
Dietary Habits, Physical Activity and Body Mass Index in Transgender and Gender Diverse Adults in Italy: A Voluntary Sampling Observational Study

 , , , ,
, , , ,  , , , , , , add
Show full author list
, , , , , , add
Show full author list
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants and Procedure
2.2. Health-Related Behaviours
2.2.1. Fruit and Vegetables Consumption
2.2.2. Fish and Red Meat Consumption
2.2.3. Milk and Yogurt Intake
2.2.4. Physical Activity
2.3. Statistical Analysis
3. Results
3.1. Fruit and Vegetables Consumption
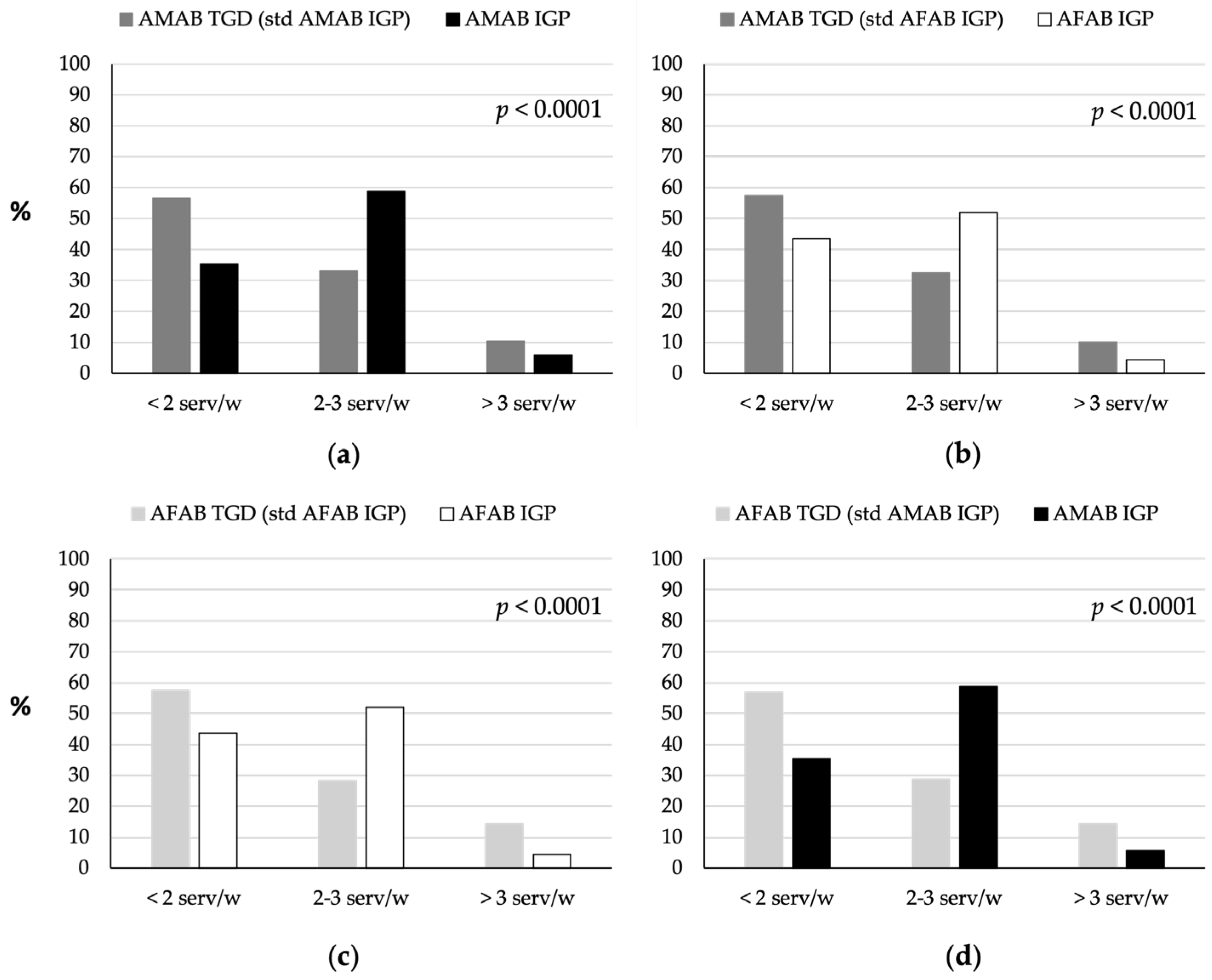
3.2. Red Meat Consumption
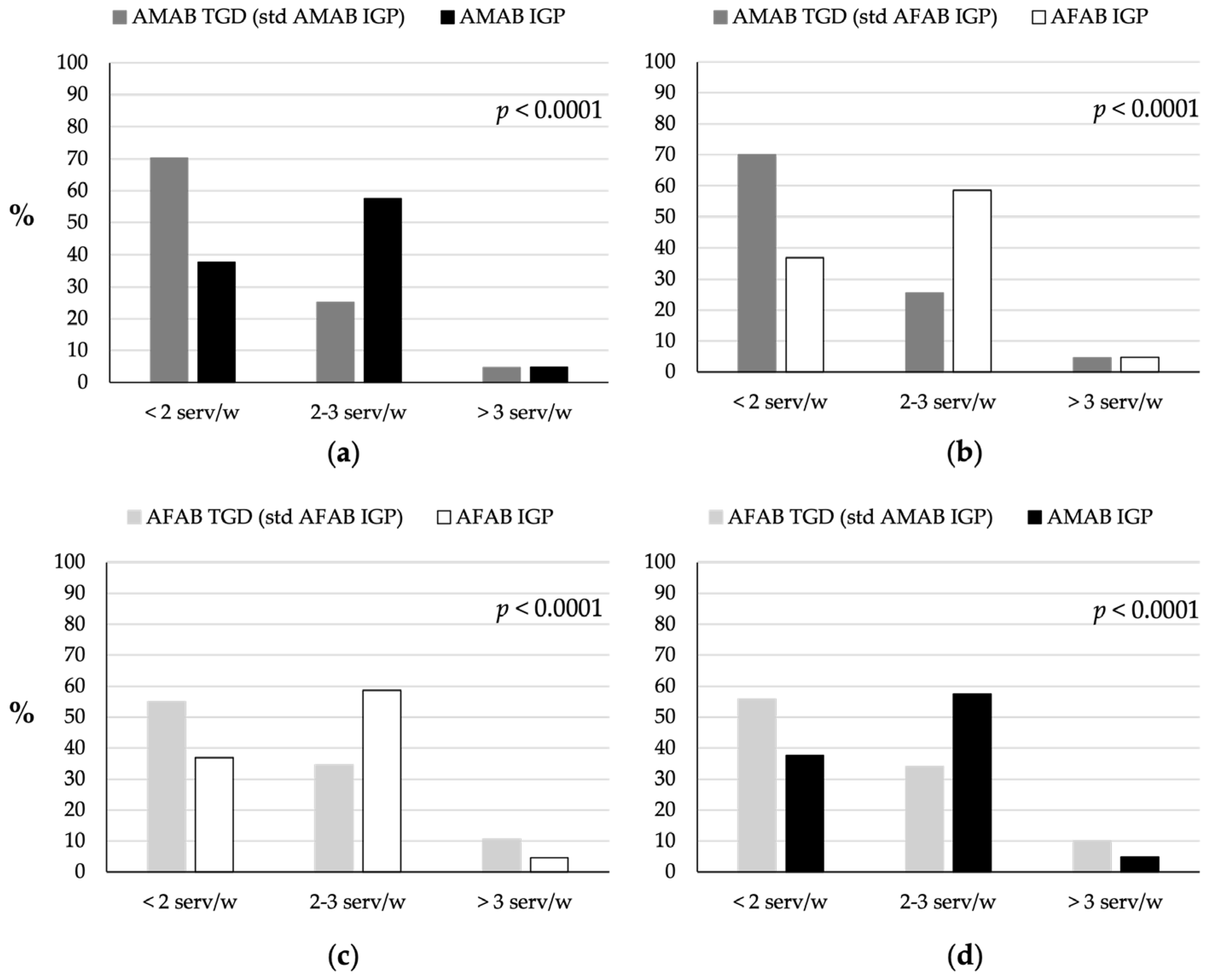
3.3. Fish Consumption
3.4. Milk and Yogurt Consumption
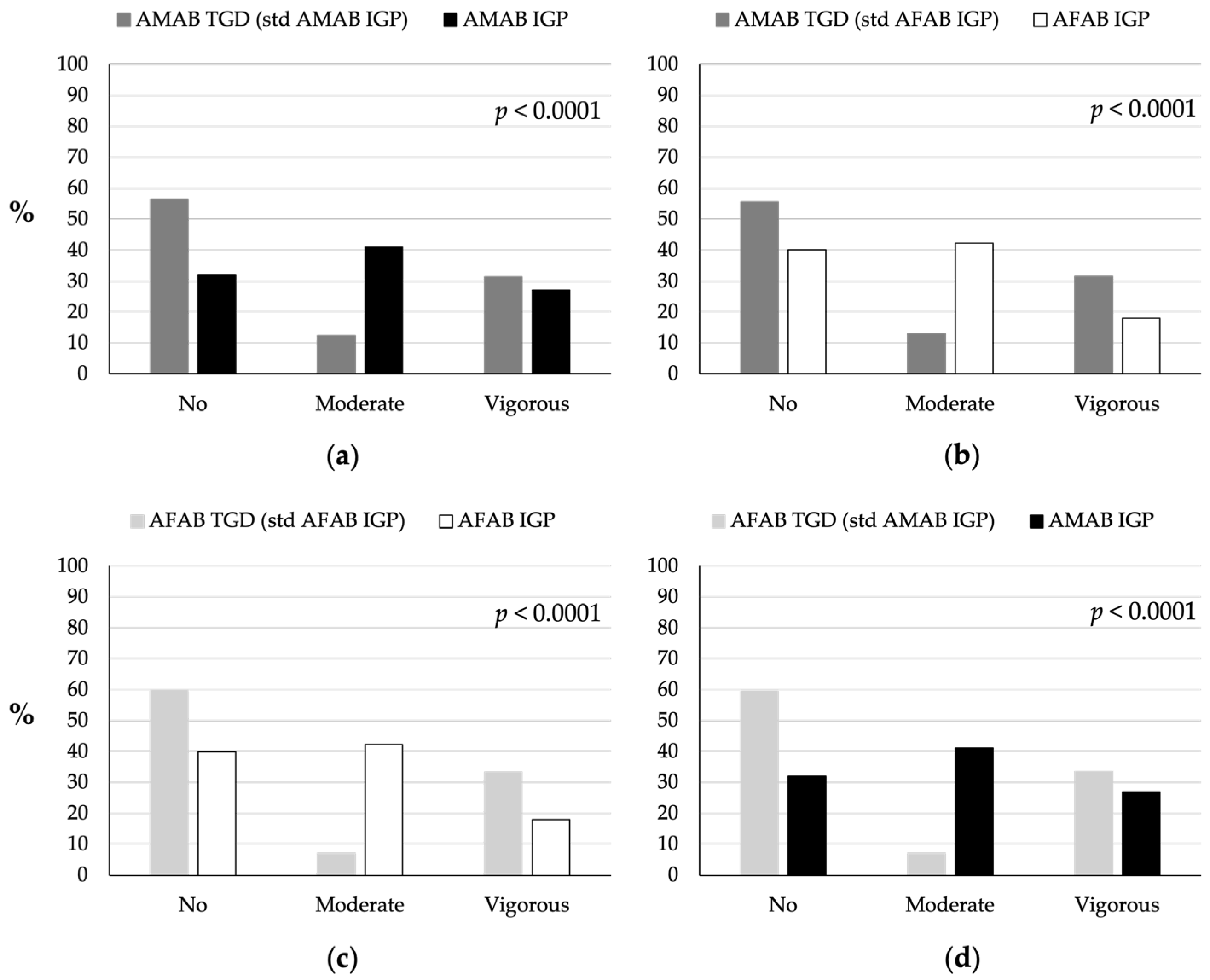
3.5. Physical Activity
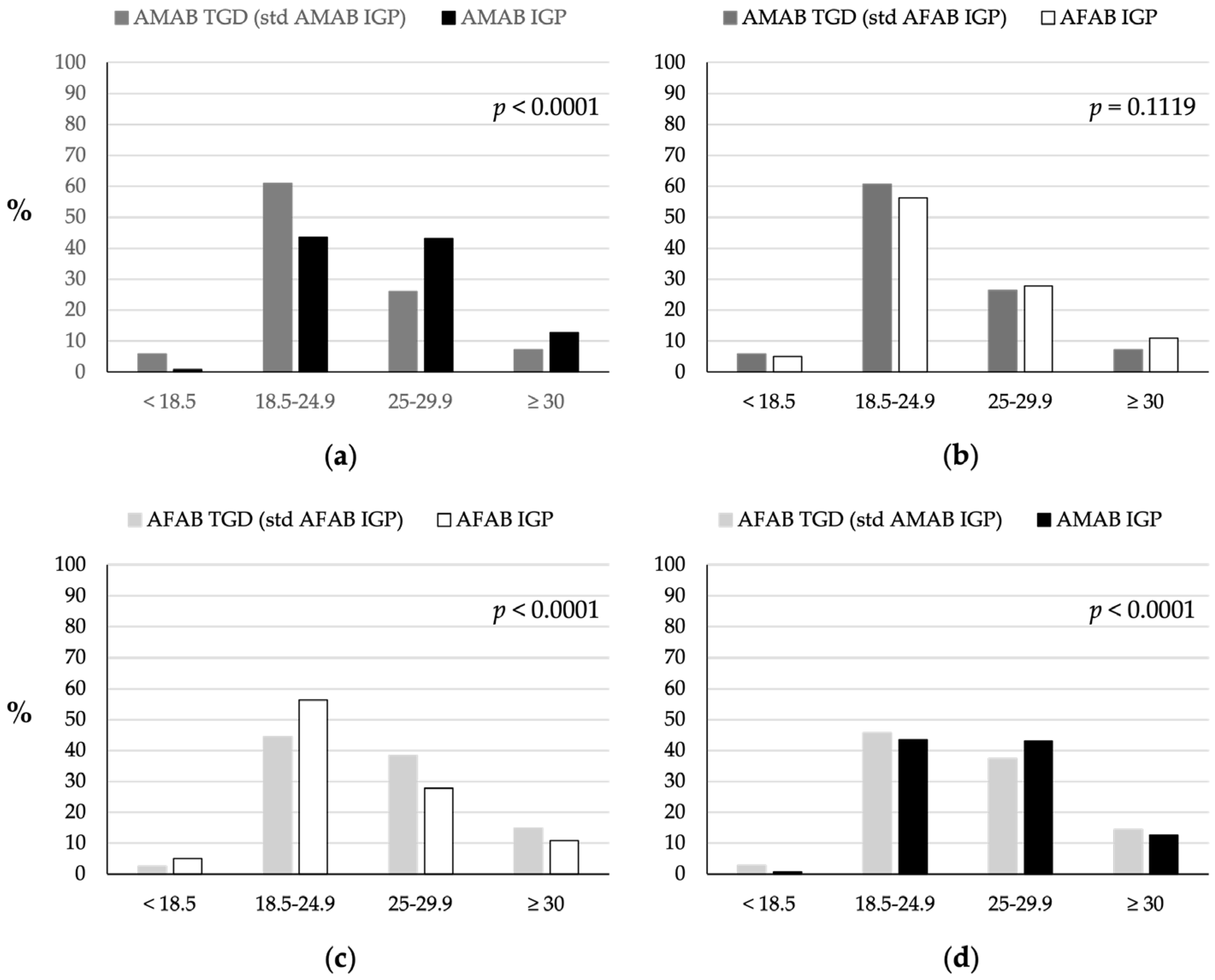
3.6. Body Mass Index
3.7. Logistic Regression Analyses
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- WHO. Int—Fact Sheets—Malnutrition. Available online: https://www.who.int/news-room/fact-sheets/detail/malnutrition (accessed on 22 July 2024).
- Afshin, A.; Sur, P.J.; Fay, K.A.; Cornaby, L.; Ferrara, G.; Salama, J.S.; Mullany, E.C.; Abate, K.H.; Abbafati, C.; Abebe, Z.; et al. Health Effects of Dietary Risks in 195 Countries, 1990–2017: A Systematic Analysis for the Global Burden of Disease Study 2017. Lancet 2019, 393, 1958–1972. [Google Scholar] [CrossRef]
- Firth, J.; Gangwisch, J.E.; Borsini, A.; Wootton, R.E.; Mayer, E.A. Food and Mood: How Do Diet and Nutrition Affect Mental Wellbeing? BMJ 2020, 369, m2382. [Google Scholar] [CrossRef] [PubMed]
- Davis, C.; Bryan, J.; Hodgson, J.; Murphy, K. Definition of the Mediterranean Diet; A Literature Review. Nutrients 2015, 7, 9139–9153. [Google Scholar] [CrossRef] [PubMed]
- WHO. Int—Fact Sheets—Healthy Diet. Available online: https://www.who.int/news-room/fact-sheets/detail/healthy-diet (accessed on 22 July 2024).
- CREA; Centro Di Ricerca Alimenti e La Nutrizione. Linee Guida per Una Sana Alimentazione. 2018. Available online: https://www.crea.gov.it/web/alimenti-e-nutrizione/-/linee-guida-per-una-sana-alimentazione-2018 (accessed on 22 July 2024).
- Rossi, L.; Berni Canani, S.; Censi, L.; Gennaro, L.; Leclercq, C.; Scognamiglio, U.; Sette, S.; Ghiselli, A. The 2018 Revision of Italian Dietary Guidelines: Development Process, Novelties, Main Recommendations, and Policy Implications. Front. Nutr. 2022, 9, 861526. [Google Scholar] [CrossRef]
- EpiCentro. It—Sorveglianza PASSI—Frutta e Verdura. Available online: https://www.epicentro.iss.it/passi/dati/frutta (accessed on 22 July 2024).
- EpiCentro. It—Sorveglianza PASSI—Attività Fisica. Available online: https://www.epicentro.iss.it/passi/dati/attivita-oms (accessed on 22 July 2024).
- EpiCentro. It—Sorveglianza PASSI—Eccesso Ponderale. Available online: https://www.epicentro.iss.it/passi/dati/sovrappeso (accessed on 22 July 2024).
- Coleman, E.; Radix, A.E.; Bouman, W.P.; Brown, G.R.; de Vries, A.L.C.; Deutsch, M.B.; Ettner, R.; Fraser, L.; Goodman, M.; Green, J.; et al. Standards of Care for the Health of Transgender and Gender Diverse People, Version 8. Int. J. Transgend. Health 2022, 23, S1–S259. [Google Scholar] [CrossRef]
- Reisner, S.L.; Poteat, T.; Keatley, J.A.; Cabral, M.; Mothopeng, T.; Dunham, E.; Holland, C.E.; Max, R.; Baral, S.D. Global Health Burden and Needs of Transgender Populations: A Review. Lancet 2016, 388, 412–436. [Google Scholar]
- Winter, S.; Diamond, M.; Green, J.; Karasic, D.; Reed, T.; Whittle, S.; Wylie, K. Transgender People: Health at the Margins of Society. Lancet 2016, 388, 390–400. [Google Scholar] [CrossRef]
- Rasmussen, S.M.; Dalgaard, M.K.; Roloff, M.; Pinholt, M.; Skrubbeltrang, C.; Clausen, L.; Kjaersdam Telléus, G. Eating Disorder Symptomatology among Transgender Individuals: A Systematic Review and Meta-Analysis. J. Eat. Disord. 2023, 11, 84. [Google Scholar] [CrossRef]
- Campbell, L.; Viswanadhan, K.; Lois, B.; Dundas, M. Emerging Evidence: A Systematic Literature Review of Disordered Eating Among Transgender and Nonbinary Youth. J. Adolesc. Health 2024, 74, 18–27. [Google Scholar] [CrossRef]
- McGregor, K.; McKenna, J.L.; Barrera, E.P.; Williams, C.R.; Hartman-Munick, S.M.; Guss, C.E. Disordered Eating and Considerations for the Transgender Community: A Review of the Literature and Clinical Guidance for Assessment and Treatment. J. Eat. Disord. 2023, 11, 75. [Google Scholar] [CrossRef]
- Egele, V.S.; Stark, R. Specific Health Beliefs Mediate Sex Differences in Food Choice. Front. Nutr. 2023, 10, 1159809. [Google Scholar] [CrossRef]
- Feraco, A.; Armani, A.; Amoah, I.; Guseva, E.; Camajani, E.; Gorini, S.; Strollo, R.; Padua, E.; Caprio, M.; Lombardo, M. Assessing Gender Differences in Food Preferences and Physical Activity: A Population-Based Survey. Front. Nutr. 2024, 11, 1348456. [Google Scholar] [CrossRef]
- Gomes, S.M.; Jacob, M.C.; Rocha, C.; Medeiros, M.F.; Lyra, C.O.; Noro, L.R. Expanding the Limits of Sex: A Systematic Review Concerning Food and Nutrition in Transgender Populations. Public Health Nutr. 2021, 24, 6436–6449. [Google Scholar] [CrossRef] [PubMed]
- Rozga, M.; Linsenmeyer, W.; Wood, J.C.; Darst, V.; Gradwell, E.K. Hormone Therapy, Health Outcomes and the Role of Nutrition in Transgender Individuals: A Scoping Review. Clin. Nutr. ESPEN 2020, 40, 42–56. [Google Scholar] [CrossRef]
- Linsenmeyer, W.; Waters, J. Sex and Gender Differences in Nutrition Research: Considerations with the Transgender and Gender Nonconforming Population. Nutr. J. 2021, 20, 6. [Google Scholar] [CrossRef]
- Marconi, M.; Pagano, M.T.; Ristori, J.; Bonadonna, S.; Pivonello, R.; Meriggiola, M.C.; Motta, G.; Lombardo, F.; Mosconi, M.; Oppo, A.; et al. Sociodemographic Profile, Health-Related Behaviours and Experiences of Healthcare Access in Italian Transgender and Gender Diverse Adult Population. J. Endocrinol. Investig. 2024, 1–14, Epub ahead of printing. [Google Scholar] [CrossRef]
- Turconi, G.; Bazzano, R.; Roggi, C.; Cena, H. Reliability and Relative Validity of a Quantitative Food-Frequency Questionnaire for Use among Adults in Italian Population. Int. J. Food Sci. Nutr. 2010, 61, 846–862. [Google Scholar] [CrossRef]
- Scazzocchio, B.; Varì, R.; Silenzi, A.; Giammarioli, S.; Masotti, A.; Baldassarre, A.; Santangelo, C.; D’Archivio, M.; Giovannini, C.; Del Cornò, M.; et al. Dietary Habits Affect Fatty Acid Composition of Visceral Adipose Tissue in Subjects with Colorectal Cancer or Obesity. Eur. J. Nutr. 2020, 59, 1463–1472. [Google Scholar] [CrossRef]
- ISTAT. Popolazione Residente 1° Gennaio 2021. Available online: http://dati.istat.it/Index.aspx?DataSetCode=DCIS_POPRES1# (accessed on 22 July 2024).
- Rippin, H.L.; Hutchinson, J.; Greenwood, D.C.; Jewell, J.; Breda, J.J.; Martin, A.; Rippin, D.M.; Schindler, K.; Rust, P.; Fagt, S.; et al. Inequalities in Education and National Income Are Associated with Poorer Diet: Pooled Analysis of Individual Participant Data across 12 European Countries. PLoS ONE 2020, 15, e0232447. [Google Scholar] [CrossRef]
- Parmenter, K.; Waller, J.; Wardle, J. Demographic Variation in Nutrition Knowledge in England. Health Educ. Res. 2000, 15, 163–174. [Google Scholar] [CrossRef]
- Puciato, D. Sociodemographic Associations of Physical Activity in People of Working Age. Int. J. Environ. Res. Public Health 2019, 16, 2134. [Google Scholar] [CrossRef]
- Frankel, H.M.; Staeheli, J.C. Calculating Body Mass Index. Ann. Intern. Med. 1992, 117, 698–699. [Google Scholar] [CrossRef] [PubMed]
- World Health Report 2002: Reducing Risks, Promoting Healthy Life; World Health Organization (WHO): Geneva, Switzerland, 2002.
- Nishi, S.K.; Khoury, N.; Valle Hita, C.; Zurbau, A.; Salas-Salvadó, J.; Babio, N. Vegetable and Fruit Intake Variety and Cardiovascular Health and Mortality: A Systematic Review and Meta-Analysis of Observational Studies. Nutrients 2023, 15, 4913. [Google Scholar] [CrossRef] [PubMed]
- Desjardins, Y. Fruit and Vegetables and Health: An Overview. In Horticulture: Plants for People and Places; Springer: Dordrecht, The Netherlands, 2014; Volume 3, pp. 965–1000. [Google Scholar]
- Lampe, J.W. Health Effects of Vegetables and Fruit: Assessing Mechanisms of Action in Human Experimental Studies. Am. J. Clin. Nutr. 1999, 70, 475S–490S. [Google Scholar] [CrossRef] [PubMed]
- Saini, R.K.; Ranjit, A.; Sharma, K.; Prasad, P.; Shang, X.; Gowda, K.G.M.; Keum, Y.-S. Bioactive Compounds of Citrus Fruits: A Review of Composition and Health Benefits of Carotenoids, Flavonoids, Limonoids, and Terpenes. Antioxidants 2022, 11, 239. [Google Scholar] [CrossRef]
- Miller, V.; Yusuf, S.; Chow, C.K.; Dehghan, M.; Corsi, D.J.; Lock, K.; Popkin, B.; Rangarajan, S.; Khatib, R.; Lear, S.A.; et al. Availability, Affordability, and Consumption of Fruits and Vegetables in 18 Countries across Income Levels: Findings from the Prospective Urban Rural Epidemiology (PURE) Study. Lancet Glob. Health 2016, 4, e695–e703. [Google Scholar] [CrossRef]
- Bishop, A.; Overcash, F.; McGuire, J.; Reicks, M. Diet and Physical Activity Behaviors Among Adolescent Transgender Students: School Survey Results. J. Adolesc. Health 2020, 66, 484–490. [Google Scholar] [CrossRef]
- Kirby, S.R.; Linde, J.A. Understanding the Nutritional Needs of Transgender and Gender-Nonconforming Students at a Large Public Midwestern University. Transgend. Health 2020, 5, 33–41. [Google Scholar] [CrossRef]
- Linsenmeyer, W.; Drallmeier, T.; Thomure, M. Towards Gender-Affirming Nutrition Assessment: A Case Series of Adult Transgender Men with Distinct Nutrition Considerations. Nutr. J. 2020, 19, 74. [Google Scholar] [CrossRef]
- Stea, T.H.; Nordheim, O.; Bere, E.; Stornes, P.; Eikemo, T.A. Fruit and Vegetable Consumption in Europe According to Gender, Educational Attainment and Regional Affiliation—A Cross-Sectional Study in 21 European Countries. PLoS ONE 2020, 15, e0232521. [Google Scholar] [CrossRef]
- Linsenmeyer, W.R. Should Clinicians Care About How Food Behaviors Express Gender Identity? AMA J. Ethics 2023, 25, E287–E293. [Google Scholar] [CrossRef] [PubMed]
- Ritzel, C.; Mann, S. The Old Man and the Meat: On Gender Differences in Meat Consumption across Stages of Human Life. Foods 2021, 10, 2809. [Google Scholar] [CrossRef] [PubMed]
- Rosenfeld, D.L. Masculinity and Men’s Resistance to Meat Reduction. Psychol. Hum. Anim. Intergroup Relat. 2023, 2, 1–11. [Google Scholar] [CrossRef]
- Lombardo, M.; Feraco, A.; Camajani, E.; Gorini, S.; Strollo, R.; Armani, A.; Padua, E.; Caprio, M. Effects of Different Nutritional Patterns and Physical Activity on Body Composition: A Gender and Age Group Comparative Study. Foods 2024, 13, 529. [Google Scholar] [CrossRef]
- Zhao, H.; Wang, M.; Peng, X.; Zhong, L.; Liu, X.; Shi, Y.; Li, Y.; Chen, Y.; Tang, S. Fish Consumption in Multiple Health Outcomes: An Umbrella Review of Meta-Analyses of Observational and Clinical Studies. Ann. Transl. Med. 2023, 11, 152. [Google Scholar] [CrossRef]
- Govzman, S.; Looby, S.; Wang, X.; Butler, F.; Gibney, E.R.; Timon, C.M. A Systematic Review of the Determinants of Seafood Consumption. Br. J. Nutr. 2021, 126, 66–80. [Google Scholar] [CrossRef]
- Pieniak, Z.; Verbeke, W.; Scholderer, J. Health-related Beliefs and Consumer Knowledge as Determinants of Fish Consumption. J. Hum. Nutr. Diet. 2010, 23, 480–488. [Google Scholar] [CrossRef] [PubMed]
- Soedamah-Muthu, S.S.; Masset, G.; Verberne, L.; Geleijnse, J.M.; Brunner, E.J. Consumption of Dairy Products and Associations with Incident Diabetes, CHD and Mortality in the Whitehall II Study. Br. J. Nutr. 2013, 109, 718–726. [Google Scholar] [CrossRef]
- Mullie, P.; Pizot, C.; Autier, P. Daily Milk Consumption and All-Cause Mortality, Coronary Heart Disease and Stroke: A Systematic Review and Meta-Analysis of Observational Cohort Studies. BMC Public Health 2016, 16, 1236. [Google Scholar] [CrossRef]
- Zhou, J.; Wu, Z.; Lin, Z.; Wang, W.; Wan, R.; Liu, T. Association of Milk Consumption with All-Cause Mortality and Cardiovascular Outcomes: A UK Biobank Based Large Population Cohort Study. J. Transl. Med. 2023, 21, 130. [Google Scholar] [CrossRef]
- Tutunchi, H.; Naghshi, S.; Naemi, M.; Naeini, F.; Esmaillzadeh, A. Yogurt Consumption and Risk of Mortality from All Causes, CVD and Cancer: A Comprehensive Systematic Review and Dose–Response Meta-Analysis of Cohort Studies. Public Health Nutr. 2023, 26, 1196–1209. [Google Scholar] [CrossRef] [PubMed]
- Zhang, X.; Chen, X.; Xu, Y.; Yang, J.; Du, L.; Li, K.; Zhou, Y. Milk Consumption and Multiple Health Outcomes: Umbrella Review of Systematic Reviews and Meta-Analyses in Humans. Nutr. Metab. 2021, 18, 7. [Google Scholar] [CrossRef]
- Pala, V.; Sieri, S.; Chiodini, P.; Masala, G.; Palli, D.; Mattiello, A.; Panico, S.; Tumino, R.; Frasca, G.; Fasanelli, F.; et al. Associations of Dairy Product Consumption with Mortality in the European Prospective Investigation into Cancer and Nutrition (EPIC)–Italy Cohort. Am. J. Clin. Nutr. 2019, 110, 1220–1230. [Google Scholar] [CrossRef] [PubMed]
- Guo, J.; Astrup, A.; Lovegrove, J.A.; Gijsbers, L.; Givens, D.I.; Soedamah-Muthu, S.S. Milk and Dairy Consumption and Risk of Cardiovascular Diseases and All-Cause Mortality: Dose–Response Meta-Analysis of Prospective Cohort Studies. Eur. J. Epidemiol. 2017, 32, 269–287. [Google Scholar] [CrossRef] [PubMed]
- Dehghan, M.; Mente, A.; Rangarajan, S.; Sheridan, P.; Mohan, V.; Iqbal, R.; Gupta, R.; Lear, S.; Wentzel-Viljoen, E.; Avezum, A.; et al. Association of Dairy Intake with Cardiovascular Disease and Mortality in 21 Countries from Five Continents (PURE): A Prospective Cohort Study. Lancet 2018, 392, 2288–2297. [Google Scholar] [CrossRef]
- Eysteinsdottir, T.; Halldorsson, T.I.; Thorsdottir, I.; Sigurdsson, G.; Sigurðsson, S.; Harris, T.; Launer, L.J.; Gudnason, V.; Gunnarsdottir, I.; Steingrimsdottir, L. Milk Consumption throughout Life and Bone Mineral Content and Density in Elderly Men and Women. Osteoporos. Int. 2014, 25, 663–672. [Google Scholar] [CrossRef]
- Torres-Gonzalez, M.; Cifelli, C.J.; Agarwal, S.; Fulgoni, V.L. Association of Milk Consumption and Vitamin D Status in the US Population by Ethnicity: NHANES 2001–2010 Analysis. Nutrients 2020, 12, 3720. [Google Scholar] [CrossRef]
- Samara, A.; Herbeth, B.; Ndiaye, N.C.; Fumeron, F.; Billod, S.; Siest, G.; Visvikis-Siest, S. Dairy Product Consumption, Calcium Intakes, and Metabolic Syndrome–Related Factors over 5 Years in the STANISLAS Study. Nutrition 2013, 29, 519–524. [Google Scholar] [CrossRef]
- Guiné, R.P.F.; Florença, S.G.; Carpes, S.; Anjos, O. Study of the Influence of Sociodemographic and Lifestyle Factors on Consumption of Dairy Products: Preliminary Study in Portugal and Brazil. Foods 2020, 9, 1775. [Google Scholar] [CrossRef]
- Van Caenegem, E.; Taes, Y.; Wierckx, K.; Vandewalle, S.; Toye, K.; Kaufman, J.-M.; Schreiner, T.; Haraldsen, I.; T’Sjoen, G. Low Bone Mass Is Prevalent in Male-to-Female Transsexual Persons before the Start of Cross-Sex Hormonal Therapy and Gonadectomy. Bone 2013, 54, 92–97. [Google Scholar] [CrossRef]
- Motta, G.; Marinelli, L.; Barale, M.; Brustio, P.R.; Manieri, C.; Ghigo, E.; Procopio, M.; Lanfranco, F. Fracture Risk Assessment in an Italian Group of Transgender Women after Gender-Confirming Surgery. J. Bone Min. Metab. 2020, 38, 885–893. [Google Scholar] [CrossRef]
- Fard, N.A.; De Francisci Morales, G.; Mejova, Y.; Schifanella, R. On the Interplay between Educational Attainment and Nutrition: A Spatially-Aware Perspective. EPJ Data Sci. 2021, 10, 18. [Google Scholar] [CrossRef]
- Warburton, D.E.R.; Bredin, S.S.D. Health Benefits of Physical Activity. Curr. Opin. Cardiol. 2017, 32, 541–556. [Google Scholar] [CrossRef] [PubMed]
- Bauman, A.E.; Reis, R.S.; Sallis, J.F.; Wells, J.C.; Loos, R.J.; Martin, B.W. Correlates of Physical Activity: Why Are Some People Physically Active and Others Not? Lancet 2012, 380, 258–271. [Google Scholar] [CrossRef] [PubMed]
- Whipple, M.O.; Pinto, A.J.; Abushamat, L.A.; Bergouignan, A.; Chapman, K.; Huebschmann, A.G.; Masters, K.S.; Nadeau, K.J.; Scalzo, R.L.; Schauer, I.E.; et al. Sex Differences in Physical Activity Among Individuals With Type 2 Diabetes Across the Life Span: A Systematic Review and Meta-Analysis. Diabetes Care 2022, 45, 2163–2177. [Google Scholar] [CrossRef]
- Grzymisławska, M.; Puch, E.; Zawada, A.; Grzymisławski, M. Do Nutritional Behaviors Depend on Biological Sex and Cultural Gender? Adv. Clin. Exp. Med. 2020, 29, 165–172. [Google Scholar] [CrossRef]
- Lightner, J.S.; Schneider, J.; Grimes, A.; Wigginton, M.; Curran, L.; Gleason, T.; Prochnow, T. Physical Activity among Transgender Individuals: A Systematic Review of Quantitative and Qualitative Studies. PLoS ONE 2024, 19, e0297571. [Google Scholar] [CrossRef]
- James, H.A.; Chang, A.Y.; Imhof, R.L.; Sahoo, A.; Montenegro, M.M.; Imhof, N.R.; Gonzalez, C.A.; Lteif, A.N.; Nippoldt, T.B.; Davidge-Pitts, C.J. A Community-Based Study of Demographics, Medical and Psychiatric Conditions, and Gender Dysphoria/Incongruence Treatment in Transgender/Gender Diverse Individuals. Biol. Sex Differ. 2020, 11, 55. [Google Scholar] [CrossRef]
- Austin, F.; Wright, K.E.; Jackson, B.; Lin, A.; Schweizer, K.; Furzer, B.J. A Scoping Review of Trans and Gender Diverse Children and Adolescents’ Experiences of Physical Activity, Sport, and Exercise Participation. Ment. Health Phys. Act. 2024, 26, 100576. [Google Scholar] [CrossRef]
- Kari, J.T.; Viinikainen, J.; Böckerman, P.; Tammelin, T.H.; Pitkänen, N.; Lehtimäki, T.; Pahkala, K.; Hirvensalo, M.; Raitakari, O.T.; Pehkonen, J. Education Leads to a More Physically Active Lifestyle: Evidence Based on Mendelian Randomization. Scand. J. Med. Sci. Sports 2020, 30, 1194–1204. [Google Scholar] [CrossRef]
- Teti, M.; Bauerband, L.A.; Rolbiecki, A.; Young, C. Physical Activity and Body Image: Intertwined Health Priorities Identified by Transmasculine Young People in a Non-Metropolitan Area. Int. J. Transgend. Health 2020, 21, 209–219. [Google Scholar] [CrossRef] [PubMed]
- Serrano, J.L.; Caminha, I.d.O.; Gomes, I.S.; Neves, E.M.; Lopes, D.T. Mulheres Trans e Atividade Física: Fabricando o Corpo Feminino. Interface Comun. Saúde Educ. 2019, 23, e180624. [Google Scholar] [CrossRef]
- Knaus, S.; Steininger, J.; Klinger, D.; Riedl, S. Body Mass Index Distributions and Obesity Prevalence in a Transgender Youth Cohort—A Retrospective Analysis. J. Adolesc. Health 2024, 75, 127–132. [Google Scholar] [CrossRef] [PubMed]
- Spanos, C.; Bretherton, I.; Zajac, J.D.; Cheung, A.S. Effects of Gender-Affirming Hormone Therapy on Insulin Resistance and Body Composition in Transgender Individuals: A Systematic Review. World J. Diabetes 2020, 11, 66–77. [Google Scholar] [CrossRef] [PubMed]
- VanKim, N.A.; Erickson, D.J.; Eisenberg, M.E.; Lust, K.; Simon Rosser, B.R.; Laska, M.N. Weight-Related Disparities for Transgender College Students. Health Behav. Policy Rev. 2014, 1, 161–171. [Google Scholar] [CrossRef]
- De Blok, C.J.; Wiepjes, C.M.; van Velzen, D.M.; Staphorsius, A.S.; Nota, N.M.; Gooren, L.J.; Kreukels, B.P.; den Heijer, M. Mortality Trends over Five Decades in Adult Transgender People Receiving Hormone Treatment: A Report from the Amsterdam Cohort of Gender Dysphoria. Lancet Diabetes Endocrinol. 2021, 9, 663–670. [Google Scholar] [CrossRef]
- Malhotra, A.; Kort, S.; Lauther, T.; Mann, N.; Skopicki, H.A.; Parikh, P.B. Prevalence and Predictors of Cardiovascular Disease and Risk Factors in Transgender Persons in the United States. Crit. Pathw. Cardiol. A J. Evid. Based Med. 2022, 21, 42–46. [Google Scholar] [CrossRef]
- Boehmer, U.; Gereige, J.; Winter, M.; Ozonoff, A.; Scout, N. Transgender Individuals’ Cancer Survivorship: Results of a Cross-sectional Study. Cancer 2020, 126, 2829–2836. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| TGD Population | AMAB TGD | AFAB TGD | ||
|---|---|---|---|---|
| p, AMAB TGD vs. AFAB TGD * | ||||
| Age | <0.001 | |||
| N. of respondents | 959 | 334 | 625 | |
| Mean (SD) | 30.46 (11.13) | 34.46 (12.80) | 28.32 (9.46) | |
| Median (Q1, Q3) | 26 (22, 37) | 31 (23, 45) | 25 (21, 33) | |
| Min, Max | 18, 68 | 18, 68 | 18, 61 | |
| n (%) | n (%) | n (%) | p, AMAB TGD vs. AFAB TGD ** | |
| Age group | <0.001 | |||
| 18–24.9 | 396 (41.29) | 105 (31.44) | 291 (46.56) | |
| 25–34.9 | 286 (29.82) | 84 (25.15) | 202 (32.32) | |
| 35–44.9 | 138 (14.39) | 57 (17.07) | 81 (12.96) | |
| 45–54.9 | 98 (10.22) | 58 (17.37) | 40 (6.40) | |
| ≥55 | 41 (4.27) | 30 (8.99) | 11 (1.76) | |
| Total | 959 (100) | 334 (100) | 625 (100) | |
| Educational level | 0.001 | |||
| Low | 224 (23.48) | 97 (29.31) | 127 (20.39) | |
| High | 730 (76.52) | 234 (70.69) | 496 (79.61) | |
| Total | 954 (100) | 331 (100) | 623 (100) | |
| Employment | <0.001 | |||
| No | 257 (26.97) | 128 (38.79) | 129 (20.71) | |
| Yes | 696 (73.03) | 202 (61.21) | 494 (79.29) | |
| Total | 953 (100) | 330 (100) | 623 (100) |
| TGD Population | AMAB TGD | AFAB TGD | ||||
|---|---|---|---|---|---|---|
| OR (95% CIs) | p | OR (95% CIs) | p | OR (95% CIs) | p | |
| Fruit and vegetables optimal consumption (Yes vs. No) | ||||||
| Sex assigned at birth (AFAB vs. AMAB) | 1.116 (0.575–2.167) | 0.745 | ||||
| Age (x + 1 vs. x) | 1.028 (1.002–1.054) | 0.033 | 1.052 (1.013–1.092) | 0.008 | 1.006 (0.969–1.045) | 0.742 |
| Educational level (High vs. Low) | 2.107 (0.868–5.118) | 0.100 | 3.013 (0.631–14.399) | 0.167 | 1.679 (0.571–4.940) | 0.347 |
| Employment (No vs. Yes) | 0.697 (0.325–1.496) | 0.354 | 0.935 (0.299–2.922) | 0.908 | 0.590 (0.201–1.734) | 0.338 |
| Red meat optimal consumption (Yes vs. No) | ||||||
| Sex assigned at birth (AFAB vs. AMAB) | 0.771 (0.580–1.026) | 0.075 | ||||
| Age (x + 1 vs. x) | 1.013 (1.001–1.025) | 0.041 | 0.998 (0.981–1.015) | 0.780 | 1.029 (1.012–1.047) | 0.001 |
| Educational level (High vs. Low) | 1.094 (0.802–1.493) | 0.571 | 1.072 (0.653–1.759) | 0.784 | 1.184 (0.787–1.781) | 0.418 |
| Employment (No vs. Yes) | 0.865 (0.639–1.170) | 0.346 | 1.293 (0.812–2.060) | 0.279 | 0.610 (0.405–0.920) | 0.018 |
| Fish optimal consumption (Yes vs. No) | ||||||
| Sex assigned at birth (AFAB vs. AMAB) | 0.939 (0.522–1.688) | 0.832 | ||||
| Age (x + 1 vs. x) | 1.016 (0.992–1.040) | 0.198 | 1.000 (0.965–1.035) | 0.987 | 1.032 (1.000–1.065) | 0.047 |
| Educational level (High vs. Low) | 2.270 (1.003–5.138) | 0.049 | 1.220 (0.421–3.537) | 0.714 | 5.042 (1.184–21.473) | 0.029 |
| Employment (No vs. Yes) | 0.676 (0.339–1.348) | 0.266 | 0.652 (0.239–1.773) | 0.402 | 0.632 (0.239–1.673) | 0.355 |
| Milk and Yogurt optimal consumption (Yes vs. No) | ||||||
| Sex assigned at birth (AFAB vs. AMAB) | 0.886 (0.633–1.240) | 0.480 | ||||
| Age (x + 1 vs. x) | 0.995 (0.981–1.010) | 0.512 | 1.002 (0.982–1.022) | 0.861 | 0.989 (0.968–1.010) | 0.291 |
| Educational level (High vs. Low) | 0.667 (0.468–0.949) | 0.024 | 0.484 (0.275–0.855) | 0.012 | 0.793 (0.500–1.259) | 0.326 |
| Employment (No vs. Yes) | 0.739 (0.512–1.067) | 0.107 | 0.527 (0.296–0.936) | 0.029 | 0.937 (0.582–1.510) | 0.790 |
| Physical activity (Yes vs. No) | ||||||
| Sex assigned at birth (AFAB vs. AMAB) | 1.193 (0.897–1.586) | 0.226 | ||||
| Age (x + 1 vs. x) | 1.004 (0.992–1.016) | 0.568 | 1.018 (1.000–1.036) | 0.045 | 0.991 (0.974–1.007) | 0.269 |
| Educational level (High vs. Low) | 1.610 (1.179–2.199) | 0.003 | 2.083 (1.247–3.479) | 0.005 | 1.373 (0.921–2.048) | 0.120 |
| Employment (No vs. Yes) | 0.790 (0.584–1.067) | 0.124 | 1.172 (0.731–1.878) | 0.511 | 0.617 (0.414–0.919) | 0.018 |
| POR (95% CIs) | p | POR (95% CIs) | p | POR (95% CIs) | p | |
| Body Mass Index (4 classes) | ||||||
| Sex assigned at birth (AFAB vs. AMAB) | 1.738 (1.308–2.309) | <0.001 | ||||
| Age (x + 1 vs. x) | 1.028 (1.017–1.041) | <0.001 | 1.028 (1.010–1.046) | 0.002 | 1.029 (1.013–1.046) | <0.001 |
| Educational level (High vs. Low) | 0.716 (0.528–0.970) | 0.031 | 0.599 (0.358–1.003) | 0.051 | 0.779 (0.533–1.140) | 0.199 |
| Employment (No vs. Yes) | 1.174 (0.870–1.584) | 0.293 | 0.933 (0.575–1.513) | 0.778 | 1.342 (0.913–1.972) | 0.135 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Santangelo, C.; Marconi, M.; Ruocco, A.; Ristori, J.; Bonadonna, S.; Pivonello, R.; Meriggiola, M.C.; Lombardo, F.; Motta, G.; Crespi, C.M.; et al. Dietary Habits, Physical Activity and Body Mass Index in Transgender and Gender Diverse Adults in Italy: A Voluntary Sampling Observational Study. Nutrients 2024, 16, 3139. https://doi.org/10.3390/nu16183139
Santangelo C, Marconi M, Ruocco A, Ristori J, Bonadonna S, Pivonello R, Meriggiola MC, Lombardo F, Motta G, Crespi CM, et al. Dietary Habits, Physical Activity and Body Mass Index in Transgender and Gender Diverse Adults in Italy: A Voluntary Sampling Observational Study. Nutrients. 2024; 16(18):3139. https://doi.org/10.3390/nu16183139
Chicago/Turabian StyleSantangelo, Carmela, Matteo Marconi, Angela Ruocco, Jiska Ristori, Stefania Bonadonna, Rosario Pivonello, Maria Cristina Meriggiola, Francesco Lombardo, Giovanna Motta, Chiara Michela Crespi, and et al. 2024. "Dietary Habits, Physical Activity and Body Mass Index in Transgender and Gender Diverse Adults in Italy: A Voluntary Sampling Observational Study" Nutrients 16, no. 18: 3139. https://doi.org/10.3390/nu16183139