1. Introduction
In 2011, Spain’s immigrant population declined slightly for the first time since the beginning of the migratory surge that characterized the first decade of the 21st century [
1]. Nevertheless, Spain remains one of the European countries with the highest volume of foreigners, at 11.7% of the population in 2013 [
2]. The sociodemographic change that immigration has brought about in the country is reflected in the significant number of recent publications that analyze different aspects of the immigrant population, including healthcare access and health service use [
3,
4,
5,
6,
7,
8,
9]. Many of these studies compare the use of services between the immigrant and autochthonous populations [
3,
4,
5,
6,
7,
8,
9]. Reviews of national and European literature [
10,
11,
12] show that, in general, given the same health needs, use of primary care services is similar among the immigrant population from low-income countries and the autochthonous population. However, this immigrant population has lower use of specialist care and higher use of emergency services. Explaining these differences requires a specific analysis of the determinants of health services use, which is a topic that has been scarcely addressed in national [
8,
13] and European [
14] literature. At the international level, no studies were found that show the specific determinants for each group, although one study shows that differences in health service use between the two groups is due to the relatively worse social and economic situation of immigrants [
14]. Only one study in Spain compares the determinants of health service use between the immigrant and autochthonous populations and it concludes that there are similar socioeconomic determinants related to health service use in both populations [
8]. The study shows that women make more use of specialist and hospitalization services, that students make less use of primary care and specialist services than do employees, and that those with poor health make more use of health services at all levels of care. The study also shows that holding a private health insurance policy is associated with lower use of primary care and greater use of specialist care [
8]. In contrast, other factors, such as education level and income, are associated with the use of health services in the autochthonous population but not in the immigrant population.
Prolonged economic crises, such as that experienced in Spain since 2008, bring about an increase in the number of citizens experiencing social and economic vulnerability [
15]; these individuals are more susceptible to the effects of the crisis, which could include a general worsening of health, a decrease in access to health services [
16] or an increase in barriers to access to healthcare [
17]. The immigrant population, along with elderly and those with few economic resources (due to unemployment or low incomes) are among the most fragile social groups and can suffer more negative consequences as a result of the economic crisis. At the international level, the study by Lusardi
et al. [
18] shows a decrease in health service use as a consequence of the crisis in five countries, particularly for households in economic distress. However, the results differ according to the health system of each country; those countries with universal health systems and lower copayments experience a smaller decline in health service use. Another study carried out in eight European countries affected by the crisis, including Spain, shows a general increase in unmet health needs (measured as the percentage of people that needed medical consultation or treatment but did not receive it) during the crisis. This increase was related to unmet need due to wait times, cost and transportation—although behavior is different for each country [
19]. Until recently, studies carried out in Spain on the effects of the economic crisis have focused on its impact on population health [
20,
21]. Only one study analyzes the effects of the crisis on the general population’s access to health services, showing a decrease in health service use compared to 2006, especially among unskilled workers [
22].
The Spanish national health system, which was characterized by universal access until 2012 in addition to specific policies designed to improve access to care for the immigrant population [
23,
24], may have cushioned the adverse consequences of the crisis during its first years. Analysis of the most recent Spanish National Health Survey [
25], carried out between 2011 and 2012, four years after the beginning of the economic crisis, permits a first approach to the impact of the crisis on health access and health service use [
26].
One of the most frequently used theoretical frameworks to analyze access to health services is that of Aday and Andersen [
27]. This framework distinguishes between actual access or use of services, and potential access or analysis of determinants, differentiating between individual factors (predisposing, enabling and need) and health service factors. Another approach that is increasingly used [
28,
29] in the analysis of access is the measurement of unmet health needs, that is, the persistence of need due to lack of adequate care [
28]. Analyzing unmet need permits identifying barriers to access throughout the continuum of care, given the same health need. These two approaches oriented this study. The objective is to analyze the changes in access to health care and the determinants of access among the immigrant and autochthonous populations in Spain between 2006 and 2012.
4. Discussion and Conclusions
This work represents a first approach to the study of changes in access to healthcare of the autochthonous and immigrant populations in Spain between 2006 and 2012. The two time periods existed within different socio-economic contexts: the first was a time of economic bonanza and the second was during the first years of a severe and sustained financial crisis. The results show that unmet healthcare need decreased in both groups in 2012 compared to 2006. Health service use remained similar, although there were some notable changes, such as the decrease in general practitioner visits for autochthons, the slight decrease in the use of emergency services by both groups, and a narrowed gap in specialist visits between both populations. The analysis of the determinants of access to healthcare shows that the factors associated with use of services in 2006 generally remained the same in 2012.
The decrease in unmet healthcare need, both in the autochthonous and immigrant population, could be associated with the increase in perception of good health during the same time period. These results agree with other studies [
19,
22], but do not agree with Eurostat data that points to an increase in unmet health need in Spain, particularly for the lowest income quintiles (2008–2012 period) [
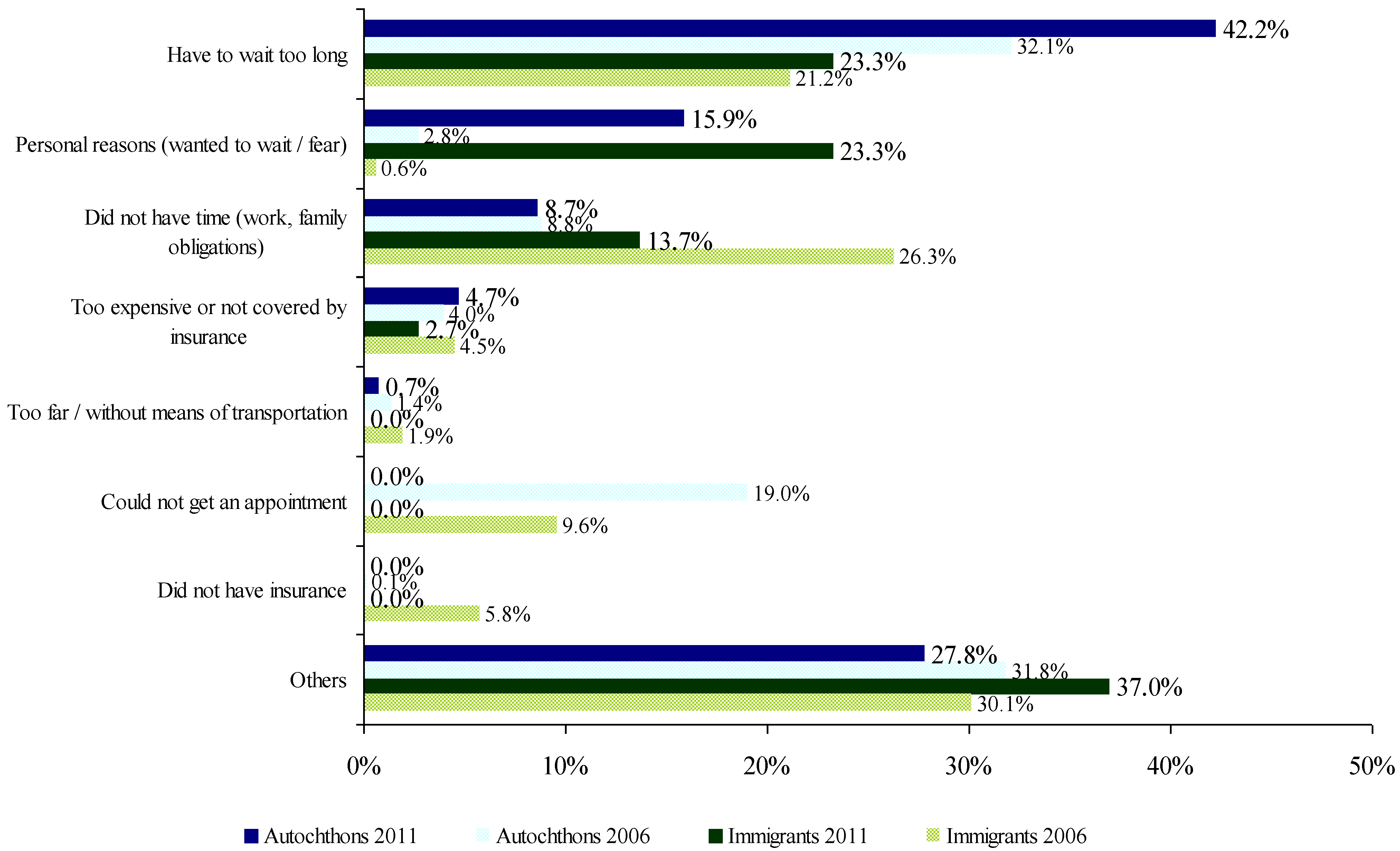
38]; this could be related to a different formulation of the question. The analysis of the reasons for unmet healthcare need show the presence of access barriers to care and changes during the time period, although these results should be interpreted with caution due to the difficulties in comparing the two surveys. They were explored through a close-ended question with contain different response options and because the category “
other reasons” cannot be further analyzed, because there was no possibility to specify a different answer from the given list. On one hand, the increase in the lack of access to care due to wait times agrees with evidence regarding the increase in waiting times within the current healthcare context [
22]. On the other hand, the marked decrease in the reason “
lack of time to attend health services due to work” in the immigrant population could be related to the increase in unemployment. This was the primary reason for unmet need in the immigrant population in 2006 and was probably associated with the fear of losing a job [
19,
39] due to precarious working situations, also described in other studies [
40].
The decrease in visits to a general practitioner in the autochthonous population, also described in another article [
22], which reached a similar level to that of the immigrant population in 2012, could be due to the improvement in self-perceived health or a decrease in administrative visits. The slight decrease in the use of emergency services could be related to greater knowledge of the health system due to longer time of residence for the immigrant population [
26]. For both immigrants and autochthons, it could also be related to the decrease in work related accidents possibly due to the increase in unemployment. Moreover, in 2012, unemployed immigrants made less use of emergency services than immigrant workers, a fact not observed in 2006 nor in existing literature [
8]. This could be related to having the time necessary to visit a general practitioner. No differences were found in either population in terms of the use of emergency services in the two surveys, in contrast to the results of other studies [
3,
4,
41]. This discrepancy could be due to the fact that the study population was under age 60, and in contrast, the other studies included the entire adult population. This would decrease the prevalence of emergency service use in autochthons such that it would seem to be less that than of the immigrant population.
In terms of specialist care, the significant difference between autochthons and immigrants in 2006, also described in other studies [
3,
4,
41], did not appear in 2012. The difference could be due to immigrants’ less favorable social and economic situations [
14] rather than their immigration status. Therefore, our results suggest that the National Health System that existed in Spain until 2012 tended towards diminishing inequalities in health service use among both populations, due to the universal access to health services in addition to specific policies developed to improve the health and access to care of the immigrant population [
9,
23]. However, it is important to note that equity in access to care does not guarantee equal access to high quality care. Inequalities related to access to quality care might still exist [
9,
23]. This is a subject that should be further studied and addressed by health policy.
The analysis of the determinants of health service use indicate that women make more use of both primary and specialist care services, which coincides with existing studies [
8,
13]. This is probably due to use related to maternity and gynecology services. The greater use of hospitalization [
8] and emergency [
13] services of immigrant women compared to autochthonous women that is described in other studies did not appear in this study, possibly because childbirth was excluded.
The most relevant difference found between both populations in this study was the pattern of inequity in the use of primary and specialist care, due to social class and the holding of a private health insurance policy on the part of the autochthonous population. Furthermore, this appears to have increased in 2012. Thus, the wealthier social classes make less use of primary care and greater use of specialist care services, corroborating the results of the only study that analyzes determinants separately [
8]. It also agrees with those studies that analyze the determinants in the general population [
42] including other socioeconomic indicators such as education level [
4,
41] or holding a private health insurance policy [
8,
43]. This inequality is less perceptible for the immigrant population, probably due to the lower proportion of immigrants in higher social classes, making it necessary to identify an indicator that better highlights the socioeconomic differences in this group.
Among the particularities of the determinants for the immigrant population, having a chronic disease was significant in determining visits to a general practitioner. This could be related to the length of residence in the country. The relatively good health immigrants compared to autochthonous population is lost over time as a consequence of adverse socioeconomic conditions; that is to say, immigrant health status declines and converges with the equivalent socioeconomic group in the autochthonous population [
44].
One aspect worth noting concerning the immigrant population’s access to care is the fact that the SNHS does not permit the analysis of relevant factors that influence access to the National Health System such as administrative status, only analyzed in qualitative studies or in quantitative studies based on surveys specifically conducted with immigrants [
9,
45]. Administrative status has probably become an important barrier to access to care [
46] due to the Royal Decree RD16/2012, which in addition to linking the right to health care to one’s affiliation to the Social Security, restricts the health rights of irregular immigrants to emergency and maternal healthcare and care for those under age 18 [
47]. Given that the SNHS 2011/12 data collection took place before the decree, and that health budget reductions and other austerity policies in public spending were introduced after 2012 [
48], further studies will be needed to evaluate their impact on access to care.
The principal limitation of this study is the lower participation of the immigrant population compared to the autochthonous population in the SNHS 2011/12. Despite the fact that the use of weighting factors gives this population as whole a weight similar to its assigned weight via the Municipal Register of Inhabitants [
49], it is important to bear in mind that representation is different by country of origin. In addition, with the grouping of immigrants into a single population, there is a loss of heterogeneity. Some studies that disaggregate this population by continent of origin show differences in health service use [
3,
4,
5,
7,
50]. As the aim of this study was to carry out a detailed analysis of the determinants of health service use, the sample size did not permit disaggregation at this level.
In conclusion, given existing data concerning access to care and health service use, access to health services did not get worse, rather we observed a decrease in unmet healthcare need and similar health service use among both groups, which could be attributed to a health system that, until 2012, maintained universal access, providing a cushion for the possible adverse effects of the crisis.


{kind=link}
