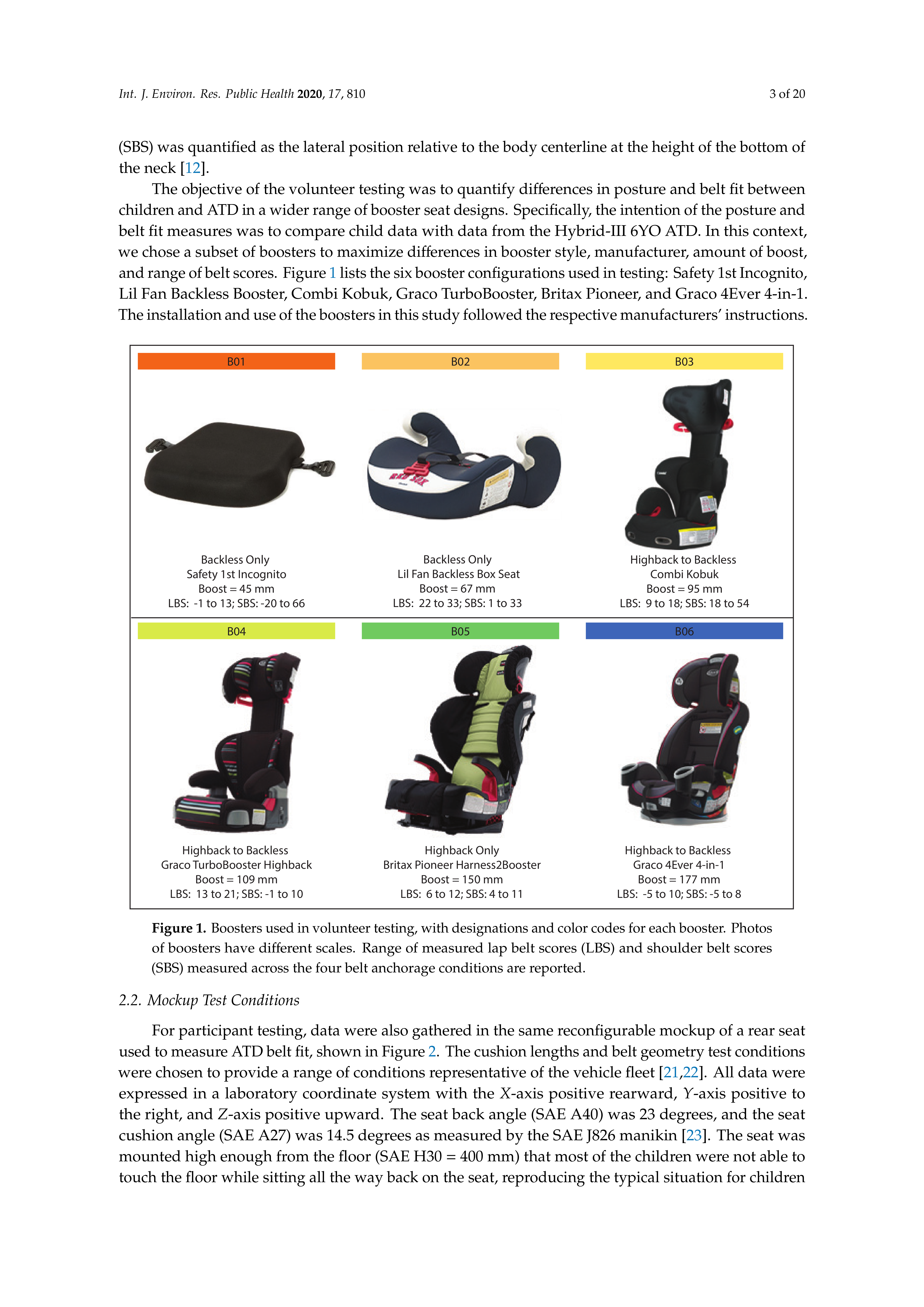
1. Introduction
Belt positioning boosters are recommended for use by children who have outgrown a forward-facing harnessed child restraint system (CRS), but are too small to achieve good belt fit using a vehicle lap-shoulder belt. The latest national estimates of booster use in the United States indicate that 45% of children aged four to seven use boosters [
1]. A prior study on belt fit showed that most children under age 11 would benefit from using a booster to achieve a good belt fit [
2]. Field data indicated that children aged 4–10 using boosters were 30–45% less likely to sustain injury in a crash compared to children using seat belts alone [
3,
4,
5].
Several studies of child posture and belt fit have identified several effectual ways boosters reduce injury risk [
6,
7,
8,
9,
10,
11,
12,
13,
14,
15]. First, since standard vehicle safety features (including the seat belt system, airbags, and interior padding) are nominally designed for adults, most booster-age children cannot reap the benefits offered by the safety features. By repositioning the child’s body upward, the booster allows a child occupant to achieve a skeletal position similar to that of an adult. Historically, products have achieved this by boosting the child’s seated position upward by at least 75–100 mm. The vertical shift re-positions the child so that the lap belt sits at the top of the thigh close to the pelvic bone. Meanwhile, the shoulder belt crosses the clavicle, the center of the sternum, and the opposite hip near the greater trochanter of the femur. The resulting seat belt fit creates an advantageous side view lap belt angle that prevents the lap belt from shifting upward during a crash. Second, boosters may have lap and shoulder belt guides to help establish and maintain good belt fit for the entire duration of travel. Third, a booster that raises the child effectively shortens the cushion length, allowing them to sit more upright and to maintain a comfortable bent leg posture throughout a trip. This modified posture also contributes to better belt fit.
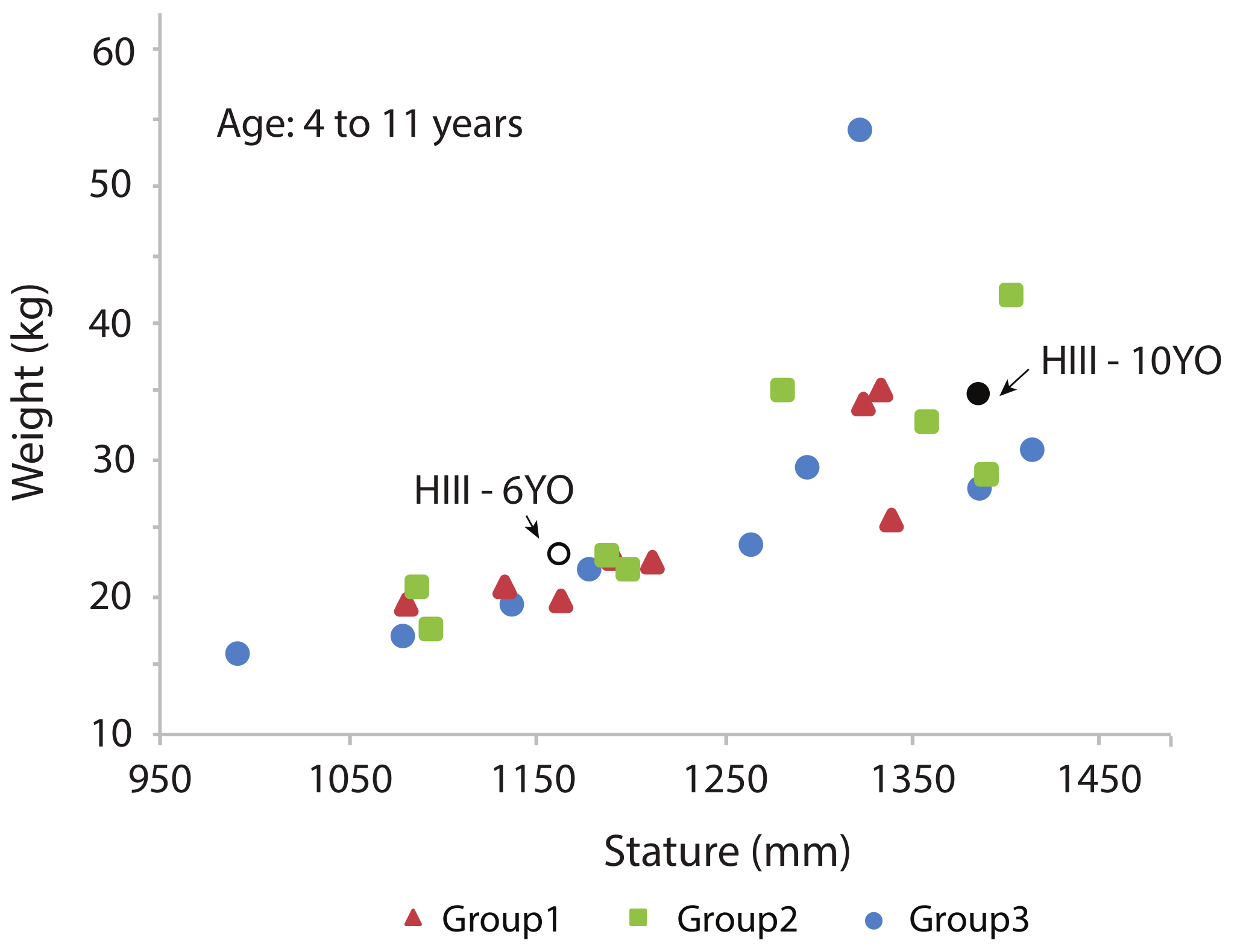
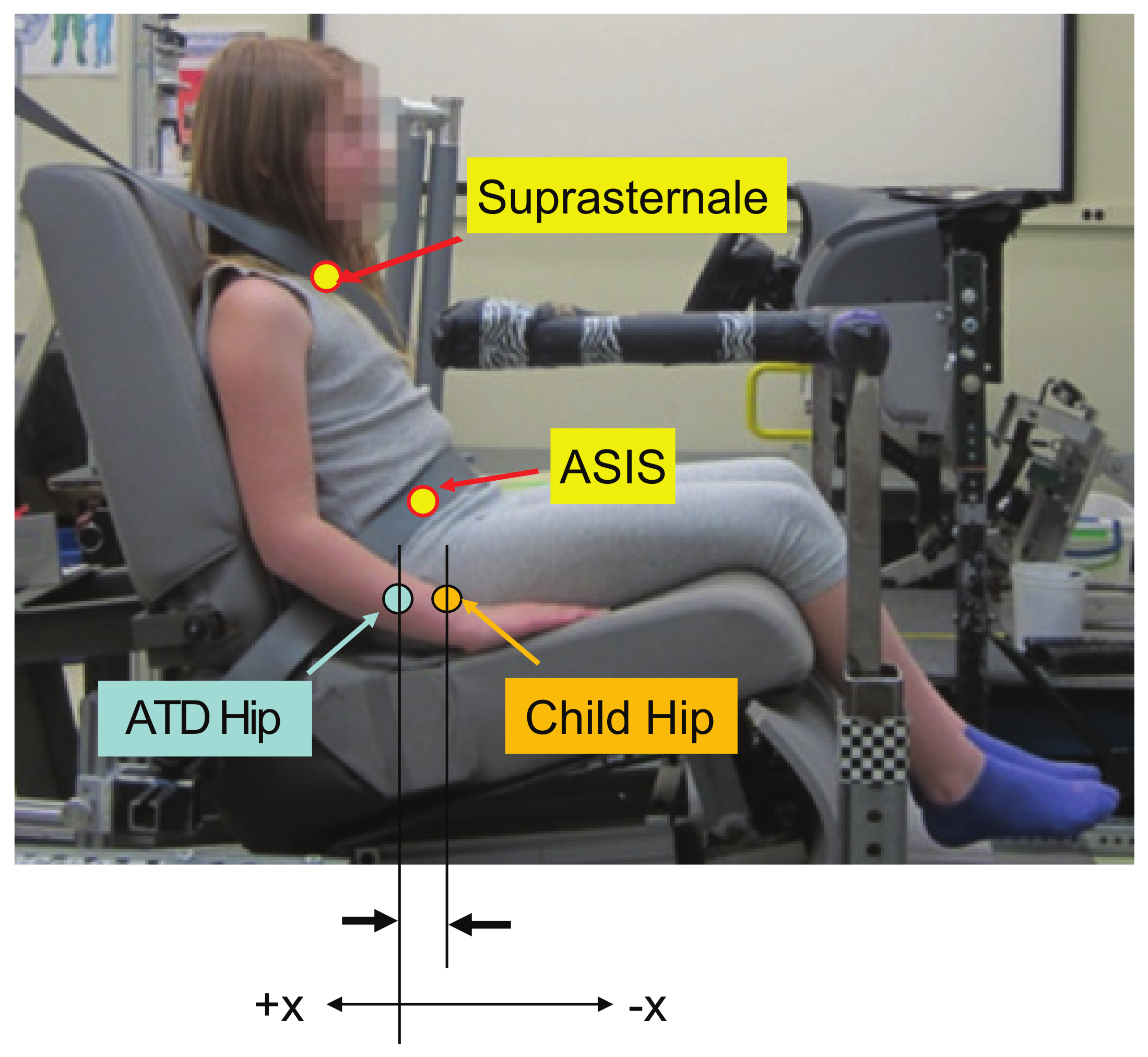
Some new boosters have reduced thickness compared with conventional boosters and consequently raise the child’s body upward to a lesser amount. Boosters that provide a minimum level of “boost” to anthropometric testing devices (ATD) have not been considered in previous studies. This boost is measured by the difference in the height of the ATD H-point (hip joint center) with and without the booster. In this context, the purpose of this research project was to measure the posture and belt fit of children and ATD in a range of boosters that included these new designs.
4. Discussion
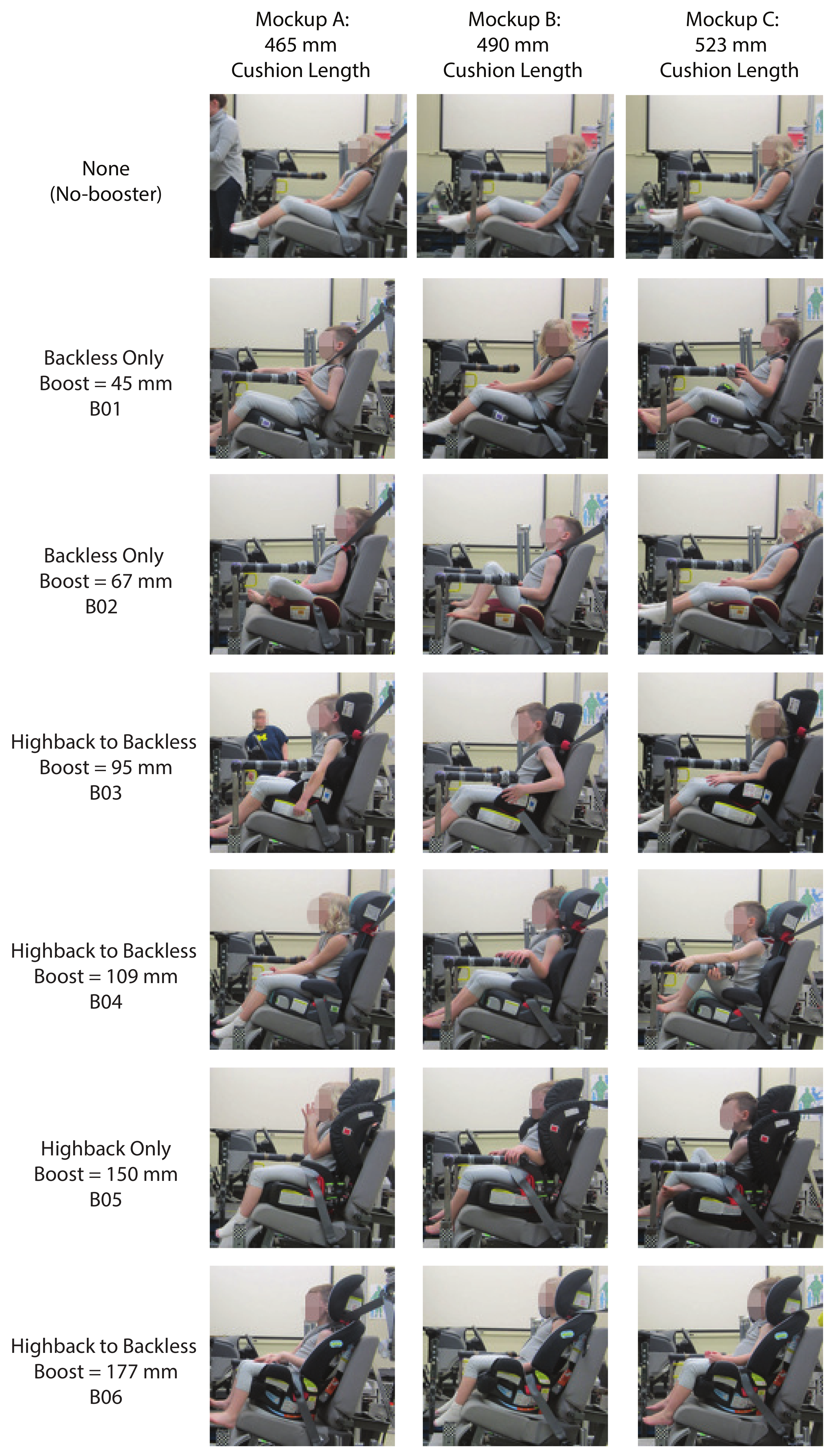
The use of belt positioning boosters reduce injury risk for child occupants compared with the use of seat belts alone. While boosters shorten the effective seat length (and thus reduce slouching), “boosting” the child relative to the vehicle interior components also achieves three additional safety benefits. First, the increase of the lap belt angle usually improves belt fit across the pelvis and reduces the risk of the occupant slipping (“submarining”) under the belt. Second, the torso belt is re-centered over the bony landmarks of the shoulder for more effective/secure restraint. Third, the child’s head is relocated in a range better protected by side airbags. Our hypothesis was that children would slouch more in lower boosters compared to taller boosters. Taller boosters effectively shorten the cushion length and enable a child’s knees to bend comfortably over the front of the booster. A low height booster may not allow the child’s knees to hang comfortably, possibly encouraging them to scoot forward to let their knees hang over the front edge of the vehicle seat. This study is the first to quantify posture and belt fit for children in booster configurations that vary widely in the amount of boost provided.
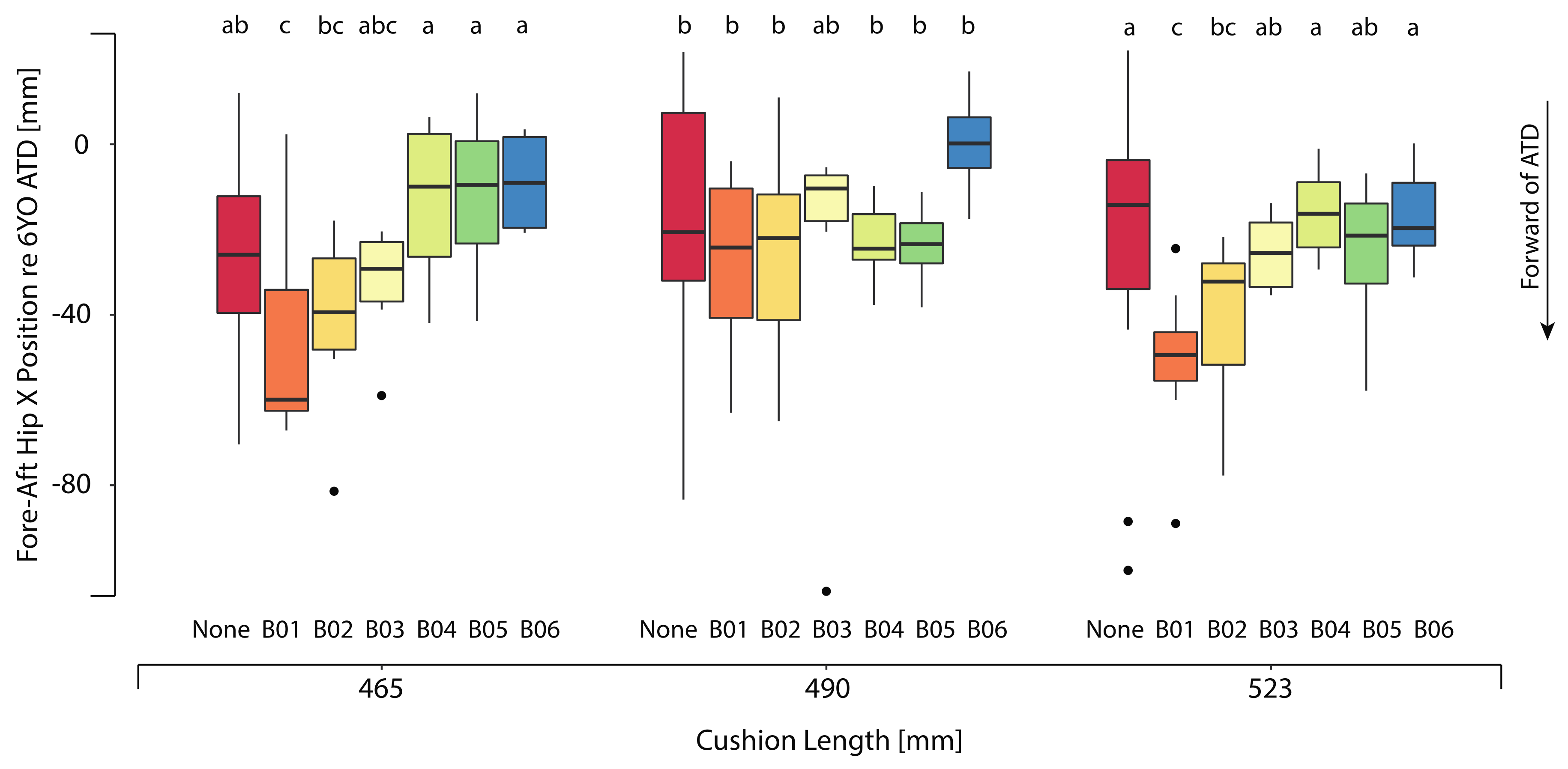
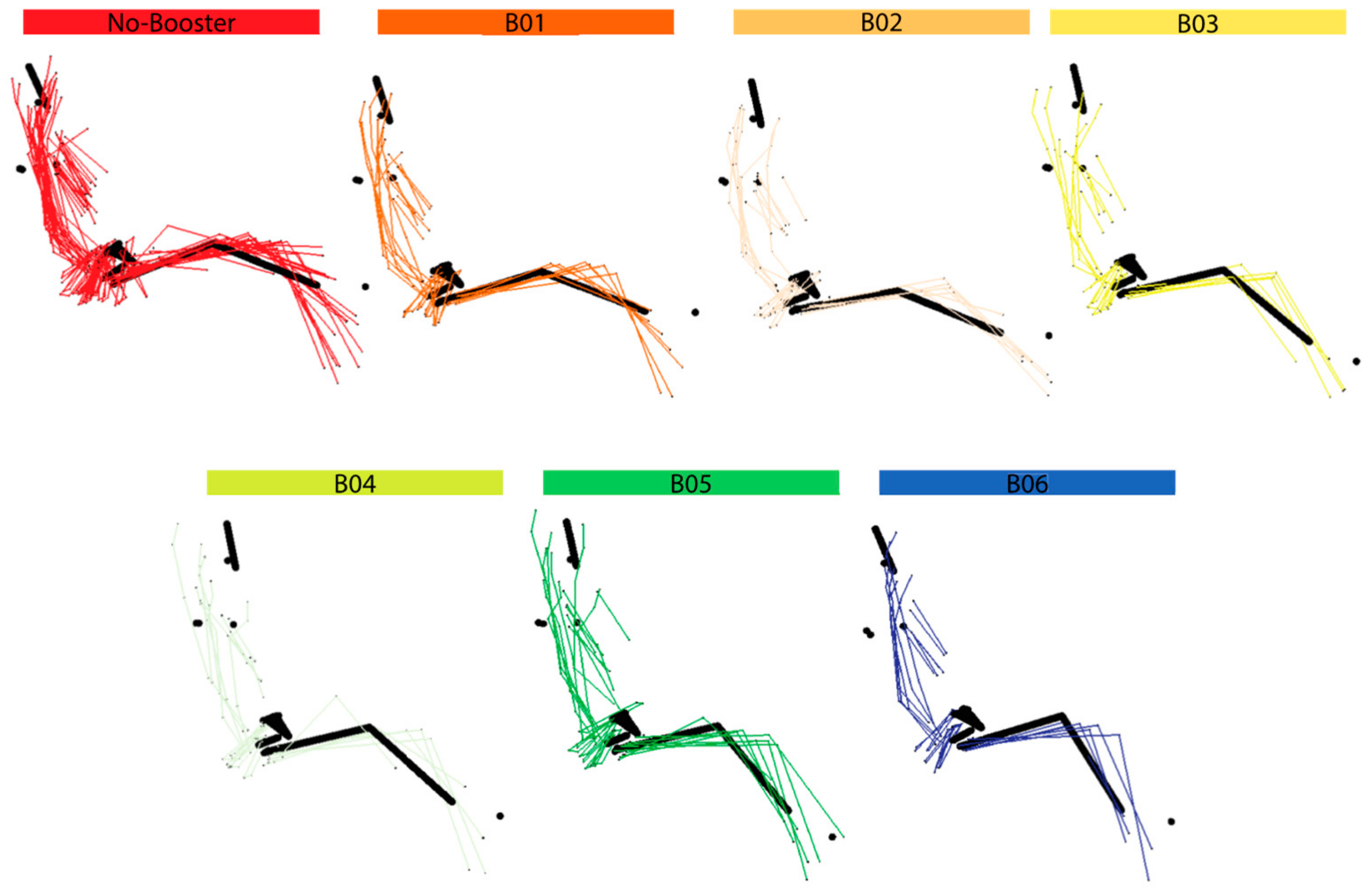
In this study, low height boosters were associated with more slouched postures, with hip positions more forward on the seat and lower head positions. Relative to the ATD, children’s hips were shifted forward more in the no-booster condition and two low height boosters vs. the taller boosters. This forward shift of the hips indicated more slumped postures. Of potential importance is the observation that posture variability among child volunteers was typically largest in the no-booster and low height booster conditions. Higher posture variability may increase the likelihood of poor restraint performance and thus greater risk of injury in the event of a crash.
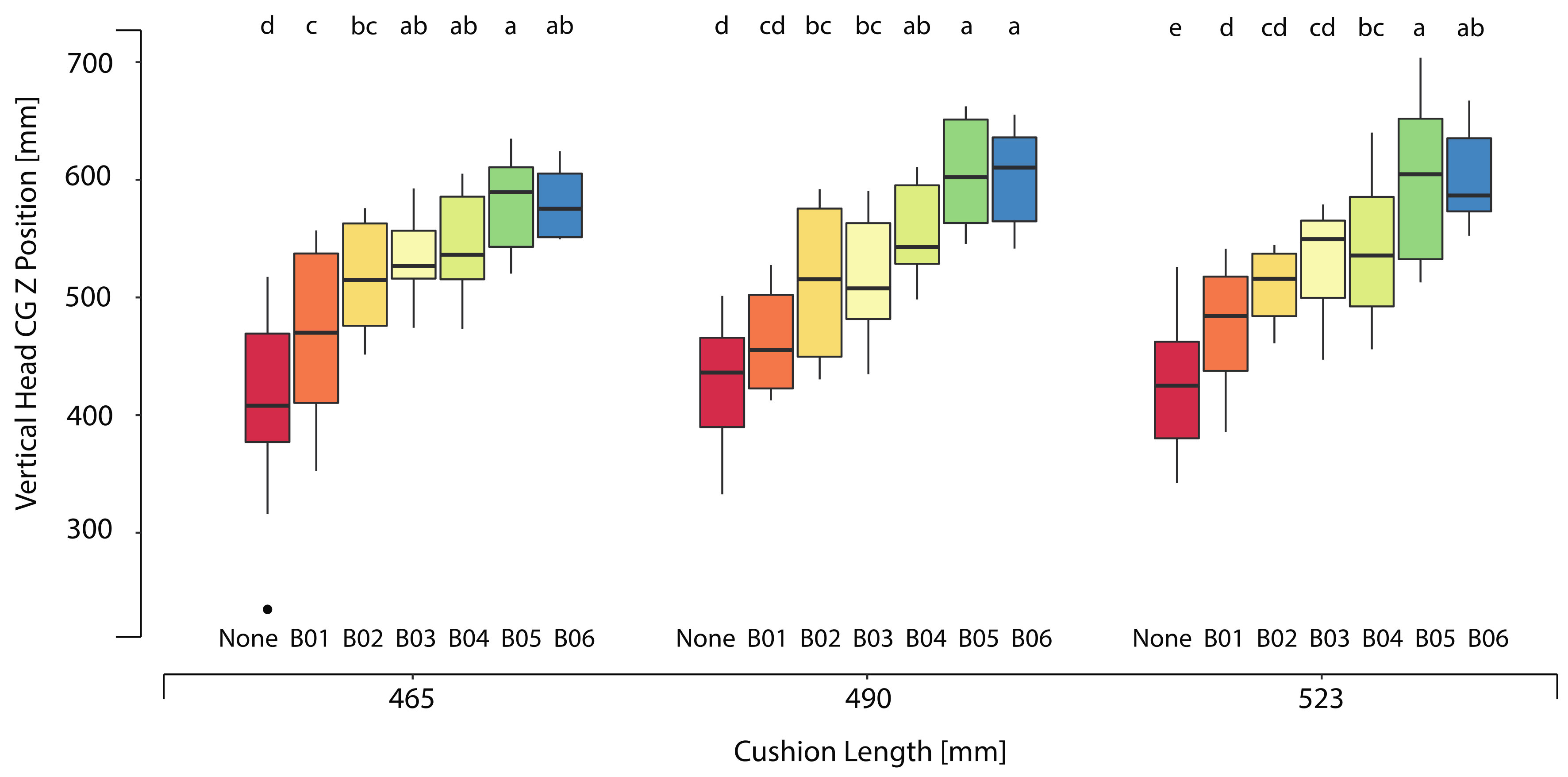
Ideally, the heads of children in boosters should be positioned within the same range of adult heads. This positioning would allow children to gain the most benefit from vehicle structures and curtain airbags that are evaluated relative to adult head positions. For the current study, we considered the head locations of the small female ATD and midsized male ATD. These locations ranged from 500 to 650 mm above the H-point as possible lower and upper bounds for child head position provided by a booster. All children participating in this study fell within the allowable stature range specified by each booster, but at least one child’s head fell below the range of the adult ATD head positions in all booster conditions. Of particular interest is the fact that the low height booster left most of the children’s heads below the adult range.
Boosters improved the average lap belt fit in all mockup conditions tested. The lap belt fit scores confirmed the benefit provided by boosters, with the no-booster condition consistently having the highest lap belt placement. Additionally under this condition, the shoulder belt fell closest to the neck. Boosters B02 through B06 also shifted the belt forward compared to the no-booster and B01 condition. The low height booster (B01, which provided only 45 mm of boost), had ineffective belt guides and had belt fit measures closest to the no-booster condition. Although the low height booster (B02) only provided 75 mm of boost, it offered better lap belt fit through the design of the lap belt guides that kept the belt low and forward of the pelvis. However, the improvement in lap belt fit varied widely among all of the boosters. Both lap belt and shoulder belt fit varied across the boosters, with no observable effect of seat cushion length. Differences in lap belt measures between no-booster and booster conditions were smaller in the current study compared to those measured in past studies [
10,
14,
15]. Since these test conditions encompassed a wider range of seat cushion lengths than in previous studies, this smaller measure may be the result of differences in parameterization of the mockup test conditions. For this study (rather than spanning the entire range of allowable angles), a range of belt angles were selected to represent the middle range seen in the vehicle fleet.
The principal limitation of this study is that all testing was conducted in a laboratory environment rather than in vehicles. Measuring child postures and belt fit in the laboratory allowed greater efficiency in testing because belt and seat geometry could be varied quickly and independently. This methodology controlled for the confounders of child occupant behavior that may be present in a naturalistic setting. Child occupant postures and behaviors have been shown to vary during everyday travel and in vehicles driven on-road [
27,
28,
29,
30]. In naturalistic driving studies (NDS) of child occupants’ head position when traveling in a CRS, Cross et al. [
27] showed that children were observed to be properly positioned in their CRS for only 58% of epochs evaluated. This sampling from Cross et al. [
27] was combined across forward-facing CRS and self-positioning boosters. In contrast, the results of the current study did not consider the effect on child posture from vehicle maneuvers, sleeping, or fidgeting. This study only captured “in-position” postures and belt fit and did not consider the effects of heavy clothing, which would be likely to degrade lap belt fit. Suboptimal postures and belt fit may increase the risk of injuries in the event of a crash [
31]. Findings from sled tests revealed compromised safety when ATD were placed in prevalent positions observed in the NDS [
31]. More specifically, suboptimal head position was associated with an increased likelihood of shoulder belt slip and greater forward head excursion.
Another limitation is that the results were based on only three seat cushion lengths obtained with a single vehicle seat mockup. Different vehicle seat and belt designs could change the relative performance of the boosters. Due to the relatively small sample of volunteers, no statistically significant differences in belt fit were observed between booster configurations. However, based on previous studies, these differences would likely be small in absolute terms.







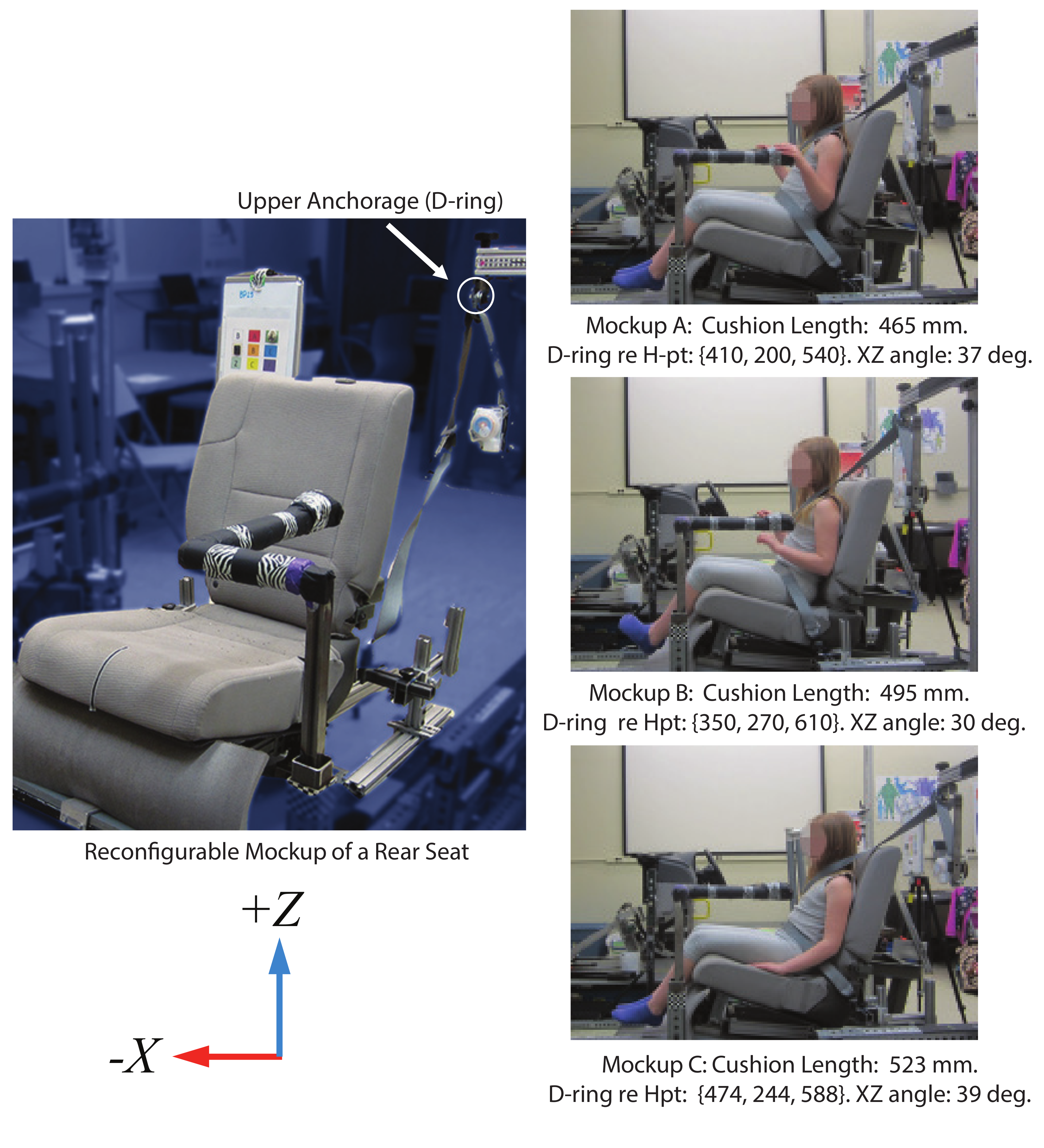







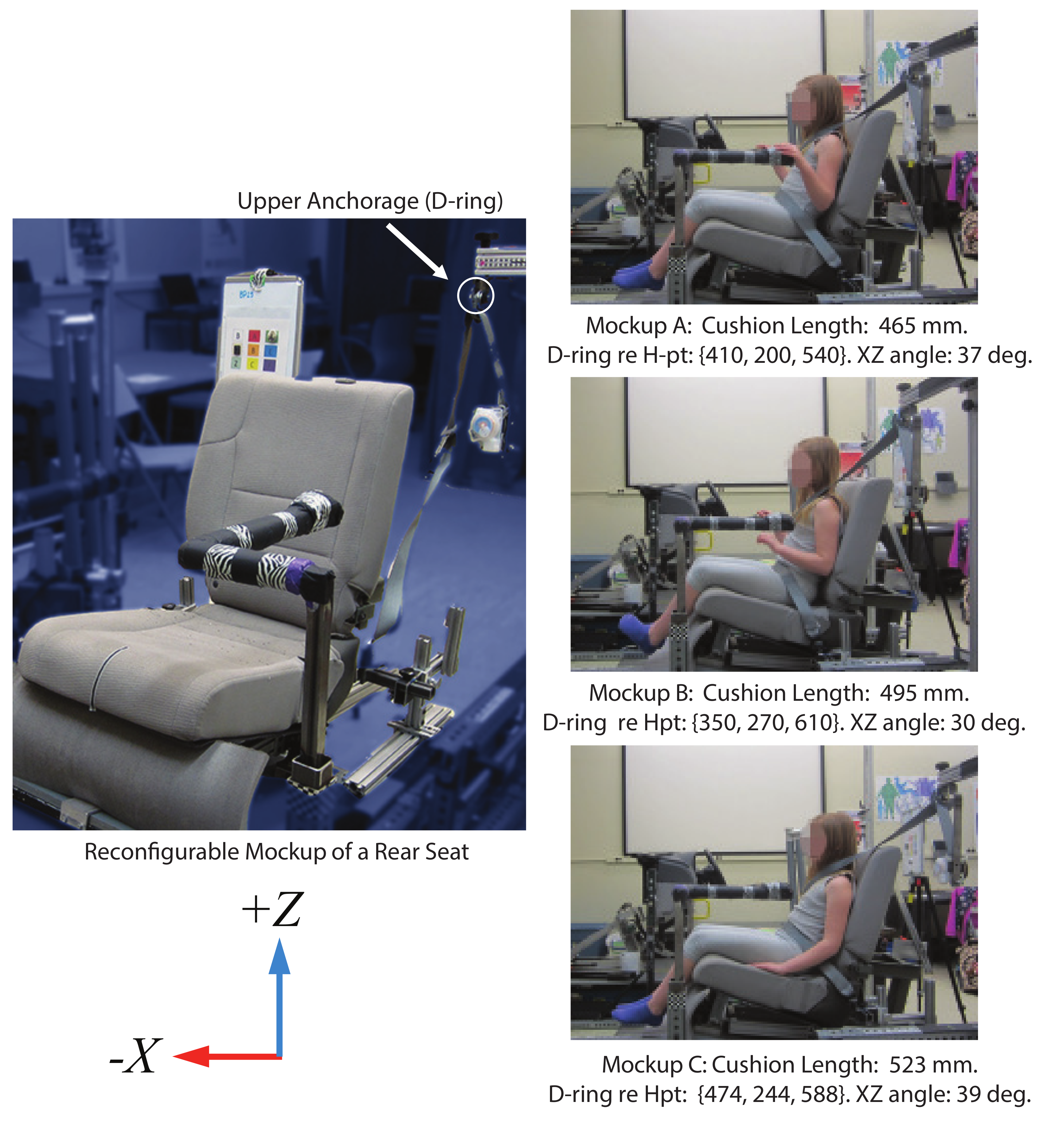
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}