1. Introduction
Lynch syndrome (also called hereditary non-polyposis colorectal cancer) is an autosomal dominant disorder that arises because of a germline mutation in at least one of four DNA mismatch repair (MMR) genes (MutL Homolog 1 (
MLH1), MutS Homolog 2 (
MSH2), MutS Homolog 6 (
MSH6), and PMS1 Homolog 2 (
PMS2)). Lynch syndrome is associated with the microsatellite instability (MSI)-high phenotype [
1]. Individuals who carry MMR mutations are at higher risk of developing a number of epithelial malignancies, such as colorectal, endometrial, ovarian, stomach, pancreas, small intestine, renal, ureteral, and brain cancer [
2,
3,
4,
5]. MMR gene mutations can be detected by a loss of expression of MMR proteins by immunohistochemistry. There is some evidence that MMR gene mutation carriers might be at increased risk of cervical cancer; however, it is currently uncertain whether cervical cancer is associated with Lynch syndrome. Herein, we report a case of Lynch syndrome-related clear cell carcinoma of the cervix with synchronous colorectal cancer, which could be distinguished from non-Lynch syndrome-related cervical cancer by immunohistochemical detection of MMR genes and MSI analysis.
2. Case
The study protocol was approved by the Ethics Committee of Shimane University Faculty of Medicine, Izumo, Japan (no. 960). The patient provided informed, written consent. A 42-year-old gravida 2, para 2 woman presented with abnormal vaginal bleeding in April 2017. Her medical history and family history were unremarkable. Levels of serum carbohydrate antigen 125 (CA 125), CA 19-9, carcinoembryonic antigen, and squamous cell carcinoma antigen were within the normal range. Her general examination was similarly unremarkable.
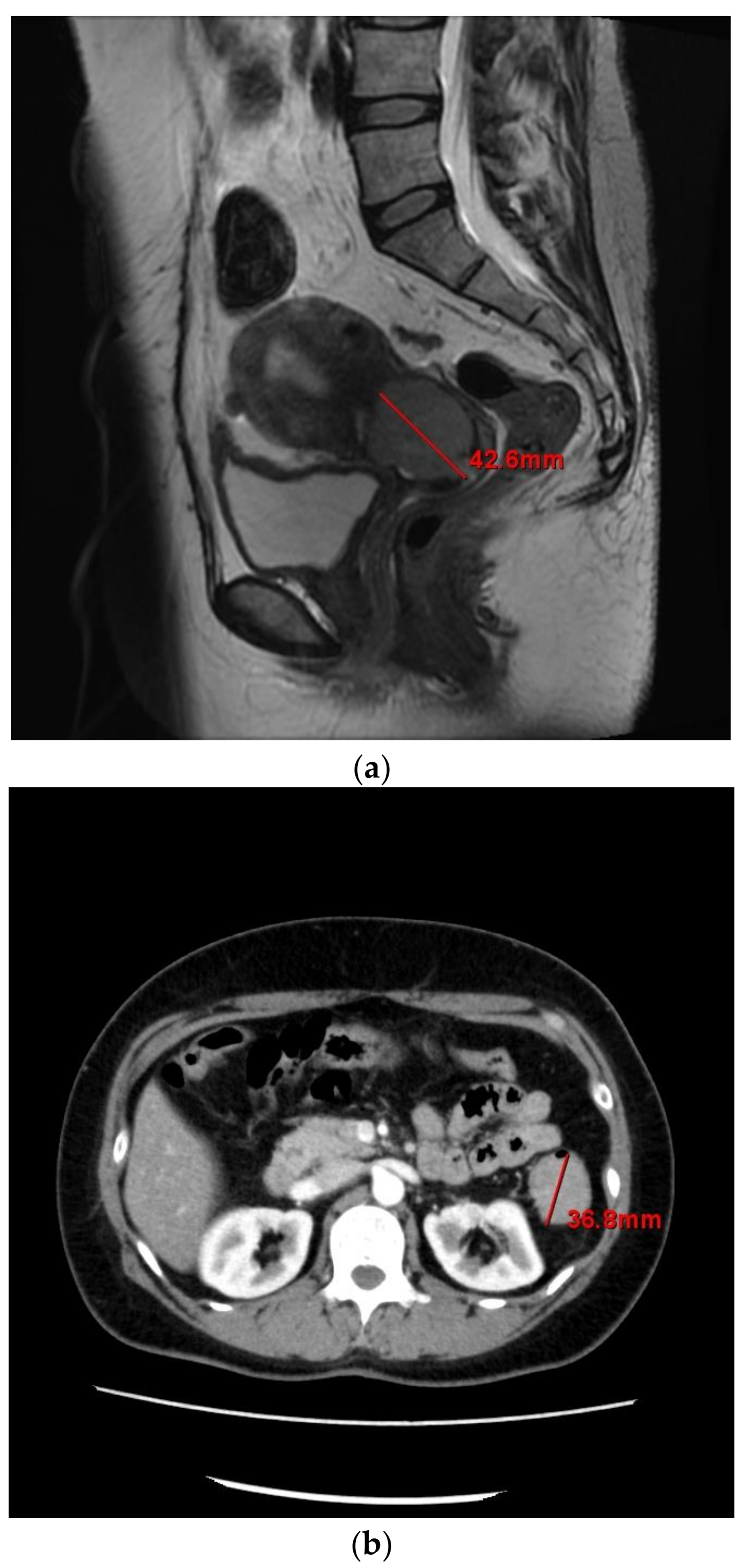
Pelvic magnetic resonance imaging indicated a tumor in the endocervix measuring 42 × 32 × 38 mm (
Figure 1a), and a tumor in the transverse colon measuring 36 mm in the largest diameter (
Figure 1b). It did not show peritonitis carcinomatosa, ascites, dissemination nodules, or metastasis to other organs. Contrast-enhanced computed tomography (CT) showed no lymphadenopathy. These findings suggested colorectal metastasis from cervical cancer or double cancer (cervical and colorectal cancer). Positron emission tomography-CT showed abnormal
18F-fluorodeoxyglucose uptake in the cervix and colorectum.
Endoscopic submucosal dissection was performed for the colorectal tumor in June 2017. The resected specimen was diagnosed as well to moderately differentiated adenocarcinoma (pT1N0M0) with negative margins. Next, radical hysterectomy, bilateral salpingo-oophorectomy, pelvic lymphadenectomy, and left hemicolectomy were performed in July 2017. After surgery, there was no visible residual disease in the pelvic region. The resected specimens in the cervix were reviewed by a pathologist and the mass was finally diagnosed as a 45 × 40 × 15-mm clear cell carcinoma of uterine cervix with lymphovascular invasion (pT2bN0M0). No tumor remained in the resected specimen in the colorectum. These findings confirmed double cancer.
The patient experienced an uneventful postoperative period and was discharged from the hospital on the 14th day after surgery. She was administered combination chemotherapy (paclitaxel 175 mg/m2 + carboplatin 700 mg/body) after the surgery and is tolerating her chemotherapy well and has remained asymptomatic and progression-free for eight months.
2.1. Pathological Findings
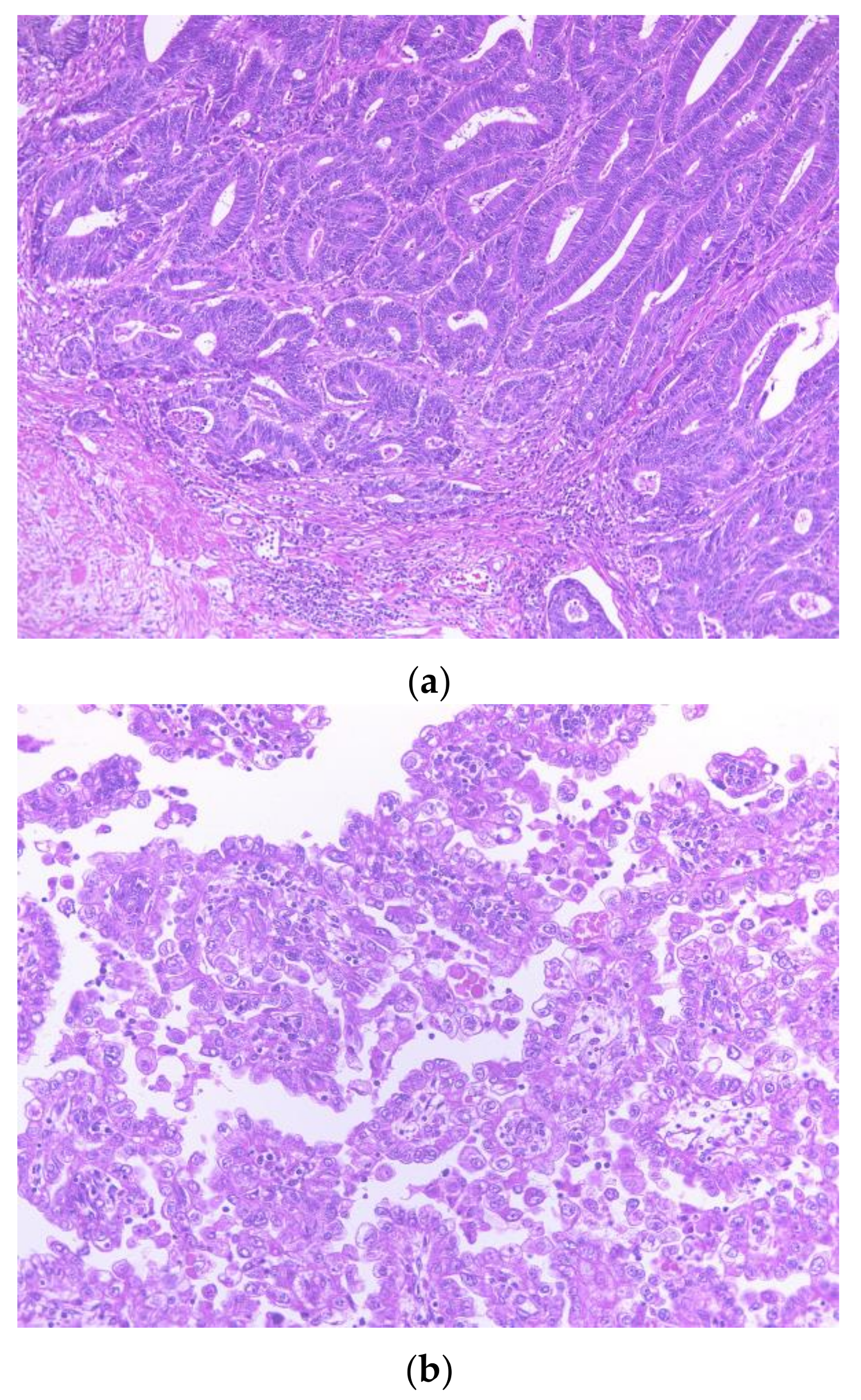
The colonic specimen showed that the tumor had invaded the submucosa, and lymphatic invasion was also identified (
Figure 2a). The cervical tumor showed a tubular pattern with a lining composed of hobnail, flat, and clear cells. There was also a papillotubular pattern visible with focal solid areas with a lining of glycogen-rich clear cell cytoplasm, as well as high-grade nuclear atypia (
Figure 2b). Histological examination revealed the absence of malignant cells in all resected samples, including the endometrium, ovaries, oviduct, cervical stump, parametria, vaginal cuff, infundibular pelvic ligaments, and pelvic nodes.
2.2. Immunohistochemical and MSI Analysis Findings
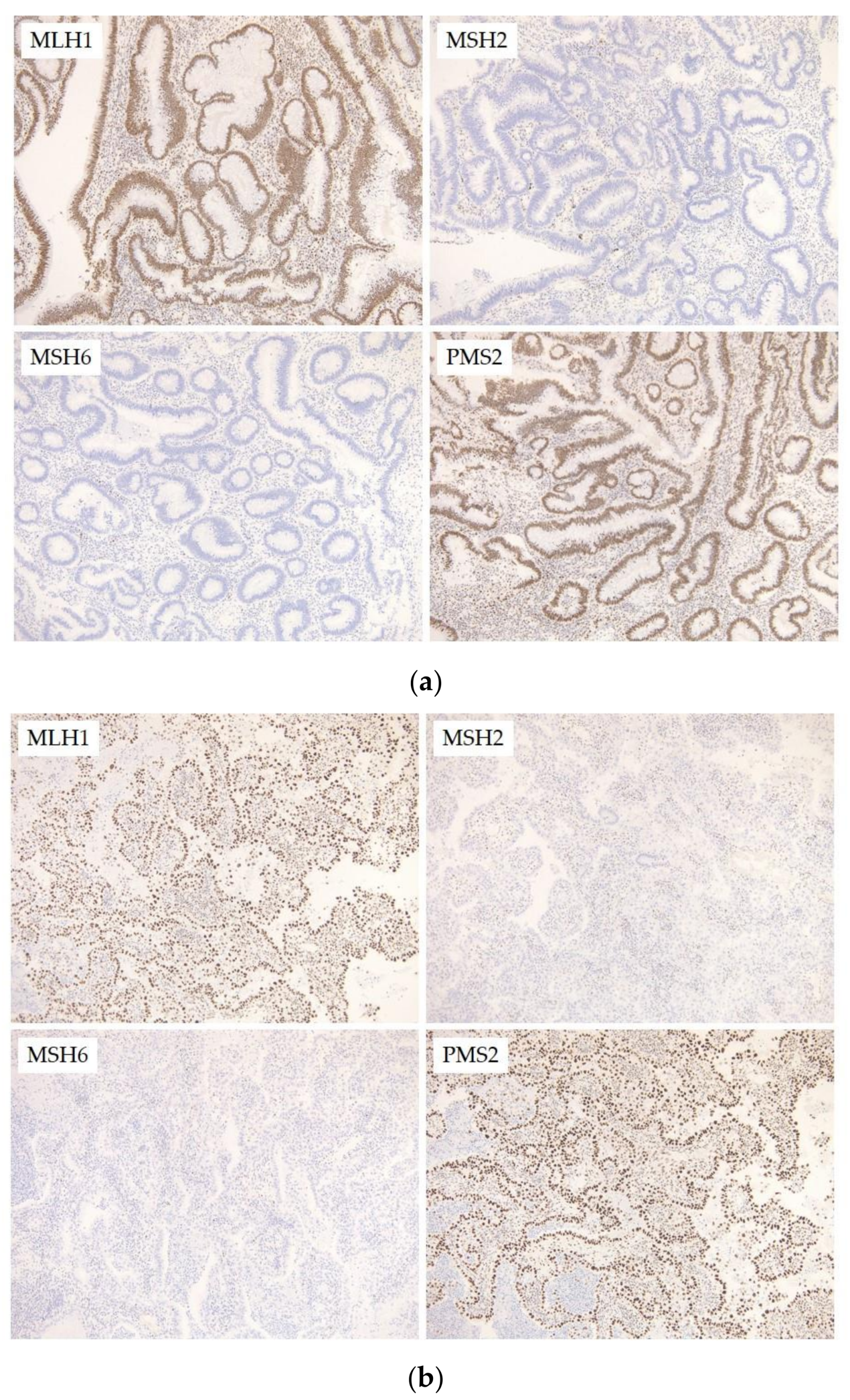
The colonic tumor was positive for MLH1 and PMS2, and showed no expression of MSH2 or MSH6, which was in agreement with the germline mutations in MSH2 and MSH6.
In the cervical tumor, the epithelial-like cells were strongly positive for hepatocyte nuclear factor 1β and p16. Napsin A was weakly expressed. The cells were negative for estrogen receptor, progesterone receptor, and vimentin. With regard to MMR gene expression, the tumor was positive for MLH1 and PMS2, and showed no expression of MSH2 or MSH6, which was in agreement with the germline mutation in MSH2 and MSH6 and consistent with the results from the colonic tumor.
For MSI analysis, genomic DNA was extracted from fresh tissue from the cervical tumor and blood samples using the QIAamp DNA Micro Kit (Qiagen, Valencia, CA, USA) according to the manufacturer’s standard protocol. We performed MSI analysis using the polymerase chain reaction (PCR) with eight microsatellite markers (BAT25, BAT26, D2S123, D5S346, D17S250, NR21, MONO27, and NR2). MSI analysis in the cervical tumor and blood using the National Cancer Institute panel revealed that the tumor had high MSI. Particularly, the cervical tumor showed instability in two microsatellite repeats (
Figure 3c), which is considered MSI-high.
3. Discussion
This study presents a fascinating case of Lynch syndrome-related colon cancer with synchronous clear cell carcinoma of the cervix.
Few case reports have described Lynch-related endocervical adenocarcinoma, the typical cervical cancer observed in women believed or shown to have MMR gene mutations [
6,
7,
8]. One case reported a germline mutation in
MSH2, in which the tumor was immunohistochemically deficient for MSH2 and MSH6 with high levels of MSI [
6], and another reported the Muir–Torre variant of Lynch syndrome, where individuals have defects in either
MSH2 or
MLH1 [
6,
7]. In the first case, there was no mention of tumor morphology [
6], whereas in the second, the neoplasm was described as an adenocarcinoma with focal serous papillary features [
7]. In the second case, there was no mention of testing the tumor for MSI or conducting immunohistochemistry for MMR proteins. A third report described a case of gastric-type adenocarcinoma of the cervix in a patient with Lynch syndrome secondary to a germline mutation in the
MSH6 MMR gene. However, MSI analysis was not performed [
8].
To the best of our knowledge, this is the first case of Lynch syndrome-related clear cell carcinoma of the cervix. Clear cell carcinomas of the cervix are rare and have occurred in two distinct situations: in association with in utero diethylstilbestrol (DES) exposure [
9] and sporadically [
10]. Our patient had not been exposed to DES, so this case was not thought to be caused by DES exposure.
The present case emphasizes the significance of examining a patient’s cancer genetics in hereditary cancer syndromes, especially if certain cancers conflict with known facts about the syndrome. Although Lynch syndrome is most often linked to colorectal and endometrial tumors, MMR gene mutation carriers commonly develop tumors at other sites at higher rates compared to those observed in the general population [
5,
11,
12]. Therefore, further studies should examine the contribution of MMR deficiency to tumorigenesis and include prospectively examined epidemiological data, tumor tissue, and tissue obtained following risk-reducing surgery in MMR gene mutation carriers, without discrimination against the involved organ. It is possible that cervical cancer in MMR gene mutation carriers may arise from the activation of tumorigenic pathways following human papilloma virus exposure. However, it is prudent to determine which organs are at higher risk of carcinogenesis with MMR deficiency. Such knowledge will allow for the identification of high-risk Lynch syndrome patients and the development of risk management strategies (individual and familial) and treatment regimens.
In summary, we describe the first case of Lynch syndrome-related clear cell carcinoma of the cervix, which indicates the possibility of an association between cervical cancer and Lynch syndrome. Suitable genetic tests for cancers are needed to determine if common genetics can account for synchronous or subsequent malignancies in patients with Lynch syndrome and their families. Such knowledge will enhance our understanding of the genetic mechanisms underlying apparently unrelated cancers.
Author Contributions
Kohei Nakamura drafted the manuscript. Toshiko Minamoto, Tomoka Ishibashi, Kaori Ohnishi and Hitomi Yamashita carried out the molecular genetic studies, participated in the sequence alignment. Ruriko Ono, Hiroki Sasamori, Sultana Razia, Mohammad Mahmud Hossain, Shanta Kamrunnahar and Noriyoshi Ishikawa carried out the staining. Masako Ishikawa participated in the sequence alignment. Kentaro Nakayama participated in the design of the study. Satoru Kyo conceived of the study, and participated in its design and coordination and helped to draft the manuscript. All authors read and approved the final manuscript.
Conflicts of Interest
The authors declare no conflict of interest.
Abbreviations
| MMR | mismatch repair |
| MLH1 | MutL Homolog 1 |
| MSH2 | MutS Homolog 2 |
| MSH6 | MutS Homolog 6 |
| PMS2 | PMS1 Homolog 2 |
| MSI | microsatellite instability |
| CA | carbohydrate antigen |
| CT | computed tomography |
| DES | diethylstilbesterol |
References
- Lynch, H.T.; Snyder, C.L.; Shaw, T.G.; Heinen, C.D.; Hitchins, M.P. Milestones of Lynch syndrome: 1895–2015. Nat. Rev. Cancer 2015, 15, 181–194. [Google Scholar] [CrossRef] [PubMed]
- Baglietto, L.; Lindor, N.M.; Dowty, J.G.; White, D.M.; Wagner, A.; Gomez Garcia, E.B.; Vriends, A.H.; Cartwright, N.R.; Barnetson, R.A.; Farrington, S.M.; et al. Risks of Lynch syndrome cancers for MSH6 mutation carriers. J. Natl. Cancer Inst. 2010, 102, 193–201. [Google Scholar] [CrossRef] [PubMed]
- Senter, L.; Clendenning, M.; Sotamaa, K.; Hampel, H.; Green, J.; Potter, J.D.; Lindblom, A.; Lagerstedt, K.; Thibodeau, S.N.; Lindor, N.M.; et al. The clinical phenotype of Lynch syndrome due to germ-line PMS2 mutations. Gastroenterology 2008, 135, 419–428. [Google Scholar] [CrossRef] [PubMed]
- Bonadona, V.; Bonaiti, B.; Olschwang, S.; Grandjouan, S.; Huiart, L.; Longy, M.; Guimbaud, R.; Buecher, B.; Bignon, Y.J.; Caron, O.; et al. Cancer risks associated with germline mutations in MLH1, MSH2, and MSH6 genes in Lynch syndrome. JAMA 2011, 305, 2304–2310. [Google Scholar] [CrossRef] [PubMed]
- Dowty, J.G.; Win, A.K.; Buchanan, D.D.; Lindor, N.M.; Macrae, F.A.; Clendenning, M.; Antill, Y.C.; Thibodeau, S.N.; Casey, G.; Gallinger, S.; et al. Cancer risks for MLH1 and MSH2 mutation carriers. Hum. Mutat. 2013, 34, 490–497. [Google Scholar] [CrossRef] [PubMed]
- Mongiat-Artus, P.; Miquel, C.; Flejou, J.F.; Coulet, F.; Verine, J.; Buhard, O.; Soliman, H.; Teillac, P.; Praz, F. Spectrum of molecular alterations in colorectal, upper urinary tract, endocervical, and renal carcinomas arising in a patient with hereditary non-polyposis colorectal cancer. Virchows Arch. 2006, 449, 238–243. [Google Scholar] [CrossRef] [PubMed]
- Nair, N.; Curtin, J.P.; Mittal, K.; Hiotis, K.L. Cervical adenocarcinoma in a patient with Lynch syndrome, Muir-Torre variant. J. Clin. Oncol. 2012, 30, E5–E6. [Google Scholar] [CrossRef] [PubMed]
- Moat, M.; O’Donnell, R.L.; McCluggage, W.G.; Ralte, A.; Edmondson, R.J. Gastric-type adenocarcinoma of the cervix in a patient with Lynch syndrome: A case report. Gynecol. Oncol. Rep. 2014, 13, 41–43. [Google Scholar] [CrossRef] [PubMed]
- Herbst, A.L. Behavior of estrogen-associated female genital tract cancer and its relation to neoplasia following intrauterine exposure to diethylstilbestrol (DES). Gynecol. Oncol. 2000, 76, 147–156. [Google Scholar] [CrossRef] [PubMed]
- Kaminski, P.F.; Maier, R.C. Clear cell adenocarcinoma of the cervix unrelated to diethylstilbestrol exposure. Obstet. Gynecol. 1983, 62, 720–727. [Google Scholar] [PubMed]
- Ryan, S.; Jenkins, M.A.; Win, A.K. Risk of prostate cancer in Lynch syndrome: A systematic review and meta-analysis. Cancer Epidemiol. Biomark. Prev. 2014, 23, 437–449. [Google Scholar] [CrossRef] [PubMed]
- Win, A.K.; Lindor, N.; Jenkins, M. Risk of breast cancer in Lynch syndrome: A systematic review. Breast Cancer Res. 2013, 15, R27. [Google Scholar] [CrossRef] [PubMed]
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).

{kind=link}
{kind=link}
{kind=link}
{kind=link}



