
Autologous Matrix Induced Chondrogenesis (AMIC) Compared to Microfractures for Chondral Defects of the Talar Shoulder: A Five-Year Follow-Up Prospective Cohort Study

 ,
, 
 ,
,  ,
, 
Abstract
:1. Introduction
2. Material and Methods
2.1. Patients Recruitment
2.2. Surgical Technique
2.3. Outcomes of Interest
2.4. Statistical Analysis
3. Results
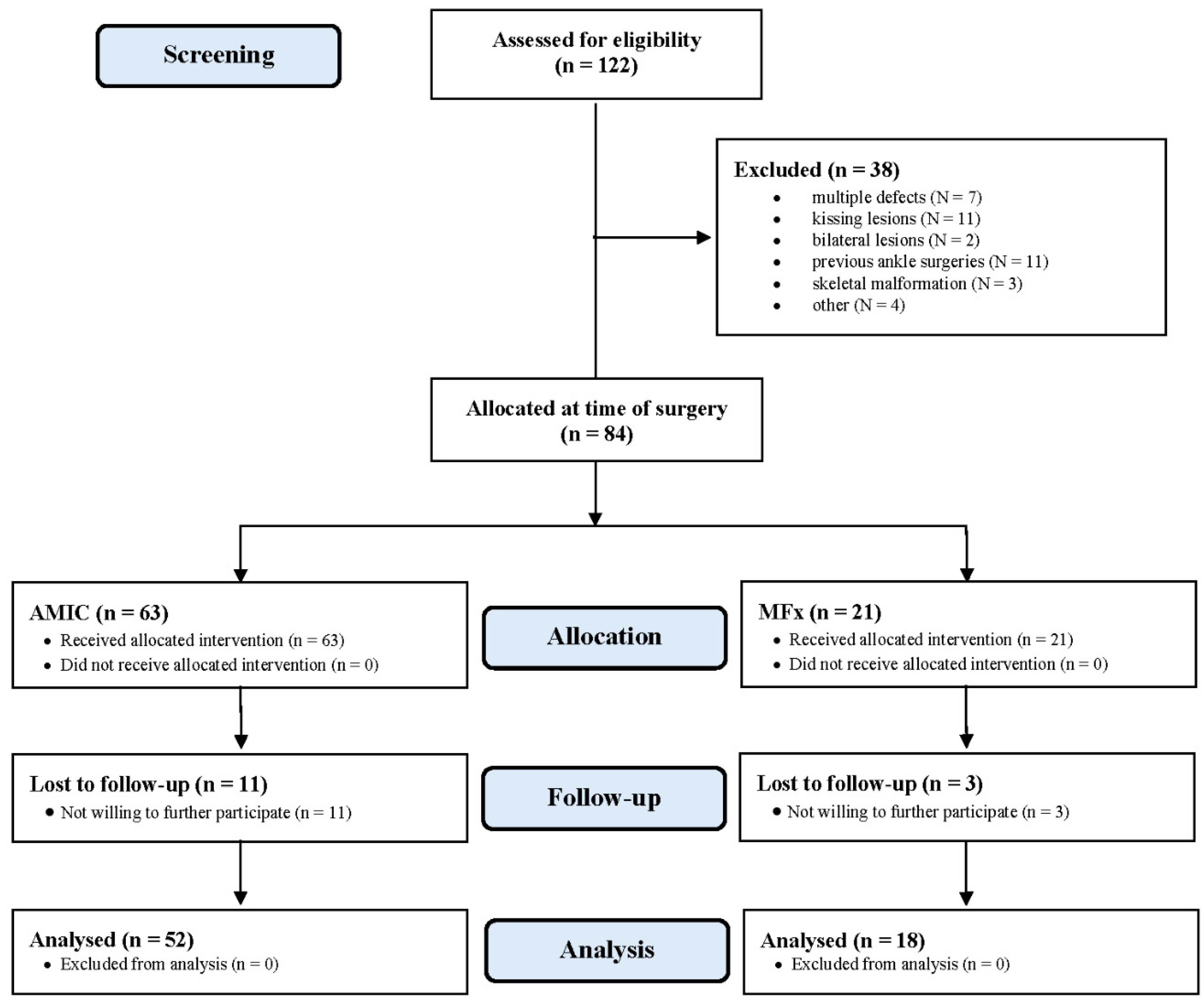
3.1. Recruitment Procedure
3.2. Patients Demographics
3.3. Outcomes of Interest
3.4. Complications
3.5. Subgroup Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Årøen, A.; Løken, S.B.; Heir, S.; Alvik, E.; Ekeland, A.; Granlund, O.G.; Engebretsen, L. Articular Cartilage Lesions in 993 Consecutive Knee Arthroscopies. Am. J. Sports Med. 2004, 32, 211–215. [Google Scholar] [CrossRef] [Green Version]
- Migliorini, F.; Berton, A.; Salvatore, G.; Candela, V.; Khan, W.; Longo, U.G.; Denaro, V. Autologous Chondrocyte Implan-tation and Mesenchymal Stem Cells for the Treatments of Chondral Defects of the Knee—A Systematic Review. Curr. Stem Cell Res. Ther. 2020, 15, 547–556. [Google Scholar] [CrossRef]
- Kreuz, P.; Steinwachs, M.; Erggelet, C.; Krause, S.; Konrad, G.; Uhl, M.; Südkamp, N. Results after microfracture of full-thickness chondral defects in different compartments in the knee. Osteoarthr. Cartil. 2006, 14, 1119–1125. [Google Scholar] [CrossRef] [Green Version]
- Scillia, A.J.; Aune, K.T.; Andrachuk, J.S.; Cain, E.L.; Dugas, J.R.; Fleisig, G.S.; Andrews, J.R. Return to Play After Chondroplasty of the Knee in National Football League Athletes. Am. J. Sports Med. 2015, 43, 663–668. [Google Scholar] [CrossRef] [PubMed]
- Castrodad, I.M.D.; Mease, S.J.; Werheim, E.; McInerney, V.K.; Scillia, A.J. Arthroscopic Chondral Defect Repair with Extracellular Matrix Scaffold and Bone Marrow Aspirate Concentrate. Arthrosc. Tech. 2020, 9, e1241–e1247. [Google Scholar] [CrossRef]
- Gudas, R.; Kalesinskas, R.J.; Kimtys, V.; Stankevičius, E.; Toliušis, V.; Bernotavičius, G.; Smailys, A. A Prospective Randomized Clinical Study of Mosaic Osteochondral Autologous Transplantation Versus Microfracture for the Treatment of Osteochondral Defects in the Knee Joint in Young Athletes. Arthrosc. J. Arthrosc. Relat. Surg. 2005, 21, 1066–1075. [Google Scholar] [CrossRef]
- Richter, D.L.; Schenck, J.R.C., Jr.; Wascher, D.C.; Treme, G. Knee Articular Cartilage Repair and Restoration Techniques: A Review of the Literature. Sports Health 2016, 8, 153–160. [Google Scholar] [CrossRef] [Green Version]
- Bertho, P.; Pauvert, A.; Pouderoux, T.; Robert, H. Treatment of large deep osteochondritis lesions of the knee by autologous matrix-induced chondrogenesis (AMIC): Preliminary results in 13 patients. Orthop. Traumatol. Surg. Res. 2018, 104, 695–700. [Google Scholar] [CrossRef]
- Smith, G.D.; Knutsen, G.; Richardson, J.B. A clinical review of cartilage repair techniques. J. Bone Jt. Surgery. Br. Vol. 2005, 87, 445–449. [Google Scholar] [CrossRef]
- Steinwachs, M.; Guggi, T.; Kreuz, P. Marrow stimulation techniques. Injury 2008, 39 (Suppl. 1), 26–31. [Google Scholar] [CrossRef]
- Aae, T.F.; Randsborg, P.-H.; Lurås, H.; Årøen, A.; Lian, Ø.B. Microfracture is more cost-effective than autologous chondrocyte implantation: A review of level 1 and level 2 studies with 5 year follow-up. Knee Surg. Sports Traumatol. Arthrosc. 2017, 26, 1044–1052. [Google Scholar] [CrossRef] [Green Version]
- El-Rashidy, H.; Villacis, D.; Omar, I.; Kelikian, A.S. Fresh Osteochondral Allograft for the Treatment of Cartilage Defects of the Talus: A Retrospective Review. J. Bone Jt. Surg. Am. Vol. 2011, 93, 1634–1640. [Google Scholar] [CrossRef]
- Behrens, P.; Bitter, T.; Kurz, B.; Russlies, M. Matrix-associated autologous chondrocyte transplantation/implantation (MACT/MACI)—5-year follow-up. Knee 2006, 13, 194–202. [Google Scholar] [CrossRef] [PubMed]
- Migliorini, F.; Eschweiler, J.; Maffulli, N.; Schenker, H.; Baroncini, A.; Tingart, M.; Rath, B. Autologous Matrix-Induced Chondrogenesis (AMIC) and Microfractures for Focal Chondral Defects of the Knee: A Medium-Term Comparative Study. Life 2021, 11, 183. [Google Scholar] [CrossRef]
- Sabaghzadeh, A.; Mirzaee, F.; Rad, H.S.; Bahramian, F.; Alidousti, A.; Aslani, H. Osteochondral autograft transfer (mosaicplasty) for treatment of patients with osteochondral lesions of talus. Chin. J. Traumatol. 2020, 23, 60–62. [Google Scholar] [CrossRef] [PubMed]
- Park, C.H.; Song, K.-S.; Kim, J.R.; Lee, S.-W. Retrospective evaluation of outcomes of bone peg fixation for osteochondral lesion of the talus. Bone Jt. J. 2020, 102-B, 1349–1353. [Google Scholar] [CrossRef]
- Weigelt, L.; Hartmann, R.; Pfirrmann, C.; Espinosa, N.; Wirth, S.H. Autologous Matrix-Induced Chondrogenesis for Osteochondral Lesions of the Talus: A Clinical and Radiological 2- to 8-Year Follow-up Study. Am. J. Sports Med. 2019, 47, 1679–1686. [Google Scholar] [CrossRef] [PubMed]
- Shimozono, Y.; Hurley, E.T.; Nguyen, J.T.; Deyer, T.W.; Kennedy, J.G. Allograft Compared with Autograft in Osteochondral Transplantation for the Treatment of Osteochondral Lesions of the Talus. J. Bone Jt. Surg. Am. Vol. 2018, 100, 1838–1844. [Google Scholar] [CrossRef]
- Ahmad, J.; Jones, K. Comparison of Osteochondral Autografts and Allografts for Treatment of Recurrent or Large Talar Osteochondral Lesions. Foot Ankle Int. 2015, 37, 40–50. [Google Scholar] [CrossRef] [PubMed]
- Kreulen, C.; Giza, E.; Walton, J.; Sullivan, M. Seven-Year Follow-up of Matrix-Induced Autologous Implantation in Talus Articular Defects. Foot Ankle Spéc. 2018, 11, 133–137. [Google Scholar] [CrossRef]
- Schneider, T.E.; Karaikudi, S. Matrix-Induced Autologous Chondrocyte Implantation (MACI) Grafting for Osteochondral Lesions of the Talus. Foot Ankle Int. 2009, 30, 810–814. [Google Scholar] [CrossRef]
- Pagliazzi, G.; Vannini, F.; Battaglia, M.; Ramponi, L.; Buda, R. Autologous Chondrocyte Implantation for Talar Osteochondral Lesions: Comparison Between 5-Year Follow-Up Magnetic Resonance Imaging Findings and 7-Year Follow-Up Clinical Results. J. Foot Ankle Surg. 2018, 57, 221–225. [Google Scholar] [CrossRef]
- Dixon, S.; Harvey, L.; Baddour, E.; Janes, G.; Hardisty, G. Functional Outcome of Matrix-Associated Autologous Chondrocyte Implantation in the Ankle. Foot Ankle Int. 2011, 32, 368–374. [Google Scholar] [CrossRef] [PubMed]
- Behrens, P. Matrixgekoppelte Mikrofrakturierung. Arthroskopie 2005, 18, 193–197. [Google Scholar] [CrossRef]
- Götze, C.; Nieder, C.; Felder, H.; Migliorini, F. AMIC for Focal Osteochondral Defect of the Talar Shoulder. Life 2020, 10, 328. [Google Scholar] [CrossRef] [PubMed]
- De Girolamo, L.; Schönhuber, H.; Viganò, M.; Bait, C.; Quaglia, A.; Thiebat, G.; Volpi, P. Autologous Matrix-Induced Chondrogenesis (AMIC) and AMIC Enhanced by Autologous Concentrated Bone Marrow Aspirate (BMAC) Allow for Stable Clinical and Functional Improvements at up to 9 Years Follow-Up: Results from a Randomized Controlled Study. J. Clin. Med. 2019, 8, 392. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Panni, A.S.; Del Regno, C.; Mazzitelli, G.; D’Apolito, R.; Corona, K.; Vasso, M. Good clinical results with autologous matrix-induced chondrogenesis (Amic) technique in large knee chondral defects. Knee Surg. Sports Traumatol. Arthrosc. 2017, 26, 1130–1136. [Google Scholar] [CrossRef]
- Schagemann, J.; Behrens, P.; Paech, A.; Riepenhof, H.; Kienast, B.; Mittelstädt, H.; Gille, J. Mid-term outcome of arthroscopic AMIC for the treatment of articular cartilage defects in the knee joint is equivalent to mini-open procedures. Arch. Orthop. Trauma Surg. 2018, 138, 819–825. [Google Scholar] [CrossRef]
- Gille, J.; Behrens, P.; Volpi, P.; De Girolamo, L.; Reiss, E.; Zoch, W.; Anders, S. Outcome of Autologous Matrix Induced Chondrogenesis (AMIC) in cartilage knee surgery: Data of the AMIC Registry. Arch. Orthop. Trauma Surg. 2012, 133, 87–93. [Google Scholar] [CrossRef] [Green Version]
- Von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gøtzsche, P.C.; Vandenbroucke, J.P. The strengthening the reporting of observational studies in epidemiology (STROBE) statement: Guidelines for reporting observational studies. J. Clin. Epidemiol. 2008, 61, 344–349. [Google Scholar] [CrossRef] [Green Version]
- Heir, S.; Nerhus, T.K.; Røtterud, J.H.; Løken, S.; Ekeland, A.; Engebretsen, L.; Årøen, A. Focal Cartilage Defects in the Knee Impair Quality of Life as Much as Severe Osteoarthritis: A Comparison of Knee Injury and Osteoarthritis Outcome Score in 4 Patient Categories Scheduled for Knee Surgery. Am. J. Sports Med. 2010, 38, 231–237. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Atala, A.; Irvine, D.J.; Moses, M.; Shaunak, S. Wound Healing Versus Regeneration: Role of the Tissue Environment in Regenerative Medicine. MRS Bull. 2010, 35, 597–606. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Buckwalter, J.A. Articular Cartilage Injuries. Clin. Orthop. Relat. Res. 2002, 402, 21–37. [Google Scholar] [CrossRef]
- Irwin, R.M.; Gao, T.; Boys, A.J.; Ortved, K.; Cohen, I.; Bonassar, L.J. Microscale strain mapping demonstrates the importance of interface slope in the mechanics of cartilage repair. J. Biomech. 2021, 114, 110159. [Google Scholar] [CrossRef] [PubMed]
- Trengove, M.A.; Di Bella, C.; O’Connor, A.J. The Challenge of Cartilage Integration: Understanding a Major Barrier to Chondral Repair. Tissue Eng. Part B Rev. 2021. [Google Scholar] [CrossRef]
- Wiewiorski, M.; Barg, A.; Valderrabano, V. Autologous Matrix-induced Chondrogenesis in Osteochondral Lesions of the Talus. Foot Ankle Clin. 2013, 18, 151–158. [Google Scholar] [CrossRef]
- Galla, M.; Duensing, I.; Kahn, T.L.; Barg, A. Open reconstruction with autologous spongiosa grafts and matrix-induced chondrogenesis for osteochondral lesions of the talus can be performed without medial malleolar osteotomy. Knee Surg. Sports Traumatol. Arthrosc. 2018, 27, 2789–2795. [Google Scholar] [CrossRef]
- Valderrabano, V.; Miska, M.; Leumann, A.; Wiewiorski, M. Reconstruction of Osteochondral Lesions of the Talus with Autologous Spongiosa Grafts and Autologous Matrix-Induced Chondrogenesis. Am. J. Sports Med. 2013, 41, 519–527. [Google Scholar] [CrossRef]
- Becher, C.; Malahias, M.A.; Ali, M.M.; Maffulli, N.; Thermann, H. Arthroscopic microfracture vs. arthroscopic autologous matrix-induced chondrogenesis for the treatment of articular cartilage defects of the talus. Knee Surg. Sports Traumatol. Arthrosc. 2019, 27, 2731–2736. [Google Scholar] [CrossRef]
- Chung, J.Y.; Lee, D.-H.; Kim, T.H.; Kwack, K.-S.; Yoon, K.H.; Min, B.-H. Cartilage extra-cellular matrix biomembrane for the enhancement of microfractured defects. Knee Surg. Sports Traumatol. Arthrosc. 2014, 22, 1249–1259. [Google Scholar] [CrossRef]
- Volz, M.; Schaumburger, J.; Frick, H.; Grifka, J.; Anders, S. A randomized controlled trial demonstrating sustained benefit of Autologous Matrix-Induced Chondrogenesis over microfracture at five years. Int. Orthop. 2017, 41, 797–804. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, K.T.; Kim, J.S.; Young, K.W.; Lee, Y.K.; Park, Y.U.; Kim, Y.H.; Cho, H.K. The use of fibrin matrix-mixed gel-type autologous chondrocyte implantation in the treatment for osteochondral lesions of the talus. Knee Surg. Sports Traumatol. Arthrosc. 2012, 21, 1251–1260. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Leumann, A.; Horisberger, M.; Buettner, O.; Mueller-Gerbl, M.; Valderrabano, V. Medial malleolar osteotomy for the treatment of talar osteochondral lesions: Anatomical and morbidity considerations. Knee Surg. Sports Traumatol. Arthrosc. 2015, 24, 2133–2139. [Google Scholar] [CrossRef]
- Zengerink, M.; Van Dijk, C.N. Complications in ankle arthroscopy. Knee Surg. Sports Traumatol. Arthrosc. 2012, 20, 1420–1431. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Amendola, A.; Petrik, J.; Webster-Bogaert, S. Ankle arthroscopy: Outcome in 79 consecutive patients. Arthrosc. J. Arthrosc. Relat. Surg. 1996, 12, 565–573. [Google Scholar] [CrossRef]
- Barber, F.A.; Click, J.; Britt, B.T. Complications of Ankle Arthroscopy. Foot Ankle 1990, 10, 263–266. [Google Scholar] [CrossRef]
- Bonnin, M.; Bouysset, M. Arthroscopy of the ankle: Analysis of results and indications on a series of 75 cases. Foot Ankle Int. 1999, 20, 744–751. [Google Scholar] [CrossRef]
- Cutsuries, A.M.; Saltrick, K.R.; Wagner, J.; Catanzariti, A.R. Arthroscopic arthroplasty of the ankle joint. Clin. Podiatr. Med. Surg. 1994, 11, 449–467. [Google Scholar]
- Ferkel, R.D.; Small, H.N.; Gittins, J.E. Complications in Foot and Ankle Arthroscopy. Clin. Orthop. Relat. Res. 2001, 391, 89–104. [Google Scholar] [CrossRef] [PubMed]
- Frey, C.; Feder, K.S.; DiGiovanni, C. Arthroscopic Evaluation of the Subtalar Joint: Does Sinus Tarsi Syndrome Exist? Foot Ankle Int. 1999, 20, 185–191. [Google Scholar] [CrossRef] [PubMed]
- Van Dijk, N.C.; Van Bergen, C.J.A. Advancements in Ankle Arthroscopy. J. Am. Acad. Orthop. Surg. 2008, 16, 635–646. [Google Scholar] [CrossRef] [PubMed]
- De Leeuw, P.A.J.; Golanó, P.; Clavero, J.A.; Van Dijk, C.N. Anterior ankle arthroscopy, distraction or dorsiflexion? Knee Surg. Sports Traumatol. Arthrosc. 2010, 18, 594–600. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Albano, D.; Martinelli, N.; Bianchi, A.; Giacalone, A.; Sconfienza, L.M. Evaluation of reproducibility of the MOCART score in patients with osteochondral lesions of the talus repaired using the autologous matrix-induced chondrogenesis technique. La Radiol. Med. 2017, 122, 909–917. [Google Scholar] [CrossRef] [PubMed]
- Blackman, A.J.; Smith, M.V.; Flanigan, D.C.; Matava, M.J.; Wright, R.W.; Brophy, R.H. Correlation between Magnetic Reso-Nance Imaging and Clinical Outcomes after Cartilage Repair surgery in the Knee: A Systematic Review and Meta-Analysis. Am. J. Sports Med. 2013, 41, 1426–1434. [Google Scholar] [CrossRef] [PubMed]
- Shive, M.S.; Stanish, W.D.; McCormack, R.; Forriol, F.; Mohtadi, N.; Pelet, S.; Desnoyers, J.; Méthot, S.; Vehik, K.; Restrepo, A. BST-CarGel® Treatment Maintains Cartilage Repair Superiority over Microfracture at 5 Years in a Multicenter Randomized Controlled Trial. Cartilage 2014, 6, 62–72. [Google Scholar] [CrossRef] [PubMed]
- Albano, D.; Martinelli, N.; Bianchi, A.; Messina, C.; Malerba, F.; Sconfienza, L.M. Clinical and imaging outcome of osteochondral lesions of the talus treated using autologous matrix-induced chondrogenesis technique with a biomimetic scaffold. BMC Musculoskelet. Disord. 2017, 18, 306. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Endpoint | AMIC (n = 52) | MFx (n = 18) | p | |
|---|---|---|---|---|
| Follow-up (months) | 44.2 ± 19.9 | 41.5 ± 18.1 | n.s. | |
| Mean age | 31.5 ± 2.1 | 33.3 ± 6.2 | n.s. | |
| Sex (female) | 44% (23 of 52) | 44% (8 of 18) | n.s. | |
| Right ankle | 52% (27 of 52) | 56% (10 of 18) | n.s. | |
| Articular side (talus) | ||||
| medial | 60% (31 of 52) | 72% (13 of 18) | n.s. | |
| lateral | 40% (21 of 52) | 18% (5 of 18) | n.s. | |
| Cancellous bone grafting (n) | 39% (20 of 52) | |||
| from osteotomy site | 14% (7 of 52) | |||
| from iliac crest | 25% (13 of 52) | |||
| Approach | ||||
| Malleolar osteotomy (n) | 44% (23 of 52) | |||
| Distraction (n) | 56% (29 of 52) | |||
| Symptom duration (months) | 48.1 ± 80.7 | 39.3 ± 50.41 | n.s. | |
| Length of stay (days) | 3.5 ± 1.6 | 1.9 ± 2.0 | 0.01 | |
| Area of defect (cm2) | 2.8 ± 1.5 | 2.4 ± 0.4 | n.s. | |
| BMI (kg/m2) | 27.1 ± 6.4 | 26.9 ± 3.8 | n.s. | |
| Endpoint | AMIC (n = 52) | MFx (n = 18) | MD | 95% CI | p |
|---|---|---|---|---|---|
| MOCART | 80.0 ± 25.4 | 66.8 ± 33.1 | 13.2 | −1.822 to 28.222 | 0.08 |
| AOFAS | 83.8 ± 12.4 | 75.0 ± 19.3 | 8.8 | 0.921 to 16.679 | 0.03 |
| VAS (0–10) | 1.9 ± 0.8 | 3.3 ± 3.1 | 1.4 | −2.326 to −0.474 | 0.003 |
| Tegner | 4.3 ± 1.5 | 3.1 ± 2.1 | 1.2 | 0.288 to 2.112 | 0.01 |
| Endpoint | AMIC (n = 52) | MFx (n = 18) | OR | 95% CI | p |
|---|---|---|---|---|---|
| Reoperation | 10% (5 of 52) | 39% (7 of 18) | 0.17 | 0.0446 to 0.6271 | 0.008 |
| Failures | 13% (7 of 52) | 50% (9 of 18) | 0.16 | 0.0459 to 0.5268 | 0.003 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Migliorini, F.; Eschweiler, J.; Maffulli, N.; Schenker, H.; Driessen, A.; Rath, B.; Tingart, M. Autologous Matrix Induced Chondrogenesis (AMIC) Compared to Microfractures for Chondral Defects of the Talar Shoulder: A Five-Year Follow-Up Prospective Cohort Study. Life 2021, 11, 244. https://doi.org/10.3390/life11030244
Migliorini F, Eschweiler J, Maffulli N, Schenker H, Driessen A, Rath B, Tingart M. Autologous Matrix Induced Chondrogenesis (AMIC) Compared to Microfractures for Chondral Defects of the Talar Shoulder: A Five-Year Follow-Up Prospective Cohort Study. Life. 2021; 11(3):244. https://doi.org/10.3390/life11030244
Chicago/Turabian StyleMigliorini, Filippo, Jörg Eschweiler, Nicola Maffulli, Hanno Schenker, Arne Driessen, Björn Rath, and Markus Tingart. 2021. "Autologous Matrix Induced Chondrogenesis (AMIC) Compared to Microfractures for Chondral Defects of the Talar Shoulder: A Five-Year Follow-Up Prospective Cohort Study" Life 11, no. 3: 244. https://doi.org/10.3390/life11030244
APA StyleMigliorini, F., Eschweiler, J., Maffulli, N., Schenker, H., Driessen, A., Rath, B., & Tingart, M. (2021). Autologous Matrix Induced Chondrogenesis (AMIC) Compared to Microfractures for Chondral Defects of the Talar Shoulder: A Five-Year Follow-Up Prospective Cohort Study. Life, 11(3), 244. https://doi.org/10.3390/life11030244