Kim, S.M.; Huang, Y.; Chen, M.; Briggs, J.P.; Gavrilova, O.; et al. Impaired glucose tolerance in the absence of adenosine A1 receptor signaling. Diabetes 2011, 60, 2578–2587. [Google Scholar] [CrossRef]
- Dong, Q.; Ginsberg, H.N.; Erlanger, B.F. Overexpression of the A1 adenosine receptor in adipose tissue protects mice from obesity-related insulin resistance. Diabetes Obes. Metab. 2001, 3, 360–366. [Google Scholar] [CrossRef]
- Dhalla, A.K.; Wong, M.Y.; Voshol, P.J.; Belardinelli, L.; Reaven, G.M. A1 adenosine receptor partial agonist lowers plasma FFA and improves insulin resistance induced by high-fat diet in rodents. Am. J. Physiol. Endocrinol. Metab. 2007, 292, 1358–1363. [Google Scholar] [CrossRef] [PubMed]
- Töpfer, M.; Burbiel, C.E.; Müller, C.E.; Knittel, J.; Verspohl, E.J. Modulation of insulin release by adenosine A1 receptor agonists and antagonists in INS-1 cells: The possible contribution of 86Rb+ efflux and 45Ca2+ uptake. Cell Biochem. Funct. 2008, 26, 833–843. [Google Scholar] [CrossRef] [PubMed]
- Fong, R.; Wang, L.; Zacny, J.P.; Khokhar, S.; Apfelbaum, J.L.; Fox, A.P.; Xie, Z. Caffeine accelerates emergence from isoflurane anesthesia in humans: A randomized, double-blind, crossover study. Anesthesiology 2018, 129, 912–920. [Google Scholar] [CrossRef] [PubMed]
- Van Dort, C.J.; Baghdoyan, H.A.; Lydic, R. Adenosine A(1) and A(2A) receptors in mouse prefrontal cortex modulate acetylcholine release and behavioral arousal. J. Neurosci. 2009, 29, 871–881. [Google Scholar] [CrossRef]
- Wang, Q.; Fong, R.; Mason, P.; Fox, A.P.; Xie, Z. Caffeine accelerates recovery from general anesthesia. J. Neurophysiol. 2014, 111, 1331–1340. [Google Scholar] [CrossRef] [PubMed]
- Kovács, Z.; Juhász, G.; Palkovits, M.; Dobolyi, A.; Kékesi, K.A. Area, age and gender dependence of the nucleoside system in the brain: A review of current literature. Curr. Top. Med. Chem. 2011, 11, 1012–1033. [Google Scholar] [CrossRef]
- Lu, H.; Chen, C.; Klaassen, C. Tissue distribution of concentrative and equilibrative nucleoside transporters in male and female rats and mice. Drug Metab. Dispos. 2004, 32, 1455–1461. [Google Scholar] [CrossRef] [PubMed]
- Rucker, B.; Pereira, G.S.; Furstenau, C.R.; Izquierdo, I.; Bonan, C.D.; Sarkis, J.J. Inhibitory avoidance task reveals differences in ectonucleotidase activities between male and female rats. Neurochem. Res. 2004, 29, 2231–2237. [Google Scholar] [CrossRef] [PubMed]
- Mansouri, M.T.; Fidler, J.A.; Meng, Q.C.; Eckenhoff, R.G.; García, P.S. Sex effects on behavioral markers of emergence from propofol and isoflurane anesthesia in rats. Behav. Brain Res. 2019, 367, 59–67. [Google Scholar] [CrossRef]
- Vincent, K.F.; Mallari, O.G.; Dillon, E.J.; Stewart, V.G.; Cho, A.J.; Dong, Y.; Edlow, A.G.; Ichinose, F.; Xie, Z.; Solt, K. Oestrous cycle affects emergence from anaesthesia with dexmedetomidine, but not propofol, isoflurane, or sevoflurane, in female rats. Br. J. Anaesth. 2023, 131, 67–78. [Google Scholar] [CrossRef]
- Newman, J.C.; Verdin, E. Ketone bodies as signaling metabolites. Trends Endocrinol. Metab. 2014, 25, 42–52. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
| Treatments | Glucose (mg/dL) | R-βHB (mmol/L) |
|---|---|---|
| Group 1 | ||
| Control | 84.43 ± 1.775 | 0.75 ± 0.027 |
| 12th day of experiments | 130.07 ± 4.748 ****/<0.0001 | 1.13 ± 0.027 ****/<0.0001 |
| Group 2 | ||
| Control | 77.00 ± 1.816 | 0.79 ± 0.027 |
| 12th day of experiments | 123.00 ± 4.235 ****/<0.0001 | 1.13 ± 0.022 ****/<0.0001 |
| Group 3 | ||
| Control | 88.00 ± 1.371 | 0.79 ± 0.019 |
| 6th day of experiments | 65.71 ± 1.962 ****/<0.0001 | 2.94 ± 0.338 ****/<0.0001 |
| 12th day of experiments | 94.79 ± 3.015 ns/0.0913 | 4.18 ± 0.228 ****/<0.0001 |
| Group 4 | ||
| Control | 81.36 ± 1.833 | 0.80 ± 0.019 |
| 6th day of experiments | 62.29 ± 1.588 ***/0.0005 | 2.56 ± 0.146 ****/<0.0001 |
| 12th day of experiments | 126.14 ± 5.122 ****/<0.0001 | 4.00 ± 0.228 ****/<0.0001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rauch, E.; Ari, C.; D’Agostino, D.P.; Kovács, Z. Exogenous Ketone Supplement Administration Abrogated Isoflurane-Anesthesia-Induced Increase in Blood Glucose Level in Female WAG/Rij Rats. Nutrients 2024, 16, 1477. https://doi.org/10.3390/nu16101477
Rauch E, Ari C, D’Agostino DP, Kovács Z. Exogenous Ketone Supplement Administration Abrogated Isoflurane-Anesthesia-Induced Increase in Blood Glucose Level in Female WAG/Rij Rats. Nutrients. 2024; 16(10):1477. https://doi.org/10.3390/nu16101477
Chicago/Turabian StyleRauch, Enikő, Csilla Ari, Dominic P. D’Agostino, and Zsolt Kovács. 2024. "Exogenous Ketone Supplement Administration Abrogated Isoflurane-Anesthesia-Induced Increase in Blood Glucose Level in Female WAG/Rij Rats" Nutrients 16, no. 10: 1477. https://doi.org/10.3390/nu16101477