
Does Mobility of the Ankle Joint Depends on Length of the Free Part of the Achilles Tendon?



Abstract
:1. Introduction
2. Methods
2.1. Study Group
- -
- Group 1 (n = 15)—participants with a normal range of dorsiflexion in the ankle joint (20° or more)
- -
- Group 2 (n = 21)—participants with a reduced range of dorsiflexion in the ankle joint (below 20°)
2.2. Sample Size Estimation
2.3. Length Calculation of the Free Part of the Achilles Tendon
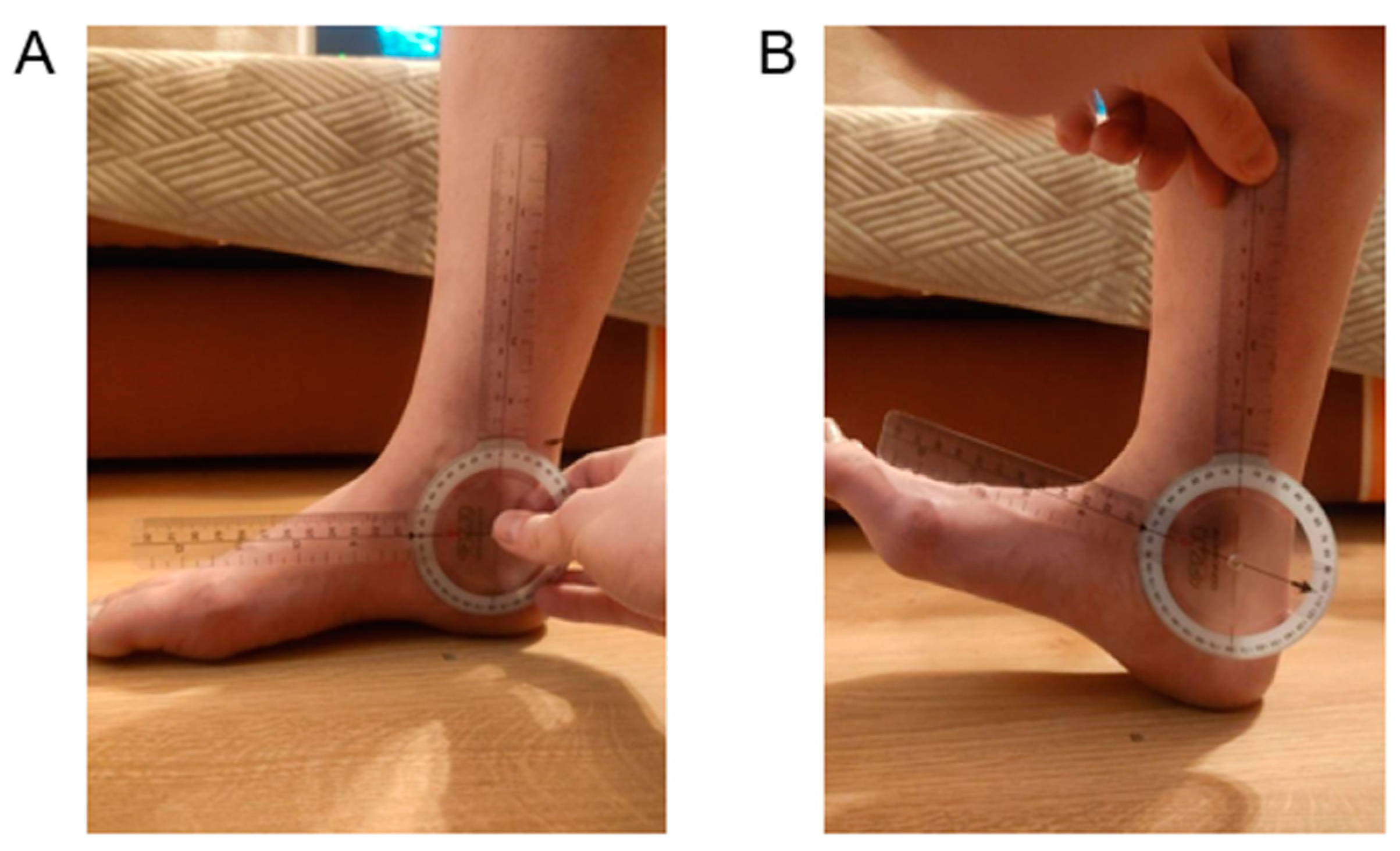
2.4. Dorsiflexion Measurements of the Ankle Joint Using a Goniometer
2.5. Measurement of Functional Mobility Regarding Dorsiflexion of the Ankle Joint Using the Weight-Bearing Lunge Test (WBLT)
2.6. Statistical Analyses
3. Results
3.1. Between-Group Comparison
3.2. Correlations
3.3. Diagnostic Value of Data
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Del Buono, A.; Chan, O.; Maffulli, N. Achilles tendon: Functional anatomy and novel emerging models of imaging classification. Int. Orthop. 2013, 37, 715–721. [Google Scholar] [CrossRef] [Green Version]
- Myers, T. Anatomy Trains: Myofascial Meridians for Manual and Movement Therapists, 2nd ed.; Churchill Livingstone: Edinburgh, UK, 2009. [Google Scholar]
- Hug, F.; Lacourpaille, L.; Maïsetti, O.; Nordez, A. Slack length of gastrocnemius medialis and Achilles tendon occurs at different ankle angles. J. Biomech. 2013, 46, 2534–2538. [Google Scholar] [CrossRef]
- Zellers, J.A.; Carmont, M.R.; Silbernagel, K.G. Achilles Tendon Resting Angle Relates to Tendon Length and Function. Foot Ankle Int. 2017, 39, 343–348. [Google Scholar] [CrossRef]
- Munteanu, S.E.; Barton, C.J. Lower limb biomechanics during running in individuals with Achilles tendinopathy: A systematic review. J. Foot Ankle Res. 2011, 4, 15. [Google Scholar] [CrossRef] [Green Version]
- Stenroth, L.; Peltonen, J.; Cronin, N.J.; Sipilä, S.; Finni, T. Age-related differences in Achilles tendon properties and triceps surae muscle architecture in vivo. J. Appl. Physiol. 2012, 113, 1537–1544. [Google Scholar] [CrossRef] [Green Version]
- Akeson, W.H.; Amiel, D.; Abel, M.F.; Garfin, S.R.; Woo, S.L. Effects of immobilization on joints. Clin. Orthop. Relat. Res. 1987, 219, 28–37. [Google Scholar] [CrossRef]
- Ghanem, I.; Massaad, A.; Assi, A.; Rizkallah, M.; Bizdikian, A.J.; El Abiad, R.; Seringe, R.; Mosca, V.; Wicart, P. Understanding the foot's functional anatomy in physiological and pathological conditions: The calcaneopedal unit concept. J. Child. Orthop. 2019, 13, 134–146. [Google Scholar] [CrossRef]
- Kaltenborn, F.; Evjenth, O. Manuelle Therapie Teil I—Extrernitäten [Eng. Manual Therapy Part 1—The Extremities], 10A; Olaf Norlis Bokhandel: Oslo, Norway, 1999. [Google Scholar]
- Schünke, M.; Schulte, E.; Schumacher, U. Prometheus Learn Atlas of Anatomy. General Anatomy and Musculoskeletal System 5. Auflage; Georg Thieme Verlag KG: Stuttgart, Germany, 2018. [Google Scholar]
- Pirri, C.; Fede, C.; Stecco, A.; Guidolin, D.; Fan, C.; De Caro, R.; Stecco, C. Ultrasound Imaging of Crural Fascia and Epimysial Fascia Thicknesses in Basketball Players with Previous Ankle Sprains Versus Healthy Subjects. Diagnostics 2021, 11, 177. [Google Scholar] [CrossRef]
- McAuliffe, S.; McCreesh, K.; Culloty, F.; Purtill, H.; O’Sullivan, K. Can ultrasound imaging predict the development of Achilles and patellar tendinopathy? A systematic review and meta-analysis. Br. J. Sports Med. 2016, 50, 1516–1523. [Google Scholar] [CrossRef]
- Pirri, C.; Stecco, C.; Fede, C.; De Caro, R.; Özçakar, L. Dynamic Ultrasound Examination of the Paratenon and Fascia in Chronic Achilles Tendinopathy. Am. J. Phys. Med. Rehabil. 2021, 100, e75. [Google Scholar] [CrossRef]
- Bredeweg, S.W.; Buist, I.; Kluitenberg, B. Differences in kinetic asymmetry between injured and non-injured novice runners: A prospective cohort study. Gait Posture 2013, 38, 847–852. [Google Scholar] [CrossRef]
- Barfod, K.W.; Riecke, A.F.; Boesen, A.; Hansen, P.; Maier, J.F.; Doessing, S.; Troelsen, A. Validity and reliability of an ultrasound measurement of the free length of the Achilles tendon. Dan Med. J. 2018, 65, A5453. [Google Scholar]
- Barfod, K.W.; Riecke, A.F.; Boesen, A.; Hansen, P.; Maier, J.F.; Døssing, S.; Troelsen, A. Validation of a novel ultrasound measurement of Achilles tendon length. Knee Surg. Sports Traumatol. Arthrosc. 2015, 23, 3398–3406. [Google Scholar] [CrossRef]
- Silbernagel, K.G.; Shelley, K.; Powell, S.; Varrecchia, S. Extended field of view ultrasound imaging to evaluate Achilles tendon length and thickness: A reliability and validity study. Muscles Ligaments Tendons. J. 2016, 6, 104–110. [Google Scholar] [CrossRef]
- Hansen, M.S.; Kristensen, M.T.; Hölmich, P.; Barfod, K.W. The Achilles Tendon Length Measure and the Achilles Tendon Resting Angle show acceptable construct validity using the Copenhagen Achilles Length Measure as gold standard. Foot Ankle Surg. 2021, 27, 655–659. [Google Scholar] [CrossRef]
- Krause, D.A.; Cloud, B.A.; Forster, L.A.; Schrank, J.A.; Hollman, J.H. Measurement of ankle dorsiflexion: A comparison of active and passive techniques in multiple positions. J. Sport Rehabil. 2011, 20, 333–344. [Google Scholar] [CrossRef]
- Langarika-Rocafort, A.; Emparanza, J.I.; Aramendi, J.F.; Castellano, J.; Calleja-González, J. Intra-rater reliability and agreement of various methods of measurement to assess dorsiflexion in the Weight Bearing Dorsiflexion Lunge Test (WBLT) among female athletes. Phys. Ther. Sport. 2017, 23, 37–44. [Google Scholar] [CrossRef]
- Powden, C.J.; Hoch, J.M.; Hoch, M.C. Reliability and minimal detectable change of the weight-bearing lunge test: A systematic review. Man Ther. 2015, 20, 524–532. [Google Scholar] [CrossRef]
- Zembaty, A. (Ed.) Kinesitherapy. Vol. I. Outline of Theoretical Foundations and Kinesitherapy Diagnostics; “Kasper” Sp. z.o.o.: Kraków, Poland, 2002. [Google Scholar]
- Schmidt, S.A.J.; Lo, S.; Hollestein, L.M. Research Techniques Made Simple: Sample Size Estimation and Power Calculation. J. Investig. Dermatol. 2018, 138, 1678–1682. [Google Scholar] [CrossRef] [Green Version]
- Zhang, X.; Deng, L.; Xiao, S.; Li, L.; Fu, W. Sex Differences in the Morphological and Mechanical Properties of the Achilles Tendon. Int. J. Environ. Res. Public Health 2021, 18, 8974. [Google Scholar] [CrossRef]
- Intziegianni, K.; Cassel, M.; Hain, G.; Mayer, F. Gender Differences of Achilles tendon Cross-sectional Area during Loading. Sports Med. Int. Open. 2017, 1, E135–E140. [Google Scholar] [CrossRef]
- McNally, E. Practical Musculoskeletal Ultrasound, 2nd ed.; Churchill Livingstone Elsevier: London, UK, 2014. [Google Scholar]
- Schober, P.; Boer, C.; Schwarte, L.A. Correlation Coefficients: Appropriate Use and Interpretation. Anesth. Analg. 2018, 126, 1763–1768. [Google Scholar] [CrossRef]
- Hajian-Tilaki, K. Receiver Operating Characteristic (ROC) Curve Analysis for Medical Diagnostic Test Evaluation. Caspian J. Intern. Med. 2013, 4, 627–635. [Google Scholar]
- Costa, M.L.; Logan, K.; Heylings, D.; Donell, S.T.; Tucker, K. The effect of Achilles tendon lengthening on ankle dorsiflexion: A cadaver study. Foot Ankle Int. 2006, 27, 414–417. [Google Scholar] [CrossRef]
- Carmont, M.R.; Grävare Silbernagel, K.; Brorsson, A.; Olsson, N.; Maffulli, N.; Karlsson, J. The Achilles tendon resting angle as an indirect measure of Achilles tendon length following rupture, repair, and rehabilitation. Asia Pac. J. Sports Med. Arthrosc. Rehabil. Technol. 2015, 2, 49–55. [Google Scholar] [CrossRef] [Green Version]
- Barfod, K.W. Achilles tendon rupture; assessment of non-operative treatment. Dan Med. J. 2014, 61, B4837. [Google Scholar]
- Glazebrook, M.; Rubinger, D. Functional Rehabilitation for Nonsurgical Treatment of Acute Achilles Tendon Rupture. Foot Ankle Clin. 2019, 24, 387–398. [Google Scholar] [CrossRef]
- Bravo-Sánchez, A.; Abián, P.; Jiménez, F.; Abián-Vicén, J. Myotendinous asymmetries derived from the prolonged practice of badminton in professional players. PLoS ONE 2019, 14, e0222190. [Google Scholar] [CrossRef] [Green Version]
- Bohm, S.; Mersmann, F.; Marzilger, R.; Schroll, A.; Arampatzis, A. Asymmetry of Achilles tendon mechanical and morphological properties between both legs. Scand. J. Med. Sci.Sports 2015, 25, e124–e132. [Google Scholar] [CrossRef]
- Silbernagel, K.G.; Nilsson-Helander, K.; Thomeé, R.; Eriksson, B.I.; Karlsson, J. A new measurement of heel-rise endurance with the ability to detect functional deficits in patients with Achilles tendon rupture. Knee Surg. Sports Traumatol. Arthrosc. 2010, 18, 258–264. [Google Scholar] [CrossRef]
- Steinfeld, Y.; Akian, R.; Rovitsky, A.; Puchkov, N.; Keren, Y. Assessment of Functional Conservative Treatment of Acute Complete Achilles Tendon Rupture. Isr Med. Assoc. J. 2021, 23, 510–515. [Google Scholar] [PubMed]
- Barfod, K.W.; Nielsen, E.G.; Olsen, B.H.; Vinicoff, P.G.; Troelsen, A.; Holmich, P. Risk of Deep Vein Thrombosis After Acute Achilles Tendon Rupture: A Secondary Analysis of a Randomized Controlled Trial Comparing Early Controlled Motion of the Ankle Versus Immobilization. Orthop. J. Sports Med. 2020, 8, 2325967120915909. [Google Scholar] [CrossRef] [PubMed]
- Sikorski, Ł.; Czamara, A. Assessment of Effectiveness of 15 Weeks of Physical Therapy on Biplanar Ankle Mobility, Gait and Pain Level in Patients Following Operative Repair of the Achilles Tendon. Ortop. Traumatol. Rehabil. 2021, 23, 33–44. [Google Scholar] [CrossRef] [PubMed]
- Ferreira, V.M.L.M.; Oliveira, R.R.; Nazareno, T.S.; Freitas, L.V.; Mendonça, L.D. Interaction of foot and hip factors identifies Achilles tendinopathy occurrence in recreational runners. Phys. Ther. Sport. 2020, 45, 111–119. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Outcome Measure | Group 1 | Group 2 | p |
|---|---|---|---|
| Number of subjects | 15 | 21 | |
| Age (years) | 25.2 ± 2.2 | 24.0 ± 1.9 | 0.09 |
| Body weight (kg) | 73.5 ± 14.1 | 68.0 ± 18.8 | 0.34 |
| Body height (cm) | 177.0 ± 10.7 | 170.8 ± 10.6 | 0.09 |
| BMI | 23.3 ± 3.1 | 22.9 ± 3.6 | 0.74 |
| Sex (women/men) | 7/8 | 14/7 | 0.31 |
| Outcome Measure | Mean ± SD | CI 95% | SEM | CV | p | ES | |
|---|---|---|---|---|---|---|---|
| Achilles tendon length (cm) | Group 1 | 6.5 ± 1.8 | 5.5–7.6 | 0.48 | 28.6 | 0.002 | 1.10 |
| Group 2 | 4.7 ± 1.4 | 4.0–5.3 | 0.31 | 31.0 | |||
| WBLT (cm) | Group 1 | 12.4 ± 2.7 | 10.8–13.9 | 0.72 | 22.5 | 0.0001 | 1.37 |
| Group 2 | 9.0 ± 2.0 | 8.0–9.9 | 0.45 | 23.3 | |||
| Ankle joint ROM (degrees) | Group 1 | 19.9 ± 0.2 | 19.7–20.1 | 0.06 | 1.29 | 0.0000 | 3.68 |
| Group 2 | 14.4 ± 2.1 | 13.5–15.4 | 0.46 | 14.7 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wawrzyński, T.; Pietrzak, B.A.; Mika, A. Does Mobility of the Ankle Joint Depends on Length of the Free Part of the Achilles Tendon? Symmetry 2022, 14, 2313. https://doi.org/10.3390/sym14112313
Wawrzyński T, Pietrzak BA, Mika A. Does Mobility of the Ankle Joint Depends on Length of the Free Part of the Achilles Tendon? Symmetry. 2022; 14(11):2313. https://doi.org/10.3390/sym14112313
Chicago/Turabian StyleWawrzyński, Tomasz, Bernadeta Angelika Pietrzak, and Anna Mika. 2022. "Does Mobility of the Ankle Joint Depends on Length of the Free Part of the Achilles Tendon?" Symmetry 14, no. 11: 2313. https://doi.org/10.3390/sym14112313