
Implementation of an Electronic National Early Warning System to Decrease Clinical Deterioration in Hospitalized Patients at a Tertiary Medical Center


Abstract
:1. Introduction
2. Materials and Methods
2.1. Definition of Adverse Events and Diagnosis Groups at Discharge
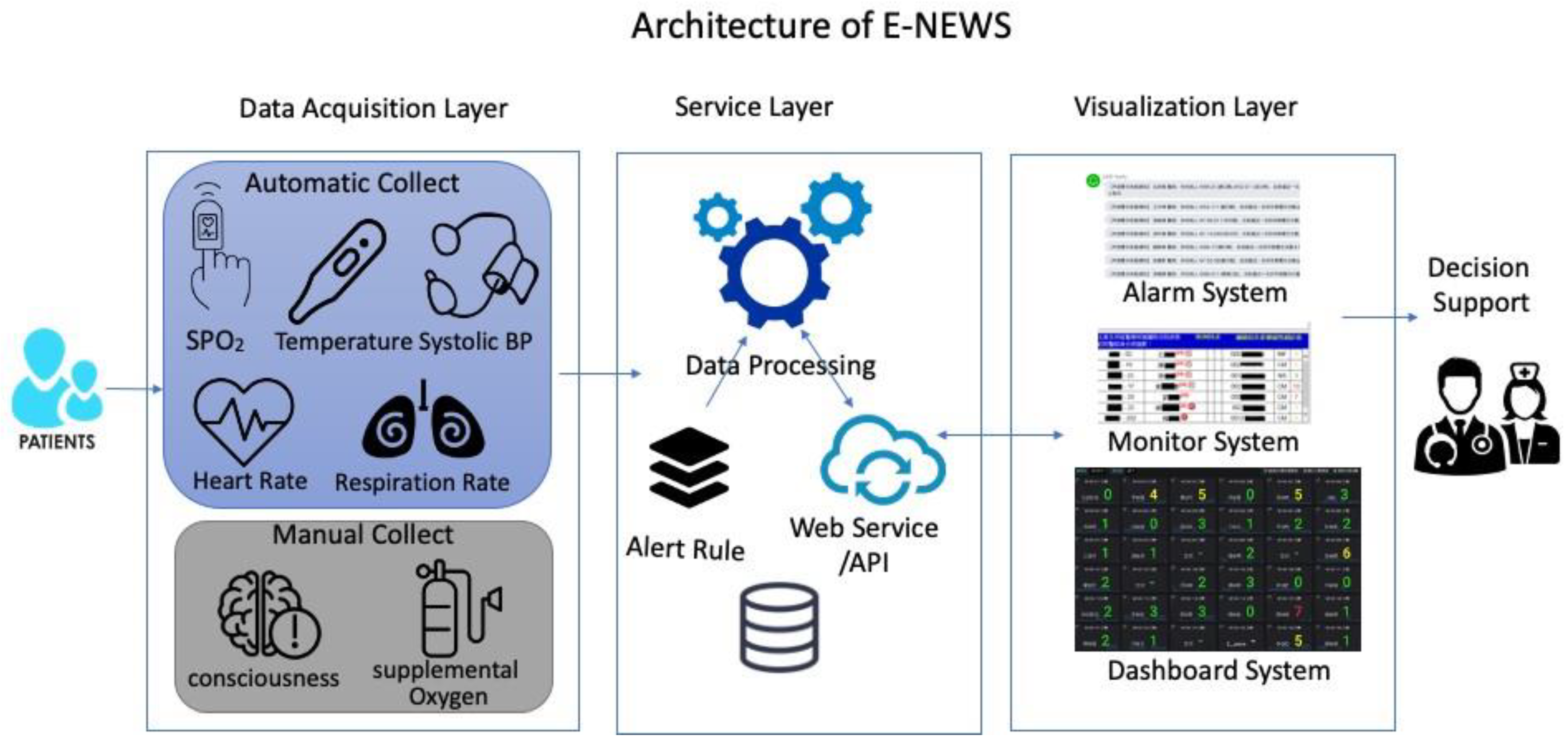
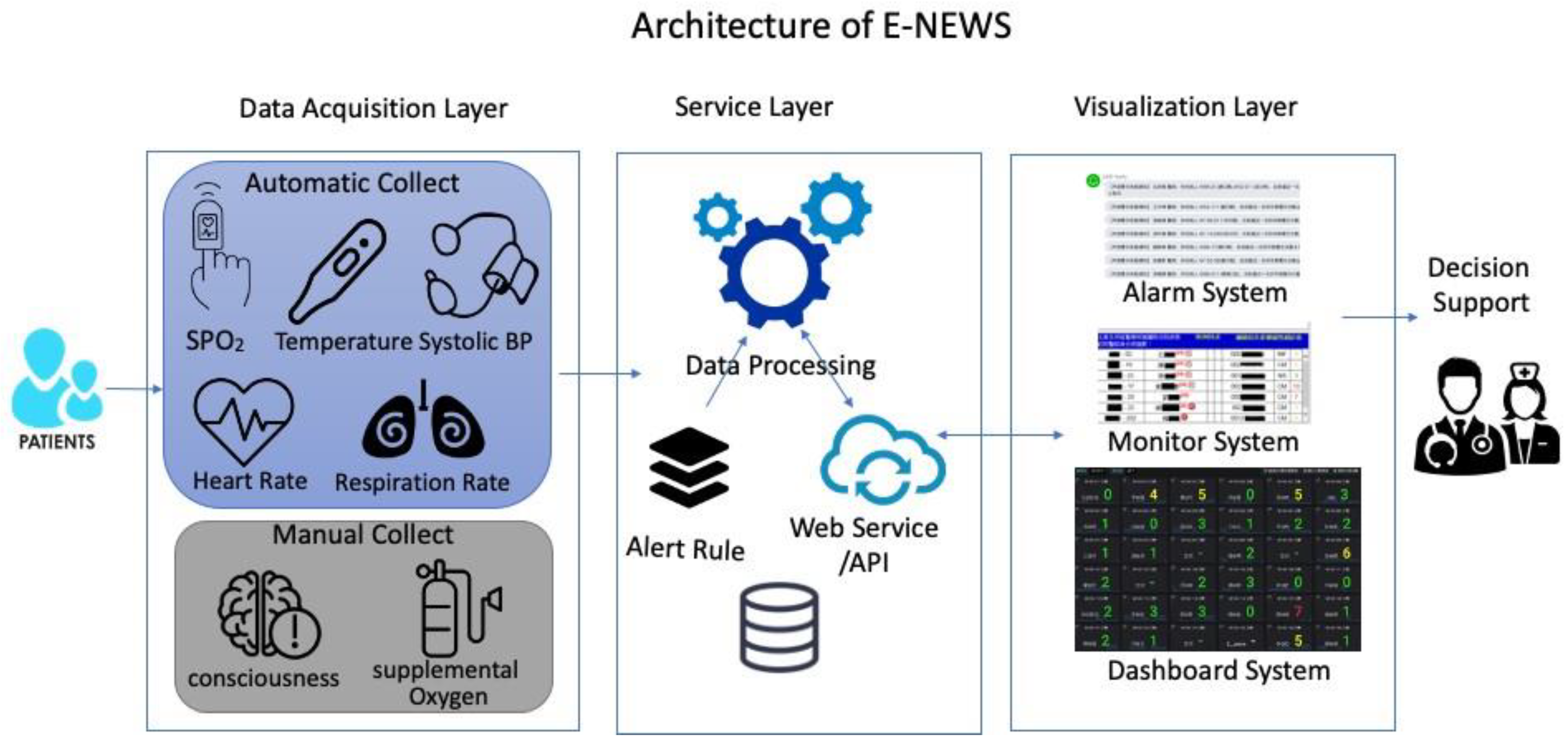
2.2. On-line Electronic NEWS System
2.3. Establishment of E-NEWS Dashboard on HIS and NIS
2.4. Implementation of E-NEWS
2.5. Statistical Analysis
3. Results
3.1. Study Population
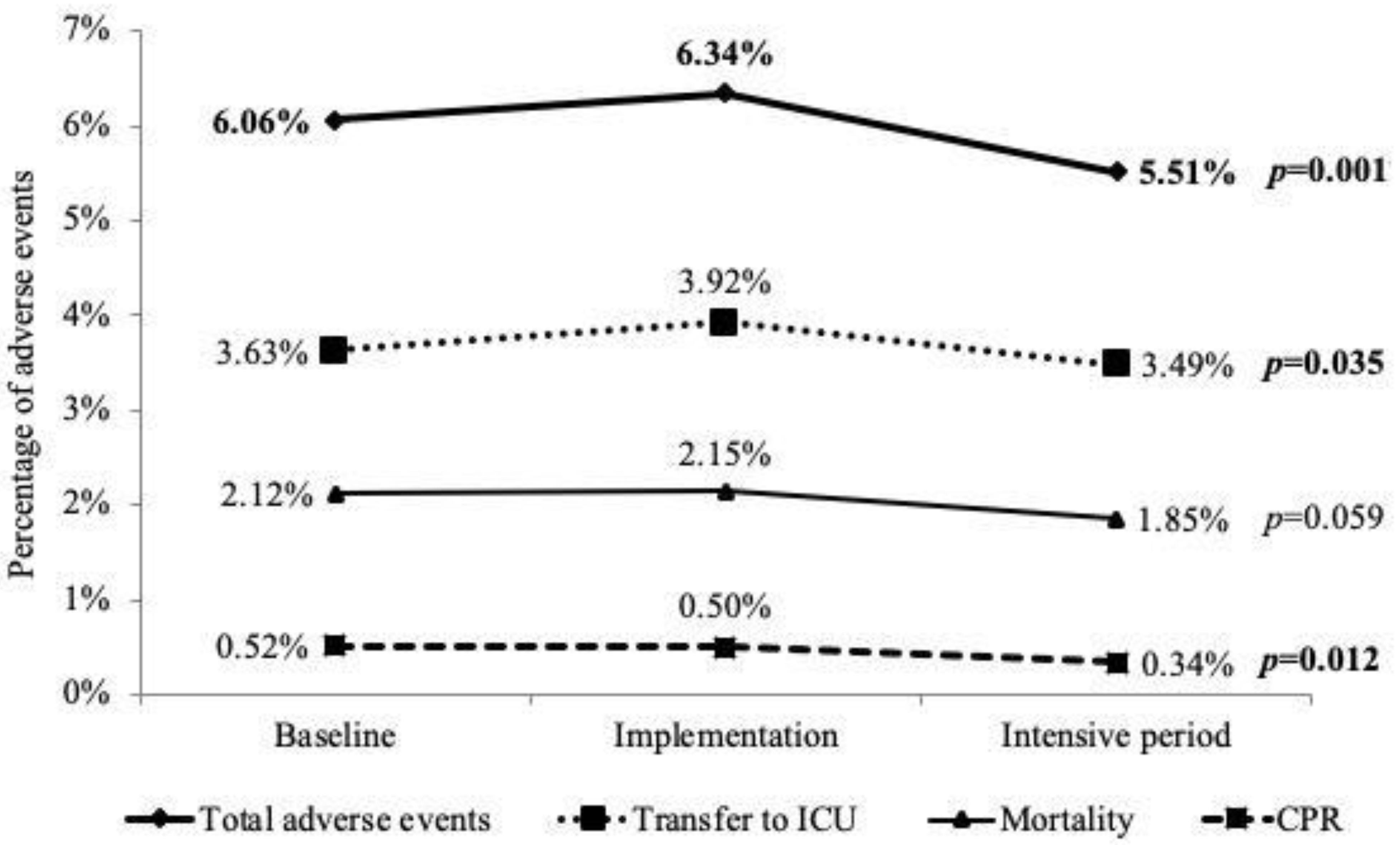
3.2. Reduction in AEs in Implementing E-NEWS
3.3. AEs in Different Clinical Situations
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Smith, A.F.; Wood, J. Can some in-hospital cardio-respiratory arrests be prevented? A prospective survey. Resuscitation 1998, 37, 133–137. [Google Scholar] [CrossRef]
- Hodgetts, T.J.; Kenward, G.; Vlackonikolis, I.; Payne, S.; Castle, N.; Crouch, R.; Ineson, N.; Shaikh, L. Incidence, location and reasons for avoidable in-hospital cardiac arrest in a district general hospital. Resuscitation 2002, 54, 115–123. [Google Scholar] [CrossRef]
- Smith, M.E.; Chiovaro, J.C.; O’Neil, M.; Kansagara, D.; Quinones, A.R.; Freeman, M.; Motu’apuaka, M.L.; Slatore, C.G. Early warning system scores for clinical deterioration in hospitalized patients: A systematic review. Ann. Am. Thorac. Soc. 2014, 11, 1454–1465. [Google Scholar] [CrossRef] [PubMed]
- Royal College of Physicians. National Early Warning Score (NEWS): Standardising the Assessment of Acute-Illness Severity in the NHS; Royal College of Physicians: London, UK, 2012. [Google Scholar]
- Royal College of Physicians. National Early Warning Score (NEWS) 2: Standardising the Assessment of Acute-Illness Severity in the NHS. Updated Report of a Working Party; Royal College of Physicians: London, UK, 2017. [Google Scholar]
- Mathukia, C.; Fan, W.; Vadyak, K.; Biege, C.; Krishnamurthy, M. Modified Early Warning System improves patient safety and clinical outcomes in an academic community hospital. J. Community Hosp. Intern. Med. Perspect. 2015, 5, 26716. [Google Scholar] [CrossRef] [PubMed]
- Nishijima, I.; Oyadomari, S.; Maedomari, S.; Toma, R.; Igei, C.; Kobata, S.; Koyama, J.; Tomori, R.; Kawamitsu, N.; Yamamoto, Y.; et al. Use of a modified early warning score system to reduce the rate of in-hospital cardiac arrest. J. Intensive Care 2016, 4, 12. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Downey, C.L.; Tahir, W.; Randell, R.; Brown, J.M.; Jayne, D.G. Strengths and limitations of early warning scores: A systematic review and narrative synthesis. Int. J. Nurs. Stud. 2017, 76, 106–119. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alam, N.; Hobbelink, E.L.; van Tienhoven, A.J.; van de Ven, P.M.; Jansma, E.P.; Nanayakkara, P.W. The impact of the use of the Early Warning Score (EWS) on patient outcomes: A systematic review. Resuscitation 2014, 85, 587–594. [Google Scholar] [CrossRef] [PubMed]
- Bedoya, A.D.; Clement, M.E.; Phelan, M.; Steorts, R.C.; O’Brien, C.; Goldstein, B.A. Minimal Impact of Implemented Early Warning Score and Best Practice Alert for Patient Deterioration. Crit. Care Med. 2019, 47, 49–55. [Google Scholar] [CrossRef] [PubMed]
- van Galen, L.S.; Dijkstra, C.C.; Ludikhuize, J.; Kramer, M.H.; Nanayakkara, P.W. A Protocolised Once a Day Modified Early Warning Score (MEWS) Measurement Is an Appropriate Screening Tool for Major Adverse Events in a General Hospital Population. PLoS ONE 2016, 11, e0160811. [Google Scholar] [CrossRef] [PubMed]
- Ghosh, E.; Eshelman, L.; Yang, L.; Carlson, E.; Lord, B. Early Deterioration Indicator: Data-driven approach to detecting deterioration in general ward. Resuscitation 2018, 122, 99–105. [Google Scholar] [CrossRef]
- Gerry, S.; Bonnici, T.; Birks, J.; Kirtley, S.; Virdee, P.S.; Watkinson, P.J.; Collins, G.S. Early warning scores for detecting deterioration in adult hospital patients: Systematic review and critical appraisal of methodology. BMJ 2020, 369, m1501. [Google Scholar] [CrossRef]
- Collins, G.S.; Reitsma, J.B.; Altman, D.G.; Moons, K.G.M. Transparent reporting of a multivariable prediction model for individual prognosis or diagnosis (TRIPOD): The TRIPOD statement. Ann. Intern. Med. 2015, 162, 55–63. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Churpek, M.M.; Yuen, T.C.; Winslow, C.; Robicsek, A.A.; Meltzer, D.O.; Gibbons, R.D.; Edelson, D.P. Multicenter development and validation of a risk stratification tool for ward patients. Am. J. Respir. Crit. Care Med. 2014, 190, 649–655. [Google Scholar] [CrossRef]
- Green, M.; Lander, H.; Snyder, A.; Hudson, P.; Churpek, M.; Edelson, D. Comparison of the Between the Flags calling criteria to the MEWS, NEWS and the electronic Cardiac Arrest Risk Triage (eCART) score for the identification of deteriorating ward patients. Resuscitation 2018, 123, 86–91. [Google Scholar] [CrossRef] [PubMed]
- Sutherasan, Y.; Theerawit, P.; Suporn, A.; Nongnuch, A.; Phanachet, P.; Kositchaiwat, C. The impact of introducing the early warning scoring system and protocol on clinical outcomes in tertiary referral university hospital. Ther. Clin. Risk Manag. 2018, 14, 2089–2095. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nannan Panday, R.S.; Minderhoud, T.C.; Alam, N.; Nanayakkara, P.W.B. Prognostic value of early warning scores in the emergency department (ED) and acute medical unit (AMU): A narrative review. Eur. J. Intern. Med. 2017, 45, 20–31. [Google Scholar] [CrossRef] [PubMed]
- Mullany, D.V.; Ziegenfuss, M.; Goleby, M.A.; Ward, H.E. Improved hospital mortality with a low MET dose: The importance of a modified early warning score and communication tool. Anaesth. Intensive Care 2016, 44, 734–741. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- de Vries, A.; Draaisma, J.M.T.; Fuijkschot, J. Clinician Perceptions of an Early Warning System on Patient Safety. Hosp. Pediatr. 2017, 7, 579–586. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
{kind=link}
| Total (n = 73,674) | Baseline (n = 23,543) | Implementation (n = 30,035) | Intensive Period (n = 20,096) | p Value | |||||
|---|---|---|---|---|---|---|---|---|---|
| n | % | n | % | n | % | n | % | ||
| Age (mean ± SD) | 57.9 | 17.1 | 58.1 | 17.3 | 57.8 | 17.2 | 57.9 | 16.8 | 0.165 |
| Gender-Male | 37,543 | (50.96%) | 12,036 | (51.12%) | 15,415 | (51.32%) | 10,092 | (50.22%) | 0.044 * |
| Diagnosis groups at discharge | |||||||||
| Cancer | 31,462 | (42.70%) | 9843 | (41.81%) | 12,945 | (43.10%) | 8674 | (43.16%) | 0.003 ** |
| Cardiovascular disorder | 12,083 | (16.40%) | 3874 | (16.45%) | 4910 | (16.35%) | 3299 | (16.42%) | 0.944 |
| Neurological (non-stroke) | 11,998 | (16.29%) | 3788 | (16.09%) | 4929 | (16.41%) | 3281 | (16.33%) | 0.597 |
| Neurological (stroke) | 3240 | (4.40%) | 1040 | (4.42%) | 1290 | (4.29%) | 910 | (4.53%) | 0.452 |
| Respiratory disorder | 7791 | (10.57%) | 2564 | (10.89%) | 3250 | (10.82%) | 1977 | (9.84%) | <0.001 ** |
| Diabetes | 10,012 | (13.59%) | 3113 | (13.22%) | 4135 | (13.77%) | 2764 | (13.75%) | 0.137 |
| Gastroenterology | 9571 | (12.99%) | 3041 | (12.92%) | 3895 | (12.97%) | 2635 | (13.11%) | 0.823 |
| Renal disorder | 6961 | (9.45%) | 2256 | (9.58%) | 2839 | (9.45%) | 1866 | (9.29%) | 0.572 |
| DNR code | 4751 | (6.45%) | 1515 | (6.44%) | 1990 | (6.63%) | 1246 | (6.20%) | 0.164 |
| Settings of clinical care | 0.994 | ||||||||
| Medical departments | 39,452 | (53.55%) | 12,600 | (53.52%) | 16,087 | (53.56%) | 10,765 | (53.57%) | |
| Surgical departments | 34,222 | (46.45%) | 10,943 | (46.48%) | 13,948 | (46.44%) | 9331 | (46.43%) | |
| Baseline | Implementation | Intensive Period | p Value | ||||
|---|---|---|---|---|---|---|---|
| n | % | n | % | n | % | ||
| Adverse events group | 1427 | (6.06%) | 1904 | (6.34%) | 1108 | (5.51%) | 0.001 ** |
| Age group | |||||||
| Age <40 | 79 | (2.12%) | 125 | (2.62%) | 77 | (2.58%) | 0.294 |
| Age 40–60 | 429 | (5.24%) | 567 | (5.34%) | 334 | (4.55%) | 0.043 * |
| Age 60–80 | 656 | (7.24%) | 839 | (7.31%) | 477 | (6.14%) | 0.003 ** |
| Age ≥80 | 263 | (10.25%) | 373 | (11.76%) | 220 | (11.05%) | 0.192 |
| Gender group | |||||||
| Female | 507 | (4.41%) | 665 | (4.55%) | 389 | (3.89%) | 0.038 * |
| Male | 920 | (7.64%) | 1239 | (8.04%) | 719 | (7.12%) | 0.027 * |
| Diagnosis at discharge | |||||||
| Cancer | 656 | (6.66%) | 874 | (6.75%) | 522 | (6.02%) | 0.080 |
| Cardiovascular disorder | 566 | (14.61%) | 780 | (15.89%) | 446 | (13.52%) | 0.011 * |
| Neurological (non-stroke) | 425 | (11.22%) | 585 | (11.87%) | 345 | (10.52%) | 0.163 |
| Neurological (stroke) | 174 | (16.73%) | 235 | (18.22%) | 145 | (15.93%) | 0.348 |
| Respiratory disorder | 406 | (15.83%) | 602 | (18.52%) | 339 | (17.15%) | 0.026 * |
| Diabetes | 361 | (11.60%) | 496 | (12.00%) | 300 | (10.85%) | 0.347 |
| Gastroenterology | 317 | (10.42%) | 349 | (8.96%) | 218 | (8.27%) | 0.015 * |
| Renal disorder | 320 | (14.18%) | 439 | (15.46%) | 257 | (13.77%) | 0.219 |
| DNR code | 896 | (4.07%) | 1216 | (4.34%) | 702 | (3.72%) | 0.005 ** |
| Settings of clinical care group | |||||||
| Medical departments | 842 | (6.68%) | 1150 | (7.15%) | 637 | (5.92%) | <0.001 ** |
| Surgical departments | 585 | (5.35%) | 754 | (5.41%) | 471 | (5.05%) | 0.464 |
| Univariate Model | Multivariate Model | |||
|---|---|---|---|---|
| OR | (95% CI) | OR | (95% CI) | |
| Stage of implementation | ||||
| Baseline | ref. | ref. | ||
| Implementation | 1.05 | (0.98–1.13) | 1.05 | (0.97–1.13) |
| Intensive period | 0.90 | (0.83–0.98) * | 0.90 | (0.83–0.98) * |
| Age | 1.03 | (1.02–1.03) ** | 1.01 | (1.01–1.01) ** |
| Gender (Male vs. Female) | 1.84 | (1.73–1.96) ** | 1.47 | (1.38–1.57) ** |
| Diagnosis group at discharge | ||||
| Cancer | 1.16 | (1.10–1.24) ** | 2.16 | (2.02–2.32) ** |
| Cardiovascular disorder | 3.88 | (3.64–4.13) ** | 2.87 | (2.65–3.10) ** |
| Neurological (non-stroke) | 2.42 | (2.26–2.59) ** | 1.64 | (1.39–1.93) ** |
| Neurological (stroke) | 3.53 | (3.21–3.89) ** | 2.08 | (1.86–2.32) ** |
| Respiratory disorder | 4.24 | (3.96–4.55) ** | 2.97 | (2.75–3.21) ** |
| Diabetes | 2.40 | (2.24–2.58) ** | 0.75 | (0.64–0.89) ** |
| Gastroenterology | 1.73 | (1.60–1.87) ** | 1.35 | (1.24–1.47) ** |
| Renal disorder | 3.16 | (2.93–3.41) ** | 1.62 | (1.49–1.77) ** |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wu, C.-L.; Kuo, C.-T.; Shih, S.-J.; Chen, J.-C.; Lo, Y.-C.; Yu, H.-H.; Huang, M.-D.; Sheu, W.H.-H.; Liu, S.-A. Implementation of an Electronic National Early Warning System to Decrease Clinical Deterioration in Hospitalized Patients at a Tertiary Medical Center. Int. J. Environ. Res. Public Health 2021, 18, 4550. https://doi.org/10.3390/ijerph18094550
Wu C-L, Kuo C-T, Shih S-J, Chen J-C, Lo Y-C, Yu H-H, Huang M-D, Sheu WH-H, Liu S-A. Implementation of an Electronic National Early Warning System to Decrease Clinical Deterioration in Hospitalized Patients at a Tertiary Medical Center. International Journal of Environmental Research and Public Health. 2021; 18(9):4550. https://doi.org/10.3390/ijerph18094550
Chicago/Turabian StyleWu, Chieh-Liang, Chen-Tsung Kuo, Sou-Jen Shih, Jung-Chen Chen, Ying-Chih Lo, Hsiu-Hui Yu, Ming-De Huang, Wayne Huey-Herng Sheu, and Shih-An Liu. 2021. "Implementation of an Electronic National Early Warning System to Decrease Clinical Deterioration in Hospitalized Patients at a Tertiary Medical Center" International Journal of Environmental Research and Public Health 18, no. 9: 4550. https://doi.org/10.3390/ijerph18094550