
Integrative Analyses of Circulating Small RNAs and Kidney Graft Transcriptome in Transplant Glomerulopathy

 , , , , ,
, , , , ,
Abstract
:1. Introduction
2. Results
2.1. Clinical Characteristics of the Patients
2.2. Histopathological Features of TG Biopsies
2.3. Circulating Small RNA Profiles from Serum of Transplant Glomerulopathy and Normal Allograft Transplant Patients
2.4. Abundant 5′ tRNA Fragments in Serum
2.5. Differentially Expressed tRNA Fragments in TG Patients
2.6. Differentially Expressed miRNAs in TG Patients
2.7. Down Regulation of Circulating miRNAs Results in Upregulation of Targets Globally
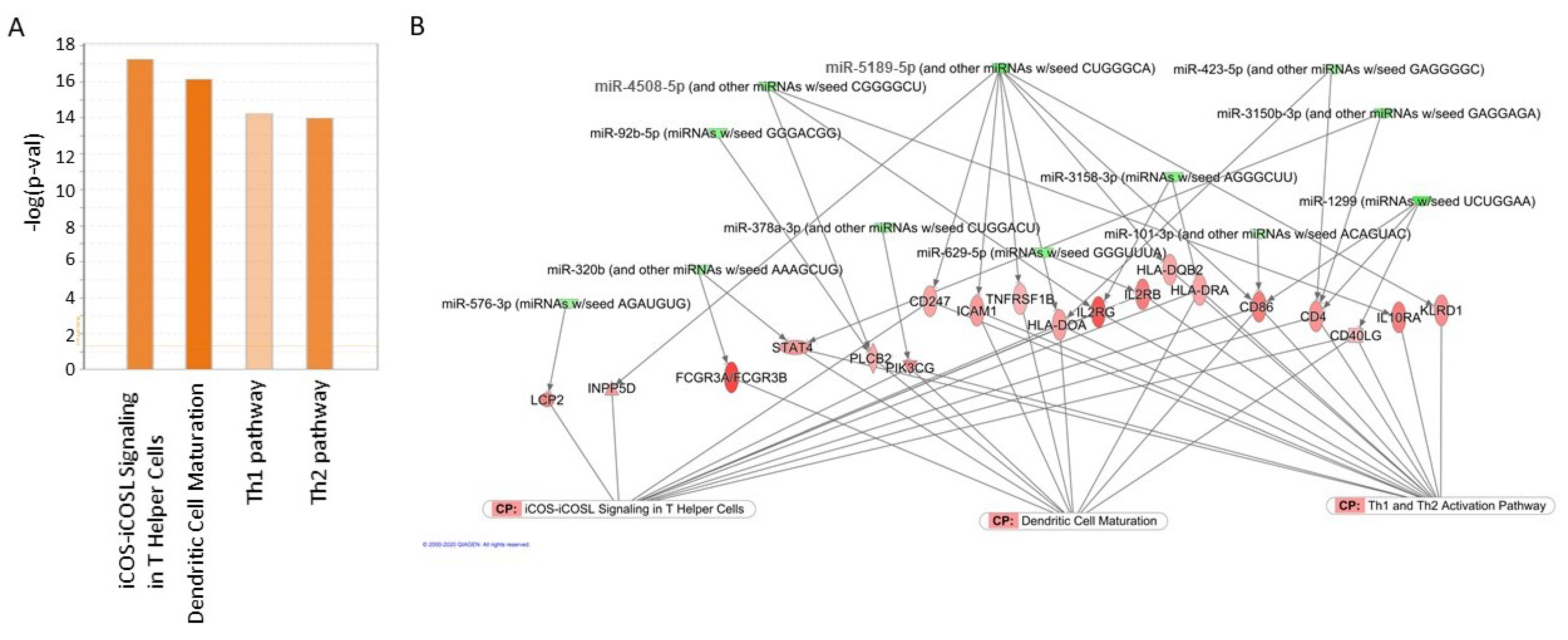
2.8. Circulating miRNAs Regulate Top Pathways Identified in Gene Expression Analysis
3. Discussion
4. Materials and Methods
4.1. Histopathology
4.2. RNA Purification from Serum and sRNA Library Preparation
4.3. sRNA Sequencing Data and Differential Expression Analysis
4.4. Differential Gene Expression Analysis Using Microarray Data
4.5. miRNA Target Prediction and Cumulative Distribution Plots
4.6. Integration of miRNA and Gene Expression Analysis
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Racusen, L.C.; Colvin, R.B.; Solez, K.; Mihatsch, M.J.; Halloran, P.F.; Campbell, P.M.; Cecka, M.J.; Cosyns, J.P.; Demetris, A.J.; Fishbein, M.C.; et al. Antibody-mediated rejection criteria—An addition to the Banff 97 classification of renal al-lograft rejection. Am. J. Transplant. 2003, 3, 708–714. [Google Scholar] [CrossRef] [PubMed]
- Mengel, M.; Sis, B.; Haas, M.; Colvin, R.B.; Halloran, P.F.; Racusen, L.C.; Solez, K.; Cendales, L.C.; Demetris, A.J.; Drachenberg, C.B.; et al. Banff 2011 Meeting Report: New Concepts in Antibody-Mediated Rejection. Arab. Archaeol. Epigr. 2012, 12, 563–570. [Google Scholar] [CrossRef] [PubMed]
- Akalin, E.; Dinavahi, R.; Dikman, S.; De Boccardo, G.; Friedlander, R.; Schroppel, B.; Sehgal, V.; Bromberg, J.S.; Heeger, P.; Murphy, B. Transplant Glomerulopathy May Occur in the Absence of Donor-Specific Antibody and C4d Staining. Clin. J. Am. Soc. Nephrol. 2007, 2, 1261–1267. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hayde, N.; Bao, Y.; Pullman, J.; Ye, B.; Calder, B.R.; Chung, M.; Schwartz, D.; Alansari, A.; De Boccardo, G.; Ling, M.; et al. The Clinical and Molecular Significance of C4d Staining Patterns in Renal Allografts. Transplantation 2013, 95, 580–588. [Google Scholar] [CrossRef]
- Lubetzky, M.; Hayde, N.; Broin, P.Ó.; Ajaimy, M.; Bao, Y.; Mohammed, O.; Schwartz, D.; Pullman, J.; Akalin, E. Molecular signatures and clinical outcomes of transplant glomerulopathy stratified by microvascular inflammation and donor-specific antibody. Clin. Transplant. 2019, 33, e13469. [Google Scholar] [CrossRef]
- Akalin, E.; Dikman, S.; Murphy, B.; Bromberg, J.S.; Hancock, W.W. Glomerular Infiltration by CXCR3+ ICOS+ Activated T Cells in Chronic Allograft Nephropathy with Transplant Glomerulopathy. Arab. Archaeol. Epigr. 2003, 3, 1116–1120. [Google Scholar] [CrossRef] [PubMed]
- Homs, S.; Mansour, H.; Desvaux, D.; Diet, C.; Hazan, M.; Büchler, M.; Lebranchu, Y.; Buob, D.; Badoual, C.; Matignon, M.; et al. Predominant Th1 and Cytotoxic Phenotype in Biopsies from Renal Transplant Recipients with Transplant Glomerulopathy. Arab. Archaeol. Epigr. 2009, 9, 1230–1236. [Google Scholar] [CrossRef]
- Elster, E.A.; Hawksworth, J.S.; Cheng, O.; Leeser, D.B.; Ring, M.; Tadaki, D.K.; Kleiner, D.E.; Eberhardt, J.S., 3rd; Brown, T.S.; Mannon, R.B. Probabilistic (Bayesian) modeling of gene expression in transplant glomerulopathy. J. Mol. Diagn. 2010, 12, 653–663. [Google Scholar] [CrossRef]
- De Serres, S.A.; Vadivel, N.; Mfarrej, B.; Grafals, M.; DeJoseph, M.; Dyer, C.; Magee, C.N.; Chandraker, A.; Gallon, L.G.; Najafian, N. Monocyte-Secreted Inflammatory Cytokines Are Associated with Transplant Glomerulopathy in Renal Allograft Recipients. Transplantation 2011, 91, 552–559. [Google Scholar] [CrossRef]
- Sun, Q.; Zhang, M.; Xie, K.; Li, X.; Zeng, C.; Zhou, M.; Liu, Z. Endothelial injury in transplant glomerulopathy is cor-related with transcription factor T-bet expression. Kidney Int. 2012, 82, 321–329. [Google Scholar] [CrossRef] [Green Version]
- Batal, I.; Girnita, A.; Zeevi, A.; Saab, B.A.; Stockhausen, S.; Shapiro, R.; Basu, A.; Tan, H.; Morgan, C.; Randhawa, P. Clinical significance of the distribution of C4d deposits in different anatomic compartments of the allograft kidney. Mod. Pathol. 2008, 21, 1490–1498. [Google Scholar] [CrossRef] [Green Version]
- Gibson, I.W.; Gwinner, W.; Bröcker, V.; Sis, B.; Riopel, J.; Roberts, I.; Scheffner, I.; Jhangri, G.S.; Mengel, M. Peritubular Capillaritis in Renal Allografts: Prevalence, Scoring System, Reproducibility and Clinicopathological Correlates. Arab. Archaeol. Epigr. 2008, 8, 819–825. [Google Scholar] [CrossRef]
- Koenig, A.; Chen, C.-C.; Marçais, A.; Barba, T.; Mathias, V.; Sicard, A.; Rabeyrin, M.; Racapé, M.; Duong-Van-Huyen, J.-P.; Bruneval, P.; et al. Missing self triggers NK cell-mediated chronic vascular rejection of solid organ transplants. Nat. Commun. 2019, 10, 1–17. [Google Scholar] [CrossRef]
- Baker, R.J.; Hernandez-Fuentes, M.P.; Brookes, P.A.; Chaudhry, A.N.; Cook, H.T.; Lechler, R.I. Loss of direct and maintenance of indirect alloresponses in renal allograft recipients: Implications for the pathogenesis of chronic allograft nephropathy. J. Immunol. 2001, 167, 7199–7206. [Google Scholar] [CrossRef] [Green Version]
- Lee, R.S.; Yamada, K.; Houser, S.L.; Womer, K.L.; Maloney, M.E.; Rose, H.S.; Sayegh, M.H.; Madsen, J.C. Indirect recognition of allopeptides promotes the development of cardiac allograft vasculopathy. Proc. Natl. Acad. Sci. USA 2001, 98, 3276–3281. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, Z.; I Colovai, A.; Tugulea, S.; Reed, E.F.; E Fisher, P.; Mancini, D.; A Rose, E.; Cortesini, R.; E Michler, R.; Suciu-Foca, N. Indirect recognition of donor HLA-DR peptides in organ allograft rejection. J. Clin. Investig. 1996, 98, 1150–1157. [Google Scholar] [CrossRef] [Green Version]
- Vella, J.P.; Spadafora-Ferreira, M.; Murphy, B.; Alexander, S.I.; Harmon, W.; Carpenter, C.B.; Sayegh, M.H. Indirect Allorecognition of Major Histocompatibility Complex Allopeptides in Human Renal Transplant Recipients with Chronic Graft Dysfunction1. Transplantation 1997, 64, 795–800. [Google Scholar] [CrossRef]
- Kumar, P.; Kuscu, C.; Dutta, A. Biogenesis and Function of Transfer RNA-Related Fragments (tRFs). Trends Biochem. Sci. 2016, 41, 679–689. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Saikia, M.; Hatzoglou, M. The Many Virtues of tRNA-derived Stress-induced RNAs (tiRNAs): Discovering Novel Mechanisms of Stress Response and Effect on Human Health. J. Biol. Chem. 2015, 290, 29761–29768. [Google Scholar] [CrossRef] [Green Version]
- Kumar, P.; Anaya, J.; Mudunuri, S.B.; Dutta, A. Meta-analysis of tRNA derived RNA fragments reveals that they are evolutionarily conserved and associate with AGO proteins to recognize specific RNA targets. BMC Biol. 2014, 12, 78. [Google Scholar] [CrossRef] [PubMed]
- Kuscu, C.; Kumar, P.; Kiran, M.; Su, Z.; Malik, A.; Dutta, A. tRNA fragments (tRFs) guide Ago to regulate gene expression post-transcriptionally in a Dicer-independent manner. RNA 2018, 24, 1093–1105. [Google Scholar] [CrossRef] [Green Version]
- Godoy, P.M.; Bhakta, N.R.; Barczak, A.J.; Cakmak, H.; Fisher, S.; MacKenzie, T.C.; Patel, T.; Price, R.W.; Smith, J.F.; Woodruff, P.G.; et al. Large Differences in Small RNA Composition Between Human Biofluids. Cell Rep. 2018, 25, 1346–1358. [Google Scholar] [CrossRef] [Green Version]
- Murillo, O.D.; Thistlethwaite, W.; Rozowsky, J.; Subramanian, S.L.; Lucero, R.; Shah, N.; Jackson, A.R.; Srinivasan, S.; Chung, A.; Laurent, C.D.; et al. exRNA Atlas Analysis Reveals Distinct Extracellular RNA Cargo Types and Their Carriers Present across Human Biofluids. Cell 2019, 177, 463–477.e15. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yu, J.; Yu, C.; Feng, B.; Zhan, X.; Luo, N.; Yu, X.; Zhou, Q. Intrarenal microRNA signature related to the fibrosis process in chronic kidney disease: Identification and functional validation of key miRNAs. BMC Nephrol. 2019, 20, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Hajarnis, S.; Yheskel, M.; Williams, D.; Brefort, T.; Glaudemans, B.; Debaix, H.; Baum, M.; Devuyst, O.; Patel, V. Suppression of microRNA Activity in Kidney Collecting Ducts Induces Partial Loss of Epithelial Phenotype and Renal Fi-brosis. J. Am. Soc. Nephrol. 2018, 29, 518–531. [Google Scholar] [CrossRef] [PubMed]
- Liu, Z.; Wang, Y.; Shu, S.; Cai, J.; Tang, C.; Dong, Z. Non-coding RNAs in kidney injury and repair. Am. J. Physiol. Physiol. 2019, 317, C177–C188. [Google Scholar] [CrossRef]
- Chiou, N.-T.; Kageyama, R.; Ansel, K.M. Selective export into extracellular vesicles and function of tRNA fragments during T cell activation. Cell Rep. 2018, 25, 3356–3370.e4. [Google Scholar] [CrossRef] [Green Version]
- Rozowsky, J.; Kitchen, R.R.; Park, J.J.; Galeev, T.R.; Diao, J.; Warrell, J.; Thistlethwaite, W.; Subramanian, S.L.; Milosavljevic, A.; Gerstein, M. exceRpt: A Comprehensive Analytic Platform for Extracellular RNA Profiling. Cell Syst. 2019, 8, 352–357.e3. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sobala, A.; Hutvagner, G. Small RNAs derived from the 5′ end of tRNA can inhibit protein translation in human cells. RNA Biol. 2013, 10, 553–563. [Google Scholar] [CrossRef] [Green Version]
- Jingushi, K.; Ueda, Y.; Kitae, K.; Hase, H.; Egawa, H.; Ohshio, I.; Kawakami, R.; Kashiwagi, Y.; Tsukada, Y.; Ko-bayashi, T.; et al. miR-629 Targets TRIM33 to Promote TGFbeta/Smad Signaling and Metastatic Phenotypes in ccRCC. Mol. Cancer Res. 2015, 13, 565–574. [Google Scholar] [CrossRef] [Green Version]
- Li, Y.; Chen, D.; Su, Z.; Li, Y.; Liu, J.; Jin, L.; Shi, M.; Jiang, Z.; Qi, Z.; Gui, Y.; et al. MicroRNA-106b functions as an oncogene in renal cell carcinoma by affecting cell proliferation, migration and apoptosis. Mol. Med. Rep. 2015, 13, 1420–1426. [Google Scholar] [CrossRef] [Green Version]
- Wang, B.; Yao, K.; Wise, A.F.; Lau, R.; Shen, H.-H.; Tesch, G.H.; Ricardo, S.D. miR-378 reduces mesangial hypertrophy and kidney tubular fibrosis via MAPK signalling. Clin. Sci. 2017, 131, 411–423. [Google Scholar] [CrossRef] [PubMed]
- Wang, W.; Gao, J.; Wang, F. MiR-663a/MiR-423-5p are involved in the pathogenesis of lupus nephritis via modulating the activation of NF-kappaB by targeting TNIP2. Am. J. Transl. Res. 2017, 9, 3796–3803. [Google Scholar]
- Lewis, B.P.; Burge, C.B.; Bartel, D.P. Conserved Seed Pairing, Often Flanked by Adenosines, Indicates that Thousands of Human Genes are MicroRNA Targets. Cell 2005, 120, 15–20. [Google Scholar] [CrossRef] [Green Version]
- Grimson, A.; Farh, K.K.-H.; Johnston, W.K.; Garrett-Engele, P.; Lim, L.P.; Bartel, D.P. MicroRNA Targeting Specificity in Mammals: Determinants beyond Seed Pairing. Mol. Cell 2007, 27, 91–105. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brandenburger, T.; Lorenzen, J.M. Diagnostic and Therapeutic Potential of microRNAs in Acute Kidney Injury. Front. Pharmacol. 2020, 11, 657. [Google Scholar] [CrossRef] [PubMed]
- Yeri, A.; Courtright, A.; Reiman, R.; Carlson, E.; Beecroft, T.; Janss, A.; Siniard, A.; Richholt, R.; Balak, C.; Rozowsky, J.; et al. Total Extracellular Small RNA Profiles from Plasma, Saliva, and Urine of Healthy Subjects. Sci. Rep. 2017, 7, srep44061. [Google Scholar] [CrossRef] [Green Version]
- Torres, A.G.; Martí, E. Toward an Understanding of Extracellular tRNA Biology. Front. Mol. Biosci. 2021, 8, 233. [Google Scholar] [CrossRef]
- Zheng, G.; Qin, Y.; Clark, W.C.; Dai, Q.; Yi, C.; He, C.; Lambowitz, A.M.; Pan, T. Efficient and quantitative high-throughput tRNA sequencing. Nat. Methods 2015, 12, 835–837. [Google Scholar] [CrossRef]
- Lyons, S.M.; Gudanis, D.; Coyne, S.M.; Gdaniec, Z.; Ivanov, P. Identification of functional tetramolecular RNA G-quadruplexes derived from transfer RNAs. Nat. Commun. 2017, 8, 1127. [Google Scholar] [CrossRef] [Green Version]
- Tosar, J.P.; Segovia, M.; Castellano, M.; Gámbaro, F.; Akiyama, Y.; Fagúndez, P.; Olivera, Á.; Costa, B.; Possi, T.; Hill, M.; et al. Fragmentation of extracellular ribosomes and tRNAs shapes the extracellular RNAome. Nucleic Acids Res. 2020, 48, 12874–12888. [Google Scholar] [CrossRef] [PubMed]
- Thompson, D.M.; Parker, R. Stressing Out over tRNA Cleavage. Cell 2009, 138, 215–219. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhou, J.; Liu, S.; Chen, Y.; Fu, Y.; Silver, A.J.; Hill, M.S.; Lee, I.; Lee, Y.S.; Bao, X. Identification of two novel func-tional tRNA-derived fragments induced in response to respiratory syncytial virus infection. J. Gen. Virol. 2017, 98, 1600–1610. [Google Scholar] [CrossRef]
- Pawar, K.; Shigematsu, M.; Sharbati, S.; Kirino, Y. Infection-induced 5′-half molecules of tRNAHisGUG activate Toll-like receptor 7. PLoS Biol. 2020, 18, e3000982. [Google Scholar] [CrossRef]
- Zhang, X.; He, X.; Liu, C.; Liu, J.; Hu, Q.; Pan, T.; Duan, X.; Liu, B.; Zhang, Y.; Chen, J.; et al. IL-4 Inhibits the Biogenesis of an Epigenetically Suppressive PIWI-Interacting RNA To Upregulate CD1a Molecules on Monocytes/Dendritic Cells. J. Immunol. 2016, 196, 1591–1603. [Google Scholar] [CrossRef] [Green Version]
- Xu, H.; Chen, W.; Zheng, F.; Tang, D.; Dai, W.; Huang, S.; Zhang, C.; Zeng, J.; Wang, G.; Dai, Y. The potential role of tRNAs and small RNAs derived from tRNAs in the occurrence and development of systemic lupus erythematosus. Biochem. Biophys. Res. Commun. 2020, 527, 561–567. [Google Scholar] [CrossRef]
- Winek, K.; Lobentanzer, S.; Nadorp, B.; Dubnov, S.; Dames, C.; Jagdmann, S.; Moshitzky, G.; Hotter, B.; Meisel, C.; Greenberg, D.S.; et al. Transfer RNA fragments replace mi-croRNA regulators of the cholinergic poststroke immune blockade. Proc. Natl. Acad. Sci. USA 2020, 117, 32606–32616. [Google Scholar] [CrossRef] [PubMed]
- Khurana, R.; Ranches, G.; Schafferer, S.; Lukasser, M.; Rudnicki, M.; Mayer, G.; Hüttenhofer, A. Identification of urinary exosomal noncoding RNAs as novel biomarkers in chronic kidney disease. RNA 2017, 23, 142–152. [Google Scholar] [CrossRef] [Green Version]
- Mami, I.; Pallet, N. tRNA fragmentation and protein translation dynamics in the course of kidney injury. RNA Biol. 2018, 15, 1147–1156. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Turchinovich, A.; Samatov, T.R.; Tonevitsky, A.G.; Burwinkel, B. Circulating miRNAs: Cell–cell communication function? Front. Genet. 2013, 4, 119. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- O’Brien, J.; Hayder, H.; Zayed, Y.; Peng, C. Overview of MicroRNA Biogenesis, Mechanisms of Actions, and Circulation. Front. Endocrinol. 2018, 9, 402. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, C.; Shi, J.; Zhao, Y. MiR-320 promotes B cell proliferation and the production of aberrant glycosylated IgA1 in IgA nephropathy. J. Cell. Biochem. 2018, 119, 4607–4614. [Google Scholar] [CrossRef]
- Aguado-Fraile, E.; Ramos, E.; Conde, E.; Rodríguez, M.; Martín-Gómez, L.; Lietor, A.; Candela, Á.; Ponte, B.; Liaño, F.; García-Bermejo, M.L. A Pilot Study Identifying a Set of microRNAs As Precise Diagnostic Biomarkers of Acute Kidney Injury. PLoS ONE 2015, 10, e0127175. [Google Scholar] [CrossRef] [PubMed]
- Mittelbrunn, M.; Gutierrez-Vazquez, C.; Villarroya-Beltri, C.; Gonzalez, S.; Sanchez-Cabo, F.; Gonzalez, M.A.; Ber-nad, A.; Sanchez-Madrid, F. Unidirectional transfer of microRNA-loaded exosomes from T cells to antigen-presenting cells. Nat. Commun. 2011, 2, 282. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Spinosa, M.; Lu, G.; Su, G.; Bontha, S.V.; Gehrau, R.; Salmon, M.D.; Smith, J.R.; Weiss, M.L.; Mas, V.R.; Upchurch, G.R., Jr.; et al. Human mesenchymal stromal cell-derived extracellular vesicles attenuate aortic aneurysm formation and macrophage activation via microRNA-147. FASEB J. 2018, 32, 6038–6050. [Google Scholar] [CrossRef] [PubMed]
- Racusen, L.C.; Solez, K.; Colvin, R.B.; Bonsib, S.M.; Castro, M.C.; Cavallo, T.; Croker, B.P.; Demetris, A.J.; Drachenberg, C.B.; Fogo, A.B.; et al. The Banff 97 working classification of renal allograft pathology. Kidney Int. 1999, 55, 713–723. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Haas, M.; Sis, B.; Racusen, L.C.; Solez, K.; Glotz, D.; Colvin, R.B.; Castro, M.C.; David, D.S.; David-Neto, E.; Bagnasco, S.M.; et al. Banff 2013 meeting report: Inclusion of c4d-negative antibody-mediated rejection and antibody-associated arterial lesions. Am. J. Transplant. 2014, 14, 272–283. [Google Scholar] [CrossRef]
- Gebert, D.; Hewel, C.; Rosenkranz, D. unitas: The universal tool for annotation of small RNAs. BMC Genom. 2017, 18, 1–14. [Google Scholar] [CrossRef]
- Jiang, H.; Wong, W.H. SeqMap: Mapping massive amount of oligonucleotides to the genome. Bioinformatics 2008, 24, 2395–2396. [Google Scholar] [CrossRef] [Green Version]
- Kozomara, A.; Griffiths-Jones, S. miRBase: Annotating high confidence microRNAs using deep sequencing data. Nucleic Acids Res. 2014, 42, D68–D73. [Google Scholar] [CrossRef] [Green Version]
- Chan, P.P.; Lowe, T.M. GtRNAdb: A database of transfer RNA genes detected in genomic sequence. Nucleic Acids Res. 2008, 37, D93–D97. [Google Scholar] [CrossRef]
- Yates, A.; Akanni, W.; Amode, M.R.; Barrell, D.; Billis, K.; Carvalho-Silva, D.; Cummins, C.; Clapham, P.; Fitzgerald, S.; Gil, L.; et al. Ensembl 2016. Nucleic Acids Res. 2016, 44, D710–D716. [Google Scholar] [CrossRef] [PubMed]
- Quast, C.; Pruesse, E.; Yilmaz, P.; Gerken, J.; Schweer, T.; Yarza, P.; Peplies, J.; Glockner, F.O. The SILVA ribosomal RNA gene database project: Improved data processing and web-based tools. Nucleic Acids Res. 2013, 41, D590–D596. [Google Scholar] [CrossRef]
- Archer, K.J.; Mas, V.R.; Oʼbrien, T.R.; Pfeiffer, R.; Lum, N.L.; Fisher, R.A. Quality Assessment of Microarray Data in a Multicenter Study. Diagn. Mol. Pathol. 2009, 18, 34–43. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Irizarry, R.A.; Hobbs, B.; Collin, F.; Beazer-Barclay, Y.D.; Antonellis, K.J.; Scherf, U.; Speed, T.P. Exploration, normalization, and summaries of high density oligonucleotide array probe level data. Biostatistics 2003, 4, 249–264. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Agarwal, V.; Bell, G.W.; Nam, J.-W.; Bartel, D.P. Predicting effective microRNA target sites in mammalian mRNAs. eLife 2015, 4, e05005. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Transplant Glomerulopathy (n = 34) | Control Group (n = 19) | |
|---|---|---|
| Median age | 51 (32, 79) | 56 (27, 71) |
| Sex, male | 56% | 79% |
| Race, Caucasian | 56% | 39% |
| Etiology of kidney disease | ||
| Diabetes Mellitus | 21% | 37% |
| Hypertension | 29% | 32% |
| Glomerular disease | 32% | 16% |
| Median time on dialysis, yr | 3 (0.7, 13) | 3 (1, 8) |
| Type of transplant, deceased | 68% | 89% |
| Median donor age | 37 (5, 63) | 36 (6, 72) |
| Donor sex, male | 47% | 63% |
| Donor race, Caucasian | 44% | 53% |
| Median Class I PRA | 10% (0%, 86%) | 0% (0%, 97%) |
| Median Class II PRA | 37% (0%, 99%) | 0% (0%, 100%) |
| Both Class I and II PRA 0% | 24% | 69% |
| Median HLA mismatch | 3 (0, 6) | 3 (0, 6) |
| Donor-specific antibody | 59% | 11% |
| Induction, anti-thymocyte | 53% | 63% |
| Median cold ischemia time | 19 (9, 43) h | 21 (9, 45) h |
| Median time to biopsy | ||
| after transplantation | 87 (3, 276) mos | 4.5 (1, 120) mos |
| Previous acute rejection | 24% | 0% |
| Median serum creatinine | 2.0 (1.0, 5.1) mg/dL | 1.7 (1.1, 3.8) mg/dL |
| Spot urine protein/creatinine | ||
| more than 0.5 g/g | 83% | 16% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kuscu, C.; Kiran, M.; Mohammed, A.; Kuscu, C.; Satpathy, S.; Wolen, A.; Bardhi, E.; Bajwa, A.; Eason, J.D.; Maluf, D.; et al. Integrative Analyses of Circulating Small RNAs and Kidney Graft Transcriptome in Transplant Glomerulopathy. Int. J. Mol. Sci. 2021, 22, 6218. https://doi.org/10.3390/ijms22126218
Kuscu C, Kiran M, Mohammed A, Kuscu C, Satpathy S, Wolen A, Bardhi E, Bajwa A, Eason JD, Maluf D, et al. Integrative Analyses of Circulating Small RNAs and Kidney Graft Transcriptome in Transplant Glomerulopathy. International Journal of Molecular Sciences. 2021; 22(12):6218. https://doi.org/10.3390/ijms22126218
Chicago/Turabian StyleKuscu, Canan, Manjari Kiran, Akram Mohammed, Cem Kuscu, Sarthak Satpathy, Aaron Wolen, Elissa Bardhi, Amandeep Bajwa, James D. Eason, Daniel Maluf, and et al. 2021. "Integrative Analyses of Circulating Small RNAs and Kidney Graft Transcriptome in Transplant Glomerulopathy" International Journal of Molecular Sciences 22, no. 12: 6218. https://doi.org/10.3390/ijms22126218