
New Prognostic Factors in Operated Extracapsular Hip Fractures: Infection and GammaTScore

 , ,
, , 
Abstract
:1. Introduction
- -
- Physiopathology: It is probably underdiagnosed when we only observe disrotation without migration. However, there are some cases when the cut-out does not progress and the fracture consolidates, but we do not know when and why this occurs [8];
- -
- -
- -
- Design improvements [16]: Smaller nail diameters and advances in PLDs;
- -
- Learning curve [17]: The quick widespread use of nails in all ECFs (instead of DHSs);
- -
- Biomechanical factors: Cleveland and Bosworth [18] wrote that the PLD distal end in the centre–centre or posteroinferior quadrant prevents from this complication. Parker [6] pointed out that the ideal position was central or inferior in anteroposterior view and central in lateral view. There is no consensus on the peripheral position with worst prognosis [4]. Baumgaertner demonstrated that a < 25 mm tip–apex distance (TAD), as the sum of anteroposterior and axial projections, is a protective factor [7]. Subsequently, new factors or modifications of previous ones have been described, but they have not been as universally accepted or recognized [19]: calcar-referenced TAD < 25 mm [20], varus reduction [21], ECF extension to the femoral neck [22], posterior subtype of Ikuta’s classification [23], vertical shear fracture [24] and intraoperative breakage/lack of lateral wall competency [25].
2. Materials and Methods
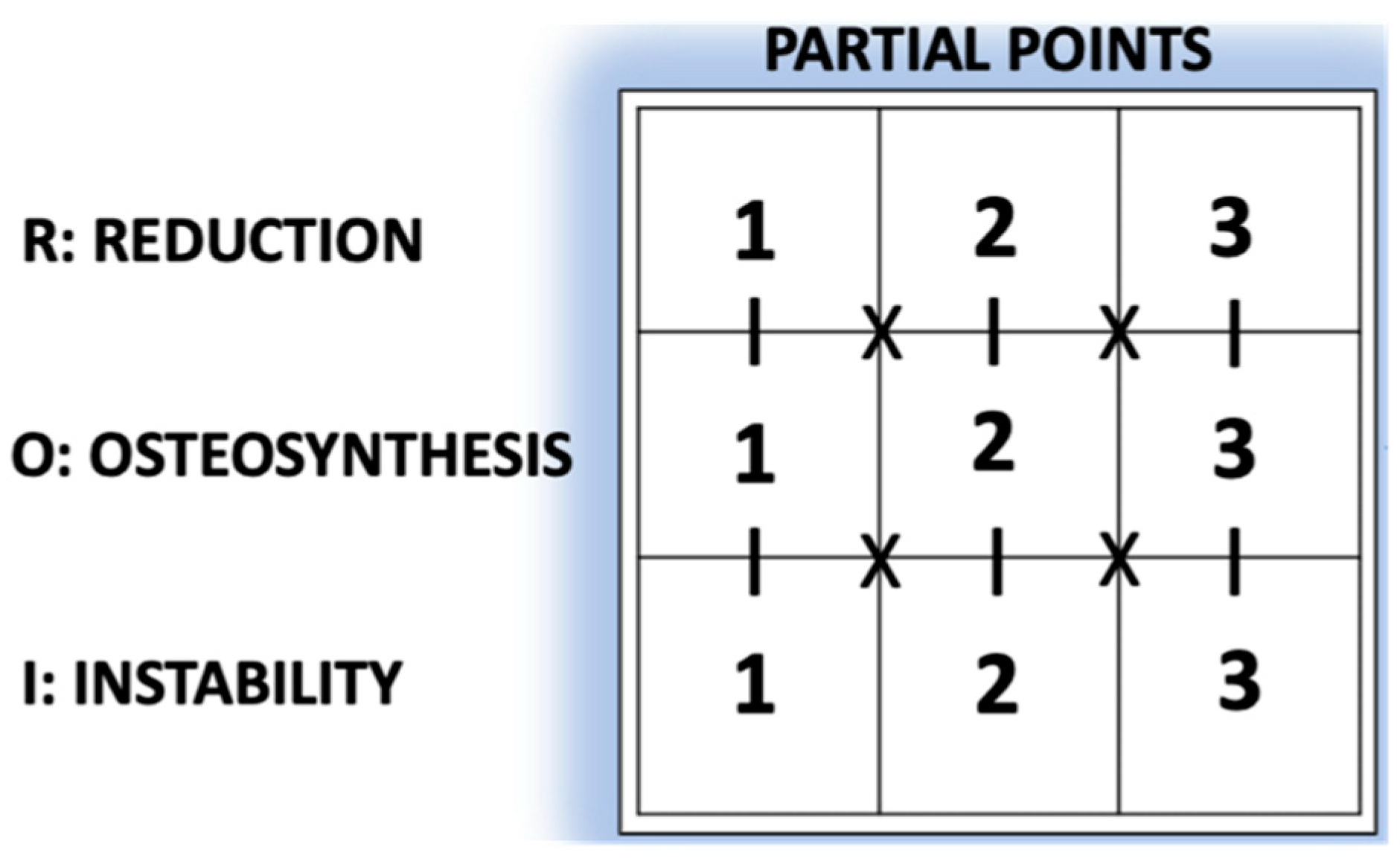
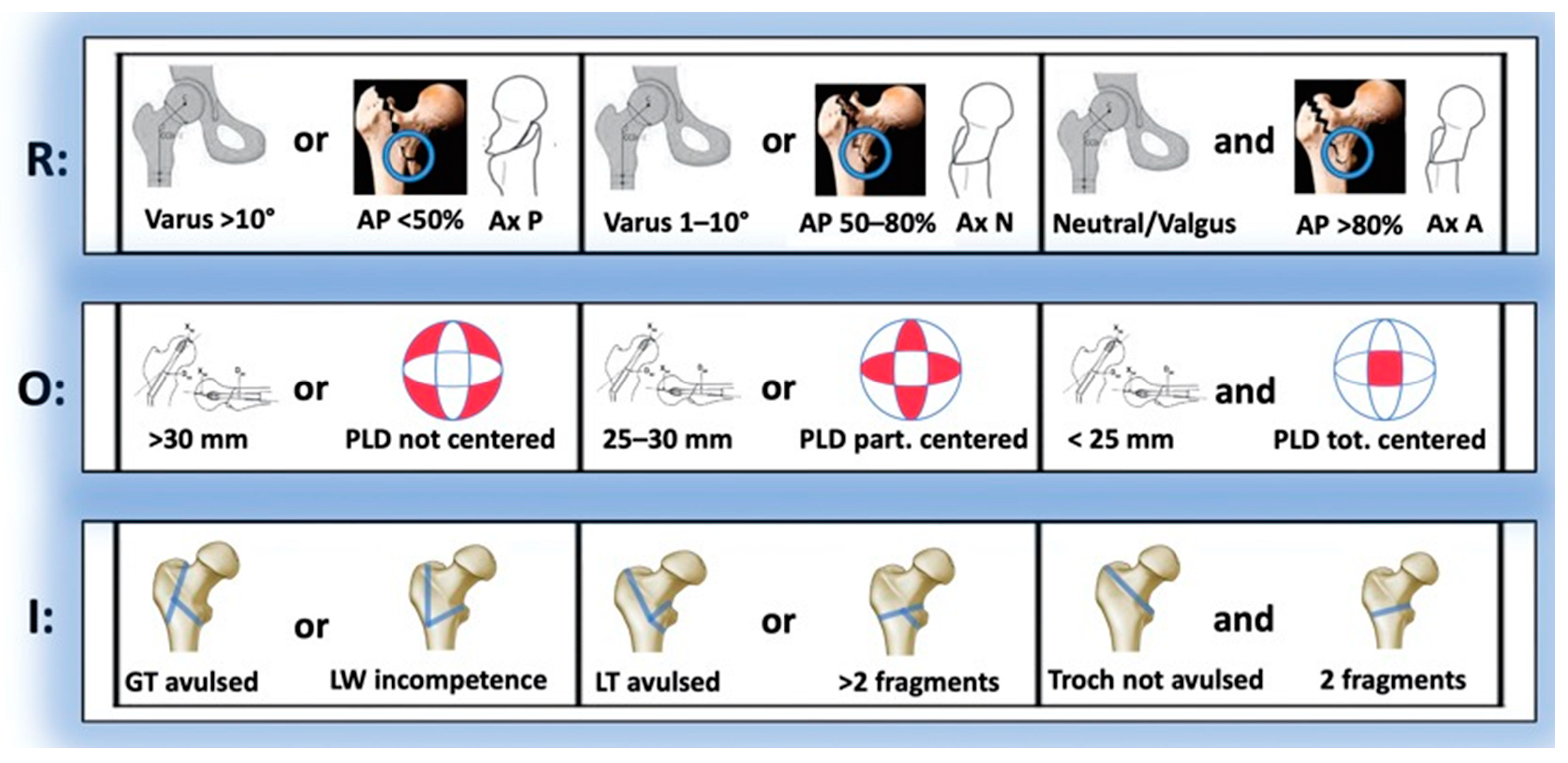
- Reduction parameter (R):
- CCD (Varus/Neutral/Valgus): Difference between the caput–collum–diaphyseal (CCD) angle of the currently operated hip and that of the contralateral one (if the latter was previously operated on, this CCD was taken as a reference);
- AP%: Percentage of cortical contact in AP view;
- P, N or A: Posterior, normal or anterior types (Ikuta’s classification, axial view).
- Osteosynthesis parameter (O):
- TAD: Tip-to-apex distance;
- PLD: Location of the proximal locking device (PLD) in the femoral head (Cleveland–Bostworth classification).
- Instability parameter (I):
- Avulsion: Defined as a radiolucent space > 5 mm in any radiological view of the greater trochanter (GT) or the lesser trochanter (LT);
- LW (lateral wall) in/competence (AO Foundation/Orthopaedic Trauma Association classification; AO/OTA classification 2018).
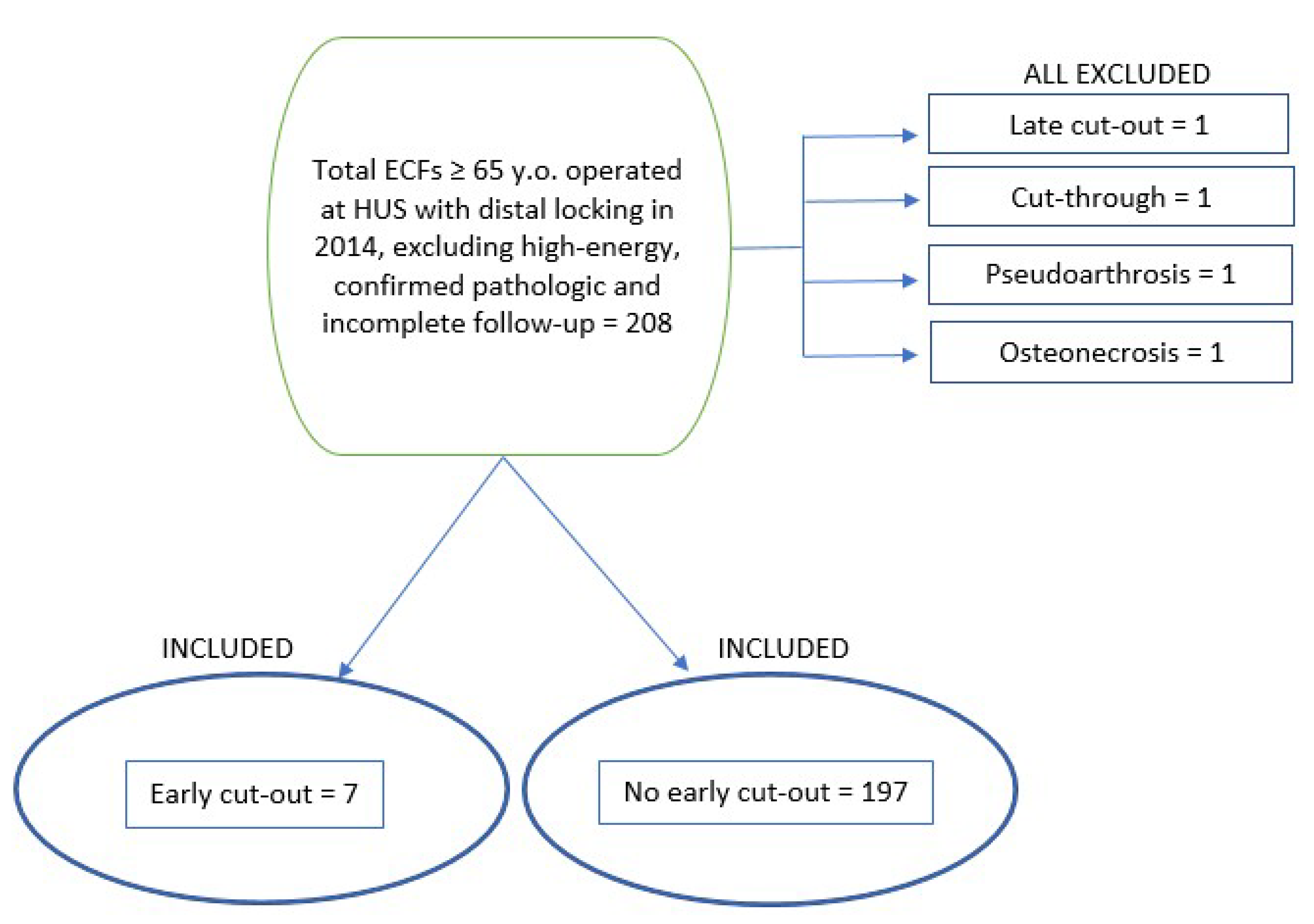
3. Results
3.1. Preoperative Variables (Table 1)

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Early Cut-Out | No Early Cut-Out | p |
|---|---|---|---|
| Age (years-old) | 83 (SD 10.31) (65;99) | 85.82 (SD 6.59) (65;103) | 0.512 c |
| Sex | 0.640 a | ||
| -Female | 5 (71.4%) | 156 (79.2%) | |
| -Male | 2 (28.6%) | 41 (20.8%) | |
| Side | 1.000 a | ||
| -Left | 3 (42.4%) | 81 (41.1%) | |
| -Right | 4 (57.6%) | 116 (58.9%) | |
| Social situation | 0.121 a | ||
| -Home, alone | 3 (42.9%) | 26 (13.2%) | |
| -Home, not alone | 3 (42.9%) | 104 (52.8%) | |
| -Institutionalized | 1 (14.3%) | 67 (34.0%) | |
| Dependency | |||
| -Barthel pre-Sx. | 86.43 (SD 16.51) (55;100) | 75.28 (SD 21.57) (10;100) | 0.150 c |
| -Barthel post-Sx. | 43.57 (SD 21.74) (15;75) | 46.78 (SD 20.93) (10;85) | 0.697 c |
| Comorbidity | |||
| -Non-age-adjusted CMI | 2.57 (SD 1.13) (1;4) | 2.15 (SD 1.29) (0;7) | 0.293 c |
| -Age-adjusted CMI | 6.42 (SD 1.27) (5;8) | 6.11 (SD 1.30) (4;11) | 0.467 c |
| Cognitive status | 1.000 a | ||
| -None | 1 (14.3%) | 33 (16.8%) | |
| -Mild | 5 (71.4%) | 130 (66.0%) | |
| -Moderate | 1 (14.3%) | 33 (16.8%) | |
| -Severe | 0 (0%) | 1 (0.5%) | |
| Previous Fx. | 1.000 a | ||
| -None | 5 (71.4%) | 114 (57.9%) | |
| -Traumatic | 0 (0%) | 6 (3.0%) | |
| -OP fracture | |||
| --Hip | 0 (0%) | 15 (7.6%) | |
| --Other locations | 2 (28.6%) | 54 (27.4%) | |
| --Both locations | 0 (0%) | 8 (4.1%) | |
| OP treatment # | 0.596 b | ||
| -No | 129 (85.4%) | 47 (82.5%) | |
| -Yes | 22 (14.6%) | 10 (17.5%) | |
| APT/ACT | 0.882 a | ||
| -None | 5 (71.4%) | 110 (55.8%) | |
| -AAS 100 | 2 (28.6%) | 39 (19.8%) | |
| -AAS 300 | 0 (0%) | 17 (8.6%) | |
| -Clopidogrel | 0 (0%) | 1 (0.5%) | |
| -Acenocumarol | 0 (0%) | 26 (13.2%) | |
| -Direct Xa | 0 (0%) | 2 (2.0%) | |
| -LMWH | 0 (0%) | 2 (2.0%) | |
| ASA | 3 (1;4) | 3 (1;4) | 0.503 d |
3.2. Perioperative Variables (Table 2)
| Variable | Early Cut-Out | No Early Cut-Out | p |
|---|---|---|---|
| Jensen | 0.345 a | ||
| Stability (Jensen) | 0.713 a | ||
| -Stable (I + II) | 3 (42.9%) | 73 (37.1%) | |
| -Unstable (III + IV + V) | 4 (57.1%) | 124 (62.9%) | |
| AO/OTA, 2007 * | 0.033 b, * | ||
| -A1 | 3 (42.9%) | 59 (29.9%) | |
| -A2 | 1 (14.3%) | 111 (56.3%) | |
| -A3 | 2 (28.6%) | 17 (8.6%) | |
| Stability(AO/OTA, 2007) | 0.305 b | ||
| Stable | 3 (42.9%) | 118 (59.9%) | |
| Unstable | 3 (42.9%) | 69 (35.0%) | |
| Basicervical (B2.1) | 1 (14.3%) | 10 (5.1%) | |
| Massoud | 1.000 b | ||
| -Stable | 4 (57.1%) | 68 (34.5%) | |
| -Unstable | 3 (42.9%) | 129 (65.5%) | |
| Average stay (days) | 9.57 (SD 2.63) (6;13) | 9.71 (SD 3.36) (4;26) | 0.880 c |
| Pre-Sx. stay (days) | 3.00 (SD 2.00) (0;5) | 3.30 (SD 2.56) (0;9) | 0.749 c |
| Post-Sx. stay (days) | 6.57 (SD 2.22) (3;9) | 6.37 (SD 2.79) (3;25) | 0.431 c |
| Blood loss (g/dl Hb) | 1.42 (SD 1.16) (0;3.0) | 1.92 (SD 1.75) (−3.5;5.9) | 0.323 c |
| Transfusions [RBC] | 1.85 (SD 1.67) (0;5) | 1.35 (SD 1.37) (0;8) | 0.427 c |
3.3. Postperative Variables
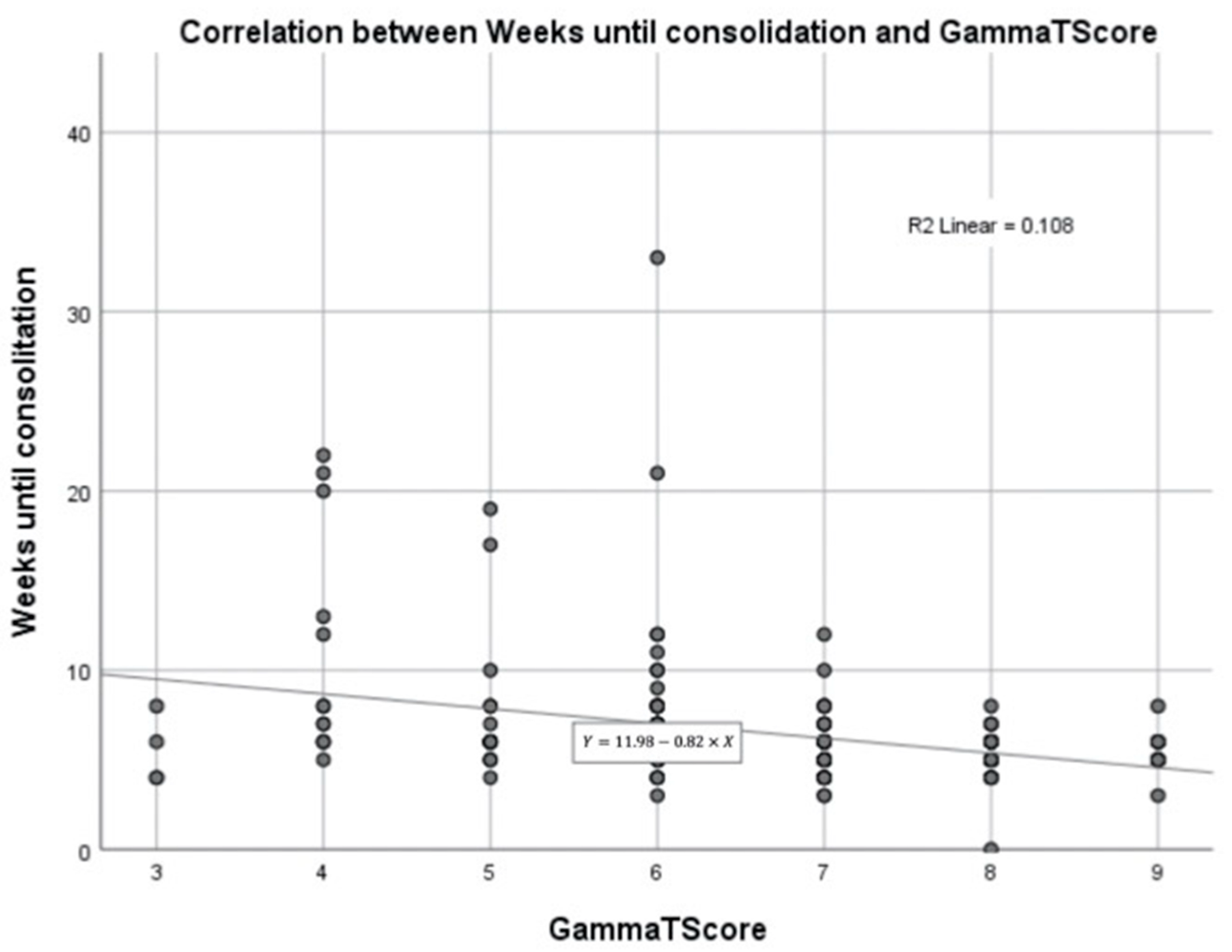
3.4. Consolidation (Figure 5)

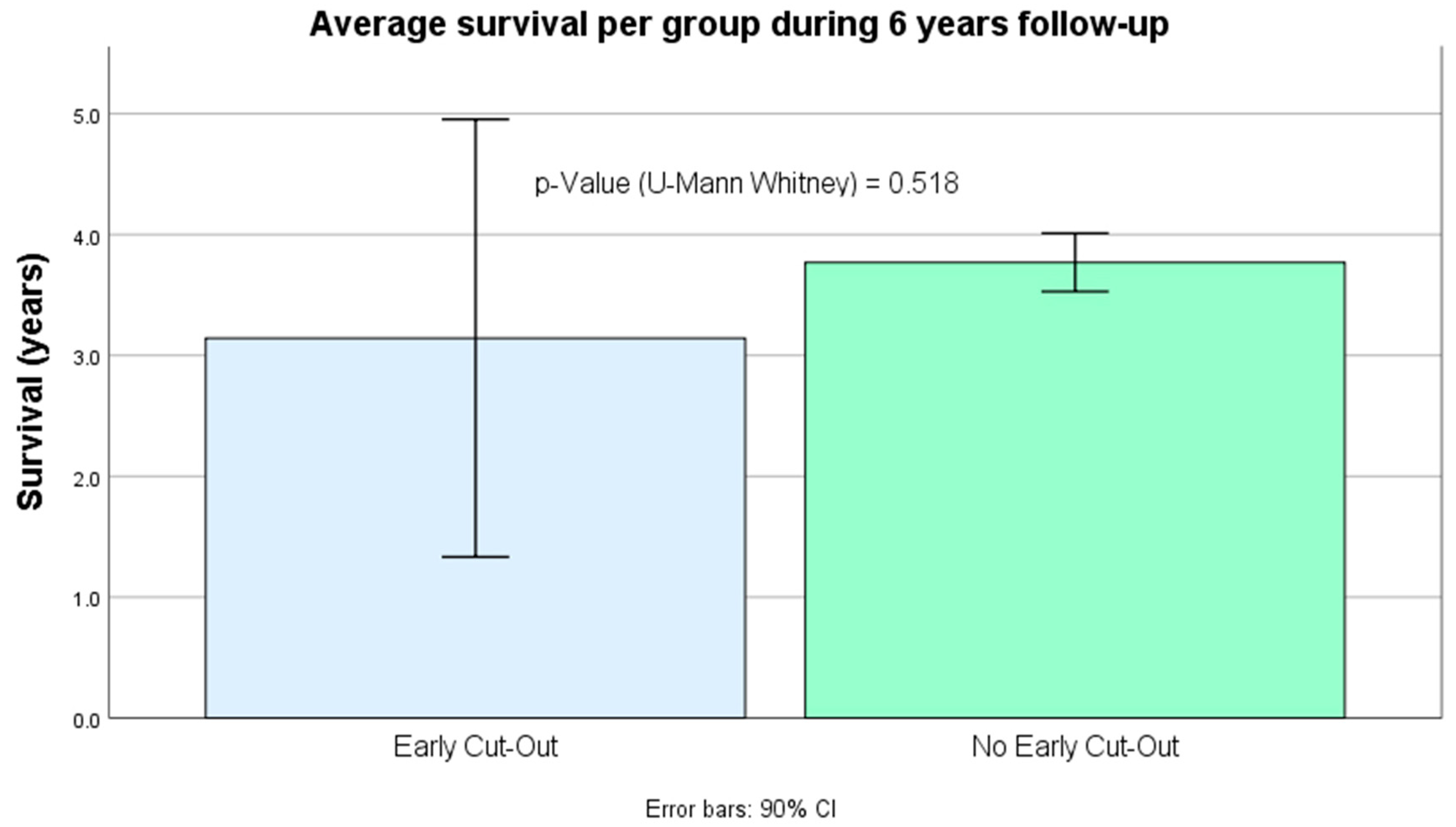
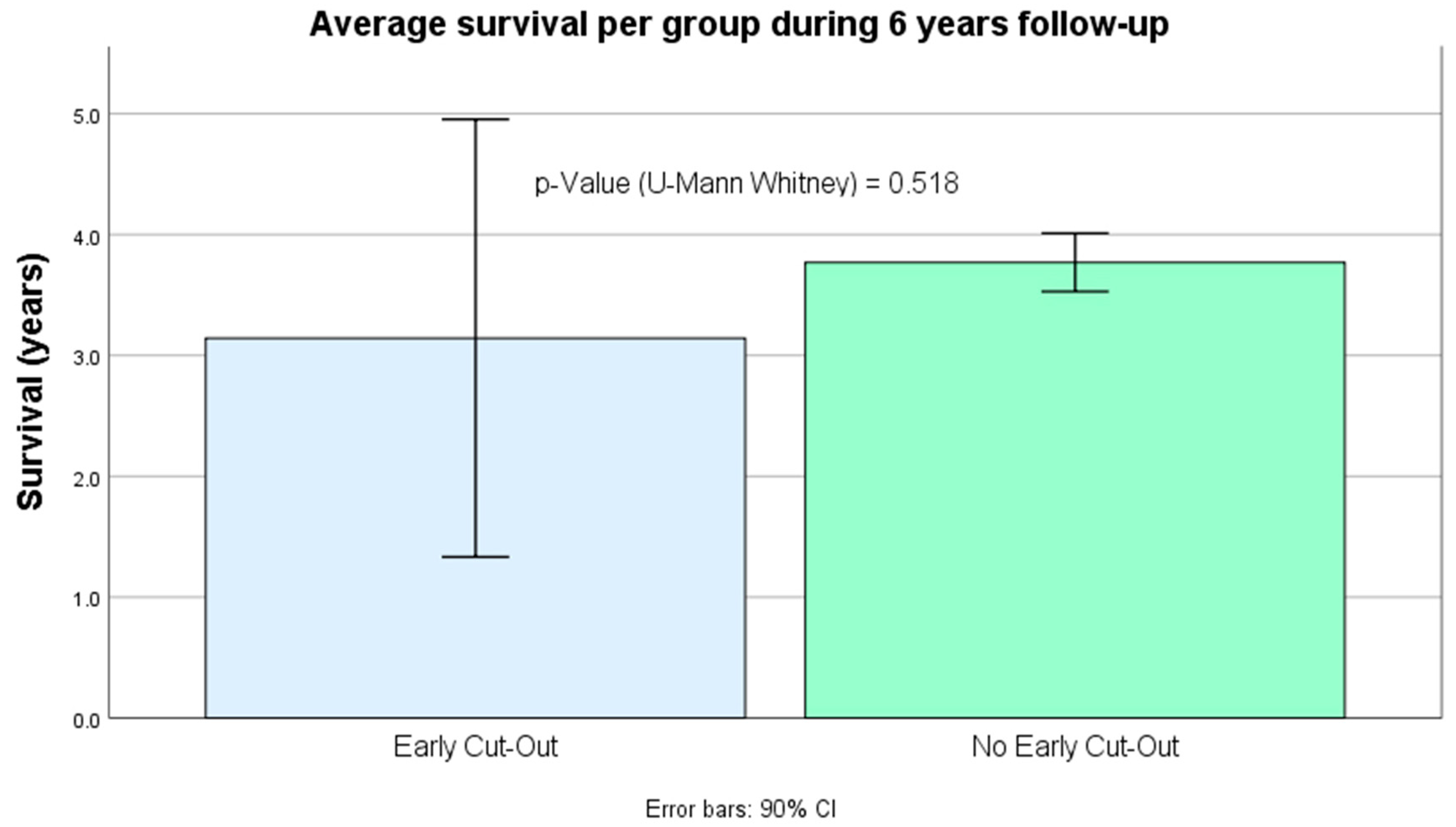
3.5. Survival (Figure 6)
3.6. Summary of Evolution of Early Cut-Out Cohort (Table 4)
| No. | Sex/(Age) | Jensen Stability | AO/OTA (1997) Stability | Massoud Stability | Immediate PWB | Detection Grade (Weeks) | IAFF (Weeks) | Consolidation/Reintervention (Weeks) | ||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Yes | No | Yes | No | 2.1 | Yes | No | ||||||
| 1 | M (88) | √ | × | √ | × | × | × | √ | Yes | III (4.7) | Yes (10.0) | No/ROM (10.7) |
| 2 | F (88) | × | √ | × | √ | × | × | √ | No | III (23) | Yes (0.71) | No/ROM (25.7) |
| 3 | F (79) | × | √ | × | √ | × | √ | × | No | II (13) | Yes (29.4) | Yes/ROM (30.0) |
| 4 | M (77) | × | √ | × | √ | × | √ | × | No | II (3.0) | No | No/PHA (3.7) |
| 5 | F (65) | √ | × | × | × | √ | √ | × | No | III (5.0) | No | No/THA (16.4) |
| 6 | F (87) | × | √ | √ | × | × | × | √ | No | I (4.3) | No | Yes/- |
| 7 | F (97) | √ | × | √ | × | × | √ | × | Yes | III (2.1) | No | No/PHA (2.86) |
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Abrahamsen, B.; van Staa, T.; Ariely, R.; Olson, M.; Cooper, C. Excess mortality following hip fracture: A systematic epidemiological review. Osteoporos. Int. 2009, 20, 1633–1650. [Google Scholar] [CrossRef] [PubMed]
- Bretherton, C.P.; Parker, M.J. Femoral Medialization, Fixation Failures, and Functional Outcome in Trochanteric Hip Fractures Treated With Either a Sliding Hip Screw or an Intramedullary Nail From Within a Randomized Trial. J. Orthop. Trauma 2016, 30, 642–646. [Google Scholar] [CrossRef] [PubMed]
- Docquier, P.L.; Manche, E.; Autrique, J.C.; Geulette, B. Complications associated with gamma nailing. A review of 439 cases. Acta Orthop. Belg. 2002, 68, 251–257. [Google Scholar] [PubMed]
- Aguado-Maestro, I.; Escudero-Marcos, R.; García-García, J.M.; Alonso-García, N.; Pérez-Bermejo, D.D.; Aguado-Hernández, H.J.; Nistal-Rodríguez, J.; García-Alonso, M. Results and complications of pertrochanteric hip fractures using an intramedullary nail with a helical blade (proximal femoral nail antirotation) in 200 patients. Rev. Esp. Cirugía Ortop. Traumatol. 2013, 57, 201–207. [Google Scholar] [CrossRef]
- Morvan, A.; Boddaert, J.; Cohen-Bittan, J.; Picard, H.; Pascal-Mousselard, H.; Khiami, F. Risk factors for cut-out after internal fixation of trochanteric fractures in elderly subjects. Orthop. Traumatol.-Surg. Res. 2018, 104, 1183–1187. [Google Scholar] [CrossRef]
- Parker, M.J. Cutting-out of the dynamic hip screw related to its position. J. Bone Jt. Surg. Br. 1992, 74, 625. [Google Scholar] [CrossRef]
- Baumgaertner, M.R.; Curtin, S.L.; Lindskog, D.M.; Keggi, J.M. The value of the tip-apex distance in predicting failure of fixation of peritrochanteric fractures of the hip. J. Bone Jt. Surg. Am. 1995, 77, 1058–1064. [Google Scholar] [CrossRef]
- Bojan, A.J.; Beimel, C.; Speitling, A.; Taglang, G.; Ekholm, C.; Jönsson, A. 3066 consecutive Gamma Nails. 12 years experience at a single centre. BMC Musculoskelet. Disord. 2010, 11, 133. [Google Scholar] [CrossRef]
- Flint, J.H.; Sanchez-Navarro, C.F.; Buckwalter, J.A.; Marsh, J.L. Intrapelvic migration of a gamma nail lag screw: Review of the possible mechanisms. Orthopedics 2010, 33, 1–5. [Google Scholar] [CrossRef]
- Frei, H.C.; Hotz, T.; Cadosch, D.; Rudin, M.; Käch, K. Central head perforation, or “cut through,” caused by the helical blade of the proximal femoral nail antirotation. J. Orthop. Trauma 2012, 26, e102–e107. [Google Scholar] [CrossRef]
- Bojan, A.J.; Beimel, C.; Taglang, G.; Collin, D.; Ekholm, C.; Jönsson, A. Critical factors in cut-out complication after Gamma Nail treatment of proximal femoral fractures. BMC Musculoskelet. Disord. 2013, 14, 1. [Google Scholar] [CrossRef] [PubMed]
- Ehlinger, M.; Favreau, H.; Eichler, D.; Adam, P.; Bonnomet, F. Early mechanical complications following fixation of proximal femur fractures: From prevention to treatment. Orthop. Traumatol. Surg. Res. 2020, 106, S79–S87. [Google Scholar] [CrossRef] [PubMed]
- Bovbjerg, P.E.; Larsen, M.S.; Madsen, C.F.; Schønnemann, J. Failure of short versus long cephalomedullary nail after intertrochanteric fractures. J. Orthop. 2020, 18, 209–212. [Google Scholar] [CrossRef] [PubMed]
- Ibrahim, I.; Appleton, P.T.; Wixted, J.J.; DeAngelis, J.P.; Rodriguez, E.K. Implant cut-out following cephalomedullary nailing of intertrochanteric femur fractures: Are helical blades to blame? Injury 2019, 50, 926–930. [Google Scholar] [CrossRef] [PubMed]
- Aktselis, I.; Papadimas, D.; Fragkomichalos, E.; Deligeorgis, A.; Kokoroghiannis, C. Intramedullary nailing of trochanteric fractures--operative technical tips. Injury 2012, 43, 961–965. [Google Scholar] [CrossRef]
- Mereddy, P.; Kamath, S.; Ramakrishnan, M.; Malik, H.; Donnachie, N. The AO/ASIF proximal femoral nail antirotation (PFNA): A new design for the treatment of unstable proximal femoral fractures. Injury 2009, 40, 428–432. [Google Scholar] [CrossRef]
- Li, S.; Chang, S.M.; Niu, W.X.; Ma, H. Comparison of tip apex distance and cut-out complications between helical blades and lag screws in intertrochanteric fractures among the elderly: A meta-analysis. J. Orthop. Sci. 2015, 20, 1062–1069. [Google Scholar] [CrossRef]
- Cleveland, M.; Bosworth, D.M.; Thompson, F.R.; Wilson, H.J., Jr.; Ishizuka, T. A ten-year analysis of intertrochanteric fractures of the femur. J. Bone Jt. Surg. Am. 1959, 41-A, 1399–1408. [Google Scholar] [CrossRef]
- Turgut, A.; Kalenderer, O.; Karapinar, L.; Kumbaraci, M.; Akkan, H.A.; Agus, H. Which factor is most important for occurrence of cutout complications in patients treated with proximal femoral nail antirotation? Retrospective analysis of 298 patients. Arch. Orthop. Trauma Surg. 2016, 136, 623–630. [Google Scholar] [CrossRef]
- Lopes-Coutinho, L.; Dias-Carvalho, A.; Esteves, N.; Sousa, R. Traditional distance “tip-apex” vs. new calcar referenced “tip-apex”—which one is the best peritrochanteric osteosynthesis failure predictor? Injury 2020, 51, 674–677. [Google Scholar] [CrossRef]
- Parker, M.; Raval, P.; Gjertsen, J.E. Nail or plate fixation for A3 trochanteric hip fractures: A systematic review of randomised controlled trials. Inj.-Int. J. Care Inj. 2018, 49, 1319–1323. [Google Scholar] [CrossRef] [PubMed]
- Khan, W.; Williams, R.; Hopwood, S.; Agarwal, S. Combined Intracapsular And Extracapsular Neck Of Femur Fractures Case Series, Literature Review And Management Recommendations. Open Orthop. J. 2017, 11, 600–608. [Google Scholar] [CrossRef] [PubMed]
- Ikuta, Y.; Nagata, Y.; Iwasaki, Y. Preoperative radiographic features of trochanteric fractures irreducible by closed reduction. Injury 2019, 50, 2014–2021. [Google Scholar] [CrossRef]
- Enocson, A.; Lapidus, L.J. The vertical hip fracture—A treatment challenge. A cohort study with an up to 9 year follow-up of 137 consecutive hips treated with sliding hip screw and antirotation screw. BMC Musculoskelet. Disord. 2012, 13, 171. [Google Scholar] [CrossRef] [PubMed]
- Hsu, C.E.; Shih, C.M.; Wang, C.C.; Huang, K.C. Lateral femoral wall thickness: A reliable predictor of post-operative lateral wall fracture in intertrochanteric fractures. Bone Jt. J. 2013, 95-B, 1134–1138. [Google Scholar] [CrossRef] [PubMed]
- Metsemakers, W.J.; Morgenstern, M.; McNally, M.A.; Moriarty, T.F.; McFadyen, I.; Scarborough, M.; Athanasou, N.A.; Ochsner, P.E.; Kuehl, R.; Raschke, M.; et al. Fracture-related infection: A consensus on definition from an international expert group. Injury 2018, 49, 505–510. [Google Scholar] [CrossRef]
- Tarazona-Santabalbina, F.J.; Ojeda-Thies, C.; Figueroa Rodríguez, J.; Cassinello-Ogea, C.; Caeiro, J.R. Orthogeriatric Management: Improvements in Outcomes during Hospital Admission Due to Hip Fracture. Int. J. Environ. Res. Public Health 2021, 18, 3049. [Google Scholar] [CrossRef]
- Jensen, J.S. Classification of trochanteric fractures. Acta Orthop. Scand. 1980, 51, 803–810. [Google Scholar] [CrossRef]
- Marsh, J.L.; Slongo, T.F.; Agel, J.; Broderick, J.S.; Creevey, W.; DeCoster, T.A.; Prokuski, L.; Sirkin, M.S.; Ziran, B.; Henley, B.; et al. Fracture and dislocation classification compendium—2007: Orthopaedic Trauma Association classification, database and outcomes committee. J. Orthop. Trauma 2007, 21, S1–S133. [Google Scholar] [CrossRef]
- Massoud, E.I. Fixation of basicervical and related fractures. Int. Orthop. 2010, 34, 577–582. [Google Scholar] [CrossRef] [Green Version]
- Fogagnolo, F.; Kfuri, M.; Paccola, C.A. Intramedullary fixation of pertrochanteric hip fractures with the short AO-ASIF proximal femoral nail. Arch. Orthop. Trauma Surg. 2004, 124, 31–37. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.R.; Kim, S.T.; Yoon, M.G.; Moon, M.S.; Heo, J.H. The stability score of the intramedullary nailed intertrochanteric fractures: Stability of nailed fracture and postoperative patient mobilization. Clin. Orthop. Surg. 2013, 5, 10–18. [Google Scholar] [CrossRef] [PubMed]
- Hernández-Pascual, C.; Santos-Sánchez, J.; García-González, J.M.; Silva-Viamonte, C.F.; Pablos-Hernández, C.; Ramos-Pascua, L.; Mirón-Canelo, J.A. Long-term outcomes of distal locking in extracapsular fractures treated with trochanteric Gamma3 nails. J. Orthop. Traumatol. 2021, 22, 48. [Google Scholar] [CrossRef]
- Mahoney, F.; Barthel, D. Functional Evaluation: The Barhel index. Md. State Med. J. 1965, 14, 61–65. [Google Scholar] [PubMed]
- Charlson, M.E.; Pompei, P.; Ales, K.L.; MacKenzie, C.R. A new method of classifying prognostic comorbidity in longitudinal studies: Development and validation. J. Chronic Dis. 1987, 40, 373–383. [Google Scholar] [CrossRef]
- Martínez de la Iglesia, J.; Dueñas Herrero, R.; Onís Vilches, M.C.; Aguado Taberné, C.; Albert Colomer, C.; Luque Luque, R. Spanish language adaptation and validation of the Pfeiffer’s questionnaire (SPMSQ) to detect cognitive deterioration in people over 65 years of age. Med. Clin. 2001, 117, 129–134. [Google Scholar] [CrossRef]
- Nuti, R.; Brandi, M.L.; Isaia, G.; Tarantino, U.; Silvestri, S.; Adami, S. New perspectives on the definition and the management of severe osteoporosis: The patient with two or more fragility fractures. J. Endocrinol. Investig. 2009, 32, 783–788. [Google Scholar] [CrossRef]
- Fitz-Henry, J. The ASA classification and peri-operative risk. Ann. R. Coll. Surg. Engl. 2011, 93, 185–187. [Google Scholar] [CrossRef]
- Horner, N.S.; Samuelsson, K.; Solyom, J.; Bjørgul, K.; Ayeni, O.R.; Östman, B. Implant-Related Complications and Mortality After Use of Short or Long Gamma Nail for Intertrochanteric and Subtrochanteric Fractures: A Prospective Study with Minimum 13-Year Follow-up. JB JS Open Access 2017, 2, e0026. [Google Scholar] [CrossRef]
- Chehade, M.J.; Carbone, T.; Awward, D.; Taylor, A.; Wildenauer, C.; Ramasamy, B.; McGee, M. Influence of Fracture Stability on Early Patient Mortality and Reoperation After Pertrochanteric and Intertrochanteric Hip Fractures. J. Orthop. Trauma 2015, 29, 538–543. [Google Scholar] [CrossRef]
- Bonnaire, F.; Weber, A.; Bösl, O.; Eckhardt, C.; Schwieger, K.; Linke, B. “Cutting out” in pertrochanteric fractures—problem of osteoporosis? Unfallchirurg 2007, 110, 425–432. [Google Scholar] [CrossRef] [PubMed]
- Lorich, D.G.; Geller, D.S.; Nielson, J.H. Osteoporotic pertrochanteric hip fractures: Management and current controversies. Instr. Course Lect. 2004, 53, 441–454. [Google Scholar] [CrossRef] [PubMed]
- Elliot-Gibson, V.; Bogoch, E.R.; Jamal, S.A.; Beaton, D.E. Practice patterns in the diagnosis and treatment of osteoporosis after a fragility fracture: A systematic review. Osteoporos. Int. 2004, 15, 767–778. [Google Scholar] [CrossRef] [PubMed]
- Lizano-Díez, X.; Keel, M.J.B.; Siebenrock, K.A.; Tey, M.; Bastian, J.D. Rehabilitation protocols in unstable trochanteric fractures treated with cephalomedullary nails in elderly: Current practices and outcome. Eur. J. Trauma Emerg. Surg. 2020, 46, 1267–1280. [Google Scholar] [CrossRef]
- Li, J.; Zhang, L.; Zhang, H.; Yin, P.; Lei, M.; Wang, G.; Wang, S.; Tang, P. Effect of reduction quality on post-operative outcomes in 31-A2 intertrochanteric fractures following intramedullary fixation: A retrospective study based on computerised tomography findings. Int. Orthop. 2019, 43, 1951–1959. [Google Scholar] [CrossRef]
- De Bruijn, K.; den Hartog, D.; Tuinebreijer, W.; Roukema, G. Reliability of predictors for screw cutout in intertrochanteric hip fractures. J. Bone Jt. Surg. Am. 2012, 94, 1266–1272. [Google Scholar] [CrossRef]
- Murena, L.; Moretti, A.; Meo, F.; Saggioro, E.; Barbati, G.; Ratti, C.; Canton, G. Predictors of cut-out after cephalomedullary nail fixation of pertrochanteric fractures: A retrospective study of 813 patients. Arch. Orthop. Trauma Surg. 2018, 138, 351–359. [Google Scholar] [CrossRef]
- Haidukewych, G.J. Intertrochanteric fractures: Ten tips to improve results. J. Bone Jt. Surg. Am. 2009, 91, 712–719. [Google Scholar]
- Meinberg, E.G.; Agel, J.; Roberts, C.S.; Karam, M.D.; Kellam, J.F. Fracture and Dislocation Classification Compendium-2018. J. Orthop. Trauma 2018, 32 (Suppl. S1), S1–S170. [Google Scholar] [CrossRef]




| Variable | Early Cut-Out | No early Cut-Out | p |
|---|---|---|---|
| Number of patients | 7 | 197 | |
| TAD | 25.54 (SD 8.81) | 22.67 (SD 6.44) | 0.395 c |
| Baumgaertner–Fogagnolo | |||
| Poor | 1 (14.3%) | 7 (3.6%) | 0.072 a |
| Moderate | 4 (57.1%) | 64 (32.5%) | |
| Good | 2 (28.6%) | 126 (64.0%) | |
| Infection (IAFF) * | 0.002 a, * | ||
| -No | 4 (57.2%) | 191 (96.9%) | |
| -Yes | 3 (42.8%) | 6 (3.1%) | |
| Immediate post-Sx. PWB | 0.451 a | ||
| -No | 5 (71.4%) | 103 (52.8%) | |
| -Yes | 2 (28.6%) | 94 (47.2%) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hernández-Pascual, C.; Santos-Sánchez, J.Á.; Hernández-Rodríguez, J.; Silva-Viamonte, C.F.; Pablos-Hernández, C.; Villanueva-Martínez, M.; Mirón-Canelo, J.A. New Prognostic Factors in Operated Extracapsular Hip Fractures: Infection and GammaTScore. Int. J. Environ. Res. Public Health 2022, 19, 11680. https://doi.org/10.3390/ijerph191811680
Hernández-Pascual C, Santos-Sánchez JÁ, Hernández-Rodríguez J, Silva-Viamonte CF, Pablos-Hernández C, Villanueva-Martínez M, Mirón-Canelo JA. New Prognostic Factors in Operated Extracapsular Hip Fractures: Infection and GammaTScore. International Journal of Environmental Research and Public Health. 2022; 19(18):11680. https://doi.org/10.3390/ijerph191811680
Chicago/Turabian StyleHernández-Pascual, Carlos, José Ángel Santos-Sánchez, Jorge Hernández-Rodríguez, Carlos Fernando Silva-Viamonte, Carmen Pablos-Hernández, Manuel Villanueva-Martínez, and José Antonio Mirón-Canelo. 2022. "New Prognostic Factors in Operated Extracapsular Hip Fractures: Infection and GammaTScore" International Journal of Environmental Research and Public Health 19, no. 18: 11680. https://doi.org/10.3390/ijerph191811680