1. Introduction
In 1999, Indonesia embarked on one of the most ambitious and rapid decentralization reforms the world had witnessed, as part of post-Suharto democratization. Along the principles of democratic decentralization, reforms granted vastly more political, administrative and fiscal autonomy to subnational governments (provinces and districts).
The outbreak of the coronavirus pandemic is testing the capability of subnational governments to handle responsibilities devolved to them in the course of decentralization reforms since 1999. The first COVID-19 cases were reported in early March 2020, among the residents of a town near Jakarta. Later in March, more cases were reported in the Maluku islands, a relatively remote archipelago in east-central Indonesia. On 13 April 2020, the President of Indonesia declared the COVID-19 pandemic as a national disaster through Presidential Decree #12 of 2020. A task force, the Task Force for the Acceleration of the Response to COVID-19, was established. The task force has developed a National Response and Mitigation Plan for COVID-19. The plan is organized in accordance with the disaster management phases of preparedness, disaster readiness/alert, disaster response, and rehabilitation and assigned responsibilities to national agencies and subnational governments, including provinces and districts. Despite all its efforts to contain the spread of the virus, the government’s response performance has been characterized as lackluster [
1]. According to the Indonesian Government, there were 1,334,634 confirmed COVID-19 cases, 155,765 active cases, and 36,166 deaths, as of 28 February 2021. The number of recovered cases was 1,142,703. When confronted with the COVID-19 pandemic, the Jokowi administration did not demonstrate effective leadership [
1]. More on the Indonesia Situation Update is available at
https://reliefweb.int/report/indonesia/situation-update-response-covid-19-indonesia-1-march-2021-enid (accessed on 15 March 2021).
The literature on disaster management suggests that the public increasingly expects better public sector leadership in response emergencies [
2]. An effective emergency response requires deploying a “whole of government” approach, including the mobilization of subnational government resources. In case of a health emergency, local health officials are typically well-positioned to identify vulnerable communities due to their proximity to people. They have familiarity with local conditions to design appropriate response actions. In addition, they are often well-placed to adopt rapidly changing circumstances during large-scale, complex emergencies, like pandemics [
3]. Furthermore, they can put in place prevention mechanisms as well as resiliency plans that can reduce the impact of an emergency on local populations [
4]. In that context, the resilience of local governments in case of a sudden nationwide shock, such as the COVID-19 pandemic, is an important determinant of the success of pandemic response [
5].
Emerging literature suggests that intergovernmental coordination mechanisms and subnational government capacity are two important ingredients of a successful “whole of government” response against coronavirus pandemic [
6]. In this commentary article, we examine the whole of government response to the coronavirus pandemic in Indonesia. Our focus in the analysis is provincial governments. We use correlation coefficient methodology to analyze the relationship between COVID-19 case fatality and death rates and provincial capacity in Indonesia.
2. Big Bang Decentralization
Without much preparation, Indonesia embarked on a far-reaching decentralization program in 1999. The first democratic elections in 1999 marked the beginning of the decentralization process. The newly elected national parliament approved the decentralization laws in May 1999—the law 22/1999 on regional government and 25/1999 on intergovernmental fiscal relations—which devolved significant authority and resources to subnational governments. The changes in the fiscal framework resulted in a new system of intergovernmental fiscal relations, which led to a substantial increase of central government transfers to subnational governments [
7].
Despite its ambitious nature, decentralization process went well, without any major hick ups [
8]. In the new decentralized government structure after 1999, there are two lower tiers of government: provinces (the second tier) and districts (the third tier).
The initial decentralization period of 1999–2004 is sometimes labeled as the period of big bang devolution of responsibilities and resources to subnational levels. In this period, legislations (laws 22/1999 and 25/1999) granted significant fiscal autonomy to district governments and devolved service delivery responsibilities, such as health, education, and infrastructure, to district governments. However, provincial governments did not receive a significant share of newly devolved responsibility. According to Buehler [
9], the motivation for shifting power to districts, bypassing provinces, was the national elites’ concerns for secession of empowered provinces. Instead, they were responsible for carrying out tasks assigned by the central government.
Over time, decentralization laws underwent two major revisions in 2004 and 2014, shifting the focus of decentralization to the provincial level. In the period between 2004 and 2014, the roles and responsibilities among provincial and district governments were rebalanced favoring provinces [
10]. The revisions in decentralization legislations brought changes in the distribution of government functions among central and subnational governments by strengthening the role of provincial governments. Provinces received supervisory powers (instead of powers of coordination) and a stronger role as representatives of the central government, particularly in the area of planning and budgeting as well as public service delivery.
In the last period, starting 2014, the emphasis has shifted to improving the quality and quantity of public services [
10]. A new law, the Law 23/2014, has transferred certain responsibilities from districts to provinces, including forest management, coastal management, mining, and senior high school education. The law has shifted authority of forest resources management from district to province level, including community empowerment programs in Lampung Province such as Village Forest (Hutan Desa) and Community Forest (Hutan Kemasyarakatan or HKm). As far as the service responsibilities are concerned, the new law has brought two important changes. First, expenditure assignment is divided into three types of responsibilities: The absolute central government affairs, the concurrent affairs, and the general affairs. The absolute central government affairs are the responsibility of the central government, including foreign affairs, justice, religion, defense, security, and monetary and fiscal policy. The concurrent affairs, of which the responsibilities are divided between the three levels of government, consist of two types: (a) obligatory affairs and (b) non-obligatory affairs. The obligatory affairs include education, health, general construction and spatial management, public housing, social affairs, and local security. Finally, the general affairs are the sole responsibility of the central government, relating to issues of national importance.
Second, the law has significantly strengthened the role of governor in the system by assigning the responsibility of monitoring and evaluation of the performance of district/municipality. The law empowers governors with the authority to abolish district regulations and approve district budgets as well as proposing the removal of the head of a district in certain circumstances. Furthermore, the law stipulates that governors have ceremonial responsibilities, like inaugurating the heads of districts and acting as mediator between conflicting districts.
Overall, decentralization reforms gave greater authority, political power and financial resources to subnational governments [
11]. As a result, Indonesia is a highly decentralized unitary country with a multiple-tier system of subnational government [
12]. The regional level consists of provinces (34) with a second level of local governments (514 cities and districts). Within the cities and regions are multiple administrative sub-divisions. At the lowest level are villages (many thousands). The system is fairly decentralized, with many public functions and a large share of national resources allocated to subnational governments. Today, subnational expenditures make up about half of total public sector spending in Indonesia [
13].
3. COVID-19 Cases and Deaths in Indonesia’s Provinces
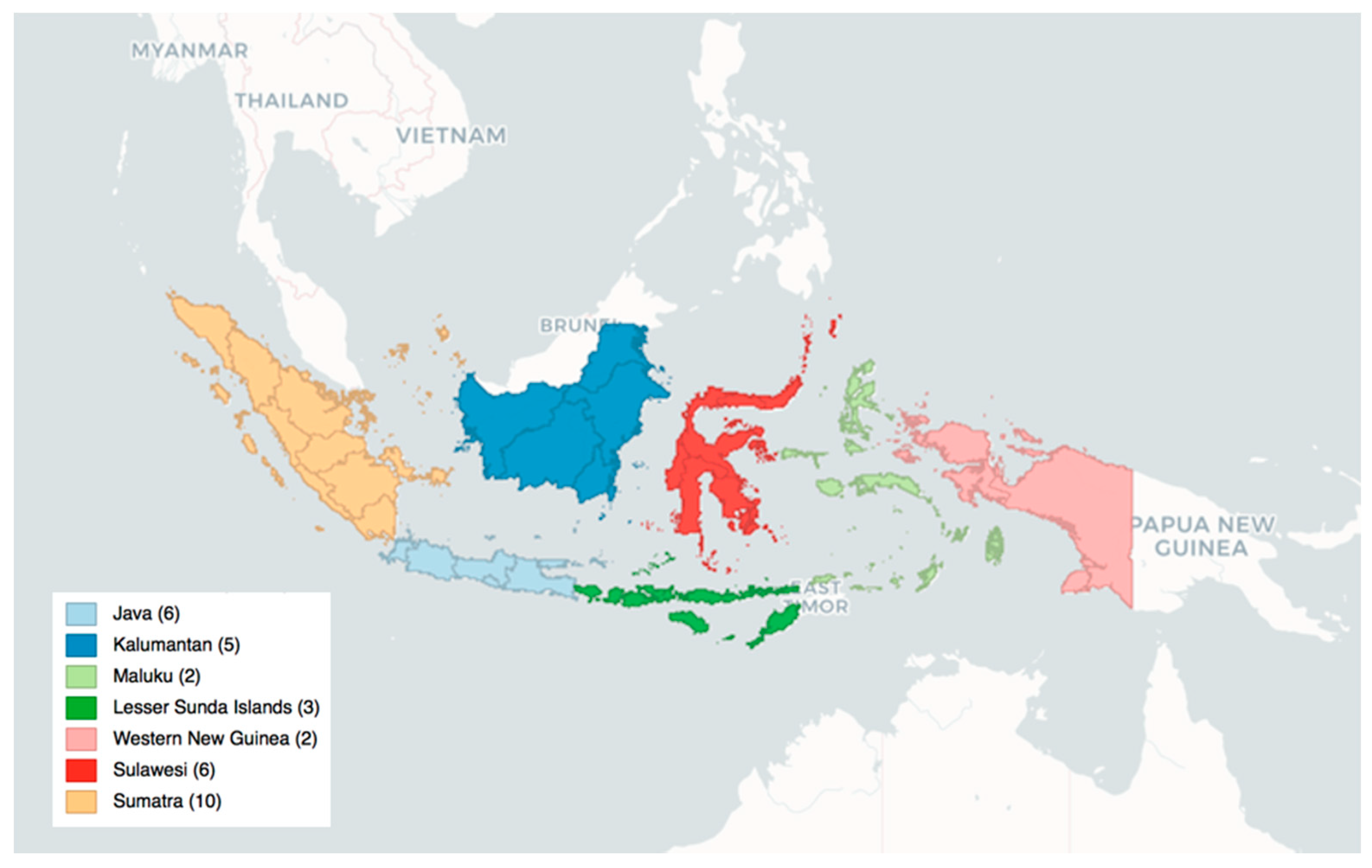
In Indonesia, there are seven regions, namely Java, Kalimantan, Maluku Islands, Lesser Sunda Islands, Western New Guinea, Sulawesi, and Sumatra.
Figure 1 shows the map of the regions in Indonesia. These seven regions are divided into 34 provinces as shown in
Table 1. Among the provinces listed above, Jakarta has the highest number of confirmed COVID-19 cases while East Nusa Tenggara ranks the lowest. However, East Java has the highest number of people who died of COVID-19 to date.
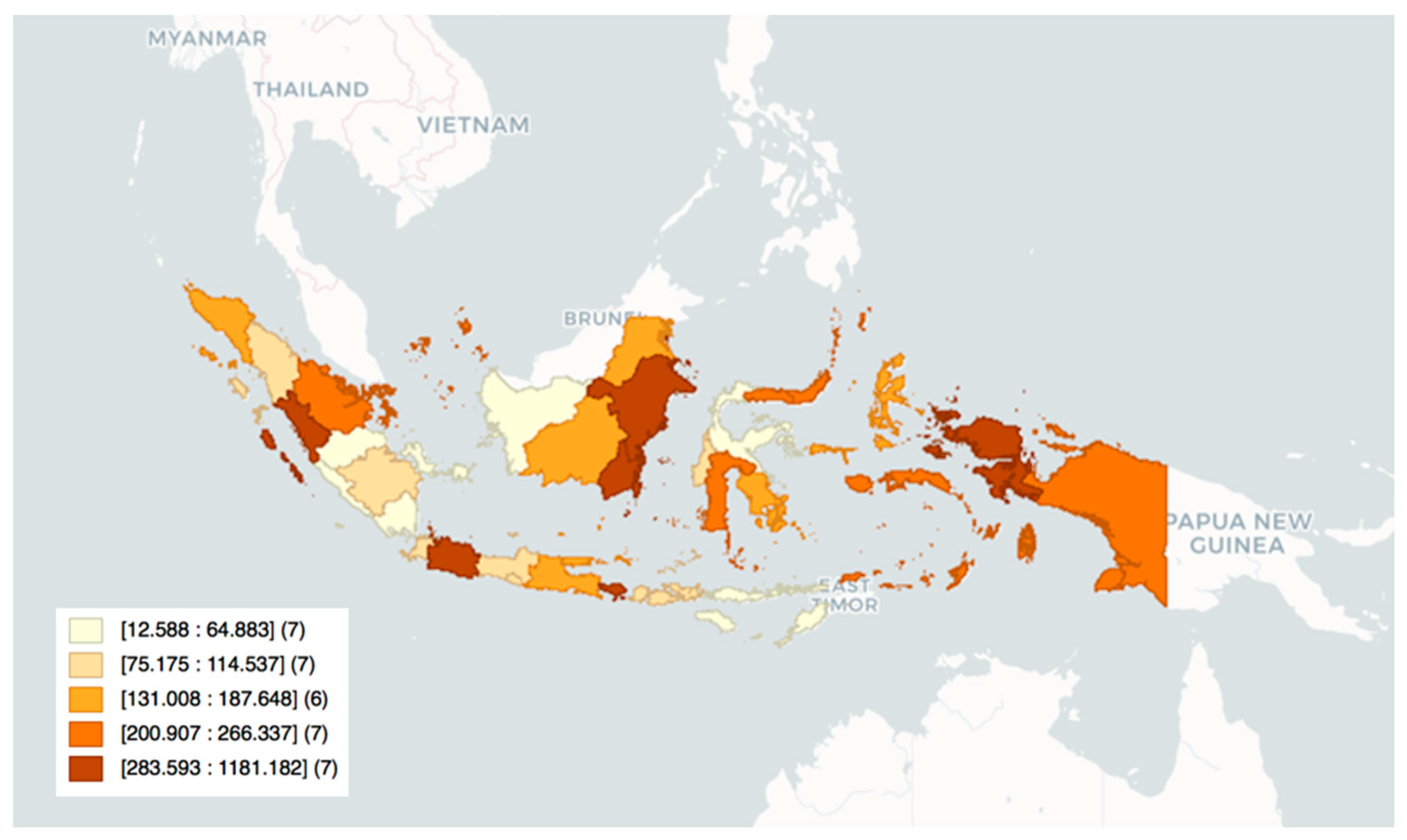
Figure 2 maps the COVID-19 cases per capita in Indonesia.
COVID-19 cases and deaths vary across the provinces.
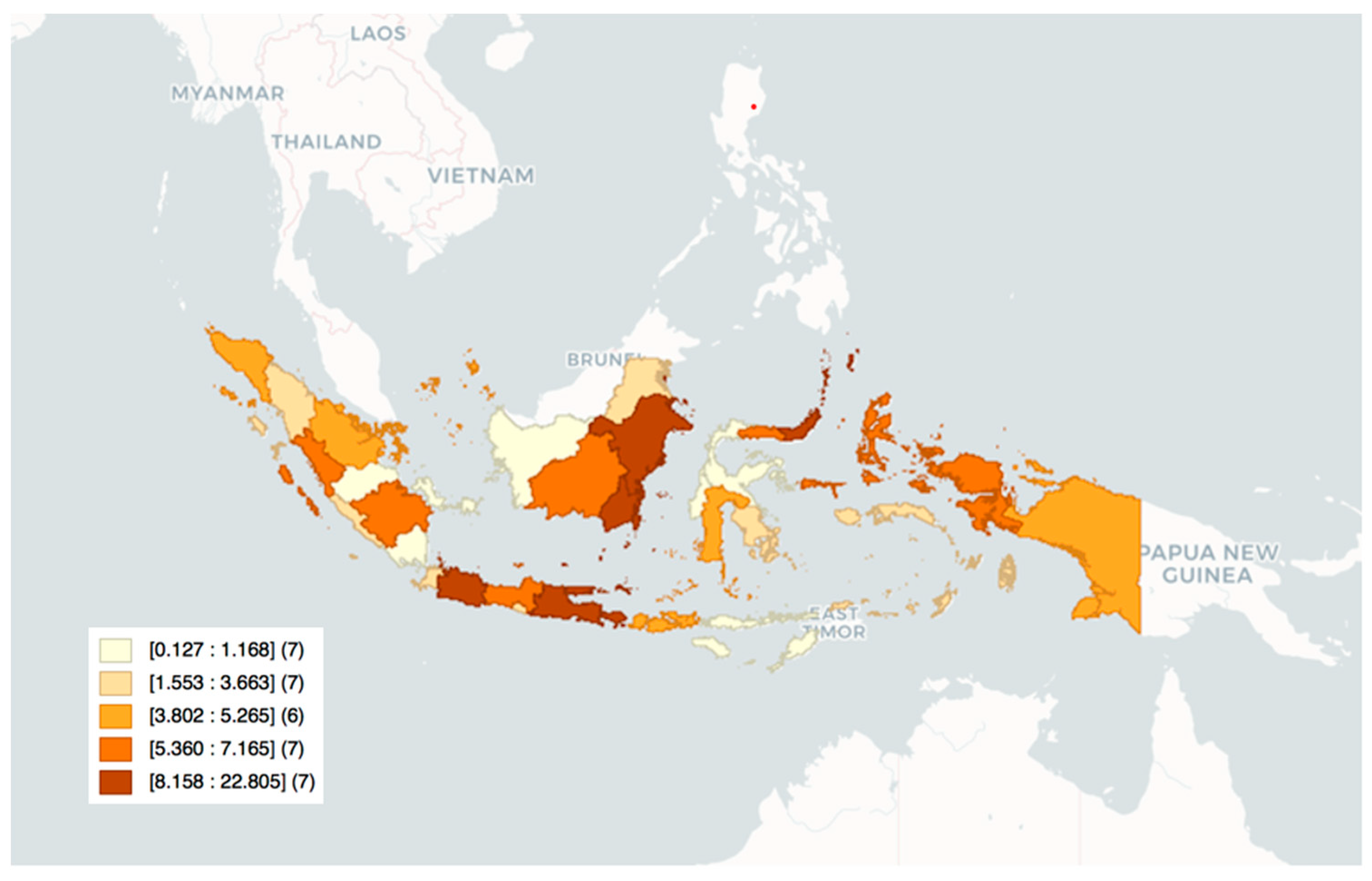
Figure 3 depicts the COVID-19 deaths per capita. Accordingly, death per capita is highest in East Kalimantan, Jakarta, East Java, and North Sulawesi, and lowest in West Kalimantan, Lampung, Jambi, and West Nusa Tenggara.
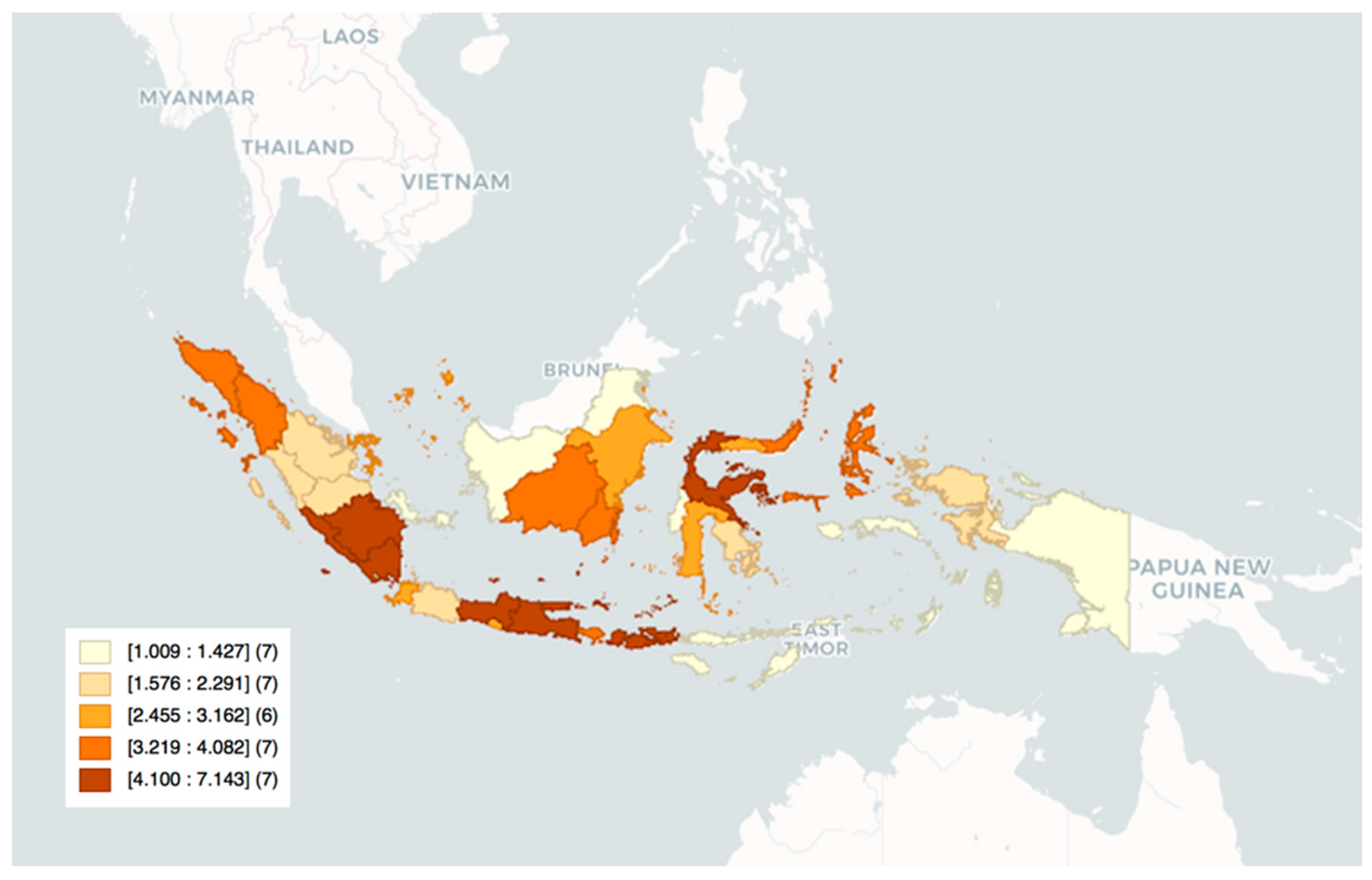
Figure 4 shows the case fatality rate across the regions. Case fatality rate is highest in South Sumatra, Lampung, Bali, and Central Sulawesi, and lowest in West Kalimantan, North Kalimantan, Papua, Bangka Belitung Islands, Maluku, and East Nusa Tenggara.
4. Pandemic Response
The impact of the coronavirus pandemic in Indonesia has been devastating, killing at least 17,000 people, leading to the loss of more than 2.6 million jobs, and a contraction of 3.5% of the GDP [
14]. Indonesia’s geographical expanse makes it difficult to fight against the coronavirus pandemic without deploying provincial governments. The geological features of the country, more than 275 million people spread across 17,500 islands with an area of 2 million km
2, presents unique logistical challenges in mounting a COVID-19 response. Due to the vast diversity of the Indonesian archipelago, effectiveness of response varies in different regions. As strengthening of provincial governments’ role in the delivery of services, including public health service, has been the focus of the government’s decentralization reforms, provinces are playing important roles in four areas in the fight against the coronavirus pandemic:
1. Increasing the level of local public health service delivery: In Indonesia, the provision of public health services is a provincial responsibility. At the beginning of the pandemic, the provincial governments established command and control structures for pandemic management as part of their Emergency Operation Centers, in order to respond to the health crisis. Provincial governments also developed contingency plans for pandemic response covering issues such as case reporting and analysis for pandemic severity, personal protective equipment stockpiling, ICU bed availability, and screening of passengers in points of entry and exit.
However, there are big inequities in the healthcare infrastructure of provinces. The majority of healthcare workers, for example, are located on the islands of Java and Sumatra. Responding to an increase in hospitalizations due to COVID-19 has put additional stress on the healthcare infrastructure of the already understaffed health facilities in smaller provinces. Therefore, some provinces have been more severely affected than others. For example, East Nusa Tenggara only had about 113 cases per million persons whereas East Kalimantan had about 12,000 cases per million persons. Provinces mostly had between 500 and 2000 cases per million [
15].
Provincial level laboratories for COVID-19 testing have been established in coordination with provincial health offices, district health offices, and
puskesmas (primary healthcare centers). However, due to the lack of clear standards and requirements, establishing the laboratories for testing took a very long time. For instance, in Aceh, it took a month to build a testing lab [
16]. Moreover, testing kits started being used without defining the clinical specifications and their accuracy has been reported to be low [
17]. By November 2020, Central Java, Jakarta, and Banten reached the testing rate recommended by the WHO while other provinces were still struggling as of December 2020 [
18].
Provinces also faced equipment shortages. At the beginning of the pandemic, most health workers were wearing raincoats instead of medical gowns [
19]. In order to address PPE shortages, around 3000 textile factories initiated the production of PPEs at the beginning of April 2020 [
19].
2. Preventing transmission and epidemiological investigations and tracking: Provincial governments play an important role in contact tracing, contact quarantine, and case isolation. Several provinces, including Jakarta, imposed lockdowns and initiated epidemiological investigations of suspected cases. After the initial cases of COVID-19 were reported in the Maluku Province, for example, the governor began limiting arrivals to the province to limit the spread of the virus. In Central Java Province, the provincial government launched the Jogo Tonggo Program (the Javanese phrase for “look after your neighbor) to encourage residents to work together in traditional ways, such as monitoring each other’s health, ensuring social distancing, and extending financial support by sharing and bartering. More on this is available from the Observatory of Public Sector Innovation (OPSI) at
https://oecd-opsi.org (accessed on 6 May 2021). In South Kalimantan, the Kampung Tangguh program helps villages to enforce public health measure by monitoring certain variables [
20]. In South Sulawesi, the innovative COVID-19 Ambassador Program is designed to lessen the burden on health facilities by providing information to local communities [
20]. A survey among university students in Jambi showed that around 60 of the students identified local government’s response as good, although about 70% of the students believed that the pandemic was at a critical stage [
21].
At the beginning of the pandemic, local governments started tracking and announcing the number of cases separately, which ended up creating a great confusion until the central government took action to be the only authority giving updates [
16]. Data transparency has been highly criticized in the sense of underreporting and lack of transparency which affected governments’ response [
17]. It has been argued that the number of people who died of COVID-19 could be three times larger than the official numbers [
22].
3. Mitigating the impact of the pandemic on other local public services: Provincial governments partnered up with international organizations to distribute water, sanitation, and hygiene (WASH) supplies for health facilities, schools, public places, and households. Specially designed hygiene kits, including items for hand hygiene, were dispatched for distribution to COVID-19 patients, high-risk populations, and vulnerable households.
4. Supporting social and economic relief activities: Provincial governments are working closely with the Ministry of Village and Disadvantaged Regions to increase coverage and benefits of unconditional cash transfers during the pandemic. Despite these acts, the public view of the economic state decreased drastically in the first nine months of 2020. In May, 65% of Indonesians reported their financial conditions had worsened compared to 2019, whereas this ratio was 21% in February [
1]. In addition, in October 2020, a new law went in effect which resulted in diminishing labor rights such as minimum wage, benefits, severance pay, etc. [
22].
5. The Relationship between COVID-19 Cases and Deaths and Provincial Governments
In this commentary, we analyzed the relationship between COVID-19 case fatality and provincial government strength. In order to proxy for governmental strength, the regional sustainable development index, public health development index, competitiveness index, and their components were utilized.
The regional sustainable development index is composed of the arithmetic and geometric averages of regional sustainable development composite index as well as the entropy method calculated by Analytical Hierarchy Process [
23].
The public health development index employs 30 public health indicators based on the Indonesian Basic Health Survey conducted in 2013 [
24]. The competitiveness index has been developed by averaging the sub-indices: quality of life and infrastructure development, macroeconomic stability, financial businesses and manpower conditions, and government and institutional setting [
25].
Subnational level Covid-19 data were gathered using the Humanitarian Data Exchange [
26] website, while data on the number of hospital units were collected from CEIC [
27].
In our analysis, Pearson’s correlation coefficient (or Pearson’s r) was used. In this manner, we first checked the linearity of the relationships between variables and outliers using scatter plots. While there were some outliers in the data, particularly regarding the COVID-19 cases, we did not remove those observations from the analysis since it is really important to examine those provinces that struggle with the severity of the pandemic. In order to check normality, Shapiro-wilk test of normality was employed. It was concluded that we failed to reject the null hypothesis of normality for all the variables except for macroeconomic stability at 10% significance level. To check the strength of correlations, we followed the guidelines by Cohen [
28]. Accordingly, if
, the correlation is small; if
, there is a moderate correlation and finally if
, the strength of the association is strong.
We present some of the key correlations in
Figure 5,
Figure 6,
Figure 7,
Figure 8 and
Figure 9 but the full list of correlations for all provinces, and separately for Java and Sumatra, can be found in the
Appendix A Table A1,
Table A2 and
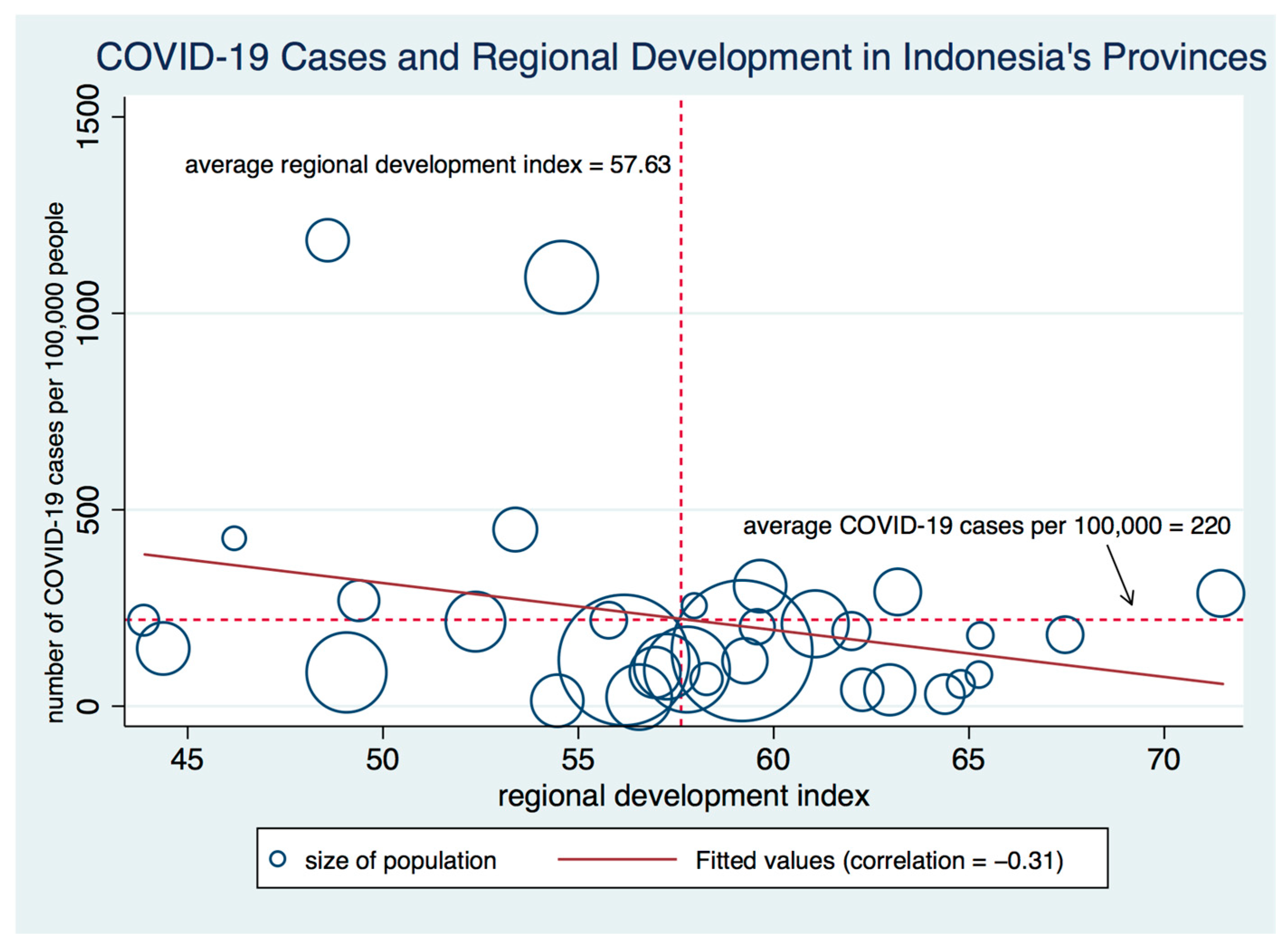
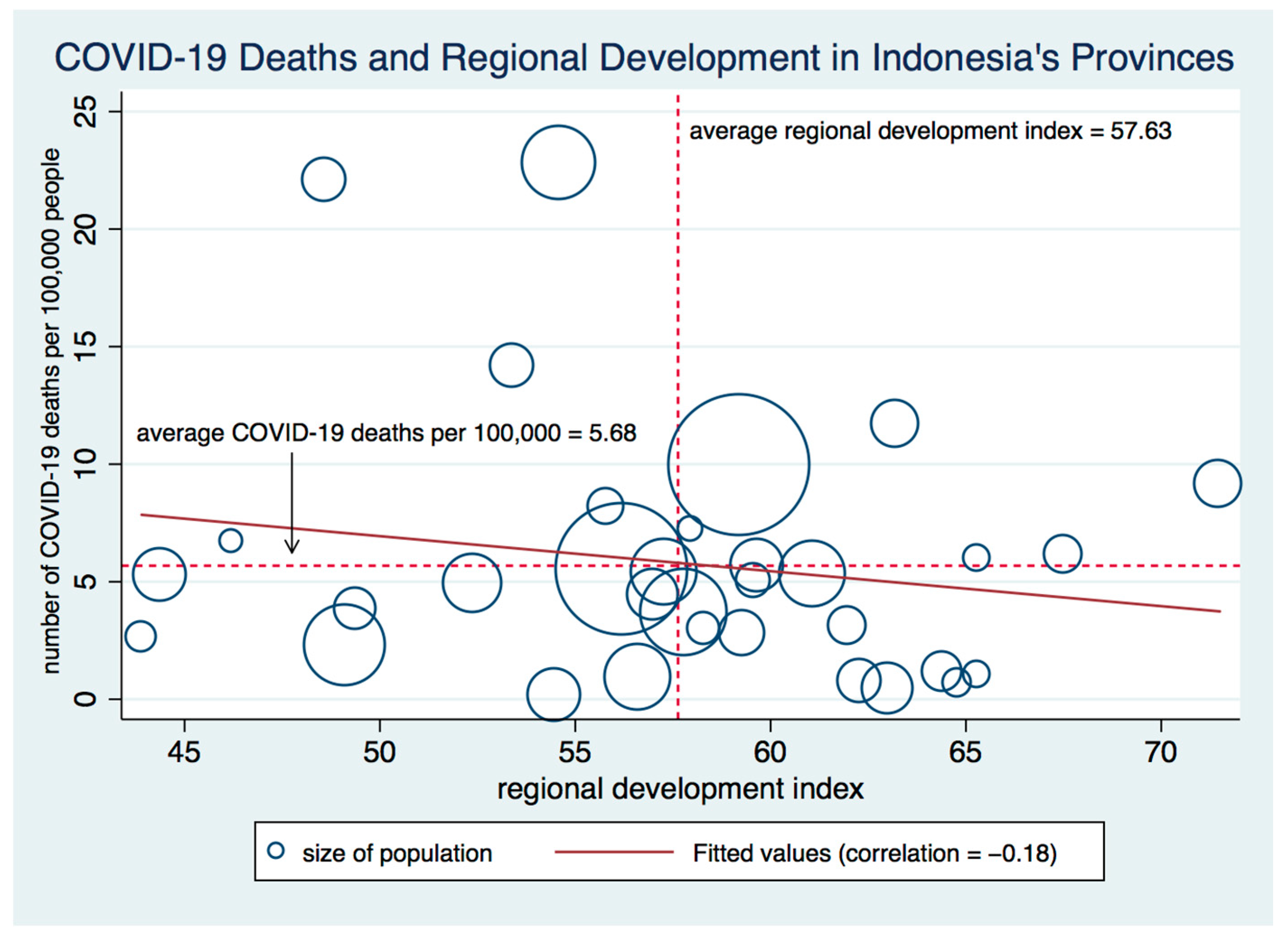
Table A3. Regional sustainable development index is one provincial development measure that shows consistently negative correlation with COVID-19 cases and deaths.
Figure 5 and
Figure 6 show the negative correlation between the regional sustainable development index and COVID-19 cases per 100,000 persons and COVID-19 deaths per 100,000 persons, respectively for the entire group of provinces. The correlation between regional sustainable development index and COVID-19 cases per 100,000 persons shown in
Figure 5 is −0.31 and statistically significant at 10% level. The correlations in
Figure 5 and
Figure 6 are relatively low due to the fact that data are for all provinces. Since Indonesia is composed of large island regions, it makes more sense to examine correlations particularly for the largest island regions. We indeed see some higher correlations for the regional sustainable development index in
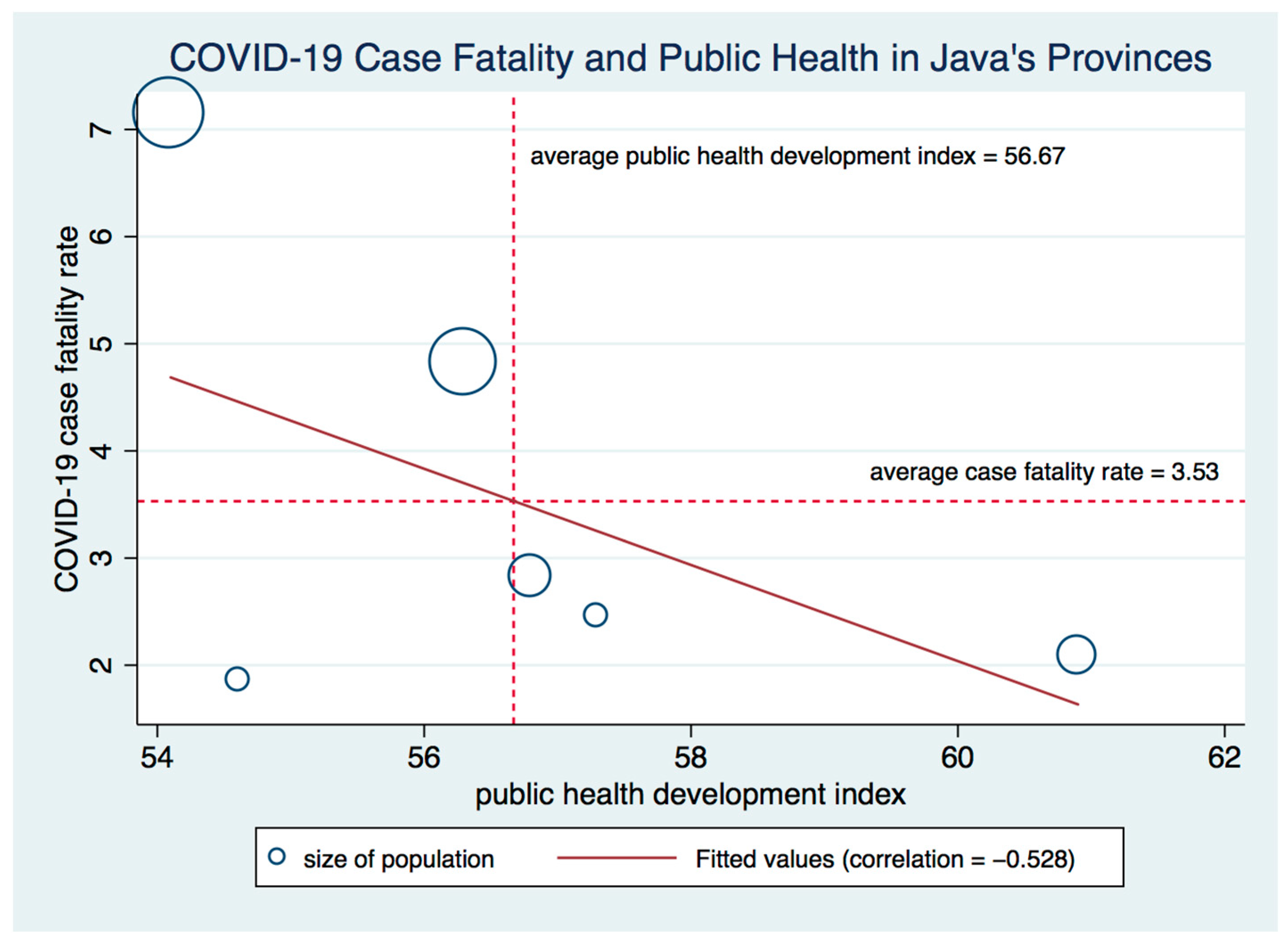
Appendix A Table A2 and
Table A3, but we see particularly high negative correlations with public health development index and some of the components of the regional competitiveness index.
Figure 7 shows a correlation of −0.528 between case fatality rate and public health development index in Java’s provinces.
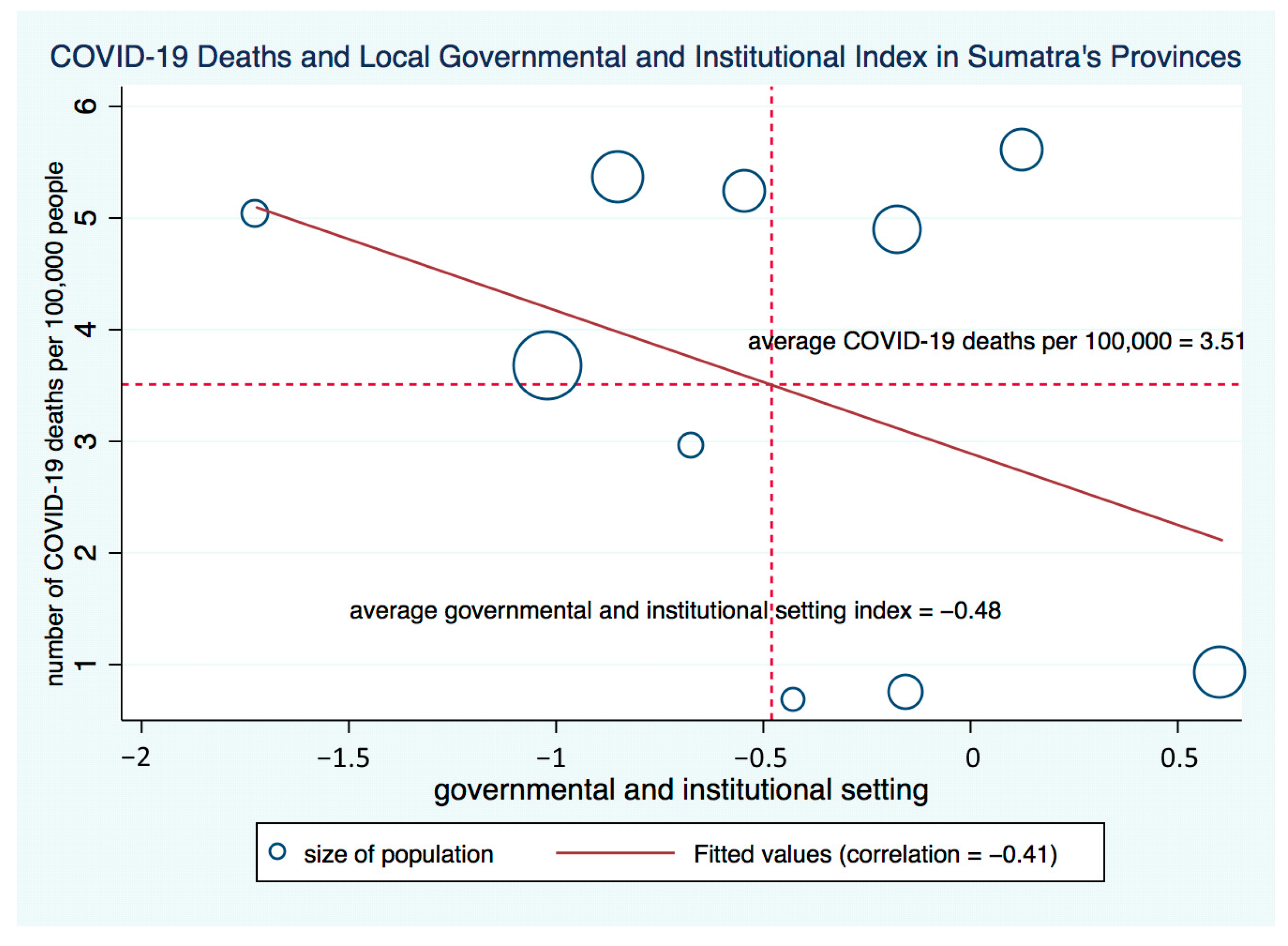
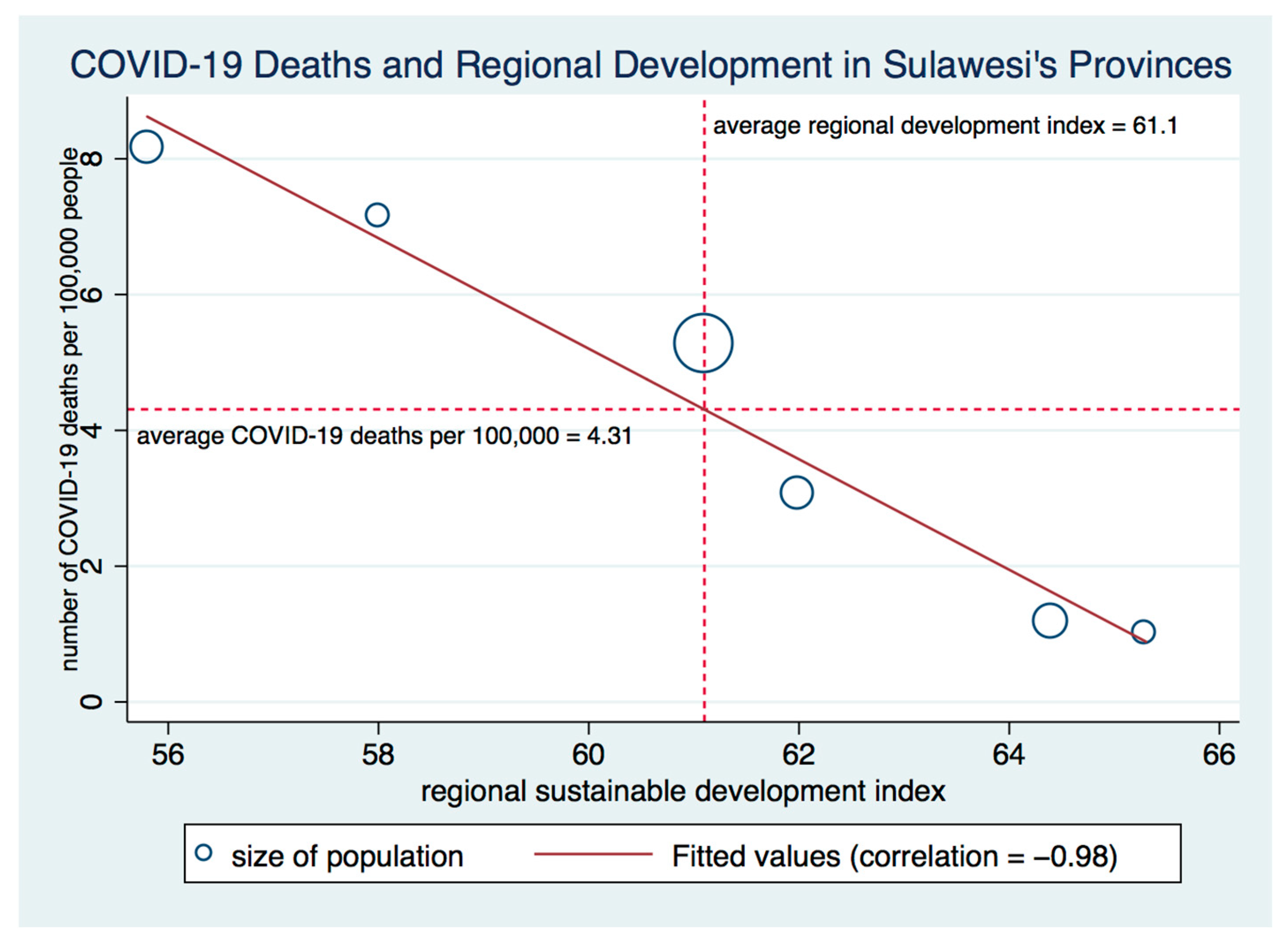
Figure 8 shows a correlation of −0.405 between COVID-19 deaths per 100,000 persons and government and institutional setting index in Sumatra’s provinces. In
Figure 9, we see almost a perfect negative correlation between the regional sustainable development index and COVID-19 deaths per 100,000 persons in Sulawesi, where the correlation coefficient is −0.98 and statistically significant at 1% level.
6. Discussion and Conclusions
The severity of the coronavirus pandemic requires mobilizing all-of government resources including local governments. As local governments are closer to people, they are well positioned to identify local vulnerabilities and design appropriate response actions.
In Indonesia, provincial governments, with support from the World Health Organization and the Ministry of Health and National Disaster Agency, prepared a provincial response plan covering the issues of coordination with the central authorities, pharmaceutical interventions, continuity of essential services, risk identification, and surveillance. They supported national efforts to fight against the pandemic through increasing the level of public health service delivery, conducting epidemiological investigation and contact tracing, mitigating the impact of the pandemic on other public services, and providing social and economic relief to citizens. However, the inherent inequities in the distribution of healthcare infrastructure and differential level of provincial capacities have a bearing on their coronavirus response.
In this commentary, we analyzed the effectiveness of provincial governments in the fight against COVID-19 pandemic indirectly. In our analysis, we have found some evidence of a negative relationship between COVID-19 case fatality and death rates and various indices of provincial strength. The correlations are higher when we examine provinces in island regions, such as Java and Sumatra, separately. Some of our findings suggest that strengthening provincial capacity is a good defense against the pandemic. Our provincial capacity variable, regional sustainable development index, is negatively correlated with COVID-19 cases and deaths. At the same time, we find considerable disparity between regions, which should draw attention to the importance of central-local government coordination in all regions. The problems with local government capacity and response to the earthquake and tsunami in 2004 was noted in previous studies [
29]. While Indonesia has gone through significant decentralization reform since 1999, the concern regarding the strength of provincial governments, particularly in terms of disaster response, has remained. We think that Indonesia should continue to invest in provincial capacity building to improve regional sustainability and resilience to natural disasters and pandemics.
We would like to note, however, that the correlations we report do not necessarily point to causal relationships and there are instances where some correlations are close to zero or positive, which also need to be investigated. More empirical research that particularly examines provinces in specific island regions, such as Java and Sumatra, is needed. It is really important to have more data that also covers micro units such as households and firms to understand the local impact of the pandemic and the effectiveness of local governments.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}








