
Accuracy of Mandibular Foramen Localization Using Digital Orthopantomogram (OPG) in Middle Eastern Population

 and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Ethical Approval, Study Design and Sampling
- Adult patients aged 18 years and older;
- Availability of digital OPG and CBCT images taken within an interval no longer than 7 days;
- No history of uncontrolled medical illnesses;
- No evidence of facial asymmetry, pathological lesions, fractures or surgeries in the mandible;
- Presence of at least 3/4 of dentition with bilateral mandibular molars (1st and 2nd), along with opposing maxillary molar teeth (to avoid variations in localization and measurement due to supra-eruption);
- No radiographic evidence of inordinate occlusal wear.
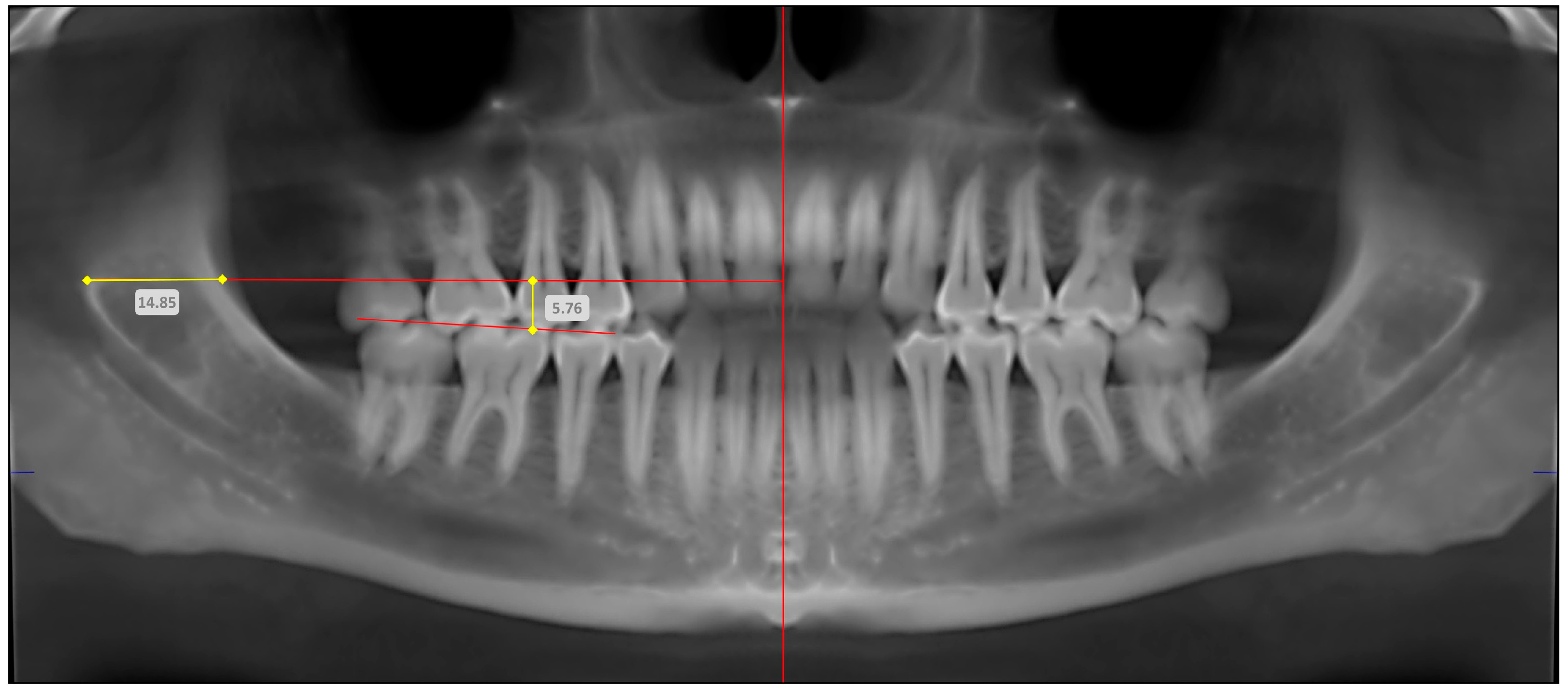
2.2. Image Acquisition for OPG and CBCT
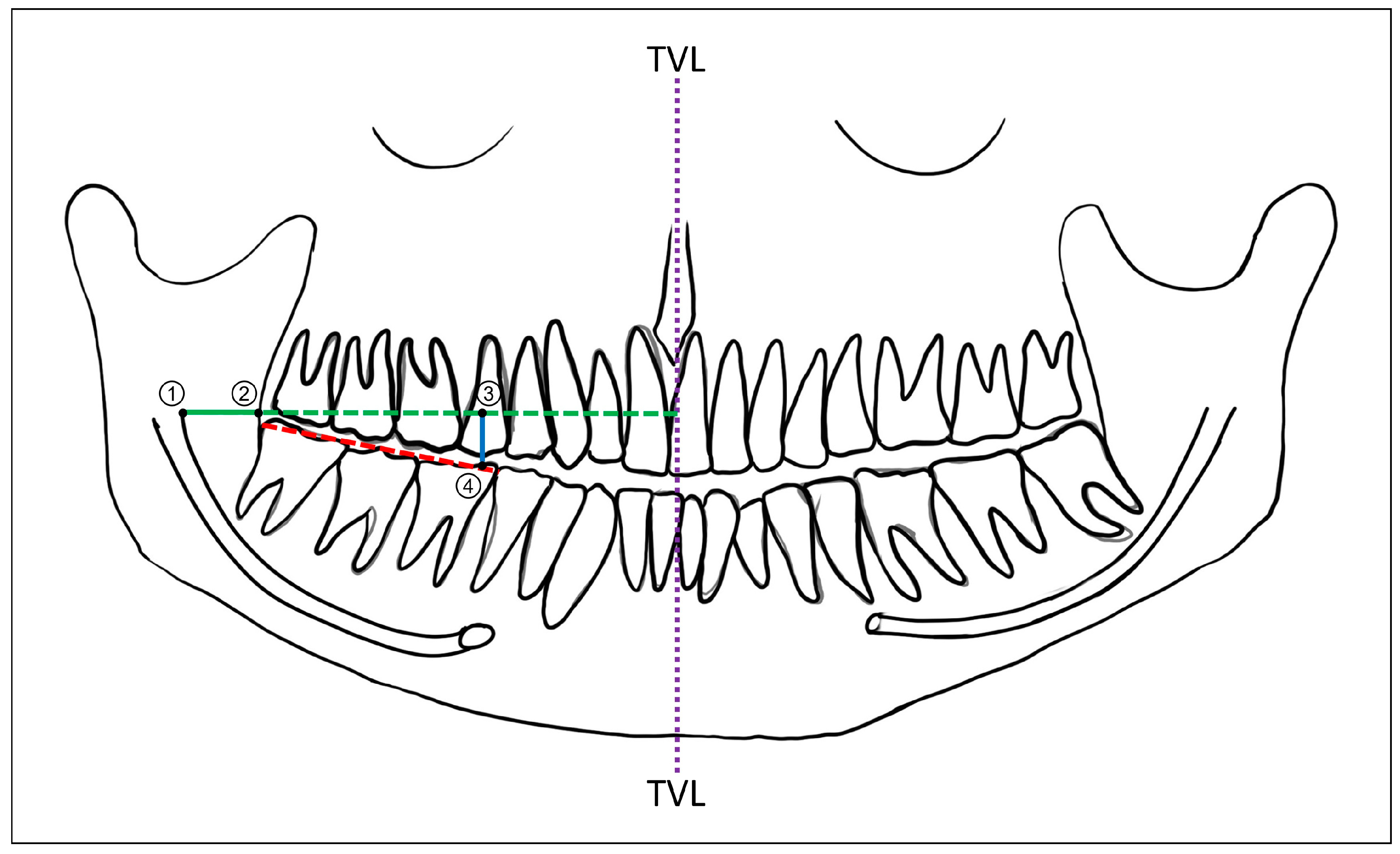
2.3. Radiographic Reference Points and Measurements
2.4. Intra- and Inter-Examiner Reliability
2.5. Statistical Analysis
3. Results
3.1. Accuracy of OPG in Determining Mandibular Foramen Location
3.2. Comparison Based on Anatomic Location (Right or Left Side) and Demographic Variables (Age and Gender)
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- De Castro, R.W.Q.; Marlière, D.A.A.; Haiter Neto, F.; Groppo, F.C.; Asprino, L. Positions of the Mandibular Foramen and Canal in Different Skeletal Classes and Implications for Bilateral Sagittal Split Osteotomy. J. Maxillofac. Oral Surg. 2024. [Google Scholar] [CrossRef]
- Mathew, A.; Mohan, N. Prevalence, length, and patterns of Anterior Loop among the South Indian population: A comparative study between Panoramic Radiography and Cone Beam Computed Tomography. Porto Biomed. J. 2023, 8, e216. [Google Scholar] [CrossRef] [PubMed]
- Vorakulpipat, C.; Arayapisit, T.; Topothai, P.; Bhunyanaphakul, V.; Tiptimaphan, K.; Apilakkitakul, N.; Chantadul, V. Determining the position of the lingula and the mandibular foramen using the antilingula in orthognathic surgery. BMC Oral Health 2024, 24, 499. [Google Scholar] [CrossRef]
- Chen, C.M.; Lee, H.N.; Chen, Y.T.; Hsu, K.J. Locating the Mandibular Lingula Using Cone-Beam Computed Tomography: A Literature Review. J. Clin. Med. 2023, 12, 881. [Google Scholar] [CrossRef]
- Ahn, B.S.; Oh, S.H.; Heo, C.K.; Kim, G.T.; Choi, Y.S.; Hwang, E.H. Cone-beam computed tomography of mandibular foramen and lingula for mandibular anesthesia. Imaging Sci. Dent. 2020, 50, 125–132. [Google Scholar] [CrossRef]
- Zhou, C.; Jeon, T.H.; Jun, S.H.; Kwon, J.J. Evaluation of mandibular lingula and foramen location using 3-dimensional mandible models reconstructed by cone-beam computed tomography. Maxillofac. Plast. Reconstr. Surg. 2017, 39, 30. [Google Scholar] [CrossRef]
- Narayan, R.K.; Ghosh, S.K. Morphological analysis of mandibular foramen through anatomical planes: Implications for inferior alveolar nerve block. Anat. Sci. Int. 2020, 95, 209–218. [Google Scholar] [CrossRef]
- Ramalingam, S.; Bhargava, D. Advances in surgical extraction of the mandibular third molars. In Transalveolar Extraction of the Mandibular Third Molars; CRC Press: Boca Raton, FL, USA, 2022; pp. 163–175. [Google Scholar]
- Gherghiţă, O.R.; Nimigean, V.R.; Csiki, I.E.; Băran-Poesina, V.; Vîrlan, M.J.R.; Nimigean, V. Direct and imaging morphometry for the localization of the mandibular foramen (MF) in dentate and edentulous human subjects. Rom. J. Morphol. Embryol. = Rev. Roum. De Morphol. Et Embryol. 2020, 61, 783–791. [Google Scholar] [CrossRef] [PubMed]
- Holliday, R.; Jackson, I. Superior position of the mandibular foramen and the necessary alterations in the local anaesthetic technique: A case report. Br. Dent. J. 2011, 210, 207–211. [Google Scholar] [CrossRef]
- Takasugi, Y.; Furuya, H.; Moriya, K.; Okamoto, Y. Clinical evaluation of inferior alveolar nerve block by injection into the pterygomandibular space anterior to the mandibular foramen. Anesth. Prog. 2000, 47, 125–129. [Google Scholar]
- Patil, K.; Guledgud, M.V.; Bhattacharya, P.T. Reliability of Panoramic Radiographs in the Localization of Mandibular Foramen. J. Clin. Diagn. Res. JCDR 2015, 9, ZC35–ZC38. [Google Scholar] [CrossRef] [PubMed]
- Thangavelu, K.; Kannan, R.; Kumar, N.S.; Rethish, E.; Sabitha, S.; Sayeeganesh, N. Significance of localization of mandibular foramen in an inferior alveolar nerve block. J. Nat. Sci. Biol. Med. 2012, 3, 156–160. [Google Scholar] [CrossRef] [PubMed]
- Kaur, R.; Singla, R.K.; Sharma, R.; Singla, S. Localization of mandibular foramen—A comparison between dry bones and orthopantomogram. J. Med. Life 2022, 15, 669–674. [Google Scholar] [CrossRef] [PubMed]
- Neves, F.S.; Nascimento, M.C.; Oliveira, M.L.; Almeida, S.M.; Bóscolo, F.N. Comparative analysis of mandibular anatomical variations between panoramic radiography and cone beam computed tomography. Oral Maxillofac. Surg. 2014, 18, 419–424. [Google Scholar] [CrossRef]
- Trost, O.; Salignon, V.; Cheynel, N.; Malka, G.; Trouilloud, P. A simple method to locate mandibular foramen: Preliminary radiological study. Surg. Radiol. Anat. SRA 2010, 32, 927–931. [Google Scholar] [CrossRef]
- Maoxia, W.; Anchun, M. A digital workflow for the inferior alveolar nerve block in the edentulous mandible. J. Prosthet. Dent. 2023, 130, 141–145. [Google Scholar] [CrossRef]
- Palma, L.F.; Almeida, F.S.O.; Lombardi, L.A.; Cavalli, M.A.; de Moraes, L.O.C. Is the inferior occlusal plane a reliable anatomic landmark for inferior alveolar nerve block? A study on dry mandibles of Brazilian adults. Morphol. Bull. L’assoc. Anat. 2020, 104, 59–63. [Google Scholar] [CrossRef]
- Lasemi, E.; Motamedi, M.H.K.; Talaeipour, A.R.; Shafaeifard, S.; Fard, M.J.K.; Navi, F.; Lasemi, R.; Zardi, Z.; Alipanah, F. Panoramic Radiographic Relationship of the Mandibular Foramen to the Anterior Border of the Ramus and Occlusal Plane as an Aid in Inferior Alveolar Nerve Block. Anesth. Prog. 2019, 66, 20–23. [Google Scholar] [CrossRef]
- Zhang, J.; Jiang, Y.; Gao, F.; Zhao, S.; Yang, F.; Song, L. A Fast Automatic Reconstruction Method for Panoramic Images Based on Cone Beam Computed Tomography. Electronics 2022, 11, 2404. [Google Scholar] [CrossRef]
- Ahmed, A.A.; Ahmed, R.M.; Jamleh, A.; Spagnuolo, G. Morphometric Analysis of the Mandibular Canal, Anterior Loop, and Mental Foramen: A Cone-Beam Computed Tomography Evaluation. Int. J. Environ. Res. Public Health 2021, 18, 3365. [Google Scholar] [CrossRef]
- Al-Shayyab, M.H. A simple method to locate mandibular foramen with cone-beam computed tomography and its relevance to oral and maxillofacial surgery: A radio-anatomical study. Surg. Radiol. Anat. SRA 2018, 40, 625–634. [Google Scholar] [CrossRef] [PubMed]
- Park, H.S.; Lee, J.H. A comparative study on the location of the mandibular foramen in CBCT of normal occlusion and skeletal class II and III malocclusion. Maxillofac. Plast. Reconstr. Surg. 2015, 37, 25. [Google Scholar] [CrossRef] [PubMed]
- Wei, X.; Gu, P.; Hao, Y.; Wang, J. Detection and characterization of anterior loop, accessory mental foramen, and lateral lingual foramen by using cone beam computed tomography. J. Prosthet. Dent. 2020, 124, 365–371. [Google Scholar] [CrossRef]
- Dhand, N.K.; Khatkar, M.S. Statulator: An Online Statistical Calculator. Sample Size Calculator for Comparing Two Independent Means. Available online: http://statulator.com/SampleSize/ss2M.html (accessed on 12 August 2024).
- Ramalingam, S.; Habib, S.R.; Sundar, C.; Dawas, A.B.; Al-Rashed, M.; Al-Bader, R. Perceptions of dental interns in Saudi Arabia toward implant placement in medically compromised patients. J. Educ. Health Promot. 2017, 6, 104. [Google Scholar] [CrossRef]
- Christmann, A.; Van Aelst, S. Robust estimation of Cronbach’s alpha. J. Multivar. Anal. 2006, 97, 1660–1674. [Google Scholar] [CrossRef]
- Ramalingam, S.; Sundar, C.; Jansen, J.A.; Alghamdi, H. Chapter 1—Alveolar bone science: Structural characteristics and pathological changes. In Dental Implants and Bone Grafts; Alghamdi, H., Jansen, J., Eds.; Woodhead Publishing: Cambridge, UK, 2020; pp. 1–22. [Google Scholar] [CrossRef]
- AlHindi, M.; Rashed, B.; AlOtaibi, N. Failure rate of inferior alveolar nerve block among dental students and interns. Saudi Med. J. 2016, 37, 84–89. [Google Scholar] [CrossRef] [PubMed]
- Feuerstein, D.; Costa-Mendes, L.; Esclassan, R.; Marty, M.; Vaysse, F.; Noirrit, E. The mandibular plane: A stable reference to localize the mandibular foramen, even during growth. Oral Radiol. 2020, 36, 69–79. [Google Scholar] [CrossRef]
- Sevmez, F.; Orhan, M.; Bahşi, I.; Yalçin, E.D. Examination of the Safe Zone in Mandibular Ramus Osteotomies. J. Craniofacial Surg. 2021, 32, 2219–2222. [Google Scholar] [CrossRef]
- Prado, F.B.; Groppo, F.C.; Volpato, M.C.; Caria, P.H. Morphological changes in the position of the mandibular foramen in dentate and edentate Brazilian subjects. Clin. Anat. 2010, 23, 394–398. [Google Scholar] [CrossRef]
- Matveeva, N.; Popovska, L.; Evrosimovska, B.; Chadikovska, E.; Nikolovska, J. Morphological alterations in the position of the mandibular foramen in dentate and edentate mandibles. Anat. Sci. Int. 2018, 93, 340–350. [Google Scholar] [CrossRef]
- Shalini, R.; RaviVarman, C.; Manoranjitham, R.; Veeramuthu, M. Morphometric study on mandibular foramen and incidence of accessory mandibular foramen in mandibles of south Indian population and its clinical implications in inferior alveolar nerve block. Anat. Cell Biol. 2016, 49, 241–248. [Google Scholar] [CrossRef] [PubMed]
- Vathariparambath, N.; Krishnamurthy, N.H.; Chikkanarasaiah, N. A Cone Beam Computed Tomographic Study on the Location of Mandibular and Mental Foramen in Indian Pediatric Population. Int. J. Clin. Pediatr. Dent. 2022, 15, 422–427. [Google Scholar] [CrossRef] [PubMed]
- Cellina, M.; Martinenghi, C.; De Nardi, S.; Palamenghi, A.; Cè, M.; Sforza, C.; Cappella, A.; Gibelli, D. Anatomy of the Mental Foramen: Relationship among Different Metrical Parameters for Accurate Localization. Appl. Sci. 2023, 13, 9235. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Description | Radiographic Technique | Abbreviation Based on Anatomic Localization | |
|---|---|---|---|---|
| Right | Left | |||
| Anteroposterior position of mandibular foramen | Horizontal distance from anteroinferior border of mandibular foramen to anterior border of mandibular ramus | OPG | MF-AP-OPG (Right) | MF-AP-OPG (Left) |
| CBCT | MF-AP-CBCT (Right) | MF-AP-CBCT (Left) | ||
| Superoinferior position of mandibular foramen | Vertical distance from anteroinferior border of mandibular foramen to mandibular occlusal plane (at level of mesial cusp of first molar) | OPG | MF-SI-OPG (Right) | MF-SI-OPG (Left) |
| CBCT | MF-SI-CBCT (Right) | MF-SI-CBCT (Left) | ||
| Mandibular Foramen Position | Anatomic Localization | Imaging Technique | t-Statistic | p-Value | Cronbach’s Alpha | |
|---|---|---|---|---|---|---|
| OPG | CBCT | |||||
| Mean ± SD (Range) | Mean ± SD (Range) | |||||
| Anteroposterior position | Right | 13.53 ± 2.44 (7.1–20.2) | 13.61 ± 2.39 (7.8–19.6) | 0.335 | 0.738 | 0.942 |
| Left | 13.19 ± 2.25 (7.7–18.1) | 13.36 ± 2.19 (8.1–18.8) | 0.773 | 0.439 | 0.903 | |
| Superoinferior position | Right | 5.25 ± 1.71 (4.2–6.2) | 5.59 ± 1.66 (4.5–6.6) | 2.038 | 0.042 | 0.939 |
| Left | 5.41 ± 1.65 (4.1–6.3) | 5.52 ± 1.61 (4.6–6.5) | 0.682 | 0.496 | 0.912 | |
| Independent Demographic Variable | Difference in Anteroposterior Position of Right Mandibular Foramen | Difference in Anteroposterior Position of Left Mandibular Foramen | Comparison between Right and Left Sides | |||
|---|---|---|---|---|---|---|
| Mean ± SD | p-Value | Mean ± SD | p-Value | p-Value | ||
| Overall (n = 204) | 0.08 ± 0.24 | - | 0.17 ± 0.22 | - | <0.01 | |
| Gender | Male (n = 100) | 0.24 ± 1.13 | 0.045 | 0.46 ± 1.29 | 0.029 | - |
| Female (n = 104) | 0.08 ± 1.12 * | 0.03 ± 1.49 * | ||||
| Age group | 18–25 years (n = 32) | 0.15 ± 0.94 * | 0.454 | 0.74 ± 2.10 * | 0.055 | - |
| 26–40 years (n = 122) | 0.11 ± 1.08 | 0.02 ± 1.49 | ||||
| ≥41 years (n = 50) | 0.15 ± 1.36 | 0.57 ± 2.62 * | ||||
| Independent Demographic Variable | Difference in Anteroposterior Position of Right Mandibular Foramen | Difference in Anteroposterior Position of Left Mandibular Foramen | Comparison between Right and Left Sides | |||
| Mean ± SD | p-Value | Mean ± SD | p-Value | p-Value | ||
| Overall (n = 204) | 0.34 ± 0.17 | - | 0.11 ± 0.16 | - | <0.01 | |
| Gender | Male (n = 100) | 0.33 ± 1.02 | 0.942 | 0.19 ± 0.75 | 0.321 | - |
| Female (n = 104) | 0.34 ± 0.94 | 0.06 ± 1.08 | ||||
| Age group | 18–25 years (n = 32) | 0.44 ± 1.22 | 0.781 | 0.14 ± 0.81 * | 0.157 | - |
| 26–40 years (n = 122) | 0.32 ± 0.96 | 0.21 ± 0.98 | ||||
| ≥41 years (n = 50) | 0.29 ± 0.87 | 0.08 ± 0.87 | ||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alali, Y.S.; Mohammed, W.A.; Alotaibi, S.M.; Alshehri, S.; Alshayban, M. Accuracy of Mandibular Foramen Localization Using Digital Orthopantomogram (OPG) in Middle Eastern Population. Diagnostics 2024, 14, 2173. https://doi.org/10.3390/diagnostics14192173
Alali YS, Mohammed WA, Alotaibi SM, Alshehri S, Alshayban M. Accuracy of Mandibular Foramen Localization Using Digital Orthopantomogram (OPG) in Middle Eastern Population. Diagnostics. 2024; 14(19):2173. https://doi.org/10.3390/diagnostics14192173
Chicago/Turabian StyleAlali, Yasser S., Wajdi A. Mohammed (Bin), Sami M. Alotaibi, Sami Alshehri, and Muath Alshayban. 2024. "Accuracy of Mandibular Foramen Localization Using Digital Orthopantomogram (OPG) in Middle Eastern Population" Diagnostics 14, no. 19: 2173. https://doi.org/10.3390/diagnostics14192173