1. Introduction
Irritable bowel syndrome (IBS) is one of the most common gastrointestinal diseases, and affects approximately 5–10% of the global population, which exerts an immense impact on the patient’s quality of life, society, and economy [
1]. The most complained symptoms include abdominal pain/discomfort and diarrhea/constipation. The pathogenesis of IBS is complex and recent studies bring the consensus that IBS mainly results from the disorder of gut–brain interactions [
2]. Furthermore, epidemiological studies suggest that genetics, diet, gut microbiota dysbiosis, gut infection, and psychological factors are all risk factors for IBS, which can exert effects on IBS via disrupting the bidirectional interactions of the gut–brain axis [
3,
4]. Considering these factors, the common therapeutics for IBS include dietary exclusion, probiotics/fecal microbiota transplant, antibiotics, psychotropic medications, and symptom-relieving drugs (e.g., antispasmodics, antidiarrheal agents, and laxative) [
5]. However, all the treatments have limited therapeutic effectiveness. Therefore, there is still an unmet need for improved understanding of the pathophysiological mechanisms of IBS to develop more effective therapeutic approaches.
Recent studies demonstrate that the diet and micronutrients play a vital role in the pathophysiology of IBS, and over 80% of IBS patients report food triggers for their complaints, such as dairy products, gluten, alcohol, and fried foods [
6,
7]. Noteworthily, dietary fibers are related to the onset of IBS symptoms, as they can exert effects on nutrients bioavailability, gut motility, stool pattern, and the gut microbiota [
8]. Specifically, the insoluble fibers, which are poorly absorbed in the gut, can provoke and exacerbate the symptoms of IBS patients, while the soluble fibers can improve stool pattern [
9,
10]. Furthermore, FODMAPs (fermentable oligosaccharides, disaccharides, monosaccharides, and polyols), which are rich in some vegetables, fruits, dairy products, and legumes, are also associated with the development and severity of symptoms in specific IBS subgroup via their fermentative and osmotic effects on the gut [
1,
11]. These findings provide some promising dietary therapies including dietary exclusion and dietary supplementation. For example, the increased intake of soluble fibers and reduced intake of insoluble fibers are suggested for IBS subjects [
8]. Moreover, a low-FODMAP diet is a recommended therapy for IBS patients by the American College of Gastroenterology. Notably, several epidemiological studies have reported the deficiency of vitamin D (Vit-D) and calcium in IBS patients [
7], which indicates that Vit-D and calcium would serve as promising targets for potential dietary therapies.
Calcium homeostasis, which plays a vital role in various cellular and biological processes, is mainly regulated by concerted action of the calciotropic hormones, such as Vit-D and parathyroid hormone (PTH) [
12]. Studies indicate that supplementation of Vit-D and calcium might help improve the symptoms of IBS patients [
13]. However, randomized controlled trials on the effects of Vit-D and calcium supplementation for IBS patients yielded contradictory results [
14,
15,
16]. Additionally, the causal relationship among Vit-D, calcium, and the risk of IBS needs to be illustrated considering the potential unmeasured confounders or reverse causality in previous observational studies.
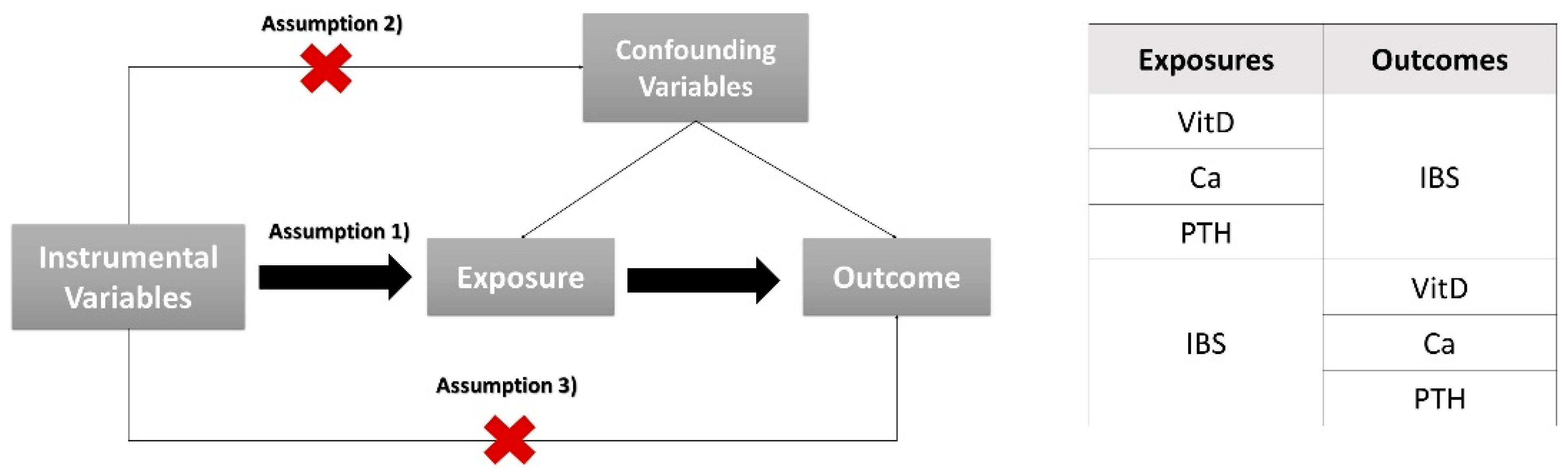
Based on Mendel’s law of inheritance, Mendelian randomization (MR) analysis can use genetic variants, namely single-nucleotide polymorphisms (SNPs), as instrumental variables (IVs) to estimate the causal effects of the predefined exposure on outcome [
17]. Since genetic variants are randomly allocated at conception and remain stable after birth, MR is less susceptible to confounding factors and reverse causation, thus simulating the randomized controlled trials in the clinic. With the existing genome-wide association study (GWAS) databank, our study is dedicated to probing the causal association between Vit-D, calcium, PTH, and IBS via a bidirectional two-sample MR study.
4. Discussion
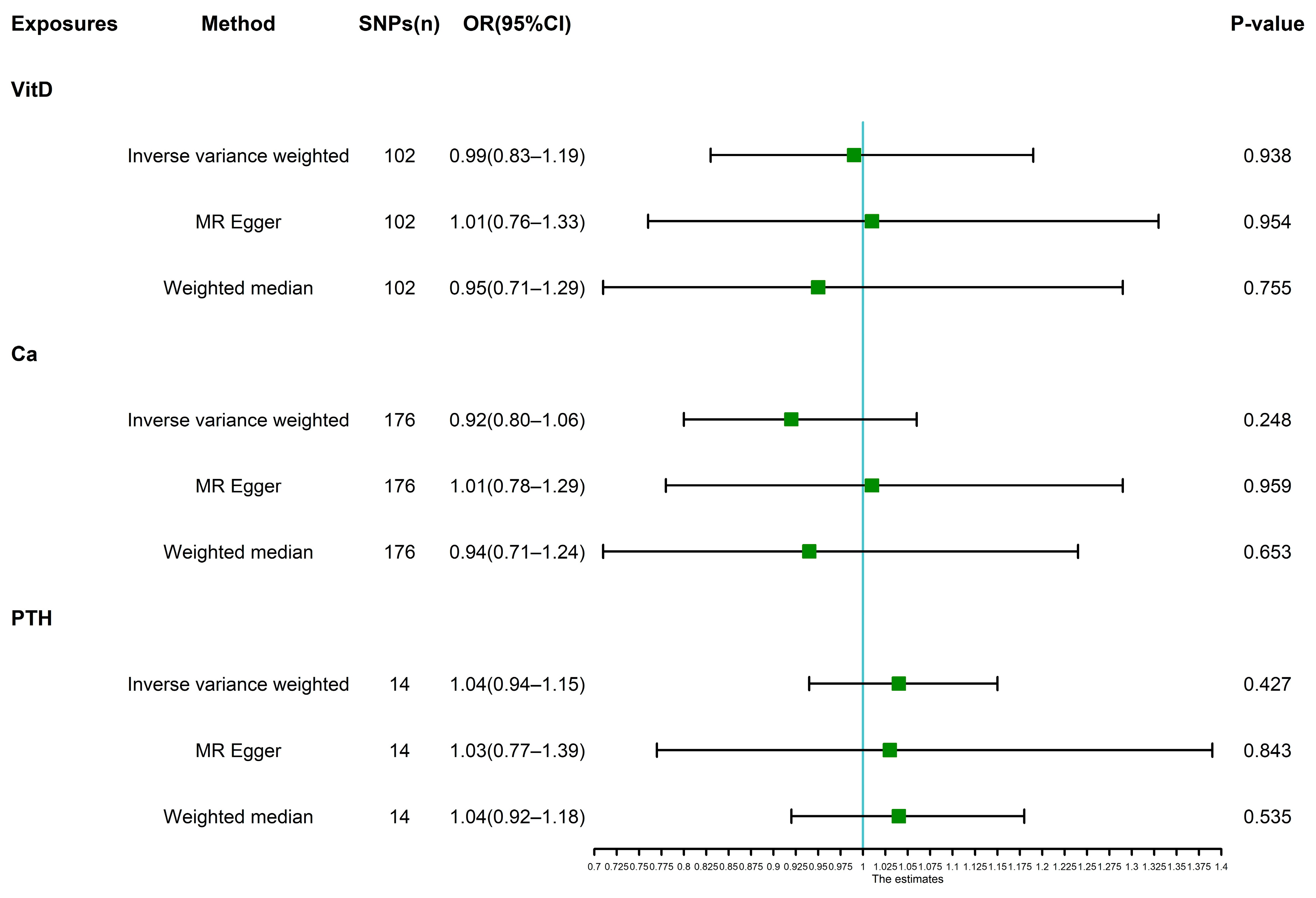
To the best of our knowledge, this is the first two-sample MR study to generally clarify the causal relationship among calcium, Vit-D, PTH, and IBS. Despite employing the latest large sample size and strong instruments, our MR results did not indicate the significantly causal associations of genetically predicted calcium, Vit-D, and PTH with the risk of IBS.
Researchers have been devoted to exploring the role of micronutrients in the pathogenesis and treatment of IBS [
27,
28]. A systematic review including 12 interventional and 14 observational studies showed that IBS patients generally had lower levels of Vit-D, vitamin B2, calcium, and iron compared with control subjects. Meanwhile, studies also found that exclusion diets were associated with deficiencies of the aforementioned micronutrients [
7]. As the major circulating form of Vit-D, 25-hydroxyvitamin D is used as indicator of Vit-D status. 25-Hydroxyvitamin D is critical to regulate calcium metabolism and a series of pathological and physiological processes in intestinal homeostasis [
29]. The various effects of Vit-D supplementation on IBS patients were reported in several randomized controlled trials and systematic reviews. Jalili et al. conducted a randomized, double-blind, placebo-controlled clinical trial to assess the impact of Vit-D supplementation on symptoms severity and quality of life (QOL) in IBS patients and found that, compared to the placebo group, Vit-D therapy could markedly improve the symptoms and QOL of IBS patients [
14]. Similarly, a systematic review and meta-analysis including four randomized, placebo-controlled trials showed that Vit-D supplementation was remarkably superior to placebo in improving the symptom severity (WMD: −84.21, 95% CI: −111.38 to −57.05, I
2 = 73.2%; WMD: −28.29, 95% CI: −49.95 to −6.62, I
2 = 46.6%, respectively) and QOL (WMD: 14.98, 95% CI: 12.06 to 17.90, I
2 = 0.0%; WMD: 6.55, 95% CI: −2.23 to 15.33, I
2 = 82.7%, respectively) of IBS patients [
30]. However, the other randomized, double-blind, placebo-controlled study by Williams et al. demonstrated that there were no improvements in the IBS symptom severity and QOL between the trial (Vit-D supplementation) and placebo groups [
15]. Moreover, a systematic review and meta-analysis based on six randomized controlled trials including 616 participants indicated that Vit-D supplementation led to no significant improvements in symptom severity and QOL of IBS subjects in contrast to placebo [
31]. Considering that Vit-D contributes to the regulation of the gut microbiome, immune system, inflammatory processes, and the intestinal mucosal barrier, the present interventional trials on IBS mainly focused on Vit-D supplementation. Few studies evaluated the effects of calcium supplementation on IBS symptom severity and QOL. In contrast to studies that reported the relationship among Vit-D, calcium, and IBS, our study suggested no causal association among Vit-D, calcium, and IBS. The contradictory findings might be explained by several factors: trial participants with different ages, races, sexes, and vitamin D statuses, sample size, intervention duration, intervention diet, and placebo effects.
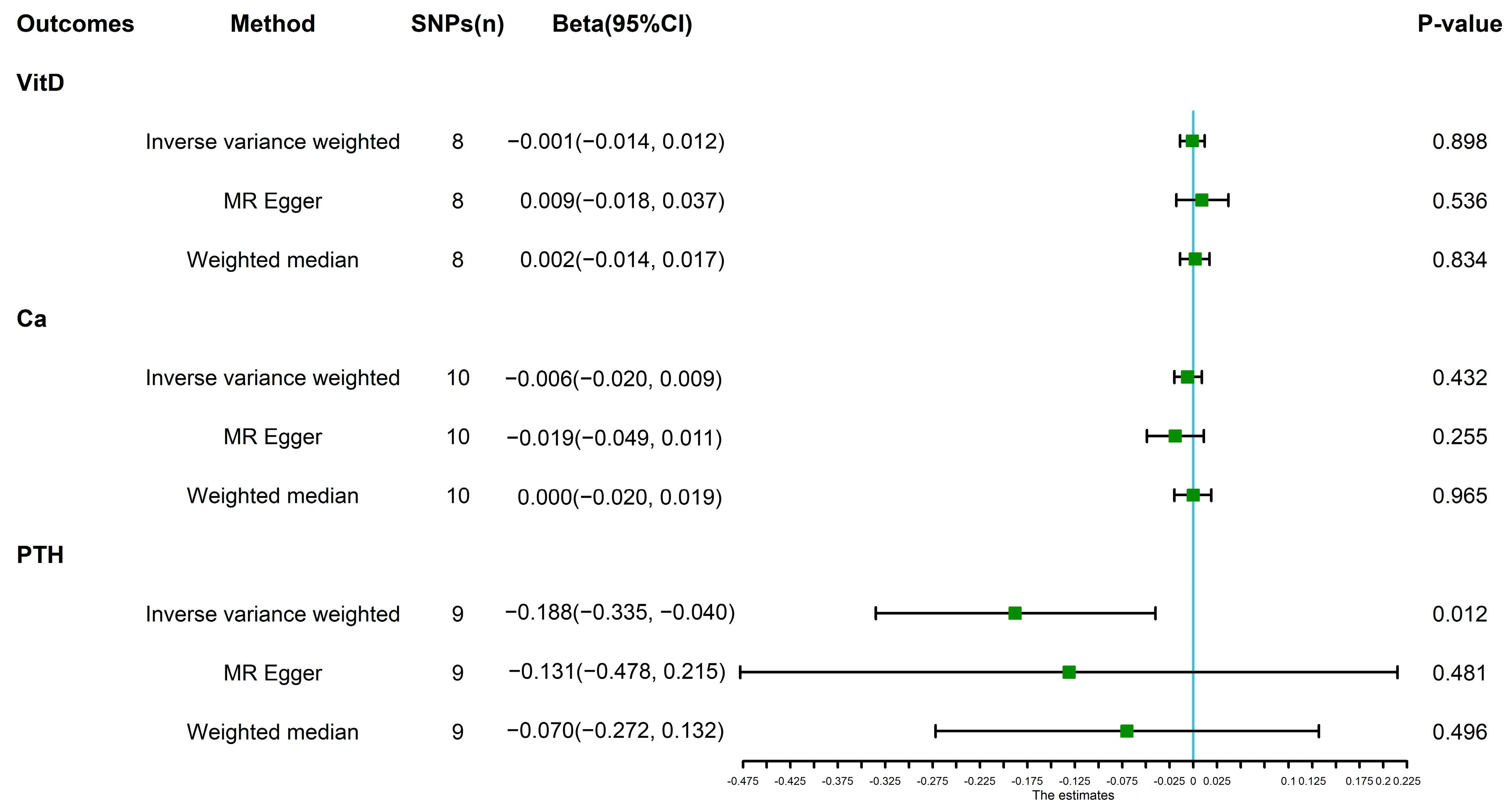
In addition, our bidirectional two-sample MR analysis identified that IBS was associated with a lower level of PTH, although there was no causal effect of PTH on IBS. The main function of PTH is to increase the concentration of serum calcium and decrease the concentration of serum phosphorus by impacting its primary target organs of bone and kidney, so as to regulate the homeostasis of calcium and phosphorus in vivo. It was noteworthy that recent studies suggested an increased risk of osteoporosis and osteoporotic fracture for IBS patients. A systematic review and meta-analysis including four cohorts and one cross-sectional study with 526,633 participants indicated that IBS patients had a remarkably higher risk of osteoporosis than the non-IBS subjects (pooled RR: 1.95, 95%CI: 1.04–3.64, I
2 = 100%) [
32]. Moreover, even though not statistically significant, IBS subjects had an increased risk of osteoporotic fracture (pooled RR: 1.58, 95%CI: 0.95–2.62, I
2 = 99%). The possible mechanisms for the association between IBS and osteoporosis comprise chronic inflammation, abnormal activation of the hypothalamic–pituitary–adrenal (HPA) axis, smoking, and malnutrition. When suffering from osteoporosis, the secretion of PTH was reduced to inhibit the activity of osteoclasts, thus impeding the progression of osteoporosis, which might be the plausible explanation for the relationship between IBS and reduced level of PTH.
To our knowledge, this is the first study to elucidate the causal correlation among calcium, Vit-D, PTH, and IBS from the perspective of genetic variants using a bidirectional two-sample MR approach. This method could greatly circumvent the possible impacts of reverse causation and residual confounding factors, such as incomplete adjustment for confounders, the absence of high-quality evidence, and relatively small sample sizes of trials. Additionally, we performed several sensitivity analyses to strengthen the robustness of our results.
However, there are some limitations associated with this study. Firstly, the study mainly analyzed the European participants enrolled in the GWAS biobank; hence, the results could not precisely reflect the fact of patients from other regions and races. Secondly, we failed to accomplish the sex-specific, IBS subtype-specific, age-specific, and race-specific analyses due to a lack of data. Lastly, MR analysis possesses some inherent shortcomings, making it impossible to eliminate the effects of confounding factors and horizontal pleiotropy.
In conclusion, the present study provides no evidence that calcium, Vit-D, and PTH are causally associated with IBS, and it suggests a lower concentration of PTH in IBS subjects. Our findings may reduce possible expenses and research interests in elucidating the effects of calcium, Vit-D, and PTH on IBS. More importantly, further research is needed to investigate the causal relationship between micronutrients and IBS.


{kind=link}
{kind=link}
{kind=link}


