

Differences in Adolescent’s Cardiometabolic Health: A Comparison Regarding Guided Team and Endurance Sports


Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
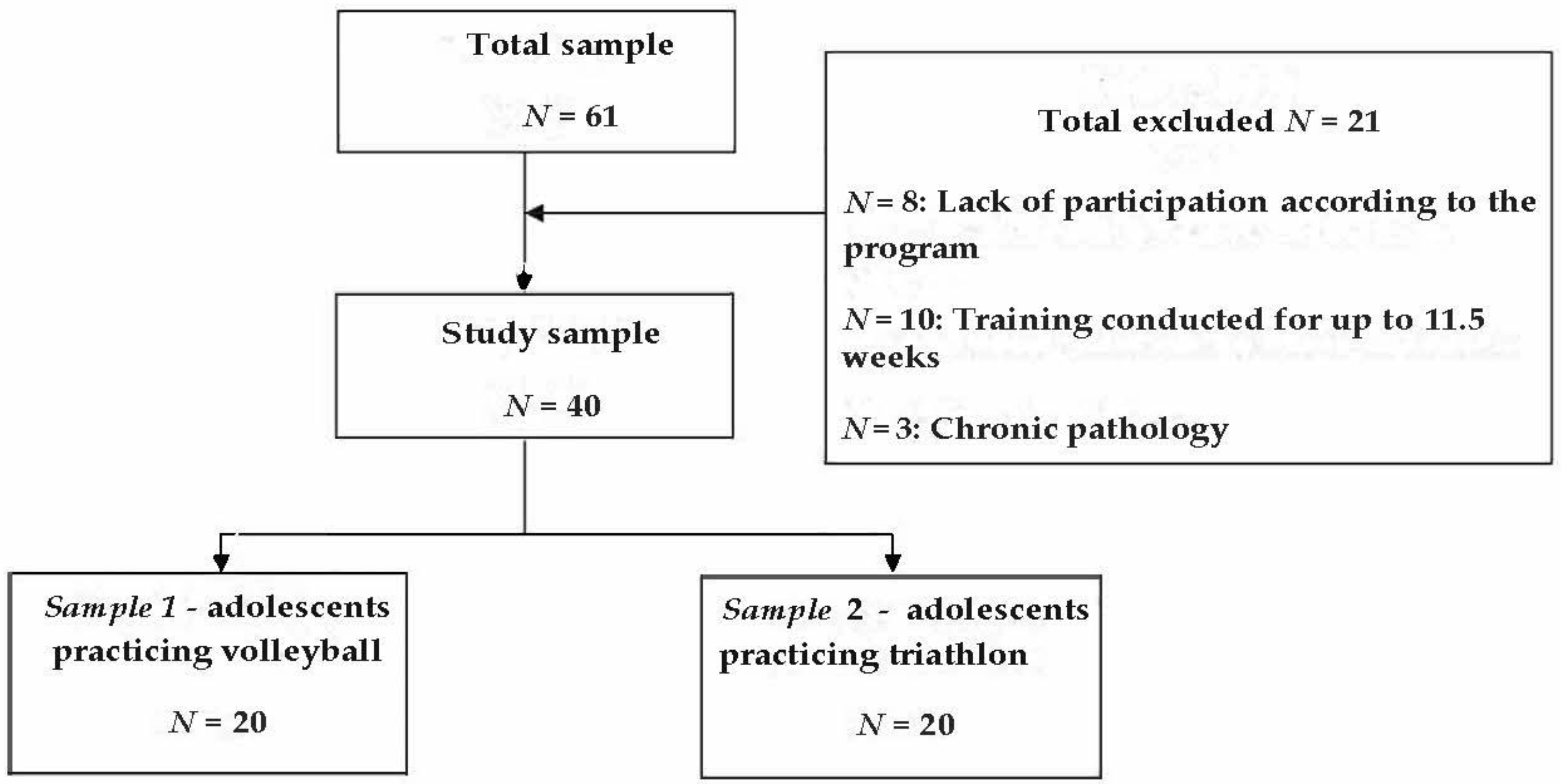
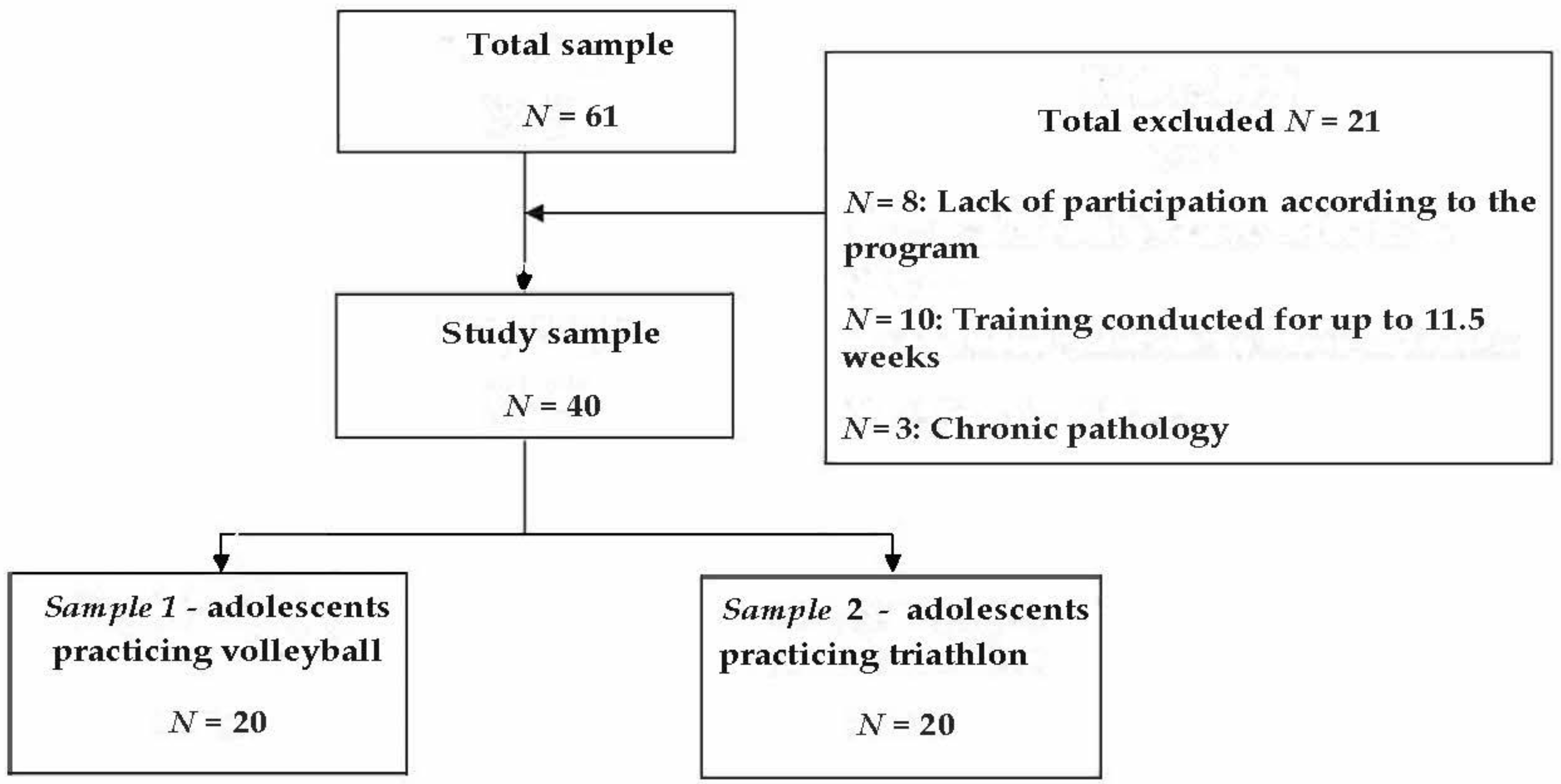
2.2. Study Participants
Training Regime
2.3. Applied Tests
2.3.1. Anthropometric Analysis
2.3.2. Basal Metabolic Rate Measurement through Indirect Calorimetry Method
2.3.3. Measuring VO2peak during an Incremental Running Test
2.4. Statistical Evaluation
3. Results
3.1. Comparative Analysis of the BMR Measurements in Both Sample 1 and Sample 2
3.2. The Results of the Incremental Test in Both Sample 1 and Sample 2
4. Discussion
4.1. Age-Related Norms
Anthropometric Results
4.2. Incremental Exercise Test Results—A Comparison with the Literature Report
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Wang, Y.; Ashokan, K. Physical Exercise: An Overview of Benefits From Psychological Level to Genetics and Beyond. Front. Physiol. 2021, 12, 731858. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.; Lee, E.-J.; Kim, H.-O. Effects of a Physical Exercise Program on Physiological, Psychological, and Physical Function of Older Adults in Rural Areas. Int. J. Environ. Res. Public Health 2021, 18, 8487. [Google Scholar] [CrossRef] [PubMed]
- Falk, B.; Dotan, R. Measurement and Interpretation of Maximal Aerobic Power in Children. Pediatr. Exerc. Sci. 2019, 31, 144–151. [Google Scholar] [CrossRef]
- Leclair, E.; Borel, B.; Thevenet, D.; Baquet, G.; Mucci, P.; Berthoin, S. Assessment of Child-Specific Aerobic Fitness and Anaerobic Capacity by the Use of the Power-Time Relationships Constants. Pediatr. Exerc. Sci. 2010, 22, 454–466. [Google Scholar] [CrossRef] [PubMed]
- Clemente, F.M.; Ardigò, L.P.; Song, W.; Lenoir, M.E.M.; Rodrigues, L.P.; Sigmundsson, H. Editorial: Children’s Exercise Physiology. Front. Physiol. 2020, 11, 269. [Google Scholar] [CrossRef] [PubMed]
- Aira, T.; Salin, K.; Vasankari, T.; Korpelainen, R.; Parkkari, J.; Heinonen, O.J.; Savonen, K.; Alanko, L.; Kannas, L.; Selänne, H.; et al. Training Volume and Intensity of Physical Activity among Young Athletes: The Health Promoting Sports Club (HPSC) Study. Adv. Phys. Educ. 2019, 9, 270–287. [Google Scholar] [CrossRef] [Green Version]
- Bassett, D.R.; Howley, E.T. Limiting Factors for Maximum Oxygen Uptake and Determinants of Endurance Performance. Med. Sci. Sports Exerc. 2000, 32, 70–84. [Google Scholar] [CrossRef] [PubMed]
- Avloniti, A.; Chatzinikolaou, A.; Deli, C.K.; Vlachopoulos, D.; Gracia-Marco, L.; Leontsini, D.; Draganidis, D.; Jamurtas, A.Z.; Mastorakos, G.; Fatouros, I.G. Exercise-Induced Oxidative Stress Responses in the Pediatric Population. Antioxidants 2017, 6, 6. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brazendale, K.; Beets, M.W.; Armstrong, B.; Weaver, R.G.; Hunt, E.T.; Pate, R.R.; Brusseau, T.A.; Bohnert, A.M.; Olds, T. Children’s Moderate-to-Vigorous Physical Activity on Weekdays versus Weekend Days: A Multi-Country Analysis. Int. J. Behav. Nutr. Phys. Act. 2021, 18, 28. [Google Scholar] [CrossRef]
- Samuel, R.D.; Zavdy, O.; Levav, M.; Reuveny, R.; Katz, U.; Dubnov-Raz, G. The Effects of Maximal Intensity Exercise on Cognitive Performance in Children. J. Hum. Kinet. 2017, 57, 85–96. [Google Scholar] [CrossRef]
- Green, D.J.; Hopman, M.T.E.; Padilla, J.; Laughlin, M.H.; Thijssen, D.H.J. Vascular Adaptation to Exercise in Humans: Role of Hemodynamic Stimuli. Physiol. Rev. 2017, 97, 495–528. [Google Scholar] [CrossRef] [PubMed]
- Xiao, W.; Soh, K.G.; Wazir, M.R.W.N.; Talib, O.; Bai, X.; Bu, T.; Sun, H.; Popovic, S.; Masanovic, B.; Gardasevic, J. Effect of Functional Training on Physical Fitness Among Athletes: A Systematic Review. Front. Physiol. 2021, 12, 738878. [Google Scholar] [CrossRef] [PubMed]
- Siramaneerat, I.; Chaowilai, C. Impact of Specialized Physical Training Programs on Physical Fitness in Athletes. J. Hum. Sport Exerc. 2020, 17, 435–445. [Google Scholar] [CrossRef]
- Miko, H.-C.; Zillmann, N.; Ring-Dimitriou, S.; Dorner, T.E.; Titze, S.; Bauer, R. Auswirkungen von Bewegung Auf Die Gesundheit. Gesundh. Bundesverb. Arzte Offentlichen Gesundh. Ger. 2020, 82 (Suppl. 3), S184–S195. [Google Scholar] [CrossRef] [PubMed]
- Ruegsegger, G.N.; Booth, F.W. Health Benefits of Exercise. Cold Spring Harb. Perspect. Med. 2018, 8, a029694. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Solsona, R.; Berthelot, H.; Borrani, F.; Sanchez, A.M.J. Mechanical, Cardiorespiratory, and Muscular Oxygenation Responses to Sprint Interval Exercises Under Different Hypoxic Conditions in Healthy Moderately Trained Men. Front. Physiol. 2021, 12, 773950. [Google Scholar] [CrossRef] [PubMed]
- Matos, N.; Winsley, R.J. Trainability of Young Athletes and Overtraining. J. Sports Sci. Med. 2007, 6, 353–367. [Google Scholar]
- Mangine, G.T.; Hoffman, J.R.; Gonzalez, A.M.; Townsend, J.R.; Wells, A.J.; Jajtner, A.R.; Beyer, K.S.; Boone, C.H.; Miramonti, A.A.; Wang, R.; et al. The Effect of Training Volume and Intensity on Improvements in Muscular Strength and Size in Resistance-Trained Men. Physiol. Rep. 2015, 3, e12472. [Google Scholar] [CrossRef] [Green Version]
- Teixeira-Coelho, F.; Fonseca, C.G.; Barbosa, N.H.S.; Vaz, F.F.; Cordeiro, L.M.D.S.; Coimbra, C.C.; Pires, W.; Soares, D.D.; Wanner, S.P. Effects of Manipulating the Duration and Intensity of Aerobic Training Sessions on the Physical Performance of Rats. PLoS ONE 2017, 12, e0183763. [Google Scholar] [CrossRef] [Green Version]
- Zeng, N.; Ayyub, M.; Sun, H.; Wen, X.; Xiang, P.; Gao, Z. Effects of Physical Activity on Motor Skills and Cognitive Development in Early Childhood: A Systematic Review. BioMed Res. Int. 2017, 2017, 2760716. [Google Scholar] [CrossRef] [Green Version]
- Schmutz, E.A.; Leeger-Aschmann, C.S.; Kakebeeke, T.H.; Zysset, A.E.; Messerli-Bürgy, N.; Stülb, K.; Arhab, A.; Meyer, A.H.; Munsch, S.; Puder, J.J.; et al. Motor Competence and Physical Activity in Early Childhood: Stability and Relationship. Front. Public Health 2020, 8, 39. [Google Scholar] [CrossRef] [PubMed]
- Versic, S.; Idrizovic, K.; Ahmeti, G.B.; Sekulic, D.; Majeric, M. Differential Effects of Resistance- and Endurance-Based Exercise Programs on Muscular Fitness, Body Composition, and Cardiovascular Variables in Young Adult Women: Contextualizing the Efficacy of Self-Selected Exercise Modalities. Medicina 2021, 57, 654. [Google Scholar] [CrossRef] [PubMed]
- Venckunas, T.; Mieziene, B.; Emeljanovas, A. Aerobic Capacity Is Related to Multiple Other Aspects of Physical Fitness: A Study in a Large Sample of Lithuanian Schoolchildren. Front. Physiol. 2018, 9, 1797. [Google Scholar] [CrossRef] [Green Version]
- Sahoo, K.; Sahoo, B.; Choudhury, A.K.; Sofi, N.Y.; Kumar, R.; Bhadoria, A.S. Childhood Obesity: Causes and Consequences. J. Fam. Med. Prim. Care 2015, 4, 187–192. [Google Scholar] [CrossRef]
- Wang, H.; Chen, Y.; Liu, J.; Sun, H.; Gao, W. A Follow-Up Study of Motor Skill Development and Its Determinants in Preschool Children from Middle-Income Family. BioMed Res. Int. 2020, 2020, 6639341. [Google Scholar] [CrossRef]
- Hestbaek, L.; Andersen, S.T.; Skovgaard, T.; Olesen, L.G.; Elmose, M.; Bleses, D.; Andersen, S.C.; Lauridsen, H.H. Influence of Motor Skills Training on Children’s Development Evaluated in the Motor Skills in PreSchool (MiPS) Study-DK: Study Protocol for a Randomized Controlled Trial, Nested in a Cohort Study. Trials 2017, 18, 400. [Google Scholar] [CrossRef] [Green Version]
- Walhin, J.-P.; Chen, Y.-C.; Hengist, A.; Bilzon, J.; Betts, J.A.; Thompson, D. The Effects of Different Forms of Daily Exercise on Metabolic Function Following Short-Term Overfeeding and Reduced Physical Activity in Healthy Young Men: Study Protocol for a Randomised Controlled Trial. Trials 2018, 19, 199. [Google Scholar] [CrossRef]
- Westerberg, E.; Molin, C.J.; Spörndly Nees, S.; Widenfalk, J.; Punga, A.R. The Impact of Physical Exercise on Neuromuscular Function in Myasthenia Gravis Patients. Medicine 2018, 97, e11510. [Google Scholar] [CrossRef]
- Hargreaves, M.; Spriet, L.L. Skeletal muscle energy metabolism during exercise. Nat. Metab. 2020, 2, 817–828. [Google Scholar] [CrossRef]
- Myers, A.M.; Beam, N.W.; Fakhoury, J.D. Resistance Training for Children and Adolescents. Transl. Pediatr. 2017, 6, 137–143. [Google Scholar] [CrossRef] [Green Version]
- Dahab, K.S.; McCambridge, T.M. Strength Training in Children and Adolescents. Sports Health 2009, 1, 223–226. [Google Scholar] [CrossRef] [PubMed]
- Granacher, U.; Lesinski, M.; Büsch, D.; Muehlbauer, T.; Prieske, O.; Puta, C.; Gollhofer, A.; Behm, D.G. Effects of Resistance Training in Youth Athletes on Muscular Fitness and Athletic Performance: A Conceptual Model for Long-Term Athlete Development. Front. Physiol. 2016, 7, 164. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Milenković, V.; Vitosevic, B.; Vidaković, M.; Nedin Ranković, G.; Ranković, J. Values Of Aerobic Capacity In Handball And Volleyball Players. Acta Med. Median. 2013, 52, 35–38. [Google Scholar] [CrossRef] [Green Version]
- Lidor, R.; Ziv, G. Physical and Physiological Attributes of Female Volleyball Players—A Review. J. Strength Cond. Res. 2010, 24, 1963–1973. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Güzel, Y.; Atakan, M.M.; Turnagöl, H.H.; Koşar, Ş.N. Association of Physical Activity Level with Body Composition in 12–14 Years Old Children: A Pilot Study. Sport Hekim. Derg. 2022, 57, 060–066. [Google Scholar] [CrossRef]
- Hottenrott, K.; Ludyga, S.; Schulze, S. Effects of High Intensity Training and Continuous Endurance Training on Aerobic Capacity and Body Composition in Recreationally Active Runners. J. Sports Sci. Med. 2012, 11, 483–488. [Google Scholar]
- Birat, A.; Bourdier, P.; Piponnier, E.; Blazevich, A.J.; Maciejewski, H.; Duché, P.; Ratel, S. Metabolic and Fatigue Profiles Are Comparable Between Prepubertal Children and Well-Trained Adult Endurance Athletes. Front. Physiol. 2018, 9, 387. [Google Scholar] [CrossRef] [Green Version]
- Shete, A.N.; Bute, S.S.; Deshmukh, P.R. A Study of VO2 Max and Body Fat Percentage in Female Athletes. J. Clin. Diagn. Res. JCDR 2014, 8, BC01–BC03. [Google Scholar] [CrossRef]
- Lleshi, E. Performance of Female Volleyball Players in VO2max. Eur. J. Soc. Sci. Educ. Res. 2021, 8, 118–121. [Google Scholar] [CrossRef]
- Salazar-Martínez, E.; de Matos, T.R.; Arrans, P.; Santalla, A.; Orellana, J.N. Ventilatory Efficiency Response Is Unaffected by Fitness Level, Ergometer Type, Age or Body Mass Index in Male Athletes. Biol. Sport 2018, 35, 393–398. [Google Scholar] [CrossRef]
- Datta, D.; Normandin, E.; ZuWallack, R. Cardiopulmonary Exercise Testing in the Assessment of Exertional Dyspnea. Ann. Thorac. Med. 2015, 10, 77–86. [Google Scholar] [CrossRef] [PubMed]
- Cristi-Montero, C. Considerations Regarding the Use of Metabolic Equivalents When Prescribing Exercise for Health: Preventive Medicine in Practice. Physician Sportsmed. 2016, 44, 109–111. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Parameter | Sample 1 | CV, % | Sample 2 | CV, % | p | Mann–Whitney U |
|---|---|---|---|---|---|---|
| Age | 16 | 10,21 | 15.5 | 12,5 | 0.5199 | 50 |
| Body weight, kg | 61,5 | 19,75 | 53,55 | 16,1 | 0.0007 | 96 |
| Body height, cm | 177 | 4,47 | 160 | 4,68 | 0.0001 | 30 |
| Fat mass, % | 20 | 16.33 | 18.55 | 34.79 | 0.5334 | 140 |
| Parameter | Sample 1 Median (Min to Max) | Sample 2 Median (Min to Max) | p | Mann–Whitney U |
|---|---|---|---|---|
| VO2, mL/min | 0.245 (0.23 to 0.29) | 0.22 (0.20 to 0.29) | 0.0087 | 115,5 |
| VCO2, mL/min | 0.23 (0.2 to 0.27) | 0.20 (0.17 to 0.26) | 0.0008 | 66 |
| RQ | 0.89 (0.83 to 0.94) | 0.86 (0.81 to 0.89) | 0.0058 | 86 |
| Fat, g/day | 62 (28 to 92) | 72.5 (52 to 113) | 0.183 | 134 |
| CHO, g/day | 277 (173 to 362) | 199.5 (150 to 318) | 0.0005 | 60 |
| BMR | 1767 (1569 to 2089) | 1585 (1403 to 2026) | 0.0074 | 88 |
| Theoretical BMR, kcal/day | 1500 (1392 to 1800) | 1392 (1248 to 1488) | 0.0001 | 72 |
| Difference between BMR and tBMR, % | 84.35 (70.09 to 104.62) | 84 (73.45 to 94.05) | 0.197 | 126 |
| BF, rc/min | 14 (11 to 18) | 18 (11 to 20) | 0.0191 | 100 |
| VT, L | 0.547 (0.45 to 0.79) | 0.45 (0.31 to 0.65) | 0.0087 | 90 |
| VE, L/min | 8.2 (6.9 to 9.9) | 7 (6.4 to 8.7) | 0.0051 | 84 |
| BMR/BSA | 988 (910 to 1230) | 1084 (987 to 1225) | 0.0201 | 100 |
| BMR/kg_Lean | 29.4 (21.5 to 36) | 32.85 (28 to 43) | 0.0003 | 56 |
| Parameter | Sample 1 Median (Min to Max) | Sample 2 Median (Min to Max) | p | Mann–Whitney U | |
|---|---|---|---|---|---|
| AT | VO2, L/min | 1.57 (0.43 to 2.5) | 1.37 (1.04 to 1.91) | 0.190 | 184 |
| VO2, ml/min/kg | 25 (17 to 30) | 25.5 (23 to 42) | 0.172 | 182 | |
| VO2/HR, ml/b | 9.5 (7 to 14) | 9 (6 to 12) | 0.573 | 216 | |
| VE/VO2, L/min | 26.85 (21.9 to 32.7) | 25.4 (20.5 to 30.9) | 0.146 | 178 | |
| VE/VCO2, L/min | 29.65 (24.2 to 34.9) | 28.4 (23.8 to 33.6) | 0.146 | 178 | |
| VCO2, L/min | 1.51 (0.8 to 2.24) | 1.26 (0.87 to 1.65) | 0.075 | 164 | |
| RQ | 0.91 (0.87 to 0.94) | 0.91 (0.82 to 0.93) | 0.644 | 220 | |
| PetO2, mmHg | 105 (98 to 113) | 106 (101 to 113) | 0.990 | 240 | |
| PetCO2, mmHg | 34.5 (29 to 42) | 37 (31 to 40) | 0.081 | 166 | |
| EE, kcal/hour | 490.5 (127 to 749) | 402.5 (295 to 566) | 0.111 | 172 | |
| RCP | VO2, L/min | 2.33 (1.58 to 3.06) | 2.04 (1.52 to 2.41) | 0.173 | 162 |
| VO2, ml/min/kg | 35 (26 to 40) | 35.5 (31 to 55) | 0.076 | 146 | |
| VO2/HR, ml/b | 12 (8 to 16) | 11.5 (8 to 13) | 0.284 | 174 | |
| VE/VO2, L/min | 31.2 (23.5 to 34.7) | 30.4 (25.6 to 37.4) | 0.423 | 184 | |
| VE/VCO2, L/min | 31.1 (23.4 to 34.8) | 30.1 (25.5 to 38.7) | 0.143 | 158 | |
| VCO2, L/min | 2.34 (1.51 to 3.07) | 2.05 (1.52 to 2.42) | 0.189 | 164 | |
| RQ | 1 (0.96 to 1) | 1.00 (0.97 to 1.03) | 0.049 | 144 | |
| PetO2, mmHg | 111 (99 to 114) | 112 (106 to 115) | 0.581 | 194 | |
| PetCO2, mmHg | 32 (30 to 46) | 35 (29 to 37) | 0.115 | 154 | |
| EE, kcal/hour | 697 (470 to 915) | 609.5 (454 to 717) | 0.158 | 160 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Martin, Ș.A.; Martin-Hadmaș, R.M. Differences in Adolescent’s Cardiometabolic Health: A Comparison Regarding Guided Team and Endurance Sports. Int. J. Environ. Res. Public Health 2022, 19, 17070. https://doi.org/10.3390/ijerph192417070
Martin ȘA, Martin-Hadmaș RM. Differences in Adolescent’s Cardiometabolic Health: A Comparison Regarding Guided Team and Endurance Sports. International Journal of Environmental Research and Public Health. 2022; 19(24):17070. https://doi.org/10.3390/ijerph192417070
Chicago/Turabian StyleMartin, Ștefan Adrian, and Roxana Maria Martin-Hadmaș. 2022. "Differences in Adolescent’s Cardiometabolic Health: A Comparison Regarding Guided Team and Endurance Sports" International Journal of Environmental Research and Public Health 19, no. 24: 17070. https://doi.org/10.3390/ijerph192417070