Interleukin-6 Gene Promoter-572 C Allele May Play a Role in Rate of Disease Progression in Multiple Sclerosis

Abstract
:1. Introduction
2. Results and Discussion
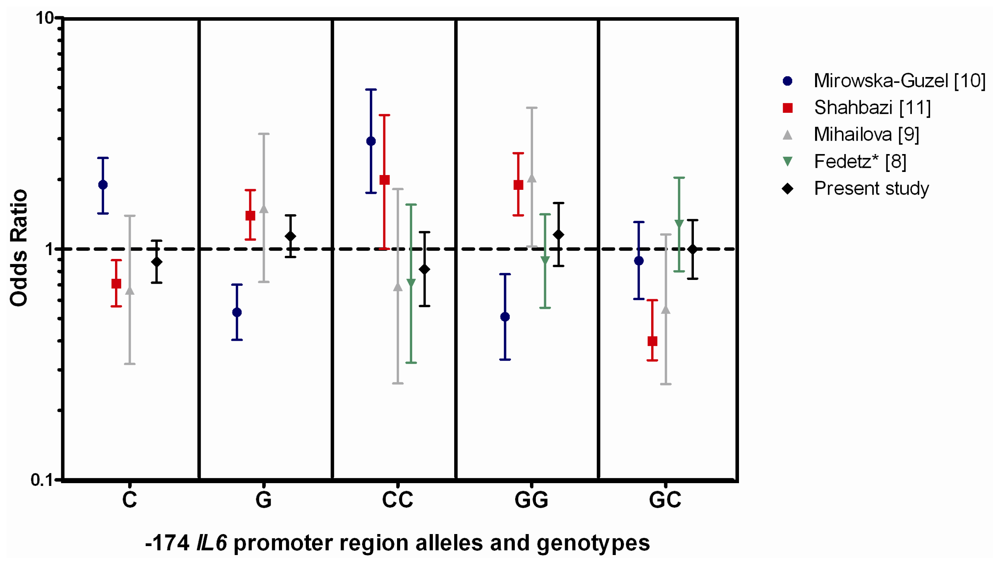
2.1. Allelic and Genotypic Frequency of the IL6 Promoter Region Polymorphisms
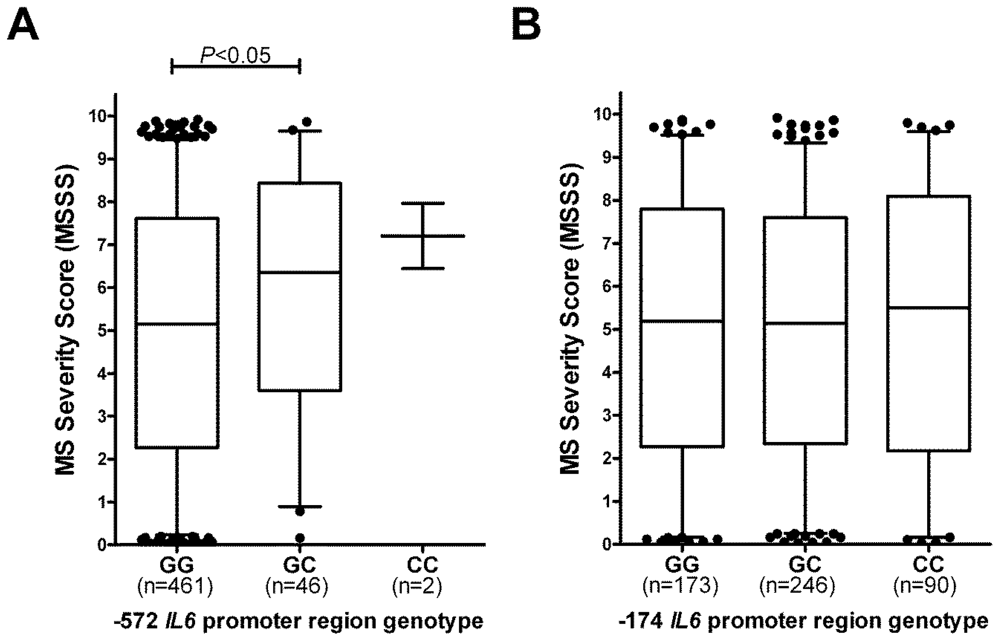
2.2. −572 IL6 Promoter Region Genotypes, but not −172 Genotypes, Associate with MS Severity
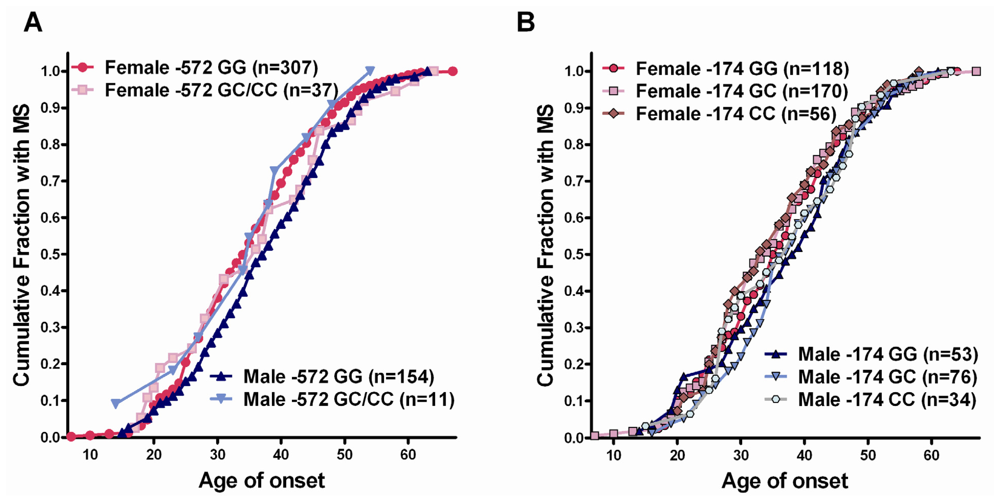
2.2.1. Interaction of Gender with Genotype
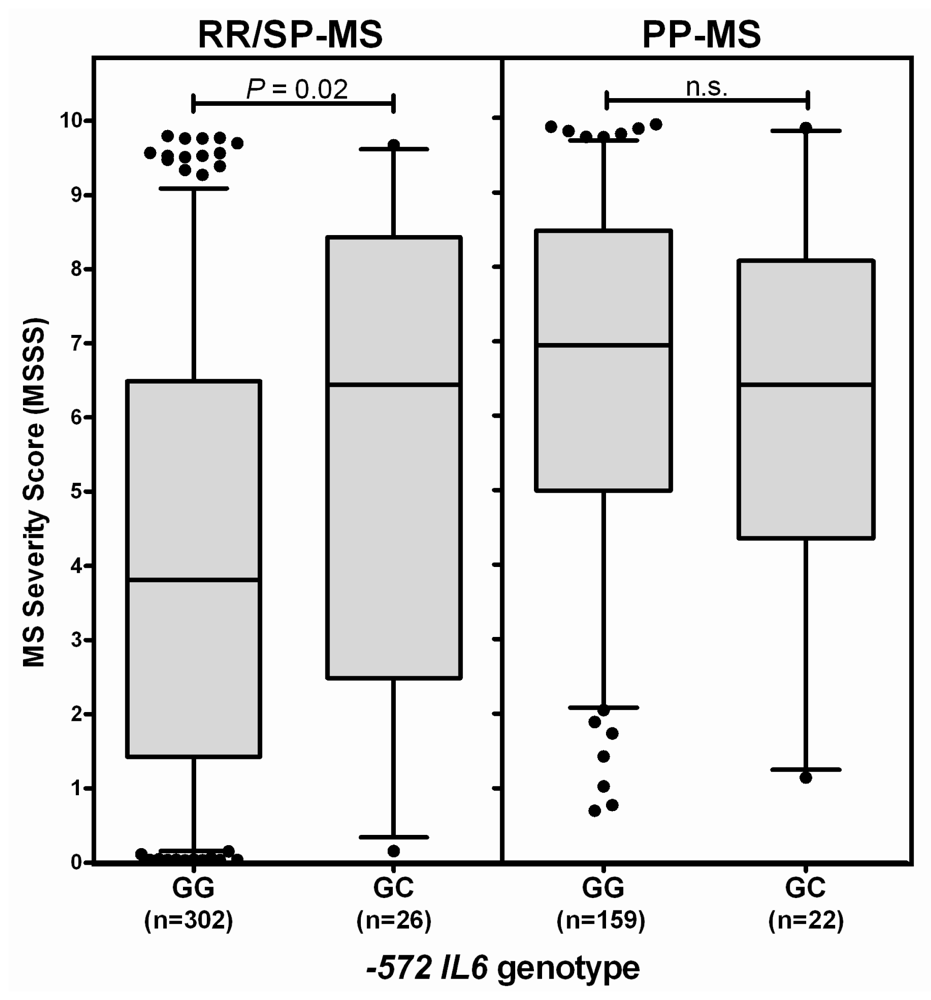
2.2.2. The −572 IL6 GC Genotype Association with MS Severity is Most Noticeable in Patients Who Initially Have RR-MS
2.2.3. Interaction of HLA Type with IL6 Promoter Region Genotype
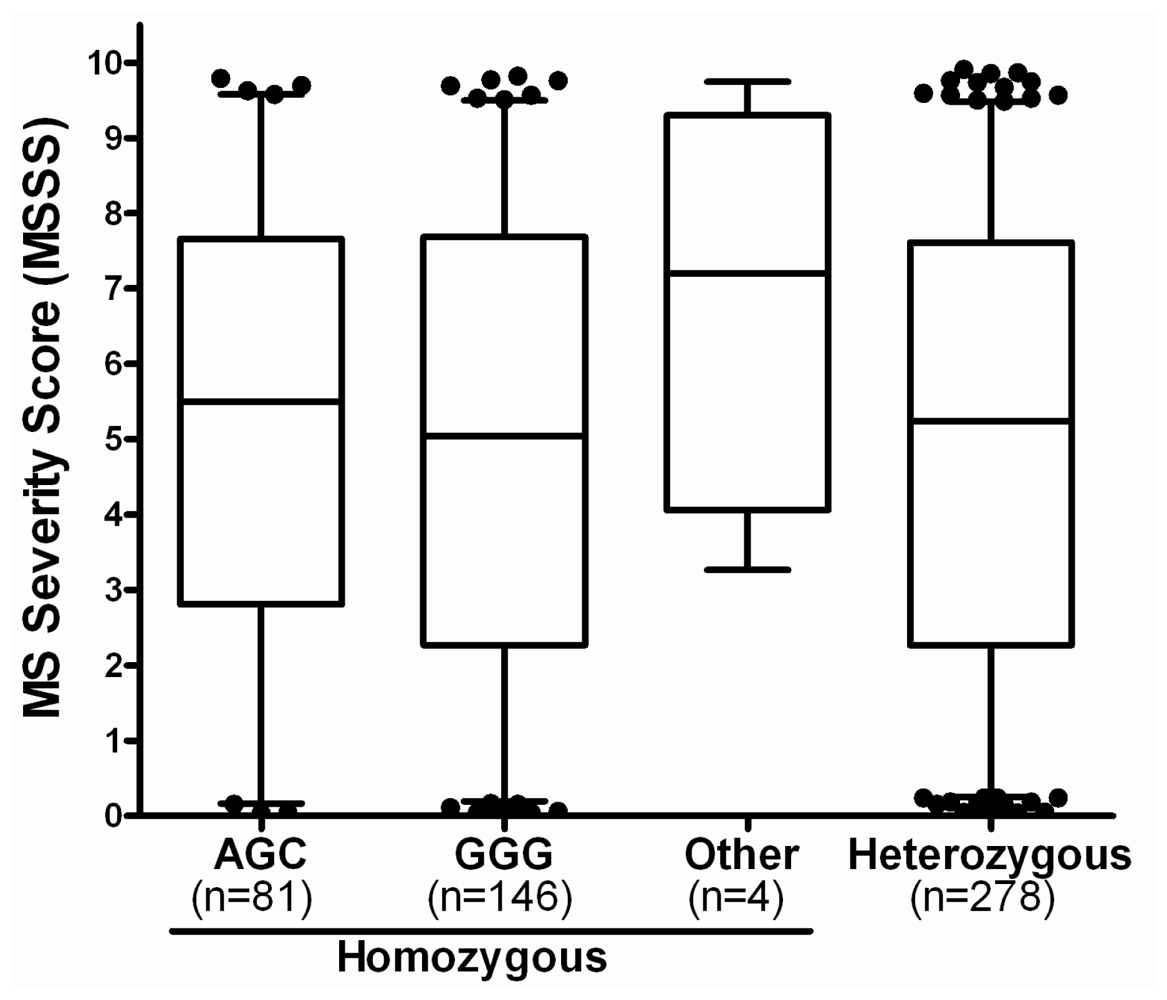
2.3. Haplotypes of the IL6 Promoter Region Polymorphisms
3. Experimental Section
3.1. Patients and Controls
3.2. Genomic DNA Isolation and Sequencing
3.3. Data Analysis
4. Conclusions
Acknowledgments
References
- Pender, M.P.; Greer, J.M. Immunology of multiple sclerosis. Curr. Allergy Asthma Rep 2007, 7, 285–292. [Google Scholar]
- Montalban, X. Primary progressive multiple sclerosis. Curr. Opin. Neurol 2005, 18, 261–266. [Google Scholar]
- Ebers, G.C. Natural history of primary progressive multiple sclerosis. Mult. Scler 2004, 10, S8–S15. [Google Scholar]
- McFarland, H.F.; Martin, R. Multiple sclerosis: A complicated picture of autoimmunity. Nat. Immunol 2007, 8, 913–919. [Google Scholar]
- The International Multiple Sclerosis Genetics Consortium. The Wellcome Trust Case Control Consortium Genetic risk and a primary role for cell-mediated immune mechanisms in multiple sclerosis. Nature 2011, 476, 214–219.
- Bahlo, M.; Booth, D.R.; Broadley, S.A.; Brown, M.A.; Foote, S.J.; Griffiths, L.R.; Kipatrick, T.J.; Lechner-Scott, J.; Moscato, P.; Perreau, V.M.; et al. Genome-wide association study identifies new multiple sclerosis susceptibility loci on chromosomes 12 and 20. Nat. Genet 2009, 41, 824–828. [Google Scholar]
- Patsopoulos, N.A.; Bayer Pharma, M.S. Genetics Working Group. Steering Committees of Studies Evaluating IFNβ-1b and a CCR1-Antagonist.Esposito, F.; Reischl, J.; Lehr, S.; Bauer, D.; et al. ANZgene Consortium; GeneMSA; International Multiple Sclerosis Genetics Consortium. Genome-wide meta-analysis identifies novel multiple sclerosis susceptibility loci. Ann. Neurol 2011, 70, 897–912. [Google Scholar]
- Fedetz, M.; Matesanz, F.; Pascual, M.; Martin, J.; Fernandez, O.; Guerrero, M.; Alcina, A. The -174/-597 promoter polymorphisms in the interleukin-6 gene are not associated with susceptibility to multiple sclerosis. J. Neurol. Sci 2001, 190, 69–72. [Google Scholar]
- Mihailova, S.; Ivanova, M.; Mihaylova, A.; Quin, L.; Mikova, O.; Naumova, E. Pro- and anti-inflammatory cytokine gene polymorphism profiles in Bulgarian multiple sclerosis patients. J. Neuroimmunol 2005, 168, 138–143. [Google Scholar]
- Mirowska-Guzel, D.; Gromadzka, G.; Mach, A.; Czlonkowski, A.; Czlonkowska, A. Association of IL1A, IL1B, ILRN, IL6, IL10 and TNF-alpha polymorphisms with risk and clinical course of multiple sclerosis in a Polish population. J. Neuroimmunol 2011, 236, 87–92. [Google Scholar]
- Shahbazi, M.; Ebadi, H.; Fathi, D.; Roshandel, D.; Mohamadhosseni, M.; Tahmasebi, A.; Shahbazi, S.; Zamani, M.; Rashidbaghan, A. HLA-DRB1*1501 intensifies the impact of IL-6 promoter polymorphism on the susceptibility to multiple sclerosis in an Iranian population. Mult. Scler 2010, 16, 1173–1177. [Google Scholar]
- Maimone, D.; Gregory, S.; Arnason, B.G.; Reder, A.T. Cytokine levels in the cerebrospinal fluid and serum of patients with multiple sclerosis. J. Neuroimmunol 1991, 32, 67–74. [Google Scholar]
- Stelmasiak, Z.; Koziol-Montewka, M.; Dobosz, B.; Rejdak, K.; Bartosik-Psujek, H.; Mitosek-Szewczyk, K.; Belniak-Legiec, E. Interleukin-6 concentration in serum and cerebrospinal fluid in multiple sclerosis patients. Med. Sci. Monit 2000, 6, 1104–1108. [Google Scholar]
- Ireland, S.J.; Blazek, M.; Harp, C.T.; Greenberg, B.; Frohman, E.M.; Davis, L.S.; Monson, N.L. Antibody-independent B cell effector functions in relapsing remitting multiple sclerosis: Clues to increased inflammatory and reduced regulatory B cell capacity. Autoimmunity 2012, 45, 400–414. [Google Scholar]
- Maimone, D.; Guazzi, G.C.; Annunziata, P. IL-6 detection in multiple sclerosis brain. J. Neurol. Sci 1997, 146, 59–65. [Google Scholar]
- Eugster, H.P.; Frei, K.; Kopf, M.; Lassmann, H.; Fontana, A. IL-6-deficient mice resist myelin oligodendrocyte glycoprotein-induced autoimmune encephalomyelitis. Eur. J. Immunol 1998, 28, 2178–2187. [Google Scholar]
- Fife, M.S.; Ogilvie, E.M.; Kelberman, D.; Samuel, J.; Gutierrez, A.; Humphries, S.E.; Woo, P. Novel IL-6 haplotypes and disease association. Genes Immun 2005, 6, 367–370. [Google Scholar]
- Fishman, D.; Faulds, G.; Jeffery, R.; Mohamed-Ali, V.; Yudkin, J.S.; Humphries, S.; Woo, P. The effect of novel polymorphisms in the interleukin-6 (IL-6) gene on IL-6 transcription and plasma IL-6 levels, and an association with systemic-onset juvenile chronic arthritis. J. Clin. Invest 1998, 102, 1369–1376. [Google Scholar]
- Muller-Steinhardt, M.; Fricke, L.; Muller, B.; Ebel, B.; Kirchner, H.; Hartel, C. Cooperative influence of the interleukin-6 promoter polymorphisms −597, −572 and −174 on long-term kidney allograft survival. Am. J. Transpl 2004, 4, 402–406. [Google Scholar]
- Roxburgh, R.H.; Seaman, S.R.; Masterman, T.; Hensiek, A.E.; Sawcer, S.J.; Vukusic, S.; Achiti, I.; Confavreux, C.; Coustans, M.; le Page, E.; et al. Multiple sclerosis severity score: Using disability and disease duration to rate disease severity. Neurology 2005, 64, 1144–1151. [Google Scholar]
- Kristiansen, O.P.; Nolsøe, R.L.; Larsen, L.; Gjesing, A.M.P.; Johannesen, J.; Larsen, Z.M.; Lykkesfeldt, A.E.; Karlsen, A.E.; Pociot, F.; Mandrup-Poulsen, T. DIEGG;DSGD. Association of a functional 17β-estradiol sensitive IL6-174G/C promoter polymorphism with early-onset type 1 diabetes in females. Hum. Mol. Genet 2003, 12, 1101–1110. [Google Scholar]
- Sadovnick, A.D. European Charcot Foundation Lecture: The natural history of multiple sclerosis and gender. J. Neurol. Sci 2009, 286, 1–5. [Google Scholar]
- Polman, C.H.; Reingold, S.C.; Edan, G.; Filippi, M.; Hartung, H.P.; Kappos, L.; Lublin, F.D.; Metz, L.M.; McFarland, H.F.; O’Connor, P.W.; et al. Diagnostic criteria for multiple sclerosis: 2005 revisions to the “McDonald Criteria”. Ann. Neurol 2005, 58, 840–846. [Google Scholar]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Group | n | % Female | Age (Mean ± SE) | MSSS * median (IQR) |
|---|---|---|---|---|
| Healthy controls | 279 | 63.1% | 42 ± 1.0 | not applicable |
| Multiple sclerosis | ||||
| All | 509 | 68.4% | 52.8 ± 0.5 | 5.24 (2.33–7.66) |
| RR-MS | 156 | 82.1% † | 46.6 ± 0.9 | 1.73 (0.49–3.42) |
| SP-MS | 172 | 69.2% | 53.4 ± 0.8 | 6.28 (4.13–8.20) |
| PP-MS | 181 | 56.9% | 57.6 ± 0.7 | 6.90 (4.82–8.49) |
| Allele/genotype | Healthy controls | Multiple sclerosis | Puncorrected vs. healthy controls | |||||
|---|---|---|---|---|---|---|---|---|
| All | RR-MS | SP-MS | PP-MS | |||||
| −597 | G | 318 (57.0%) | 607 (59.6%) | 182 (58.3%) | 209 (60.8%) | 216 (59.7%) |  | n.s. |
| A | 240 (43.0%) | 411 (40.4%) | 130 (41.7%) | 135 (39.2%) | 146 (40.3%) | |||
| GG | 94 (33.7%) | 181 (35.6%) | 54 (34.6%) | 64 (37.2%) | 63 (34.8%) | n.s. | ||
| GA | 130 (46.6%) | 245 (48.1%) | 74 (47.4%) | 81 (47.1%) | 90 (49.7%) | n.s. | ||
| AA | 55 (19.7%) | 83 (16.3%) | 28 (17.9%) | 27 (15.7%) | 28 (15.5%) | n.s. | ||
| −572 | G | 517 (92.7%) | 968 (95.1%) | 301 (96.5%) | 328 (95.3%) | 339 (93.6%) | | 0.047 (all MS); |
| C | 41 (7.3%) | 50 (4.9%) | 11 (3.5%) | 16 (4.7%) | 23 (6.4%) | 0.03 (RR-MS) | ||
| GG | 244 (87.5%) | 461 (90.6%) | 145 (92.9%) | 157 (91.3%) | 159 (87.8%) | n.s. | ||
| GC | 29 (10.4%) | 46 (9.0%) | 11 (7.1%) | 14 (8.1%) | 21 (11.6%) | n.s. | ||
| CC | 6 (2.2%) | 2 (0.4%) | 0 (0%) | 1 (0.6%) | 1 (0.6%) | 0.047 (all MS) | ||
| −174 | G | 307 (55.0%) | 592 (58.2%) | 176 (56.4%) | 204 (59.3%) | 212 (58.6%) | | n.s. |
| C | 251 (45.0%) | 426 (41.8%) | 136 (43.6%) | 140 (40.7%) | 150 (41.4%) | |||
| GG | 86 (30.8%) | 173 (34.0%) | 50 (32.1%) | 62 (36.0%) | 61 (33.7%) | n.s. | ||
| GC | 135 (48.4%) | 246 (48.3%) | 76 (48.7%) | 80 (46.5%) | 90 (49.7%) | n.s. | ||
| CC | 58 (20.8%) | 90 (17.7%) | 30 (19.2%) | 30 (17.4%) | 30 (16.6%) | n.s. | ||
| Homozygous haplotype (−597, −572, −174) | Healthy controls (n = 124) | Multiple sclerosis | Puncorrected vs. healthy controls | |||
|---|---|---|---|---|---|---|
| All (n = 231) | RR-MS (n = 72) | SP-MS (n = 84) | PP-MS (n = 75) | |||
| GGG | 85 (68.5%) | 146 (63.2%) | 45 (62.5%) | 53 (63.1%) | 48 (64.0%) | n.s. |
| ACG | 39 (31.5%) | 81 (35.1%) | 27 (37.5%) | 29 (34.5%) | 25 (33.3%) | n.s. |
| Other | 0 (0%) | 4 (1.7%) | 0 (0%) | 2 (2.4%) | 2 (2.7%) | n.s. |
© 2012 by the authors; licensee Molecular Diversity Preservation International, Basel, Switzerland. This article is an open-access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/3.0/).
Share and Cite
Yan, J.; Liu, J.; Lin, C.Y.; ANZGene; Csurhes, P.A.; Pender, M.P.; McCombe, P.A.; Greer, J.M. Interleukin-6 Gene Promoter-572 C Allele May Play a Role in Rate of Disease Progression in Multiple Sclerosis. Int. J. Mol. Sci. 2012, 13, 13667-13679. https://doi.org/10.3390/ijms131013667
Yan J, Liu J, Lin CY, ANZGene, Csurhes PA, Pender MP, McCombe PA, Greer JM. Interleukin-6 Gene Promoter-572 C Allele May Play a Role in Rate of Disease Progression in Multiple Sclerosis. International Journal of Molecular Sciences. 2012; 13(10):13667-13679. https://doi.org/10.3390/ijms131013667
Chicago/Turabian StyleYan, Jun, Jia Liu, Clement Yihao Lin, ANZGene, Peter A. Csurhes, Michael P. Pender, Pamela A. McCombe, and Judith M. Greer. 2012. "Interleukin-6 Gene Promoter-572 C Allele May Play a Role in Rate of Disease Progression in Multiple Sclerosis" International Journal of Molecular Sciences 13, no. 10: 13667-13679. https://doi.org/10.3390/ijms131013667